On This Page – Quick Medical Summary
Your CMP results, explained — start here
A flagged number on a blood test can turn an ordinary afternoon into a spiral of worry, and you deserve a clear answer fast. This guide explains the comprehensive metabolic panel (CMP) — what each of its 14 measurements means, what a high or low result usually does and doesn’t indicate, and what to do next. Wherever you are right now, start here:
- You have your results and something is flagged. Jump to how to read your report and the marker-by-marker sections below — and know that a single abnormal result is rarely a diagnosis on its own. This is also the place to start if you’re reading a panel for a parent or someone you care for.
- You’ve been told you need a CMP. Start with what the test measures and why your provider ordered it, then check the fasting and preparation guidance so tomorrow’s blood draw goes smoothly.
- You’re worried about what it costs. Skip ahead to what a CMP costs with and without insurance, where the same test is cheapest, and how to avoid a surprise bill.
- You get this test regularly to monitor a condition. Focus on the pattern-reading and “what can throw off your results” sections, which explain how providers track your numbers over time rather than reacting to one reading.
You do not need a medical background to use this guide. Each section translates the clinical terms into plain language, shows you the sourced reference ranges, and points you to the exact question worth asking your provider.
ℹ️ Medical Disclaimer: The result interpretations, reference ranges, condition information, medication effects, fasting guidance, and cost and insurance details in this article reflect current clinical references from the sources cited and are for general education only. They are not medical advice and cannot interpret your individual results. A comprehensive metabolic panel is read in the context of your full panel, your health history, the medicines you take, and your provider’s judgment — one out-of-range value is not a diagnosis. Talk with your primary care provider or the clinician who ordered your test before making any decision based on your results, and seek prompt medical care for severe or rapidly worsening symptoms.
What is a comprehensive metabolic panel?
A comprehensive metabolic panel is a routine blood test that measures 14 different substances in your blood to give your provider a broad picture of your metabolism, organ function, and chemical balance. It checks your blood sugar, kidney and liver function, protein levels, and the electrolytes that keep your fluids and acid–base balance in range. It is one of the most commonly ordered blood tests in routine care.
You may also see it labeled chem 14, chemistry panel, chemistry screen, or metabolic panel — different names for the same test.
What a CMP measures
The 14 substances fall into five groups, each telling a different part of the story:
- Blood sugar: glucose, your body’s main energy source.
- Kidney markers: blood urea nitrogen (BUN) and creatinine, waste products your kidneys filter out.
- Liver markers: the enzymes ALP (alkaline phosphatase), ALT (alanine transaminase), and AST (aspartate aminotransferase), plus bilirubin, a waste product from the breakdown of old red blood cells.
- Proteins: albumin, the main protein made by your liver, and total protein.
- Electrolytes and a mineral: sodium, potassium, bicarbonate, and chloride, plus calcium — minerals that control fluid balance, pH, and the proper function of your nerves, muscles, and heart.
The NIH’s overview groups the panel this exact way, and notes that a CMP can flag certain conditions before you have symptoms.
🔬 How It Works: “Metabolism” is simply how your body turns food into energy and clears the waste that process creates. Your liver and kidneys do much of that work, so the levels of the substances they produce, use, or filter act like a status readout on those organs. A CMP takes a snapshot of that readout from a single tube of blood.
Why your provider ordered one
A CMP shows up in a few common situations. It is a standard part of a routine checkup, where it screens your overall health and can surface a problem before symptoms appear.
Your provider may also order it to investigate a symptom — such as fatigue — that could have many causes, to check for liver disease, kidney disease, or a metabolic disorder, or to re-check a result that was abnormal before. If you take a medication that can affect your liver or kidneys, a CMP helps confirm the drug is working and not causing side effects.
What a CMP can and can’t tell you
A CMP is a wide-angle screening test, not a specific diagnosis. It is good at pointing to where a problem might be — sugar, kidneys, liver, or electrolytes — so your provider knows what to look at next.
It cannot, on its own, confirm a disease. A high glucose reading may point toward diabetes, for example, but confirming that takes additional testing and your provider’s interpretation of the whole picture. Think of the panel as the opening question, not the final answer.
CMP vs BMP vs CBC: what’s the difference?
If your order or results mention a different panel, the distinction is simple. A basic metabolic panel (BMP) includes 8 of the 14 tests in a CMP; the CMP adds 6 more that assess your liver and proteins. A complete blood count (CBC) is an entirely different test that looks at your blood cells rather than your blood chemistry.
CMP vs BMP
The CMP contains everything a BMP does, plus the liver and protein markers. Per the NIH, a BMP does not include total protein, albumin, bilirubin, or the three liver enzymes (ALP, ALT, and AST).
That difference is the whole point: if your provider wants to check your liver or your protein levels, they order the fuller CMP. If they only need blood sugar, kidney function, and electrolytes, a BMP is enough.
How a CBC is different
A CBC measures the cells in your blood — red cells, white cells, and platelets — to screen for issues like anemia, infection, and clotting problems. It does not measure glucose, kidneys, liver, or electrolytes.
Providers often order a CBC and a CMP together at a routine physical because the two tests answer different questions: the CBC covers your blood cells, the CMP covers your body chemistry.
| Panel | What it measures | Number of tests | Best for / key clinical detail |
|---|---|---|---|
| CMP (comprehensive metabolic panel) | Blood sugar, kidney markers, liver markers, proteins, electrolytes, calcium | 14 | The fullest routine chemistry screen; the only one of the three that checks liver function and proteins |
| BMP (basic metabolic panel) | Blood sugar, kidney markers, electrolytes, calcium | 8 | Blood sugar, kidney, and electrolyte check without the liver and protein tests |
| CBC (complete blood count) | Red cells, white cells, platelets | Not a chemistry panel | Screens for anemia, infection, and clotting issues — measures blood cells, not chemistry |
Panel contents per MedlinePlus, National Library of Medicine (NIH), 2023.
If you want to go deeper on the shorter chemistry panel, see our guide to what a basic metabolic panel measures; to understand the blood-cell test that’s often drawn alongside it, see how a CBC differs from a CMP.
How to read your CMP report and normal ranges
Your CMP results will list the level of each of the 14 substances measured, and once you know the layout, the page of numbers and abbreviations becomes readable. Before looking at any single value, it helps to understand the five things printed on every result line and why “normal” is defined the way it is.
The five things on every result line
Each line of your report shows the same five pieces of information:
- The test name — what was measured (for example, BUN, calcium, or ALT).
- Your result — the measured number.
- The unit — how it’s measured, such as mg/dL (milligrams per deciliter) or mEq/L.
- The reference range — the expected range for that test at that lab.
- A flag — a note (often “H” or “L”) if your value is above or below the range.
The single most useful habit when reading your report is to compare each result only to the reference range printed next to it on your report, not to a number from another lab or website.
Why “normal” ranges differ between labs
Reference ranges vary slightly from lab to lab, because each laboratory sets its ranges based on its own equipment and the population it tests. That is why the same value can be flagged at one lab and be in range at another, and why your own report’s range is the one that matters.
🔬 How It Works: A “normal range” is usually built from the middle 95% of results in a large group of healthy people. By design, that means about 1 in 20 perfectly healthy people will fall just outside the range on any given test — purely by chance. It’s one reason a single mildly out-of-range value, on its own, often turns out to be nothing.
The 14 markers at a glance
The ranges below are commonly used adult reference ranges published by the University of Rochester Medical Center. Use them only as a general guide — your lab’s ranges, printed on your own report, are the ones to compare your results against, and normal values can differ by age, sex, and lab.
| Marker | Commonly used adult reference range | What it mainly reflects |
|---|---|---|
| Glucose (fasting) | 70–99 mg/dL | Blood sugar / energy metabolism |
| BUN (blood urea nitrogen) | 8–20 mg/dL | Kidney function |
| Creatinine | 0.5–1.1 mg/dL (female); 0.7–1.3 mg/dL (male) | Kidney function |
| Sodium | 136–145 mEq/L | Fluid balance (electrolyte) |
| Potassium | 3.5–5.0 mEq/L | Nerve, muscle, and heart function (electrolyte) |
| Chloride | 98–106 mmol/L | Fluid and acid–base balance (electrolyte) |
| Carbon dioxide (bicarbonate) | 23–30 mmol/L | Acid–base balance (electrolyte) |
| Calcium | 8.6–10.2 mg/dL | Nerves, muscles, heart, bone |
| Total protein | 5.5–9.0 g/dL | Overall protein status |
| Albumin | 3.5–5.5 g/dL | Liver and nutrition status |
| ALP (alkaline phosphatase) | 30–120 IU/L | Liver and bone |
| ALT (alanine aminotransferase) | 10–40 IU/L | Liver |
| AST (aspartate aminotransferase) | 10–40 IU/L | Liver (and other tissues) |
| Total bilirubin | 0.3–1.0 mg/dL | Liver / red blood cell breakdown |
Reference ranges per University of Rochester Medical Center Health Encyclopedia (© 2000–2026); ranges vary by laboratory. For the NIH’s plain-language overview of the panel, see the National Library of Medicine’s guide to the comprehensive metabolic panel.
What a “high” or “low” flag does and doesn’t mean
A flag tells you a value sat outside the reference range — it does not tell you that you have a disease. Everyday factors like a recent meal, dehydration, exercise, or a medication can nudge a value out of range in a person who is perfectly healthy.
What your provider looks for is the pattern: which markers are off, by how much, in which direction, and whether they fit together and match your history. A borderline value on one marker is read very differently from several related markers that are clearly abnormal. The marker-by-marker sections that follow explain what each result tends to mean — always as general education, and always as one piece your provider reads alongside the rest.
What your glucose level on a CMP means
Glucose is the first number many people look for, and it’s the one tied to a specific, well-defined set of thresholds. High glucose on a CMP can point toward diabetes or prediabetes — but whether you fasted before the test changes how the number is read, and a single result is never a diagnosis on its own.
What glucose measures
Glucose is the sugar your body uses as its main source of energy, and your CMP reports the amount circulating in your blood at the moment of the draw. Your body normally holds it in a fairly narrow range using insulin and other hormones.
Because food raises blood sugar, the same value means different things depending on whether you had eaten. That is why the glucose portion of a CMP is often ordered as a fasting test.
What a high glucose result may mean
A fasting glucose result is interpreted against the standard diabetes thresholds. On a fasting sample, 70–99 mg/dL is the typical range, 100–125 mg/dL falls in the prediabetes range, and 126 mg/dL or higher on more than one occasion meets the threshold for diabetes.
📊 Clinical Data Point: The CDC and the American Diabetes Association define a fasting plasma glucose of 100–125 mg/dL as prediabetes and 126 mg/dL or higher as diabetes (confirmed on a repeat test). An A1C of 5.7–6.4% indicates prediabetes, and 6.5% or higher indicates diabetes. (Source: CDC; ADA Standards of Care in Diabetes, 2026.)
A high reading does not automatically mean diabetes. Recent food, physical or emotional stress, illness, and some medicines — such as steroids — can all raise blood sugar temporarily.
What a low glucose result may mean
A low glucose result (hypoglycemia) is less common on routine testing and can also have simple explanations, such as a long fast before the draw or certain diabetes medications. Persistent or symptomatic low readings — shakiness, sweating, confusion — are worth prompt attention.
When glucose points toward diabetes screening
If your fasting glucose lands in the prediabetes or diabetes range, the usual next step is confirmation, not conclusion. Providers typically repeat the test or add an A1C, which reflects your average blood sugar over the prior two to three months.
🩺 Physician Note: Diagnostic guidelines call for a single abnormal glucose to be confirmed — with a repeat test or a second type of test — before diabetes is diagnosed. One high reading on one panel is a reason to look closer, not a diagnosis.
✅ Patient Action: If your glucose is flagged, ask your primary care provider: “Was this a fasting sample, and do I need an A1C or a repeat glucose test to confirm what this means?” For where your everyday numbers should sit, see our guide to normal blood sugar levels explained.
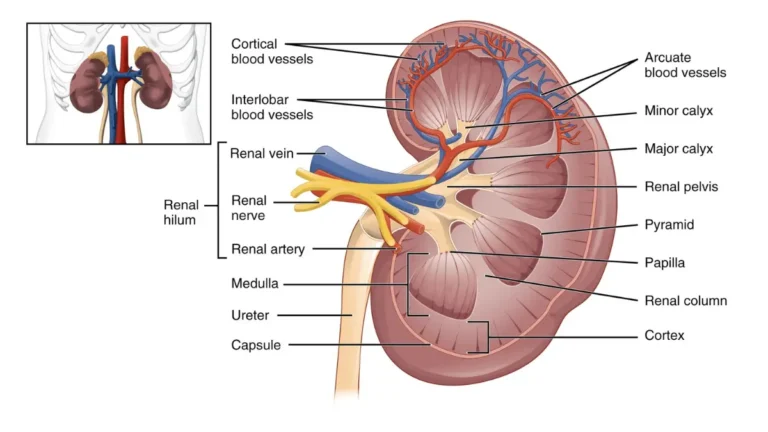
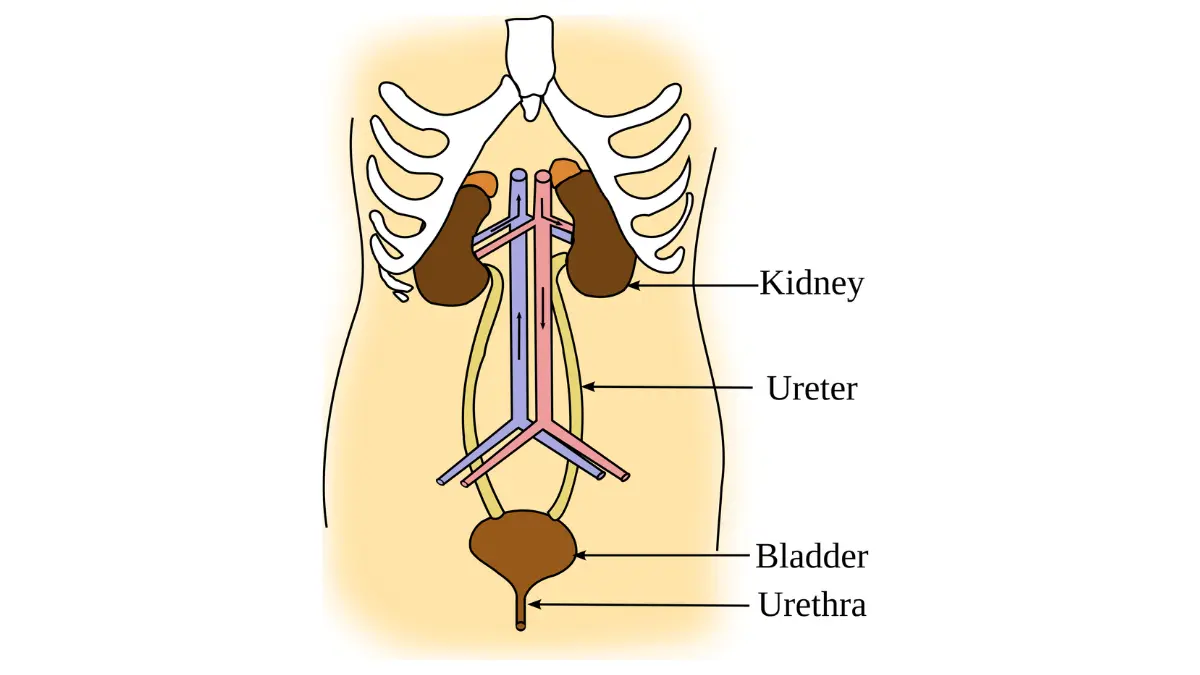
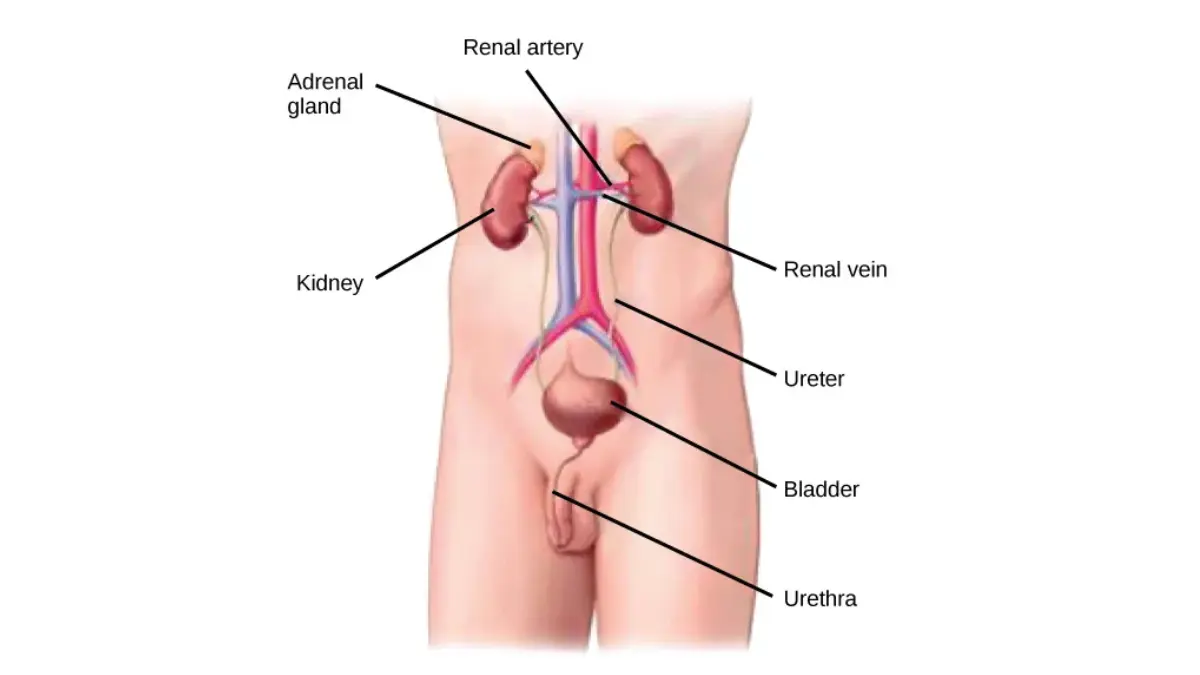
Kidney markers: BUN, creatinine and eGFR
Three of the 14 markers focus on your kidneys, the organs that filter waste from your blood. Together, BUN, creatinine, and the calculated eGFR show how well that filtering is working — though everyday factors move them too, so one high value rarely tells the whole story.
BUN — what it is and what changes it
Blood urea nitrogen (BUN) is a waste product made when your body breaks down protein, and your kidneys filter it out. A higher BUN can reflect reduced kidney filtration, but it also rises with dehydration and a high-protein diet, and can shift with certain medications.
Because so many everyday things affect it, BUN is most useful read alongside creatinine rather than alone.
Creatinine and the BUN/creatinine ratio
Creatinine is a waste product from the normal breakdown of muscle, cleared by your kidneys. As kidney function declines, creatinine in the blood tends to rise. Because it comes from muscle, normal creatinine varies with body size and muscle mass, and it can rise temporarily with dehydration or intense exercise.
Your provider may look at the BUN/creatinine ratio to help tell apart causes such as dehydration from kidney-specific problems.
🔬 How It Works: Your kidneys act as filters, pulling waste products like urea and creatinine out of your blood and passing them into your urine. When the filters slow down, those waste products build up in the blood — which is why rising BUN and creatinine can be an early signal that the kidneys are not clearing waste as efficiently.
eGFR — your kidney filtration estimate
The estimated glomerular filtration rate (eGFR) is a calculation, not a directly measured value; it is estimated from your creatinine along with your age and other factors to gauge how well your kidneys filter. A higher number is better.
📊 Clinical Data Point: According to the NIH’s kidney institute (NIDDK), an eGFR of 60 or higher is generally in the normal range, an eGFR below 60 for three months or more may indicate chronic kidney disease, and an eGFR of 15 or lower signals kidney failure. eGFR also declines naturally with age. (Source: NIDDK, National Institutes of Health.)
What an abnormal kidney panel may (and may not) mean
A single mildly reduced eGFR or a slightly high creatinine is not a diagnosis of kidney disease — dehydration alone can produce it, and eGFR falls somewhat with age. Chronic kidney disease is defined by reduced filtration that persists over months, or by other evidence of kidney damage, which is why providers look at trends and repeat testing rather than one panel.
Early kidney disease often causes no symptoms, which is part of why these markers are checked on routine panels.
✅ Patient Action: If your kidney markers are flagged, ask your primary care provider (who may refer you to a nephrologist if it persists): “Could dehydration explain this, should it be rechecked, and do I need a urine test for protein?” For a fuller walkthrough see our guide to what BUN, creatinine and eGFR reveal, and the NIH’s guide to kidney disease tests and diagnosis.
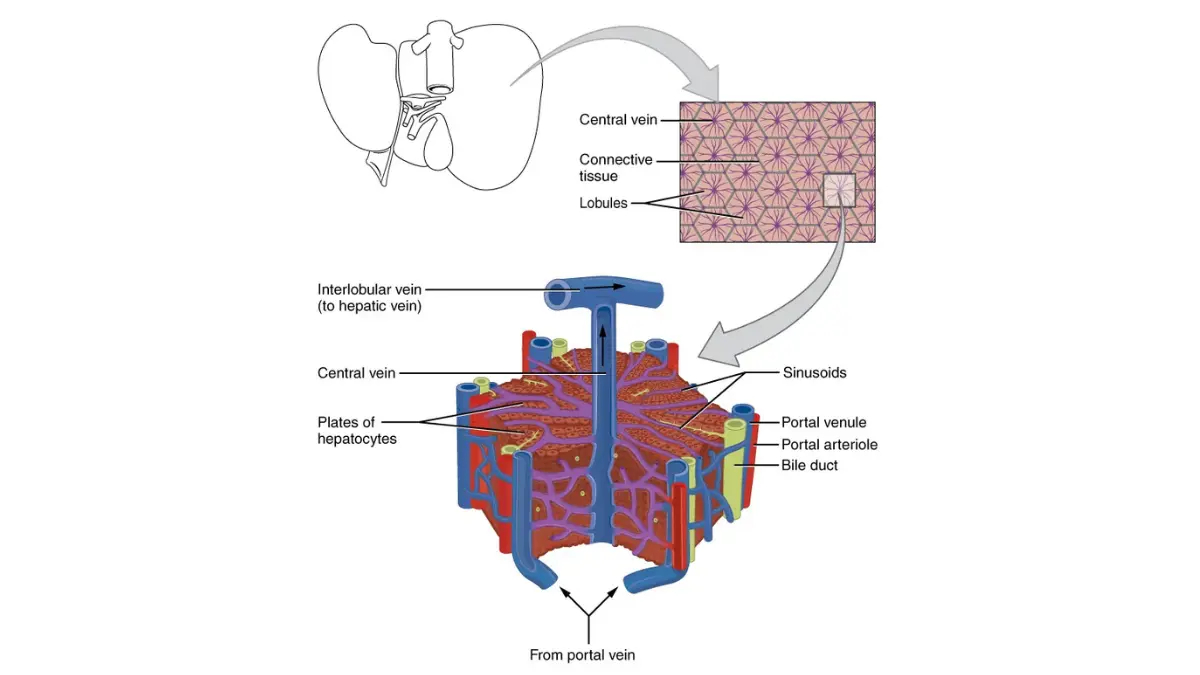
Liver markers: ALT, AST, ALP and bilirubin
Four of the panel’s markers reflect your liver. Liver enzymes — ALT, AST, and ALP — along with bilirubin can flag liver stress, but mild elevations are common and often have harmless explanations.
ALT and AST — the liver enzymes
ALT (alanine aminotransferase) and AST (aspartate aminotransferase) are enzymes released into the blood when liver cells are stressed or injured. ALT is the more liver-specific of the two; AST is also found in muscle, heart, and other tissues, so a high AST is not always about the liver.
Common, non-serious causes of mildly elevated ALT and AST include certain medications, alcohol, fatty liver, and even intense exercise before the test.
🔬 How It Works: ALT and AST mostly live inside liver cells. When those cells are inflamed or damaged, some of the enzyme leaks out into the bloodstream — so a higher blood level is a sign the liver cells are under some kind of stress, not a measure of how well the liver is functioning overall.
Alkaline phosphatase (ALP)
ALP (alkaline phosphatase) is an enzyme found in the liver’s bile ducts and also in bone. Because of that, a high ALP can come from the liver — such as a problem with bile flow — or from bone, and it is normally higher in growing children and during pregnancy.
Providers often interpret ALP together with the other liver markers to work out where it is coming from.
Bilirubin — the waste-product marker
Bilirubin is a waste product from the normal breakdown of old red blood cells; the liver processes it and clears it in bile. When bilirubin builds up, it can cause the yellowing of the skin or eyes known as jaundice.
A mildly high bilirubin is not always a problem — a common, harmless inherited condition called Gilbert’s syndrome raises it without causing disease.
🩺 Physician Note: Elevated liver disease markers are among the most common findings in routine bloodwork, and elevation alone does not mean liver damage — these enzymes come from other organs too, and the pattern across ALT, AST, ALP, and bilirubin matters more than any single value. Liver tests can also read normal in some liver disease, so results are interpreted in context.
What elevated liver values may (and may not) mean
Because everyday factors move these markers, a mild elevation on one panel is usually a reason to look again rather than a diagnosis. Providers read the pattern — which markers are up, and whether ALT and AST (pointing to liver cells) or ALP and bilirubin (pointing to bile flow) dominate — alongside your history and medications.
✅ Patient Action: If your liver markers are flagged, ask your primary care provider (or a gastroenterologist/hepatologist if it persists): “Could a medication, alcohol, or recent exercise explain this, and should these be repeated before further testing?” For detail on each enzyme, see our guide to understanding ALT, AST and liver enzymes.
Electrolytes: sodium, potassium and more
Four markers on your CMP are electrolytes — minerals that carry an electrical charge and keep your fluids, nerves, muscles, and pH in balance. An electrolyte imbalance most often comes from hydration, medications, or kidney issues rather than a rare disease.
Sodium — fluid balance
Sodium is the main electrolyte controlling your body’s fluid balance. A high sodium level (hypernatremia) is often linked to dehydration, while a low sodium level (hyponatremia) often reflects too much fluid diluting the blood.
Both extremes are usually read in the context of your hydration, medications, and other markers.
Potassium — the heart-and-muscle electrolyte
Potassium is essential for your nerves, muscles, and especially your heart. Low potassium (hypokalemia) is commonly caused by diuretics, vomiting, or diarrhea, while high potassium (hyperkalemia) can result from reduced kidney function or certain medications.
Mild potassium changes often cause no symptoms and are picked up only on testing.
⚠️ Clinical Warning: Markedly high or low potassium can affect your heart’s rhythm and is treated as urgent. If a potassium result is flagged as very high or very low — especially alongside palpitations, severe muscle weakness, or a very slow or irregular heartbeat — contact your provider or seek care promptly rather than waiting for a routine follow-up.
Chloride and CO2 (bicarbonate) — acid-base balance
Chloride and carbon dioxide (reported as bicarbonate) help manage your body’s acid–base (pH) balance. Low bicarbonate can point toward acidosis (too much acid) and high bicarbonate toward alkalosis; chloride tends to shift with fluid balance and the other electrolytes.
These two are rarely interpreted alone — they round out the picture the other electrolytes and your history provide.
When an electrolyte imbalance needs attention
Because diuretics and other medications, dehydration, and kidney function all move electrolytes, a single mildly abnormal value is often explained by something straightforward. Your provider looks at which electrolytes are off together, your medications, and your kidney markers to decide whether it matters.
✅ Patient Action: If an electrolyte is flagged, ask your primary care provider: “Could a medication I take — like a diuretic — or my hydration be causing this, and does it need rechecking?” For the bigger picture see our guides to electrolyte imbalance causes and symptoms and what causes high potassium.
Albumin, total protein and calcium explained
The remaining markers cover two blood proteins and calcium. Albumin, total protein, and calcium are read alongside the rest of the panel, because each is influenced by several body systems rather than one.
Albumin and total protein
Albumin is the main protein made by your liver; total protein measures albumin plus the other proteins in your blood. Low albumin can reflect liver disease, kidney disease (which can leak protein into urine), poor nutrition, or inflammation, so it is read in context rather than as a single answer.
Some reports also show the albumin/globulin (A/G) ratio, another way of looking at the balance between these proteins.
What low albumin may mean
Because albumin is made by the liver, a low level is one clue among several that the liver or another system may be under strain — but it is not specific to any one condition. Your provider weighs it against your liver enzymes, kidney markers, and overall picture.
Calcium — beyond bones
Calcium does far more than build bones: the small fraction in your blood is needed for your nerves, muscles, heart, and blood clotting to work. About half of your blood calcium is bound to albumin, which is why a low albumin can lower the measured total calcium and why the two are interpreted together.
🔬 How It Works: Your body holds blood calcium in a tight range using parathyroid hormone (PTH) and vitamin D, which draw calcium from food and bone as needed. When that control system is off — for example, an overactive parathyroid gland — blood calcium can drift high or low even though your bones store most of the body’s supply.
When protein or calcium values matter
A high calcium level (hypercalcemia) is most often related to an overactive parathyroid gland, and less commonly to certain cancers, excess vitamin D, or dehydration. A low calcium can relate to vitamin D deficiency, kidney problems, or parathyroid issues. As with the rest of the panel, one out-of-range value is a prompt to look further, not a diagnosis.
✅ Patient Action: If your calcium or protein is flagged, ask your primary care provider: “Does this fit anything in my history, should it be repeated, and do I need a calcium test corrected for my albumin, or a PTH test?”
What can throw off your CMP results
Before reading any value as a sign of disease, it helps to know how many ordinary things move these numbers. Food, hydration, medications, and even which lab ran the test can all nudge a result out of range in someone who is perfectly healthy — which is why an abnormal result is so often explained by something simple.
Food, fasting and hydration
Eating before the test is the most common reason a glucose result runs high, and it can affect other values too. Dehydration concentrates your blood and can raise markers like BUN, creatinine, and sodium, while overhydration can dilute them.
If you were told to fast and did not, or you were unusually dehydrated, mention it — your provider may simply repeat the test.
Medications and supplements
Many everyday medicines shift CMP values. Diuretics and corticosteroids (such as prednisone) can move your electrolytes and glucose, and a range of prescription and over-the-counter drugs, supplements, and hormones can affect the liver and kidney markers.
This is why your provider asks what you take — and why you should not stop any medication before a blood test unless your provider tells you to.
Exercise, timing and lab-to-lab variation
Intense exercise before the draw can temporarily raise muscle-related markers like AST and creatinine. Pregnancy shifts several values, and results can differ simply because a different lab with different equipment ran them.
✅ Patient Action: Since hydration moves several markers, one concrete prep step helps: arrive well-hydrated unless you were told otherwise. Our daily water intake calculator can help you gauge a reasonable target for your body size.
Reading patterns, not single numbers
This is the part that turns a page of scary numbers back into something manageable. Providers rarely react to one flagged value in isolation — they read the pattern across all 14 markers, in the context of your history, and decide what, if anything, it means.
Why one value rarely tells the story
A single mildly out-of-range result is common and frequently harmless, partly because reference ranges are built so that about 1 in 20 healthy people fall just outside them by chance. What carries meaning is several related markers moving together in a way that fits a picture.
Kidney, liver and glucose patterns
Grouped markers tell a cleaner story than any one number. BUN and creatinine rising together, with a lower eGFR, points toward kidney filtration; ALT and AST up together suggests liver-cell stress; a fasting glucose in the diabetes range with a high A1C points toward diabetes.
Even then, these are directions for your provider to investigate — not conclusions you can draw alone.
🩺 Physician Note: The single most important thing to understand about a CMP is that clinicians interpret results as a pattern, not as isolated numbers. One value slightly outside its range, with everything else normal and no symptoms, is read very differently from a cluster of related abnormalities — which is exactly why a single flag on your report is rarely a diagnosis.
What “borderline” usually means
A value sitting just outside its range is often called borderline, and it usually means “worth watching or repeating,” not “abnormal and dangerous.” Trends over time — how a number moves across several tests — tell your provider more than one snapshot.
When a pattern needs prompt follow-up
Some results do warrant quicker attention: markedly abnormal potassium, a sharply reduced eGFR, or strikingly high liver enzymes, especially alongside symptoms. If your report flags a value as critically high or low, your provider or the lab will usually reach out — but you can always call to ask.
✅ Patient Action: Bring your full report to your provider and ask: “Looking at the whole panel and my history, does anything here form a pattern, and what’s the next step?” If you’re weighing your longer-term risk for conditions these markers touch, our genetic risk assessment tool can help start that conversation.
Do you need to fast for a CMP?
If your test is coming up, this is usually the most pressing question. You may need to fast for several hours before a CMP — but not always, so the instruction your provider gives you is the one to follow.
Fasting: when and how long
When fasting is required, it is typically for 8 to 12 hours before the draw, mainly so your glucose reading is accurate. Some providers order a CMP without fasting if blood sugar is not the focus, so always go by your specific instructions.
What you can drink
Water is usually allowed and even encouraged during a fast, since being hydrated makes the blood draw easier. Avoid coffee, juice, and other drinks unless your provider says otherwise, because they can affect results.
What to expect during the blood draw
A CMP needs one small blood sample, taken from a vein in your arm with a needle, and the draw itself usually takes only a few minutes. There is very little risk — you may feel a brief sting and have slight bruising afterward, which fades quickly.
For a fuller rundown of do’s and don’ts, see our guide to fasting before a blood test.
How much a CMP costs and where to get one
If cost is your worry, the good news is that a CMP is one of the more affordable blood tests — and the price you pay depends far more on where you get it than on the test itself. The comprehensive metabolic panel is billed under a single code, and the same 14 tests can cost wildly different amounts across settings.
CMP cost with and without insurance
Without insurance, a CMP commonly runs anywhere from about $10 to $400, and direct-to-consumer labs often price it around $30 to $50. At a hospital outpatient lab, the same panel can cost several times more.
📊 Clinical Data Point: A CMP is billed under one code, CPT 80053. Without insurance, the same 14-test panel commonly ranges from roughly $10 to $400, with direct-to-consumer labs often near $30–$50 and hospital outpatient labs sometimes exceeding $1,000 — a spread driven mostly by the site of service. (Sources: Solv Health; CoveredUSA/CMS Clinical Laboratory Fee Schedule, 2026.)
| Where you get it | Typical cost without insurance | Best for / key detail |
|---|---|---|
| Direct-to-consumer / independent lab (Quest, Labcorp networks) | ~$30–$50 | Lowest cash price; the physician order is often included |
| Doctor’s office + lab | ~$150–$350+ | Bundled with a visit; visit and order fees add up |
| Urgent care + lab | ~$100–$250+ | Faster, but a visit fee applies |
| Hospital outpatient lab | ~$200–$600+ (occasionally far higher) | Usually the most expensive site of service |
Compiled from Solv Health, Personalabs, and MDsave cash-price data (2026); CMP billed under CPT 80053. Prices vary widely by location and lab.
Why the same test varies so much
The biggest driver of what you pay is the site of service — the same panel is routinely two to three times more expensive at a hospital outpatient lab than at an independent or direct-to-consumer lab. Facility fees, phlebotomy charges, and the physician’s interpretation fee can stack on top of the base lab charge.
If you are paying cash, asking for the price up front and comparing an independent lab to a hospital lab can save a large share of the cost.
Medicare and preventive coverage
Whether insurance covers a CMP depends on why it was ordered. Under Affordable Care Act rules, certain screenings — such as a diabetes or cholesterol screening for people who meet the criteria — are covered at no cost as preventive care; a full CMP, however, is often billed as diagnostic (especially when ordered to investigate a symptom or monitor a condition), which means it can apply to your deductible.
You can review the covered preventive list at HealthCare.gov’s guide to preventive care benefits, and ask whether your test is coded as preventive or diagnostic. Medicare Part B generally covers a medically necessary CMP ordered by your provider, typically at no cost when the provider accepts assignment.
Ordering your own CMP (at-home and direct-to-consumer)
Several national labs let you order a CMP yourself online, without a separate doctor’s visit, often for around $30 to $50. These use the same major lab networks your provider uses; you book a nearby draw or an at-home phlebotomy visit, and results come through a portal.
Affiliate disclosure: If you order through some of the direct-to-consumer testing links on this site, we may earn a commission at no extra cost to you. This is general education, not a recommendation to test — order lab work with guidance from your clinician, who can tell you which tests you actually need and help you interpret the results.
✅ Patient Action: Before your draw, ask: “What’s the cash price, is this billed as preventive or diagnostic, and can I get a Good Faith Estimate?” Under the No Surprises Act, if you’re uninsured or paying cash, you’re entitled to a Good Faith Estimate of costs before scheduled care. For a broader breakdown, see our guide to what blood work costs without insurance and how at-home blood testing works.
What to do if your CMP results are abnormal
If you are here because a number came back flagged, start with the calmest accurate fact available: a single out-of-range value on a CMP is usually not a diagnosis. What matters next is a short, clear plan — not a search spiral.
First: don’t panic over a single flag
One mildly abnormal marker, with the rest of your panel normal and no symptoms, is common and frequently benign. Everyday factors — food, hydration, a medication, recent exercise — explain many flags, and your provider reads the whole pattern rather than the one number.
When to call your provider promptly
Most abnormal results can wait for a routine follow-up, but some deserve a quicker call: a value flagged as critically high or low, or an abnormal result alongside real symptoms such as severe weakness, confusion, palpitations, or yellowing of the skin or eyes. When in doubt, calling your provider’s office to ask is always reasonable.
Questions to ask about your results
Walking into your appointment with the right questions turns anxiety into action. A short, specific list helps your provider give you clear answers.
- Which of my values are outside the range, and by how much?
- Could a medication I take, my hydration, or how I prepared for the test explain any of them?
- Do any of these need to be repeated, and if so, when?
- Do any results point to a condition you want to investigate further?
✅ Patient Action: Bring your full report to your primary care provider and ask the single most useful question first: “Which of these values, if any, actually need action?” To make that conversation easier, download our free CMP Results Decoder + Questions to Ask Your Doctor — a one-page guide with the 14 markers, their typical ranges, and the questions above, ready to bring to your visit.
Common questions about your CMP results
1. What is a comprehensive metabolic panel?
A comprehensive metabolic panel (CMP) is a routine blood test that measures 14 substances in your blood, giving a broad picture of your blood sugar, kidney and liver function, proteins, and electrolytes. It is one of the most common tests ordered at checkups and to help investigate symptoms or monitor conditions.
2. What does a CMP test check for?
A CMP checks five areas from one blood sample: blood sugar (glucose), kidney markers (BUN, creatinine), liver markers (ALT, AST, ALP, bilirubin), proteins (albumin, total protein), and electrolytes plus calcium (sodium, potassium, chloride, bicarbonate, calcium). Together they screen your metabolism and organ function.
3. What’s the difference between a CMP and a BMP?
A basic metabolic panel (BMP) includes 8 of the 14 tests in a CMP. The CMP adds six more — total protein, albumin, bilirubin, and the liver enzymes ALP, ALT, and AST — so it also assesses your liver and proteins, which a BMP does not.
4. Do you have to fast for a CMP?
Sometimes. When fasting is needed, it is usually for 8 to 12 hours before the draw, mainly for an accurate glucose reading, and water is generally allowed. Some CMPs are drawn without fasting, so follow the specific instructions your provider gives you.
5. How long do CMP results take?
CMP results are usually available within about one to three business days, depending on the lab. Your provider, the lab, or a patient portal will typically deliver them, with each of the 14 markers listed next to its reference range.
6. What does high glucose on a CMP mean?
A high fasting glucose can signal prediabetes (100–125 mg/dL) or diabetes (126 mg/dL or higher), but recent food, stress, illness, or medications can also raise it. One reading is not a diagnosis. Talk with your provider about whether you need an A1C or a repeat test to confirm what it means.
7. What do high ALT and AST mean?
ALT and AST are enzymes released when liver cells are stressed, so elevations can reflect the liver — but medications, alcohol, fatty liver, and even intense exercise commonly raise them, and AST also comes from muscle. Discuss any elevation with your provider, who may simply repeat the test.
8. What do high BUN or creatinine mean?
BUN and creatinine are waste products your kidneys filter, so higher levels can reflect reduced kidney function — but dehydration, a high-protein diet, and muscle mass also raise them. They are read together, and one high value often just needs rechecking. Ask your provider whether hydration could explain it.
9. What is eGFR on a CMP?
The eGFR is a calculated estimate of how well your kidneys filter, based on your creatinine, age, and other factors. An eGFR of 60 or higher is generally normal; below 60 for three months or more may indicate chronic kidney disease. Discuss a low eGFR with your provider, as it can also dip with age or dehydration.
10. What does low albumin mean?
Albumin is the main protein your liver makes, and a low level can reflect liver disease, kidney disease, poor nutrition, or inflammation. It is not specific to one condition and is read alongside your other markers. Ask your provider what your albumin means in the context of your full panel.
11. What electrolyte problems can a CMP detect?
A CMP measures sodium, potassium, chloride, and bicarbonate, so it can flag imbalances often caused by hydration, medications like diuretics, or kidney issues. Markedly abnormal potassium can affect the heart and needs prompt attention. Discuss any flagged electrolyte with your provider, especially if you take a diuretic.
12. How much does a CMP cost without insurance?
Without insurance, a CMP commonly costs about $10 to $400, with direct-to-consumer labs often around $30 to $50 and hospital outpatient labs sometimes far higher. The test is billed under CPT 80053, and the biggest cost factor is where you have the blood drawn.
13. Is a CMP covered by insurance or Medicare?
It depends on why it is ordered. Some screenings are covered at no cost as preventive care, but a full CMP is often billed as diagnostic and can apply to your deductible. Medicare Part B generally covers a medically necessary CMP ordered by your provider when the provider accepts assignment.
14. Can I get a CMP without a doctor’s order?
Yes. Several direct-to-consumer labs let you order a CMP online without a separate doctor visit, often for around $30 to $50, using the same national lab networks. You book a draw or at-home visit and get results through a portal, though your clinician is still the best person to interpret them.
15. What can affect CMP results?
Eating before the test, dehydration, certain medications and supplements, recent intense exercise, pregnancy, and even differences between labs can all shift CMP values. This is why one out-of-range result is often explained by something ordinary, and why your provider may repeat a flagged test.
16. What conditions can a CMP help detect?
A CMP can help screen for or monitor diabetes, kidney disease, liver disease, and electrolyte imbalances, and it can surface a problem before you have symptoms. It points your provider toward what to investigate rather than confirming a diagnosis on its own. Discuss any abnormal results with your provider.
Your next steps after a CMP
If you arrived at this page worried about a flagged number, you should be leaving with more clarity and a plan — not more fear. A comprehensive metabolic panel is a wide-angle snapshot of your metabolism and organ function, and the single most important thing to carry with you is that one value outside its range is rarely a diagnosis; your provider reads the whole pattern, alongside your history.
The most valuable next step is always the same conversation. Before your next appointment, write down every value on your report that sits outside its range, and ask your provider one question first: “Which of these, if any, actually need action — and could a medication I take, my hydration, or how I prepared for the test explain them?”
To make that easier, download our free CMP Results Decoder + Questions to Ask Your Doctor, a one-page guide you can bring to your visit. From here, many readers find it helpful to go deeper on what BUN, creatinine and eGFR reveal, understanding ALT, AST and liver enzymes, or what blood work costs without insurance.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.