
On This Page – Quick Medical Summary
Quick Answer: Adrenaline (also called epinephrine) is a hormone and neurotransmitter released by your adrenal glands within 3–5 seconds of a perceived threat. It triggers your fight-or-flight response — accelerating your heart, widening your airways, sharpening your senses, and flooding your muscles with energy — all before you consciously react.
What Is Adrenaline? Your Body’s Built-In Emergency System
Adrenaline is one of the most powerful chemical messengers your body produces. It works as both a hormone (released into the bloodstream) and a neurotransmitter (transmitting signals between nerve cells) — a dual role that gives it extraordinary reach across nearly every organ system.
Most people have felt it: the sudden hammering heartbeat before a car accident you barely avoided, or the electric surge before stepping on stage. That sensation is adrenaline, already at work.
Adrenaline vs. Epinephrine — Are They the Same Thing?
Yes — they are identical. The difference is purely geographic and professional convention:
| Term | Used By | Context |
|---|---|---|
| Adrenaline | UK, Australia, Europe, general public | Common medical and lay usage |
| Epinephrine | USA, clinical/pharmacological settings | FDA drug labels, hospital protocols |
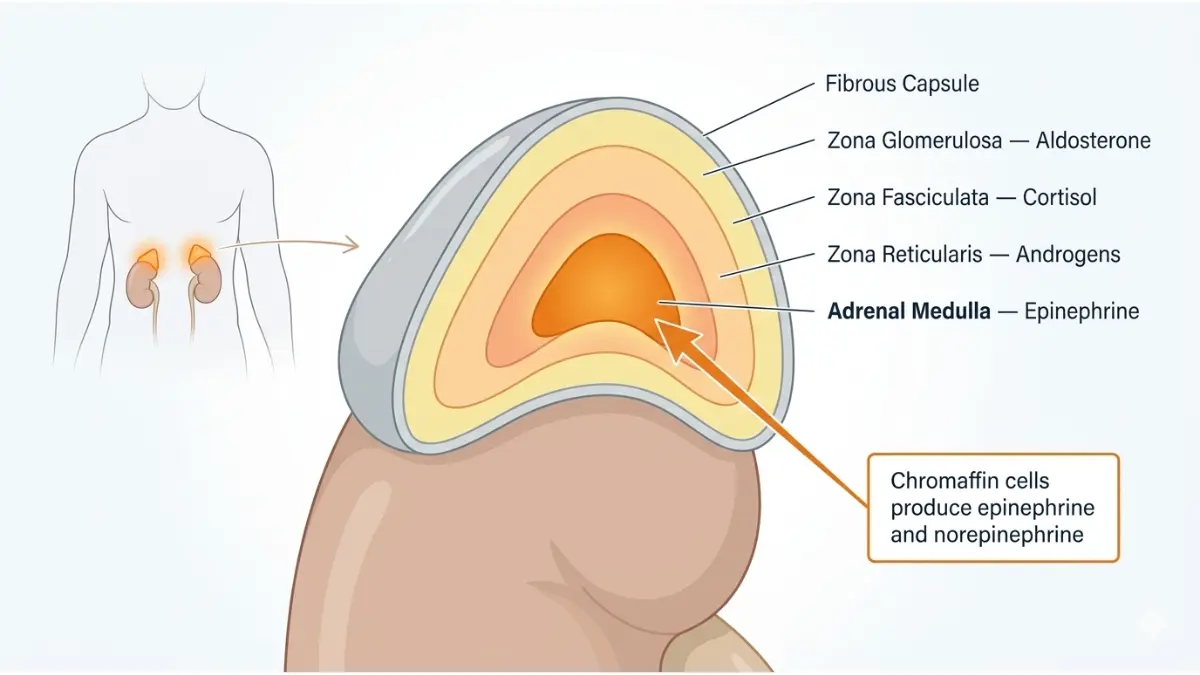
Both terms describe the exact same catecholamine hormone. According to NIH StatPearls, epinephrine is produced primarily in the adrenal medulla — the inner core of your adrenal glands, which sit like small pyramids on top of each kidney.
Is Adrenaline a Hormone or a Neurotransmitter?
Both. This is one of the most commonly misunderstood facts about adrenaline. When secreted by the adrenal glands into the bloodstream, it acts as a hormone — traveling systemically to affect distant organs. When released by certain neurons in the brain and spinal cord, it acts as a neurotransmitter — passing signals directly between nerve cells.
The adrenal medulla releases adrenaline and norepinephrine in roughly a 4:1 ratio during acute stress, per NIH catecholamine physiology research. This burst is what creates the full-body cascade you feel during an adrenaline rush.
If you’re experiencing unexplained physical symptoms like racing heart or sudden sweating, our Symptom Checker can help you identify what may be going on.
What Triggers an Adrenaline Rush? The 5-Second Body Cascade
Most people think adrenaline takes a while to kick in. It doesn’t. The cascade from threat detection to full hormonal response happens in under 8 seconds — faster than most people can finish a sentence.
James, a 41-year-old teacher from Chicago, described it perfectly: “I swerved to avoid a truck on the highway. By the time I realized what happened, my heart was already pounding out of my chest. I didn’t decide to react — my body just did it.”
That’s the adrenaline cascade at work.
The 5-Step Adrenaline Trigger Cascade
| Step | What Happens | Time |
|---|---|---|
| 1 | Amygdala (brain’s threat center) detects danger | < 1 second |
| 2 | Hypothalamus signals the sympathetic nervous system | 1–2 seconds |
| 3 | Nerve signal reaches the adrenal glands | 2–3 seconds |
| 4 | Adrenaline floods into the bloodstream | 3–5 seconds |
| 5 | Full fight-or-flight response activates body-wide | 5–8 seconds |

What Triggers This Cascade?
Physical threats:
- Sudden loud noise or collision
- Physical injury or extreme exercise
- Extreme cold or pain
Psychological triggers:
- Public speaking, interviews, competitive events
- Watching a horror film or riding a rollercoaster
- Anxiety, PTSD episodes, panic attacks
Medical triggers:
- Pheochromocytoma (adrenal tumor — covered in Section 5)
- Severe hypoglycemia (low blood sugar)
- Certain medications and stimulants
The Endocrine Society’s adrenal hormone resource confirms that both real and perceived threats activate this same cascade — which is why anxiety disorders can trigger adrenaline surges even when no actual danger is present.
Organ by Organ — Exactly What Adrenaline Does Inside You
This is what no competitor fully explains. Adrenaline doesn’t just “speed up your heart.” It simultaneously reprograms seven distinct organ systems within seconds. Here’s what’s happening inside your body right now when adrenaline hits.
Quick Reference: Adrenaline’s Effect on Every System
| Body System | Adrenaline’s Effect | Why It Happens |
|---|---|---|
| Heart | Rate increases 20–30 bpm; stronger contractions | More oxygenated blood to muscles |
| Lungs | Airways (bronchioles) widen; breathing rate rises | Maximum oxygen intake |
| Eyes | Pupils dilate; peripheral vision sharpens | Better threat detection in low light |
| Muscles | Blood flow surges; glycogen converts to glucose | Instant fuel for fighting or fleeing |
| Digestive system | Peristalsis slows or stops; blood redirected away | Energy redirected to survival systems |
| Blood sugar | Rises rapidly (glycogen breakdown in liver) | Immediate fuel for brain and muscles |
| Pain sensitivity | Decreases significantly | Injuries don’t slow your escape |

Heart & Circulation
Adrenaline binds to beta-1 adrenergic receptors on heart muscle cells, causing faster and stronger contractions. Heart rate can jump 20–30 beats per minute within seconds. Blood vessels in the skin and gut constrict, while those supplying the heart and major muscles dilate — redirecting the blood exactly where it’s needed.
Lungs & Airways
Adrenaline causes bronchodilation — the smooth muscle surrounding your airways relaxes, opening the passages wider. This is why epinephrine is the first-line emergency treatment for anaphylaxis: it immediately reverses the airway swelling that can be fatal. Breathing becomes faster and deeper to maximize oxygen delivery.
Eyes & Senses
Your pupils dilate within seconds of an adrenaline surge, allowing more light into the eye. This sharpens visual acuity — especially in dim conditions — and expands peripheral awareness. Many people report tunnel focus during intense adrenaline events, which is the brain ruthlessly prioritizing threat-relevant visual information.
Muscles
Adrenaline triggers the liver to break down glycogen into glucose, flooding the bloodstream with fast energy. Blood flow to skeletal muscles increases dramatically, delivering that glucose directly where it’s needed for explosive physical output. This is the biochemical reason people sometimes display extraordinary strength during emergencies.
Pain Sensitivity
One of the most striking effects: adrenaline significantly reduces pain perception. It does this partly through endorphin release and partly through direct effects on pain receptors. This is why soldiers or accident victims can sustain serious injuries and not feel them until after the crisis passes.
Digestion
Adrenaline essentially shuts down your digestive system during an emergency. Blood is redirected away from the stomach and intestines. Saliva decreases (causing dry mouth). Peristalsis slows or stops. The “butterflies in your stomach” sensation before a performance? That’s your gut vessels constricting as blood rushes away.
Blood Sugar
Adrenaline stimulates the pancreas to stop producing insulin while simultaneously driving glucose release from the liver. This spike in blood sugar provides rapid fuel for your brain and muscles. For people managing diabetes, frequent stress-triggered adrenaline surges can meaningfully disrupt glucose control — making stress management a clinical priority, not just a lifestyle suggestion. Use our Blood Sugar Converter to track patterns alongside your healthcare provider.
What This Means For You: Every physical symptom of an adrenaline rush — pounding heart, dry mouth, tunnel vision, shaking hands — has a precise biological purpose. Your body isn’t malfunctioning. It’s running a survival program that has kept humans alive for 300,000 years.
How Long Does Adrenaline Last — and the Memory Connection No One Talks About
How Long Does an Adrenaline Rush Last?
The hormone itself clears your bloodstream surprisingly fast. But the effects linger considerably longer.
Adrenaline Timeline After a Surge:
0–5 seconds → Adrenaline released into bloodstream
5–30 seconds → Full body-wide response (heart, lungs, muscles, eyes)
2–3 minutes → Blood adrenaline half-life — hormone begins clearing
20–60 minutes → Physical symptoms may persist (shaking, jitteriness, pallor)
1–3 hours → Full physiological baseline recovery
The lingering symptoms — trembling, fatigue, rapid heart rate — occur because your body needs time to clear the hormone metabolites and restore normal receptor sensitivity. This is completely normal.
Feeling exhausted after a stressful event or panic attack isn’t weakness — it’s your body recovering from running its emergency systems at full power. If adrenaline-related stress disrupts your sleep, our Sleep Calculator can help you optimize your recovery window.
Adrenaline and Memory — The Surprising Science Competitors Miss
Here’s something Healthline, WebMD, and Cleveland Clinic all fail to mention: adrenaline directly enhances long-term memory formation.
Research published in PMC (2024) confirms that adrenaline released during emotionally stressful events modulates memory consolidation through an indirect pathway involving the vagus nerve and the brain’s nucleus tractus solitarius (NTS). The result: memories formed during high-adrenaline moments are encoded more deeply and recalled more vividly than ordinary memories.
This is why:
- You can remember exactly where you were on a frightening day, years later
- Near-miss accidents feel “burned in” to your memory
- PTSD involves intrusive, hyperdetailed traumatic memories — adrenaline’s memory-enhancement mechanism gone pathological
What This Means For You: If you find yourself replaying a frightening event over and over, that’s partly adrenaline’s memory-enhancement biology at work. Understanding the mechanism can help reduce self-blame. If this is affecting your daily life, speaking with a mental health professional is strongly recommended. You can also explore our related guide on how to reduce anxiety naturally.
When Adrenaline Becomes Dangerous — Too Much, Too Often
Occasional adrenaline surges are normal and beneficial. But chronic excess adrenaline — whether from unrelenting stress or a medical condition — can cause serious, lasting damage.
Symptoms of Too Much Adrenaline (Chronic Stress-Driven)
When your body releases adrenaline repeatedly without resolution (as in anxiety disorders, work burnout, or PTSD), the cumulative effects include:
- Persistent high blood pressure — vessel constriction over time damages arterial walls
- Chronic insomnia — adrenaline signals your brain to stay alert, suppressing melatonin
- Heart palpitations — repeated receptor stimulation creates irregular rhythms
- Unexplained weight changes — metabolic disruption from constant glucose spikes
- Anxiety and irritability — baseline sympathetic nervous system overactivation
- Jitteriness and tremors — residual motor neuron activation
Monitor your cardiovascular baseline with our Heart Rate Zone Calculator — elevated resting heart rate is often the first measurable sign of chronic adrenaline overactivation.
Adrenaline vs. Cortisol — A Critical Comparison
Many people confuse these two stress hormones. They’re both produced by your adrenal glands, but they operate on completely different timescales and mechanisms.
| Feature | Adrenaline | Cortisol |
|---|---|---|
| Speed of release | Seconds | Minutes to hours |
| Duration of effect | Short burst (minutes) | Prolonged (hours to days) |
| Produced in | Adrenal medulla (inner) | Adrenal cortex (outer) |
| Primary trigger | Immediate physical/emotional threat | Sustained or anticipated stress |
| Main body effect | Emergency physical response | Metabolic & immune adaptation |
| Long-term risk | Cardiovascular damage, insomnia | Immune suppression, weight gain, diabetes risk |

Pheochromocytoma — When Too Much Adrenaline Has a Medical Cause
In rare cases, excess adrenaline isn’t driven by stress — it’s driven by a tumor.
A pheochromocytoma is a rare tumor of the adrenal medulla that causes the gland to produce and release excessive catecholamines, including adrenaline and norepinephrine. As confirmed by Johns Hopkins Medicine, these tumors affect men and women equally and are most commonly diagnosed in the 30s–50s. In approximately 25–35% of cases, there is a hereditary genetic component.
Red flag symptoms requiring medical evaluation:
- Episodic severe high blood pressure (sometimes uncontrolled by medication)
- Intense headaches during blood pressure spikes
- Profuse sweating without exertion
- Rapid heart rate (tachycardia) in episodes lasting 5–20 minutes
- Pallor (skin turning pale) during attacks
- Sense of impending doom during episodes
Diagnosis involves plasma-fractionated metanephrine testing (per Endocrine Society guidelines), followed by CT or MRI imaging. Treatment is surgical removal, which is typically curative.
If you have a family history of adrenal tumors or genetic syndromes like MEN2 or Von Hippel-Lindau disease, our Genetic Risk Assessment Tool can help you understand your inherited risk profile before speaking with your physician.
⚠️ When to See a Doctor Urgently: If you experience repeated episodes of severe hypertension, palpitations, and sweating without an obvious trigger — especially if they cluster in “spells” — seek medical evaluation promptly. Untreated pheochromocytoma carries serious cardiovascular risk.
How to Calm Down After an Adrenaline Rush — and How Adrenaline Saves Lives
5 Evidence-Based Techniques to Reset After an Adrenaline Surge
Once the threat passes, your body needs active help transitioning back to baseline. Here are the five most clinically supported methods:
1. Diaphragmatic Breathing (Most Effective) Deep, slow belly breaths directly stimulate the vagus nerve, activating the parasympathetic nervous system — the biological counterswitch to adrenaline’s sympathetic activation. Breathe in for 4 counts, hold for 4, exhale for 6–8 counts. Repeat for 5 minutes.
2. Cold Water on the Face or Wrists This triggers the dive reflex — a hard-wired mammalian response that slows heart rate and blood pressure within seconds. Splashing cold (not ice) water on your face is particularly effective.
3. Light Movement or Walking Adrenaline prepares your body to move — so moving burns off the glucose and hormones it released. A 5–10 minute slow walk helps clear adrenaline metabolites faster than sitting still, which often prolongs the jittery aftermath.
4. Progressive Muscle Relaxation Deliberately tensing and releasing each muscle group from feet to face counteracts the tension adrenaline loads into your musculature. This technique has Level A evidence for anxiety and stress response management.
5. Grounding (5-4-3-2-1 Sensory Method) Name 5 things you see, 4 you can touch, 3 you hear, 2 you smell, 1 you taste. This technique anchors your brain back to the present moment, reducing amygdala arousal that sustains the adrenaline loop.
For ongoing anxiety management strategies, see our comprehensive guide on how to reduce anxiety naturally, and explore our BCAA guide if you’re curious how exercise-related hormones interact with stress recovery.
Adrenaline as a Life-Saving Medication
Synthetic epinephrine is one of medicine’s most essential drugs. According to the FDA-approved Adrenalin prescribing information via DailyMed, epinephrine is indicated for:
| Medical Use | How It Works | Delivery Method |
|---|---|---|
| Anaphylaxis (severe allergic reaction) | Reverses airway swelling, raises blood pressure | EpiPen/autoinjector — 0.3mg IM into outer thigh |
| Cardiac arrest (CPR) | Stimulates heart muscle contractions | 1mg IV bolus per ACLS protocol |
| Septic shock | Raises dangerously low blood pressure | Continuous IV infusion in ICU |
| Eye surgery | Maintains pupil dilation | Direct ophthalmic application |
2024 FDA Update: The FDA approved Neffy — an epinephrine nasal spray — as a new non-injection delivery option for anaphylaxis, making emergency adrenaline accessible without needles. This is particularly significant for people with needle phobia or in situations where autoinjectors aren’t available.
If you carry an EpiPen:
- Always inject into the outer thigh (vastus lateralis muscle) — never the buttock
- After use, go to the nearest emergency room immediately, even if symptoms improve
- Effects begin within 1–5 minutes; a second dose may be given after 5–10 minutes if needed
Frequently Asked Questions About Adrenaline
1. What exactly does adrenaline do to your body?
Adrenaline triggers your fight-or-flight response — speeding your heart rate, widening airways, dilating pupils, boosting blood sugar, redirecting blood to muscles, and reducing pain sensitivity, all within seconds of a perceived threat.
2. Is adrenaline a hormone or a neurotransmitter?
Both. It acts as a hormone when released by the adrenal glands into the bloodstream, and as a neurotransmitter when used by neurons in the central nervous system to transmit signals.
3. What triggers an adrenaline rush?
Physical threats (injury, near-accidents), psychological triggers (fear, excitement, anxiety), extreme exercise, and certain medical conditions like pheochromocytoma can all trigger adrenaline release.
4. How long does an adrenaline rush last?
Adrenaline clears from the blood within 2–3 minutes (half-life), but physical symptoms — shaking, elevated heart rate, jitteriness — can persist for 20–60 minutes. Full physiological recovery typically takes 1–3 hours.
5. What does too much adrenaline feel like?
Chronic excess adrenaline causes high blood pressure, insomnia, palpitations, anxiety, tremors, and unexplained weight changes. Episodic severe surges may indicate a medical condition like pheochromocytoma.
6. What’s the difference between adrenaline and cortisol?
Adrenaline is fast-acting (seconds), short-lived, and triggers immediate physical emergency response. Cortisol is slower (minutes to hours), longer-lasting, and drives metabolic and immune adaptation to sustained stress.
7. Can adrenaline affect your memory?
Yes. Research shows adrenaline enhances long-term memory consolidation for emotionally significant events via the vagus nerve pathway — which is why frightening experiences are recalled more vividly than ordinary ones.
8. How do you calm down after an adrenaline rush?
The five most effective methods are diaphragmatic breathing, cold water on the face, light walking, progressive muscle relaxation, and the 5-4-3-2-1 sensory grounding technique.
9. Can too much adrenaline be dangerous?
Yes. Chronic adrenaline excess damages blood vessel walls, raises cardiovascular disease risk, disrupts sleep, and contributes to anxiety disorders. Rare adrenal tumors (pheochromocytoma) can cause life-threatening adrenaline overproduction.
10. What is adrenaline used for medically?
Epinephrine (adrenaline) is used to treat anaphylaxis, cardiac arrest, and septic shock. The 2024 FDA-approved Neffy nasal spray provides a needle-free option for emergency anaphylaxis treatment.
11. Is “adrenaline deficiency” a real condition?
Rarely. Even people who’ve lost both adrenal glands retain adrenaline-like function because 90% of the body’s norepinephrine (which performs similar roles) comes from the nervous system — not the adrenal glands. True isolated adrenaline deficiency is exceedingly rare and typically involves genetic enzyme disorders.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.