On This Page – Quick Medical Summary
You opened your patient portal, saw your CBC with differential results, and one line is flagged high or low — which is probably why you’re here. This guide walks through all five white blood cell types, what a normal range looks like, and what a high or low value in each one can and can’t tell you.
Where you go next depends on your situation. If you’re holding a printout with one flagged value, jump to that cell type — each has its own plain-language section below. If your neutrophils are low, or you’re receiving chemotherapy, the neutropenia section covers the numbers that matter most. If you’re getting ready for an appointment, the FAQ and the closing questions-to-ask list will help you walk in prepared.
One value slightly outside the range is often not dangerous, and this guide shows exactly what would make a result worth urgent attention. For the wider picture, see how to read your CBC results step by step and the full complete blood count overview.
ℹ️ Medical Disclaimer: This article is general health education, not a diagnosis, treatment plan, or medication advice. Interpreting a real blood result — and deciding on any testing, treatment, or precaution — depends on your symptoms, history, and other labs, so review your specific results with a licensed physician or the clinician who ordered the test. If your counts point to a possible blood disorder, ask for a referral to a hematologist.
The 5 white blood cell types your differential measures
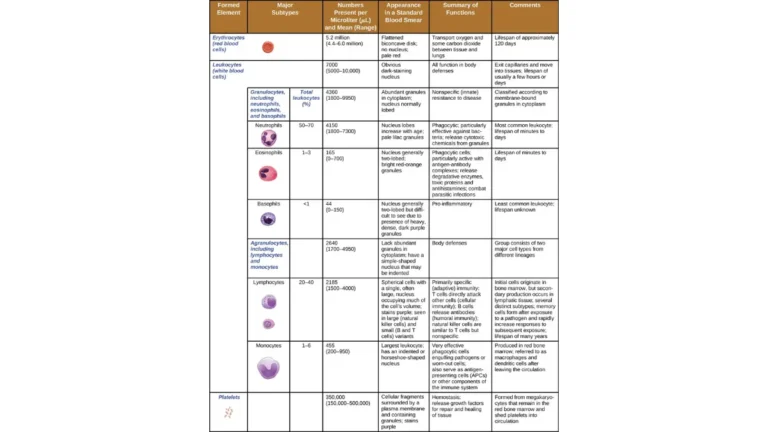
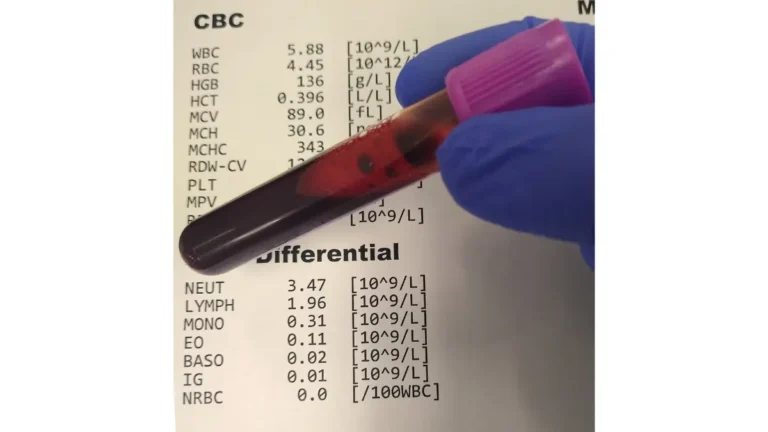
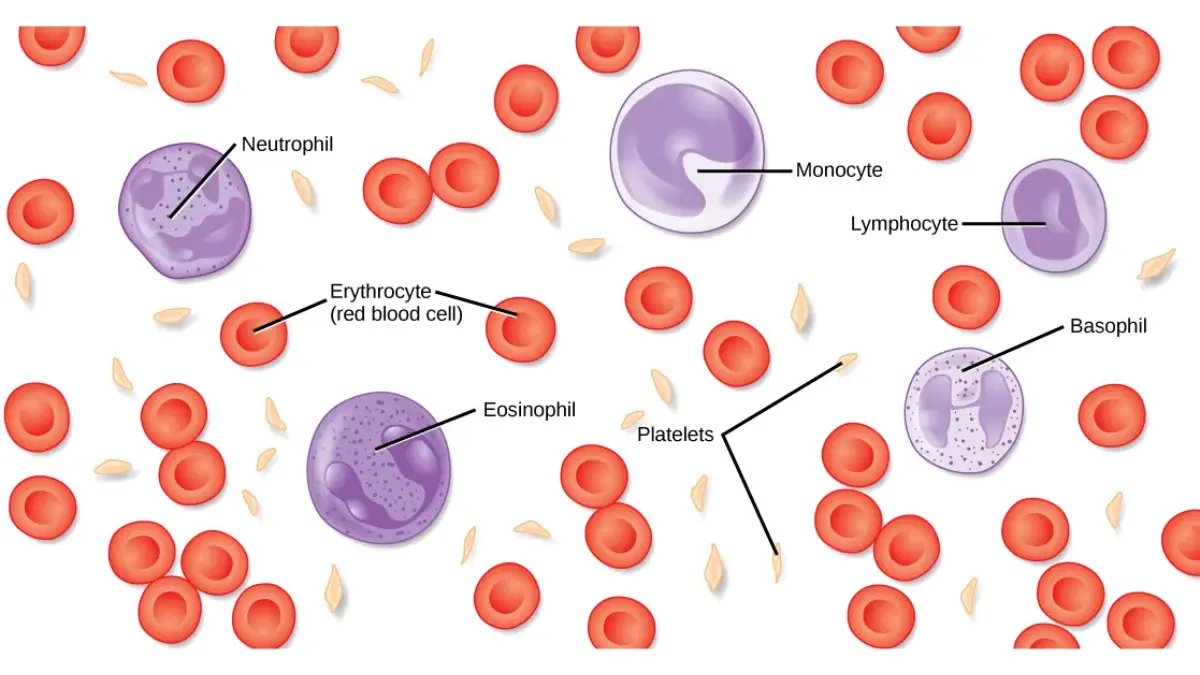
A CBC with differential measures the amount of each of the five white blood cell types your body uses to fight illness. Knowing what each one does makes every “high” or “low” flag easier to read.
Neutrophils, lymphocytes, and monocytes (the big three)
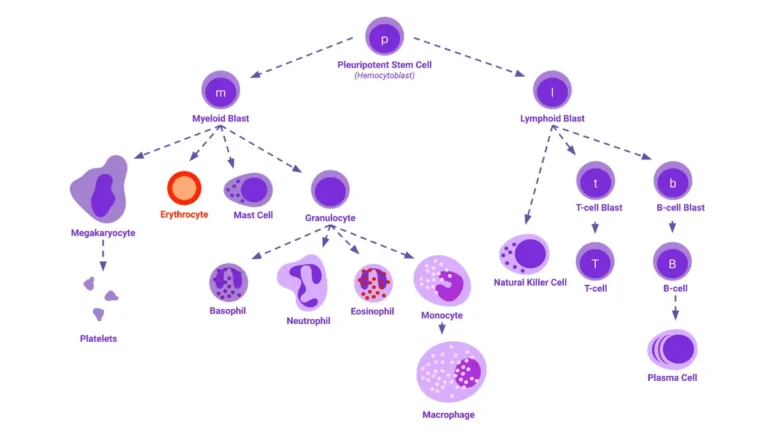
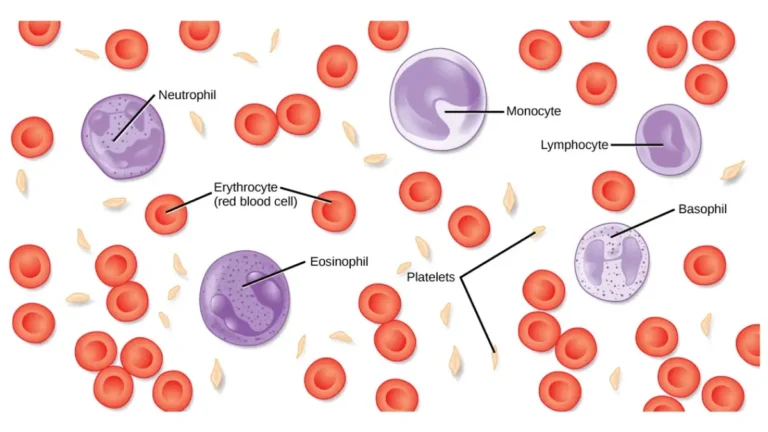
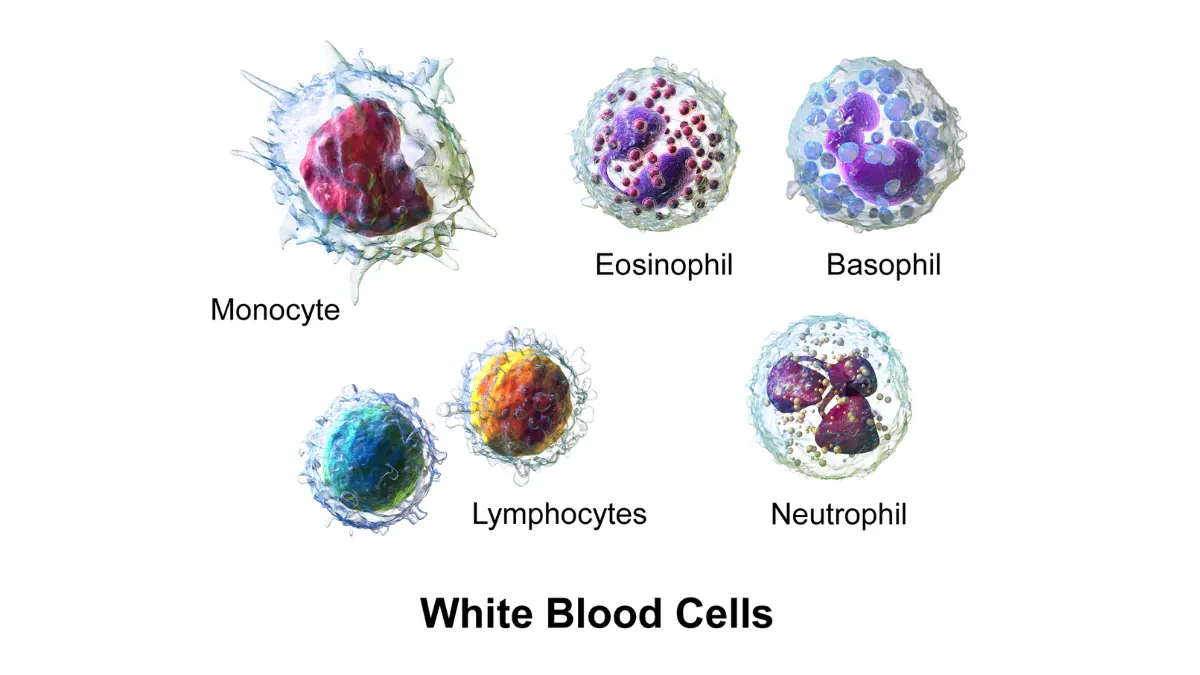
Neutrophils are the most common white blood cell and your body’s main defense against bacterial and fungal infection. Lymphocytes — which include B cells and T cells — mainly target viral infections and help your immune system remember past ones. Monocytes clear bacteria, viruses, and dead cells, and help alert other immune cells to a threat.
Eosinophils and basophils (the specialists)
Eosinophils defend against parasites and are involved in allergic reactions and inflammation. Basophils release enzymes during allergic reactions and asthma. These two are the least numerous, so small shifts can look dramatic as a percentage even when the actual change is minor.
🔬 How It Works: A lab machine (or a technician reading a stained smear) sorts your white cells into these five types and reports each as a percentage of the total and as an absolute number. Doctors group them as granulocytes (neutrophils, eosinophils, basophils) and non-granulocytes (lymphocytes, monocytes) based on how they look under a microscope.
The differential is only one part of the CBC, which also reports red blood cells, hemoglobin, and your platelet count. You can read the government reference on the five white blood cell types and what they do for more detail.
Normal CBC differential ranges (and % vs absolute)
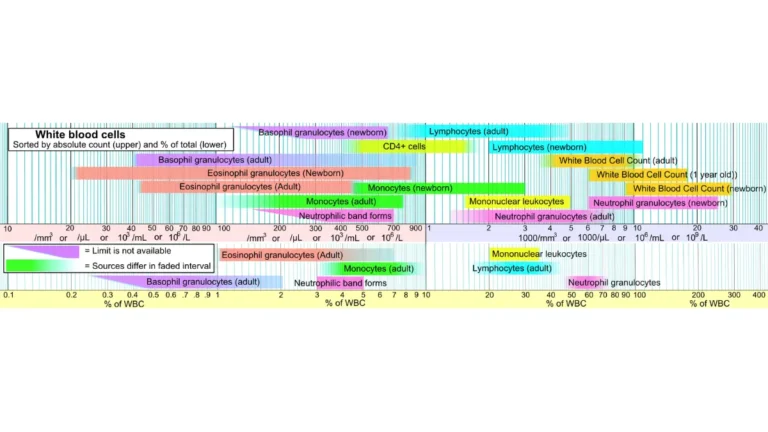
Reference ranges are the numbers your lab prints next to your result, and they vary slightly between labs. The values below are the commonly used adult ranges — always read yours against your own lab’s printed range.
| White cell type | Typical share of WBCs | What it mainly does |
|---|---|---|
| Neutrophils | 40–60% | First responders to bacterial/fungal infection |
| Lymphocytes | 20–40% | Target viral infections (B and T cells) |
| Monocytes | 2–8% | Clear debris; alert other immune cells |
| Eosinophils | 1–4% | Parasites, allergies, inflammation |
| Basophils | 0.5–1% | Allergic reactions and asthma |
| Bands (young neutrophils) | 0–3% | Immature neutrophils |
Source note: adult reference percentages per NIH MedlinePlus (Blood differential test). Ranges are lab-specific.
📊 Clinical Data Point: In absolute numbers, a normal neutrophil count runs about 1,500–8,000 cells/µL, and monocytes about 200–1,000 cells/µL — Source: NIH/NCBI StatPearls (Normal and Abnormal CBC With Differential, 2024). Total white cells normally run 4,500–11,000 cells/µL (NIH MedlinePlus).
Absolute count vs percentage — why it matters
Your absolute count multiplies the total white cell count by each type’s percentage, and it is usually more meaningful than the percentage alone. That is because percentages always add up to 100, so a “low” percentage of one cell can simply reflect a “high” percentage of another rather than a real drop.
🩺 Physician Note: A common point of confusion is a flagged percentage that isn’t actually a problem. Clinicians generally watch the absolute number — especially the absolute neutrophil count — because it reflects the true quantity of cells, not just their share.
For the other blood cells on your report, a full CBC normal range chart lays out red cells, hemoglobin, and platelets. The government tables for normal differential reference ranges and the reference intervals for each white cell type are worth bookmarking.
What high neutrophils and a “left shift” can mean
A high neutrophil count, called neutrophilia, is one of the most commonly flagged lines — and most of the time the cause is not serious. Neutrophils rise with infection, inflammation, physical stress, or certain medications, and even a hard workout or acute stress can nudge the total white count up.
Common reasons neutrophils run high
The usual drivers are a bacterial infection, inflammation from an injury or illness, recent surgery, smoking, pregnancy, or medications such as corticosteroids. Because so many everyday things raise neutrophils, a single high reading usually prompts your clinician to look at your symptoms and repeat the test rather than to assume something rare.
What “left shift” and band cells mean
If your report mentions a left shift or bands, that means immature neutrophils have appeared in your blood — cells that are normally kept in the bone marrow.
🔬 How It Works: When demand for neutrophils spikes (often during infection), the marrow releases younger cells called bands before they fully mature. Seeing them is a sign the marrow is working hard, not a diagnosis on its own.
Rarely, abnormal or truly immature cells can point to a bone marrow problem such as leukemia — but this is exactly the kind of pattern a doctor evaluates with further testing, and one result does not confirm it. If your total white count is the flagged value, a high white blood cell count covers the broader causes.
✅ Patient Action: If your neutrophils are flagged high with a note about bands or a left shift, ask your primary care physician: “Given my symptoms, does this look like infection, inflammation, or stress — and should we repeat the CBC to see if it settles?”
What high or low lymphocytes, monocytes, eosinophils, and basophils suggest
Once you have interpreted the neutrophil line, the other four cell types follow the same “high can suggest / low can suggest” logic. None of these values diagnoses a condition by itself.
Lymphocytes
A high lymphocyte count (lymphocytosis) most often reflects a viral infection, and it usually settles as you recover. Some blood cancers such as leukemia and lymphoma can also raise it, which is why a persistent, unexplained rise is followed up. A low count (lymphopenia) is seen with some infections, immune suppression, and certain treatments.
Monocytes and eosinophils
A high monocyte count (monocytosis) can follow viral or parasitic infection, tuberculosis, autoimmune conditions such as inflammatory bowel disease or lupus, and — less commonly — bone marrow disorders. A high eosinophil count (eosinophilia) most often points to allergies, asthma, or a parasitic infection.
Basophils
Basophils are the rarest white cell, and a mildly high value often traces to allergic or inflammatory conditions. A persistent, clear rise (basophilia) is sometimes evaluated for a bone marrow condition, so it is followed up rather than assumed benign. As with every value here, your doctor reads the number alongside your symptoms, history, and the rest of the CBC — a single flag is a prompt for context, not a conclusion.
Low neutrophils (neutropenia): the numbers that matter
Low neutrophils — a condition called neutropenia — is the one differential finding that can carry real urgency, because neutrophils are your front line against infection. This section explains the thresholds so you can understand your report; the specific precautions and any treatment are decisions for your care team, not something to manage on your own.
Mild, moderate, and severe neutropenia
Neutropenia is generally defined as an absolute neutrophil count below 1,500 cells/µL, and severity is graded by how far it drops.
📊 Clinical Data Point: Mild neutropenia is an ANC of about 1,000–1,500 cells/µL; moderate is 500–1,000 cells/µL; and severe is below 500 cells/µL, where infection risk rises sharply — Source: Cleveland Clinic, corroborated by Yale Medicine, NIH, and the American Cancer Society. About half of people receiving chemotherapy develop neutropenia, typically with counts lowest around 7–14 days after a cycle (Cleveland Clinic; American Cancer Society).
When low neutrophils are an emergency
Typically it is severe neutropenia that raises the risk of dangerous infection, and the key warning sign is fever.
⚠️ Clinical Warning: A fever in someone with severe neutropenia — known as febrile neutropenia — is a medical emergency, because the body may not be able to contain an infection. If you have a known low neutrophil count and develop a fever, contact your care team immediately or seek emergency care; do not wait to see if it passes.
If your total white count is low rather than your neutrophils specifically, a low white blood cell count explains the range of causes, and neutropenia goes deeper on living with a low count. The American Cancer Society’s guidance on low neutrophil counts and infection risk is a trustworthy patient resource.
✅ Patient Action: If your ANC is low, ask the clinician who ordered the test (or your oncology team, if you’re in treatment): “What is my ANC today, what precautions should I take, and exactly which symptoms mean I should seek emergency care?”
When to worry about your CBC differential — and what to ask
Most abnormal differential results are not emergencies, and knowing which ones warrant a prompt call helps you act without panicking. The pattern doctors watch is not a single mild flag but a large change, or one that persists on repeat testing.
Results that usually aren’t urgent
A value that sits just outside the range, especially right after an illness, is frequently not significant. Recent infection, physical or emotional stress, pregnancy, menstruation, dehydration, and some medications can all shift counts temporarily, which is why a repeat test often tells the real story.
Results that need prompt or emergency attention
A markedly high or low value, a result that stays abnormal on repeat, or an abnormal count paired with symptoms deserves prompt medical contact. And the one clear emergency from the section above still holds: a fever with a known severely low neutrophil count needs care right away. If you have symptoms alongside an abnormal count, you can check your symptoms to help organize what to tell your clinician.
✅ Patient Action: Bring your printout to your primary care clinician and ask: “Could this be from a recent illness or medication? Should we repeat the CBC? Do my symptoms change what this means? And do I need a referral to a specialist?”
Frequently asked questions
1. What are the 5 types of white blood cells in a CBC differential?
A CBC with differential measures neutrophils, lymphocytes, monocytes, eosinophils, and basophils. Neutrophils fight bacteria, lymphocytes target viruses, monocytes clear debris, eosinophils handle parasites and allergies, and basophils act in allergic reactions. Together they show how your immune system is responding.
2. What is a normal CBC differential?
In adults, neutrophils typically make up 40–60% of white cells, lymphocytes 20–40%, monocytes 2–8%, eosinophils 1–4%, and basophils 0.5–1%. Absolute counts matter more than percentages, and every lab prints its own reference range, so compare your result to the range on your own report.
3. What does it mean if your neutrophils are high?
A high neutrophil count (neutrophilia) most often reflects a bacterial infection, inflammation, physical stress, smoking, pregnancy, or medications such as steroids. A single high value is usually not serious and often settles on repeat testing. Discuss a persistent or unexplained rise with your clinician.
4. What does a low neutrophil count mean?
A low neutrophil count is called neutropenia, defined as an absolute neutrophil count below 1,500 cells/µL; below 500 is severe and carries higher infection risk. A fever with severe neutropenia is an emergency. If your count is low, ask your care team what precautions and follow-up you need.
5. What do high lymphocytes indicate?
A high lymphocyte count (lymphocytosis) most commonly reflects a viral infection and usually resolves as you recover. Less often, blood cancers such as leukemia or lymphoma can raise it, which is why a persistent, unexplained increase is investigated. Talk with your clinician about a lymphocyte count that stays high.
6. What’s the difference between absolute and percentage counts?
The percentage is each cell type’s share of your total white cells, while the absolute count is the actual number per microliter. Because percentages always total 100, a low percentage of one cell can just mean a high percentage of another. Doctors generally rely on the absolute count.
7. What do high eosinophils mean?
A high eosinophil count (eosinophilia) most often points to allergies, asthma, or a parasitic infection. Eosinophils are normally a small share of white cells, so even modest rises can stand out on a report. A persistent elevation should be reviewed with your clinician.
8. What does a “left shift” mean on a blood test?
A left shift means immature neutrophils (bands) have appeared in your blood, which are normally kept in the bone marrow. It usually signals that the marrow is releasing cells quickly, often during an infection. It is a clue your doctor interprets with the rest of your results, not a diagnosis.
9. Can a CBC with differential detect leukemia?
A CBC with differential can flag patterns — very high or low counts, or abnormal and immature cells — that prompt further testing for conditions like leukemia. It does not diagnose leukemia on its own; that requires additional tests such as a blood smear or bone marrow exam. Discuss any abnormal result with your clinician.
10. What causes high monocytes?
A high monocyte count (monocytosis) can follow viral or parasitic infections, tuberculosis, and autoimmune conditions such as inflammatory bowel disease or lupus, and less commonly a bone marrow disorder. As with other white cells, one elevated value is read in context. Ask your clinician whether a persistent rise needs follow-up.
11. When should I worry about my CBC differential results?
A single value slightly outside the range, especially after an illness, is often not significant. A markedly abnormal result, one that persists on repeat testing, or an abnormal count with symptoms warrants prompt medical contact. A fever with a known severely low neutrophil count is an emergency — seek care immediately.
The bottom line on your CBC differential
A CBC with differential is a window into how your immune system is responding, but no single flagged value tells the whole story. Read each result against your own lab’s range, remember that the absolute count usually matters more than the percentage, and treat low neutrophils as the one finding to take seriously — especially if a fever appears.
The most useful next step is to bring your printout to the clinician who ordered it and ask the specific questions above. If you’d like a quick reference, download our one-page “Understanding Your CBC Differential” summary, or read the full complete blood count overview to see how the differential fits with the rest of your results.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.