
On This Page – Quick Medical Summary
Adrenaline — also called epinephrine — is a hormone and neurotransmitter produced by your adrenal glands. It is the primary chemical responsible for your body’s fight-or-flight response, triggering rapid physical changes within seconds of a perceived threat. Understanding what adrenaline does, when it becomes harmful, and how to manage it is essential for anyone dealing with chronic stress, anxiety, or unexplained physical symptoms.
What Is Adrenaline (Epinephrine) and Where Does It Come From?
Adrenaline vs. Epinephrine — Same Hormone, Two Names
Many patients ask: “Is adrenaline the same as epinephrine?” The answer is yes — completely.
Adrenaline is the British Approved Name (BAN), used widely in the UK, Australia, and Canada. Epinephrine is the International Nonproprietary Name (INN), standard in the United States. Both words describe the exact same molecule. When your ER doctor injects “epi,” and when a skydiver feels an “adrenaline rush,” they are talking about the same hormone.
Is Adrenaline a Hormone or a Neurotransmitter?
Both — and that’s what makes it uniquely powerful.
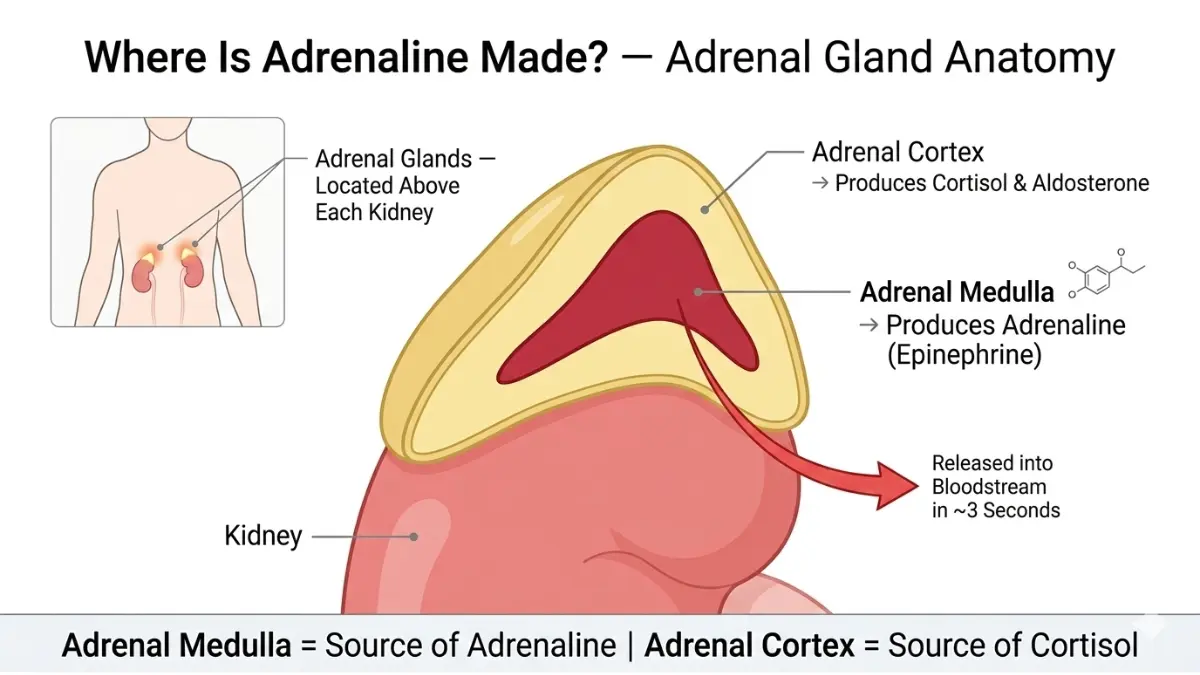
As a hormone, adrenaline is made in the adrenal medulla (the inner part of your adrenal glands, which sit atop each kidney) and released directly into your bloodstream. As a neurotransmitter, small amounts are produced in neurons of the central nervous system, where it transmits signals between nerve cells.
According to StatPearls at the National Center for Biotechnology Information (NCBI), adrenaline belongs to a class of molecules called catecholamines — the same family as norepinephrine (noradrenaline) and dopamine.
Quick-Reference Comparison: Adrenaline vs. Norepinephrine vs. Cortisol
| Hormone | Produced In | Releases Within | Duration of Effect | Primary Role |
|---|---|---|---|---|
| Adrenaline | Adrenal medulla | Seconds | 20–60 minutes | Immediate fight-or-flight |
| Norepinephrine | Nerve endings + adrenal medulla | Seconds | 20–40 minutes | Sustained alertness, blood pressure |
| Cortisol | Adrenal cortex | 2–5 minutes | Hours | Prolonged stress, metabolism |
Key Takeaway: Adrenaline is your body’s fastest emergency signal — it fires in seconds and affects virtually every organ simultaneously.
What Does Adrenaline Actually Do to Your Body?
The 90-Second Cascade — From Brain to Body
When your brain detects a threat — real or perceived — a specific sequence fires:
- Your amygdala (the brain’s threat detector) sends an alarm signal
- The hypothalamus activates your sympathetic nervous system
- Signals travel through your autonomic nerves to the adrenal glands
- Adrenaline floods your bloodstream within 2–3 seconds
- Every organ that has adrenergic receptors changes its behaviour instantly
As Harvard Health Publishing explains, this cascade happens so fast that your body reacts to danger before your conscious mind has fully registered it.
Heart, Lungs, Blood Vessels: The Immediate Response
- Heart: Beats faster and harder, pushing blood to muscles
- Lungs: Airways dilate, allowing more oxygen per breath
- Blood vessels: Constrict in the skin and gut; dilate in muscles
- Liver: Rapidly releases stored glucose into the bloodstream for instant energy
- Blood: Clotting speed increases (in case of injury)
If you’ve ever experienced your heart pounding before a job interview or public speech, that is adrenaline — triggered not by physical danger, but by perceived psychological threat.
Eyes, Muscles, and the Pain Factor
- Pupils dilate to improve peripheral vision
- Muscle fibres receive increased blood flow for strength and speed
- Pain perception drops — adrenaline blunts pain signals, which is why athletes can continue performing through injuries they don’t notice until after the game
To understand how your heart responds during adrenaline surges, our Heart Rate Zone Calculator can help you identify your personal physiological thresholds during stress or exercise.
Alpha and Beta Receptors — The Mechanism Competitors Skip
Adrenaline doesn’t just “flood your body.” It docks onto specific receptor types, producing different effects depending on the receptor:
| Receptor Type | Location | Adrenaline Effect |
|---|---|---|
| Alpha-1 (α1) | Blood vessels | Vasoconstriction (raises blood pressure) |
| Alpha-2 (α2) | Pancreas | Suppresses insulin release |
| Beta-1 (β1) | Heart | Increases heart rate and force |
| Beta-2 (β2) | Lungs, airways | Bronchodilation (opens airways) |
| Beta-3 (β3) | Fat tissue | Stimulates fat breakdown |
This is precisely why beta-blocker medications (like propranolol) reduce stage fright — they block β1 receptors, preventing adrenaline from speeding up the heart without blocking adrenaline production itself.

What Triggers an Adrenaline Rush — and What Does It Feel Like?
Common Triggers: Real Danger vs. Perceived Threat
Your adrenal glands cannot distinguish between a charging bear and a difficult conversation with your boss. Any threat — physical or psychological — triggers the same response.
| Real Physical Triggers | Psychological / Perceived Triggers |
|---|---|
| Car accident, fall, injury | Work deadline or presentation |
| Sudden loud noise | Argument or conflict |
| Extreme cold or heat | Watching a horror film |
| Intense physical exercise | Checking social media after a post |
| Allergic reaction onset | Replaying a stressful memory at night |
Adrenaline Rush Symptoms — What Your Body Is Signaling
When an adrenaline rush occurs, most people report:
- Pounding or racing heartbeat (palpitations)
- Rapid, shallow breathing
- Trembling hands or shaky legs
- Sweating, particularly on the palms and forehead
- Dilated pupils and heightened visual sharpness
- Dry mouth
- Surge of physical energy or restlessness
- Reduced ability to feel pain
These symptoms typically peak within 1–3 minutes and can persist for 20–60 minutes after the trigger passes, as adrenaline is gradually metabolised.
If these symptoms recur frequently without a clear trigger, use our Symptom Checker to help identify patterns before speaking with your doctor.
How Long Does Adrenaline Last in Your System?
The adrenaline molecule itself has a very short half-life — approximately 2–3 minutes in the bloodstream. However, the physiological effects (racing heart, heightened alertness, dilated pupils) can last 20 to 60 minutes, because downstream processes — including norepinephrine activity and elevated blood glucose — continue well after the initial adrenaline surge.
Why Does Adrenaline Spike at Night?
This is one of the most-asked questions on health forums — and one that no competitor covers with any depth.
Here’s what happens: When you lie down in a quiet, dark room, your brain is no longer distracted by external input. Unresolved stress, anxiety, and replayed memories activate your amygdala. Your hypothalamus responds as though a genuine threat exists, triggering an adrenaline release with no physical outlet for the resulting energy.
The result: racing heart, inability to sleep, restlessness, and heightened anxiety — a clinical pattern that reinforces the stress cycle. Disrupted sleep from nighttime adrenaline surges compounds stress hormone dysregulation. Our Sleep Calculator can help you assess how much sleep debt you may be accumulating as a result.
If you’re experiencing persistent anxiety related to these hormonal patterns, our guide on how to reduce anxiety naturally provides evidence-based strategies.
What This Means For You: If you regularly feel wired at bedtime with no clear reason, your body may be triggering adrenaline responses to psychological stress. This is treatable and manageable — see Section 6.
What Happens When Your Body Produces Too Much Adrenaline?
Signs of Chronic Adrenaline Overload
Occasional adrenaline surges are protective. Chronic elevation — common in people with anxiety disorders, high-stress jobs, or PTSD — is damaging.
Symptoms of chronic adrenaline excess include:
- Persistent heart palpitations at rest
- Frequent headaches and dizziness
- Unexplained weight loss despite normal eating
- Chronic insomnia or broken sleep
- Constant feeling of being “on edge” or unable to relax
- Excessive sweating without exertion
- Recurrent anxiety or panic attacks
According to Mayo Clinic’s evidence-based stress research, long-term activation of the stress response system disrupts almost all of the body’s processes, including cardiovascular, immune, and metabolic function.
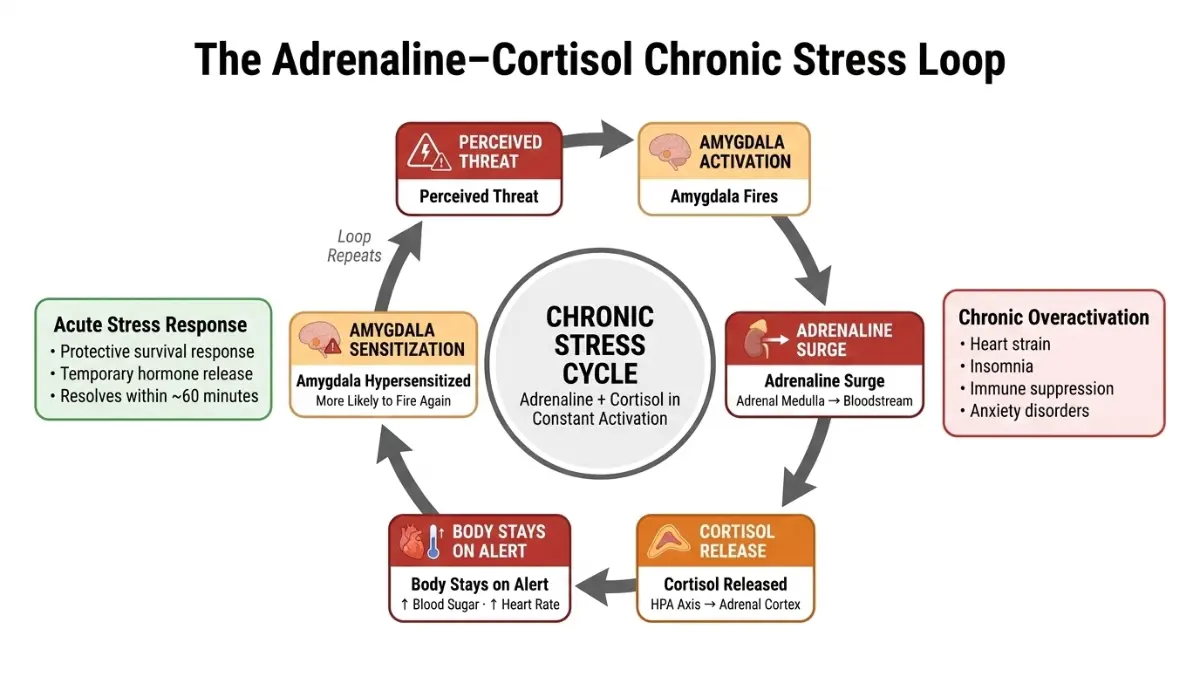
Adrenaline and Cortisol — The Dangerous Double Stress Hormone Loop
Most people think of adrenaline and cortisol as separate stress hormones. In reality, they form a reinforcing feedback loop that amplifies chronic stress:
- Adrenaline fires first — the immediate response (seconds)
- If the threat persists, the HPA axis activates
- The hypothalamus releases CRH → pituitary releases ACTH → adrenal cortex releases cortisol
- Cortisol keeps blood glucose elevated and sustains the alert state
- Elevated cortisol keeps the amygdala on high alert, making it more likely to trigger another adrenaline surge
This loop is the physiological engine behind chronic anxiety disorders, burnout, and stress-related heart disease. Research published via NCBI’s Physiology of Stress Reaction confirms that chronic activation leads to elevated oxidative stress, endothelial dysfunction, and increased risk of atherosclerosis.
Because adrenaline triggers rapid glucose release from the liver, people under chronic stress often experience blood sugar dysregulation. Our Blood Sugar Converter can help you monitor trends if you track your glucose levels.
Pheochromocytoma — When a Tumour Causes Excess Adrenaline
This is something no top-ranking competitor explains for lay readers — and it matters.
A pheochromocytoma is a rare, usually benign tumour of the adrenal medulla that causes the gland to produce excessive amounts of adrenaline and norepinephrine. It affects approximately 0.1–0.6% of people with high blood pressure, according to the Endocrine Society.
Red-flag symptoms that warrant urgent medical evaluation:
- Episodic severe headaches
- Sudden, unexplained spikes in blood pressure
- Profuse sweating with no exertion
- Rapid heart rate episodes
- Feeling of impending doom during episodes
Important: These symptoms are often mistaken for anxiety or panic disorder. If you experience them repeatedly, a simple plasma or urine catecholamine test can confirm or rule out a pheochromocytoma.
Long-Term Health Risks of Sustained High Adrenaline
| Body System | Long-Term Risk |
|---|---|
| Cardiovascular | Hypertension, arrhythmia, increased heart attack risk |
| Immune | Suppressed immunity, increased susceptibility to infection |
| Metabolic | Insulin resistance, blood glucose dysregulation |
| Neurological | PTSD, memory consolidation disruption, anxiety disorders |
| Sleep | Chronic insomnia, sleep architecture disruption |
Adrenaline as a Life-Saving Medication — Clinical Uses of Epinephrine
EpiPen and Anaphylaxis — Adrenaline’s Most Critical Medical Use
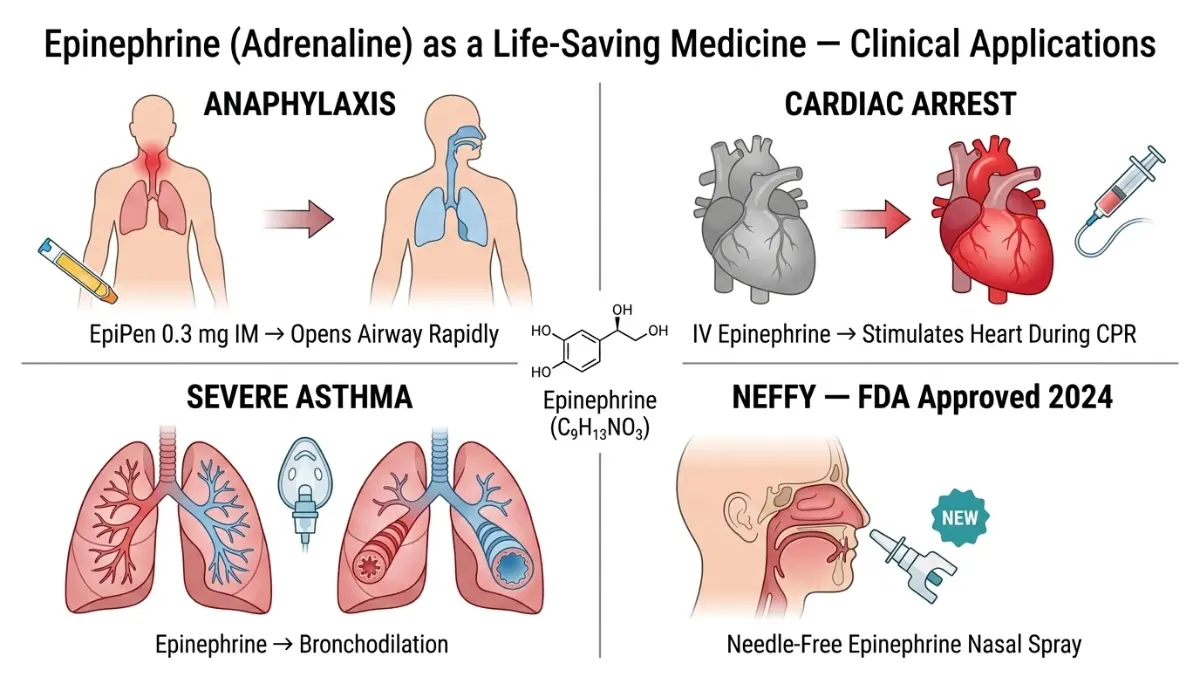
When someone experiences anaphylaxis — a severe, potentially fatal allergic reaction — adrenaline is the only first-line treatment. No antihistamine or steroid works fast enough.
According to a 2025 clinical review in Clinical and Translational Allergy (PMC), anaphylaxis affects between 1.6% and 5.1% of the U.S. population, with approximately 225 deaths per year attributable to the reaction. The review notes that misconceptions about epinephrine use persist even among healthcare providers.
Adrenaline reverses anaphylaxis by:
- Constricting blood vessels → raises blood pressure
- Relaxing airway muscles → opens the throat
- Reducing swelling in the larynx and bronchi
- Stimulating the heart → prevents cardiac collapse
The standard auto-injector (EpiPen) delivers 0.3 mg intramuscularly into the outer thigh.
Medical Uses of Epinephrine — Complete Reference Table
| Medical Condition | How Epinephrine Helps | Route of Administration |
|---|---|---|
| Anaphylaxis | Reverses airway swelling, raises BP | IM auto-injector (EpiPen) |
| Cardiac arrest | Stimulates heart, restores rhythm | IV/IO during CPR |
| Septic shock | Raises blood pressure | IV infusion |
| Severe asthma attack | Bronchodilation | Nebulised or IM |
| Eye surgery | Maintains pupil dilation | Local injection |
| Local anaesthesia | Prolongs numbing, reduces bleeding | Mixed with anaesthetic |
Neffy — The 2024 FDA-Approved Epinephrine Nasal Spray
This is breaking medical news that all top competitors have missed entirely.
In June 2024, the U.S. Food and Drug Administration approved Neffy — the first intranasal epinephrine spray for treating anaphylaxis in adults and children. Neffy delivers 2 mg of epinephrine per spray into the nasal passage, offering a needle-free alternative for patients who delay EpiPen use due to needle phobia (a documented clinical barrier to timely treatment).
Clinical trials showed Neffy achieved comparable epinephrine blood levels to intramuscular injection. For patients managing severe allergies, this represents a meaningful advance in emergency accessibility. If you’re identifying potential inherited allergy or genetic risk factors, our Genetic Risk Assessment Tool can offer personalised insights.
How to Calm an Adrenaline Rush — What Actually Works
Breathing Techniques That Stop the Adrenaline Response
The most clinically validated way to halt an adrenaline surge is vagus nerve activation through controlled breathing. This switches your nervous system from sympathetic (fight-or-flight) to parasympathetic (rest-and-digest) mode.
The 4-7-8 Method (clinically supported):
- Inhale through your nose for 4 seconds
- Hold your breath for 7 seconds
- Exhale slowly through your mouth for 8 seconds
- Repeat 3–4 cycles
Why it works: The extended exhale activates the vagus nerve, signalling the brainstem to reduce heart rate and lower adrenaline output. Research from Harvard Medical School confirms that slow, deep breathing reliably activates the parasympathetic nervous system.
Box breathing (4-4-4-4) is used by U.S. Navy SEALs and emergency medicine practitioners for the same reason.
Exercise — Using Adrenaline Productively
The exercise paradox: Physical activity triggers an adrenaline release — but regular exercise actually trains your adrenal response to be faster, more precise, and faster to recover.
Athletes show significantly lower resting adrenaline levels and quicker post-stress recovery compared to sedentary individuals. This is called autonomic nervous system conditioning.
Practically: after a stressful event, a 10–20 minute brisk walk metabolises circulating adrenaline faster than sitting still. Your body evolved to use adrenaline physically — movement is the most natural reset mechanism. Use our Heart Rate Zone Calculator to identify the optimal moderate-intensity zone for stress recovery exercise. During intense adrenaline-driven exercise, your sweat rate increases substantially — our Water Intake Calculator helps you maintain optimal hydration.
Long-Term Stress Management to Reduce Chronic Adrenaline
Sustainable adrenaline regulation requires consistent lifestyle practices:
| Strategy | Mechanism | Evidence Level |
|---|---|---|
| Regular aerobic exercise | Lowers baseline sympathetic tone | Strong (RCT-supported) |
| 7–9 hours sleep nightly | Reduces HPA axis hyperactivation | Strong |
| Mindfulness/meditation | Reduces amygdala reactivity | Moderate-strong |
| Reducing caffeine | Directly stimulates adrenaline release | Moderate |
| Cold-water face immersion | Triggers vagal (parasympathetic) reflex | Moderate |
| Limiting late-night screen use | Reduces nighttime perceived-threat triggers | Moderate |
| Social connection | Oxytocin release suppresses cortisol-adrenaline loop | Moderate |
Our depression guide and guide on neuroplasticity and rewiring the brain explore how chronic stress hormones affect mental health and how the brain can recover.
When to See a Doctor About Your Adrenaline Levels
Seek medical evaluation if you experience:
- Heart palpitations at rest occurring more than twice per week
- Unexplained episodes of sweating, headaches, and high blood pressure together
- Tremors or shakiness without exertion or caffeine
- Panic-like episodes that wake you from sleep
- Blood pressure spikes with no identified cause
A doctor can request a 24-hour urine catecholamine test or plasma metanephrines to measure adrenaline and its metabolites. This is the standard screening test for pheochromocytoma and chronic catecholamine excess.
What This Means For You: Most people experiencing adrenaline-related symptoms have a manageable, lifestyle-driven cause. But if symptoms are severe, episodic, and occur at rest, don’t dismiss them as anxiety — get tested.
Frequently Asked Questions About Adrenaline
1. What is the difference between adrenaline and epinephrine?
They are identical. Adrenaline is the British name; epinephrine is the American/international medical name for the same hormone and neurotransmitter.
2. Is adrenaline a hormone or a neurotransmitter?
Both. It functions primarily as a hormone released from the adrenal glands into the bloodstream, but also acts as a neurotransmitter in small amounts within the central nervous system.
3. What triggers an adrenaline rush?
Any perceived threat — physical (a car accident, a loud noise) or psychological (a presentation, an argument, or even a stressful thought) — activates the adrenal glands to release adrenaline within seconds.
4. How long does adrenaline last in your body?
The hormone itself has a half-life of 2–3 minutes in the blood. However, its physiological effects — racing heart, dilated pupils, elevated blood glucose — can persist for 20 to 60 minutes after the trigger.
5. Can adrenaline cause a heart attack?
Prolonged or extremely high adrenaline surges can stress the heart. A condition called Takotsubo cardiomyopathy (“broken heart syndrome”) is directly triggered by massive adrenaline release during intense emotional distress, causing temporary heart muscle dysfunction.
6. What are the symptoms of too much adrenaline?
Chronic excess adrenaline presents as persistent palpitations, insomnia, unexplained sweating, elevated blood pressure, anxiety, tremors, and weight loss. When caused by a tumour, these symptoms occur in sudden, severe episodes.
7. Why does adrenaline spike at night?
With no external stimulation, the brain processes unresolved stress and perceived threats during quiet periods. This activates the amygdala, triggering adrenaline release even without physical danger — a primary driver of nocturnal anxiety and insomnia.
8. What is adrenaline used for medically?
Adrenaline is the first-line treatment for anaphylaxis, cardiac arrest, and septic shock. It is also used during surgical procedures to prolong local anaesthesia and reduce bleeding.
9. How do you calm an adrenaline rush quickly?
The most effective immediate technique is slow, extended-exhale breathing (such as the 4-7-8 method), which activates the vagus nerve and shifts the nervous system from sympathetic to parasympathetic mode within 2–3 minutes.
10. What is a pheochromocytoma?
A pheochromocytoma is a rare adrenal gland tumour that causes excess adrenaline and norepinephrine production. It presents with episodic hypertension, headaches, and sweating, and is diagnosed through urine or blood catecholamine testing.
11. Can chronic stress permanently damage your adrenaline system?
Prolonged chronic stress can dysregulate the HPA axis and alter adrenal sensitivity. Research shows that sustained elevation of stress hormones contributes to lasting cardiovascular, immune, and neurological changes — though these are largely reversible with proper lifestyle intervention and, when necessary, medical treatment.
For personalised health information based on your individual risk profile, explore mymedicineadvisor.com — home to 21 internationally credentialed medical experts and a suite of free health tools.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.