On This Page – Quick Medical Summary
⚡ Quick Answer: Haematopoietic stem cells (HSCs) are rare, self-renewing cells in the bone marrow that produce every type of blood cell in the human body — including red blood cells, white blood cells, and platelets. They are the biological foundation of bone marrow transplantation, gene therapy, and some of the most powerful cancer treatments available in 2026.
Your Body Makes 500 Billion Blood Cells Every Day — Here’s the Cell Doing It
In 2019, Marcus, a 34-year-old father from Atlanta, was diagnosed with acute myeloid leukemia (AML). His haematologist told him three words that changed everything: “You need a transplant.” Specifically, a haematopoietic stem cell transplant — one that would replace his diseased blood-forming cells with healthy ones from a matched donor. Two years later, Marcus was in complete remission.
What made that possible? A remarkably rare type of cell called a haematopoietic stem cell.
What Are Haematopoietic Stem Cells?
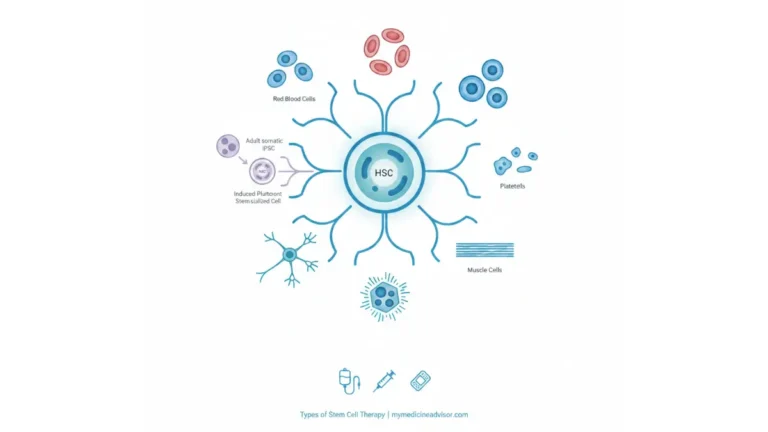
Haematopoietic stem cells (HSCs) are the master cells of your blood system. Every single blood cell in your body — from the red cells carrying oxygen to your brain, to the white cells fighting infections right now — originates from haematopoietic stem cells.
These cells have two extraordinary abilities:
- Self-renewal — They can copy themselves indefinitely, maintaining a lifelong supply
- Multipotency — They can differentiate into any of the many blood cell types the body needs
Here is what makes them even more remarkable: they represent only about 1 in every 10,000 bone marrow cells. Despite being incredibly rare, a tiny number of haematopoietic stem cells can reconstruct an entire blood and immune system from scratch — a fact that forms the entire scientific basis of bone marrow transplantation.
According to the NIH National Library of Medicine’s Stem Cells resource, stem cells are unique because they can divide, self-renew, and develop into specialized cell types — properties that make haematopoietic stem cells one of the most studied and clinically valuable cell types in medicine.
🔑 Key Takeaway: One haematopoietic stem cell can potentially replenish your entire blood and immune system. This is not theoretical — it is the basis of over 50,000 transplant procedures performed globally every year.
If you are experiencing unexplained symptoms such as fatigue, unusual bruising, or repeated infections, use our Symptom Checker to help identify whether a blood-related evaluation may be warranted.
Inside the Bone Marrow — Where the Blood Cell Masterkey Lives
Haematopoietic stem cells do not simply float freely in the bloodstream. They live in highly specialized microenvironments — and understanding where they live explains a great deal about how they work.
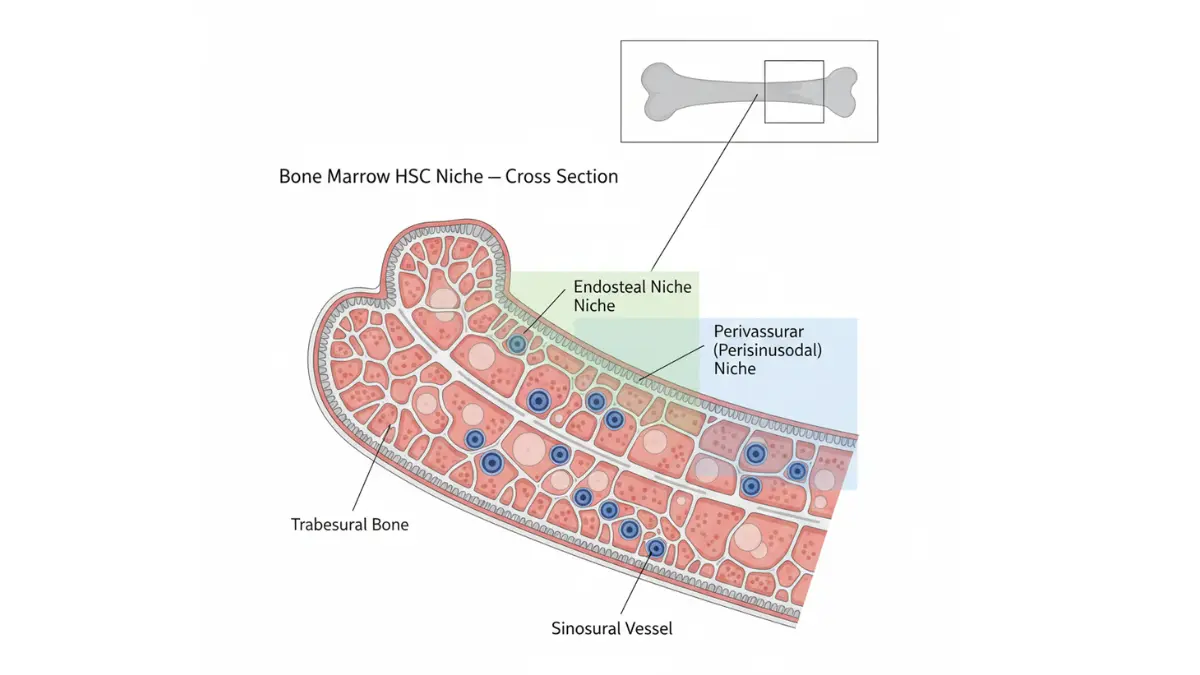
The Bone Marrow Niche
In adults, the primary home of haematopoietic stem cells is the red bone marrow, located in the cores of flat bones like the pelvis, sternum, and vertebrae. Within the marrow, HSCs occupy specific regions called perisinusoidal niches — zones near blood vessels where protective signals keep stem cells in a dormant, protected state.
This dormancy is intentional. Haematopoietic stem cells spend most of their lives in a state of quiescence (low activity), which protects them from exhaustion and DNA damage over decades of life.
Other Sources of Haematopoietic Stem Cells
Beyond bone marrow, HSCs are also found in smaller quantities in:
- Peripheral blood — especially after mobilisation using growth factor injections
- Umbilical cord blood — a rich source collected at birth, now banked globally
- Fetal liver — the primary site of blood cell production before birth
Every Blood Cell You Have Comes From Here
The process by which haematopoietic stem cells generate all blood cells is called haematopoiesis. The table below shows every major blood cell type produced — and what happens if those cells fail.
| Blood Cell Type | Lineage | Primary Function | Consequence of Failure |
|---|---|---|---|
| Red blood cells (erythrocytes) | Myeloid | Oxygen transport | Anaemia, fatigue |
| Platelets (thrombocytes) | Myeloid | Blood clotting | Dangerous bleeding |
| Neutrophils | Myeloid | Bacterial defence | Severe infections |
| Monocytes/Macrophages | Myeloid | Inflammation, immunity | Immune dysregulation |
| T cells | Lymphoid | Adaptive immune response | Immune deficiency |
| B cells | Lymphoid | Antibody production | Repeated infections |
| Natural killer (NK) cells | Lymphoid | Cancer cell surveillance | Reduced tumour defence |
🔑 What This Means For You: When bone marrow fails — whether from disease, chemotherapy, or a genetic disorder — every single cell type in this table is affected simultaneously. This is why haematopoietic stem cell transplantation can be life-saving.
Not All Blood Stem Cells Are Equal — The 3-Tier Hierarchy Explained
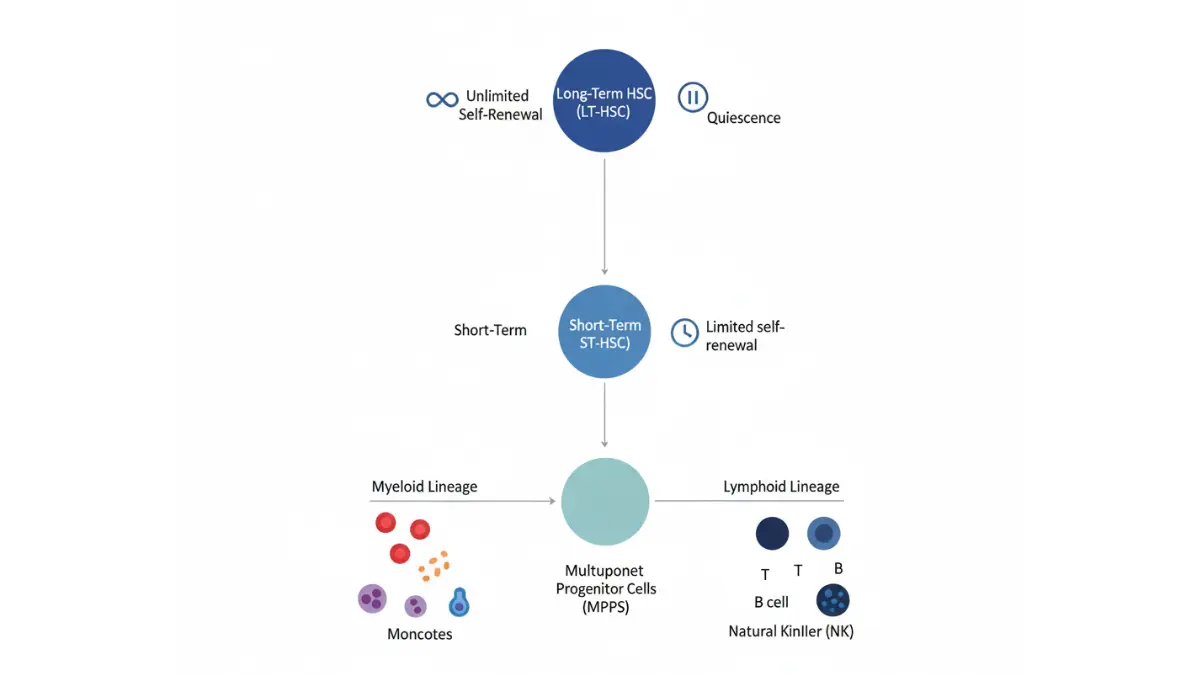
Most descriptions of haematopoietic stem cells treat them as a single population. That is a significant oversimplification. HSCs exist in a precise three-tier hierarchy, and understanding this hierarchy is essential for grasping why transplant outcomes vary so dramatically between patients.
Tier 1: Long-Term Haematopoietic Stem Cells (LT-HSCs)
LT-HSCs are the true master cells. They possess unlimited self-renewal capacity and can reconstitute the entire haematopoietic system indefinitely. These are the cells that matter most in bone marrow transplantation — only LT-HSCs provide permanent, lifelong engraftment.
Tier 2: Short-Term Haematopoietic Stem Cells (ST-HSCs)
ST-HSCs have limited self-renewal capacity — they can replenish themselves for only a few months before transitioning into progenitor cells. They serve as an important bridge between the master cells and the rapidly dividing progenitors.
Tier 3: Multipotent Progenitor Cells (MPPs)
MPPs have lost the ability to self-renew but retain the capacity to differentiate into multiple blood cell lineages. They are the production-line workers of the haematopoietic system.
The 4 Defining Properties of All Haematopoietic Stem Cells
- Self-renewal — Divide to create identical daughter stem cells, maintaining the pool indefinitely
- Multipotency — Differentiate into any blood cell type across both myeloid and lymphoid lineages
- Quiescence — Remain dormant in the bone marrow niche, protecting genomic integrity
- Mobilisation — Respond to physiological stress by migrating from bone marrow into peripheral blood
🔬 2024 Research Update: Immune Rejuvenation Via HSC Targeting
A landmark study published in Nature (Ross et al., March 2024) by researchers at Stanford University demonstrated something remarkable: depleting myeloid-biased HSCs in aged mice actually restored a younger, more functional immune system. The study showed that the proportion of myeloid-biased HSCs increases with age, driving chronic inflammation and reduced adaptive immunity. Selectively removing these cells rejuvenated immune function — a finding with profound implications for treating age-related blood disorders.
Date-stamped: Nature, March 27, 2024 | Evidence level: Preclinical with Phase I translation advancing
If you have a family history of blood cancers or inherited haematological disorders, our Genetic Risk Assessment Tool can help you evaluate your personal risk profile.
The 15+ Diseases That Haematopoietic Stem Cell Transplants Can Treat
When most people hear “stem cell transplant,” they think of leukemia. The reality is far broader. Haematopoietic stem cell transplantation (HSCT) is one of the most versatile treatments in all of medicine, with over 50,000 procedures performed globally each year according to the World Marrow Donor Association.
Blood Cancers
- Acute Myeloid Leukemia (AML) — the most common indication for allogeneic HSCT
- Acute Lymphoblastic Leukemia (ALL) — particularly in high-risk or relapsed cases
- Chronic Myeloid Leukemia (CML) — for cases resistant to targeted therapy
- Multiple Myeloma — autologous transplant is standard of care
- Hodgkin’s and Non-Hodgkin’s Lymphoma — both autologous and allogeneic approaches used
Non-Cancerous Blood Disorders
- Sickle Cell Disease — currently the only available cure for this debilitating condition
- Beta-Thalassaemia Major — transplant can eliminate lifelong transfusion dependency
- Aplastic Anaemia — HSC transplant is curative in younger patients with matched donors
- Myelodysplastic Syndrome (MDS) — the only potentially curative option
Immune Deficiency Conditions
- Severe Combined Immunodeficiency (SCID) — transplant is performed in infancy and is life-saving
- Wiskott-Aldrich Syndrome
- Chronic Granulomatous Disease
2026 Survival and Outcomes Reference Table
| Disease | Transplant Type | Reported Survival Rate | Source |
|---|---|---|---|
| Acute Myeloid Leukemia | Allogeneic | ~40–60% at 5 years | PMC/NHLBI data |
| Sickle Cell Disease | Allogeneic (matched sibling) | ~85–95% | Published clinical data |
| Aplastic Anaemia | Allogeneic | ~70–80% at 5 years | NHLBI-affiliated studies |
| Multiple Myeloma | Autologous | ~68.8% alive at 10 years | PMC published data |
| Non-Hodgkin’s Lymphoma | Autologous/Allogeneic | ~74% PFS at 2 years | BMT CTN Trial data |
For a detailed guide on the full transplant process — from eligibility testing to discharge and recovery — the American Cancer Society’s Stem Cell Transplant Guide provides comprehensive, verified information.
Understanding Your Transplant Type: A Plain-English Guide
Autologous — Your own stem cells are collected before chemotherapy and reinfused afterwards. Used primarily for multiple myeloma and certain lymphomas. Lower rejection risk; no GVHD.
Allogeneic — Stem cells from a matched donor (related or unrelated). Used for leukemia, aplastic anaemia, sickle cell. Higher risk profile but offers a graft-versus-tumour effect that can eliminate residual cancer cells.
Syngeneic — From an identical twin. Ideal match, extremely rare.
US Cost Context (2026)
- Autologous HSCT: $100,000–$180,000
- Allogeneic HSCT: $250,000–$400,000
- Insurance coverage: Most major US insurers cover HSCT for approved indications. Always verify coverage before proceeding.
If you are managing post-transplant metabolic monitoring, our Blood Sugar Converter can help you track and convert glucose values between measurement units.
5 Haematopoietic Stem Cell Breakthroughs from 2025–2026 That Could Change Medicine
This is where mymedicineadvisor.com delivers what Wikipedia, Nature, and Healthline all fail to provide together — a clear, accessible, and verified summary of the most important recent HSC science and what it means for patients today.
Breakthrough 1: MYCT1 — The Stemness Regulator Discovered
Scientists identified MYCT1 as a crucial regulator of the core properties that make haematopoietic stem cells behave as true stem cells. This discovery, reported in Nature in 2025, may finally enable reliable ex vivo expansion of HSCs — meaning clinicians could grow enough stem cells in the laboratory to dramatically improve transplant availability for patients who currently cannot find sufficient matched donor cells.
🟡 Status: Preclinical validation complete; human application in early development
Breakthrough 2: Ferroptosis Inhibition Unlocks Ex Vivo Expansion
A 2025 study showed that inhibiting ferroptosis — a specific form of programmed cell death — dramatically extends the survival and expansion of haematopoietic stem cells grown outside the body. This breakthrough could transform the supply constraints that currently limit transplantation, particularly for patients relying on cord blood units where cell numbers are always limited.
🟡 Status: Preclinical; rapid translation expected
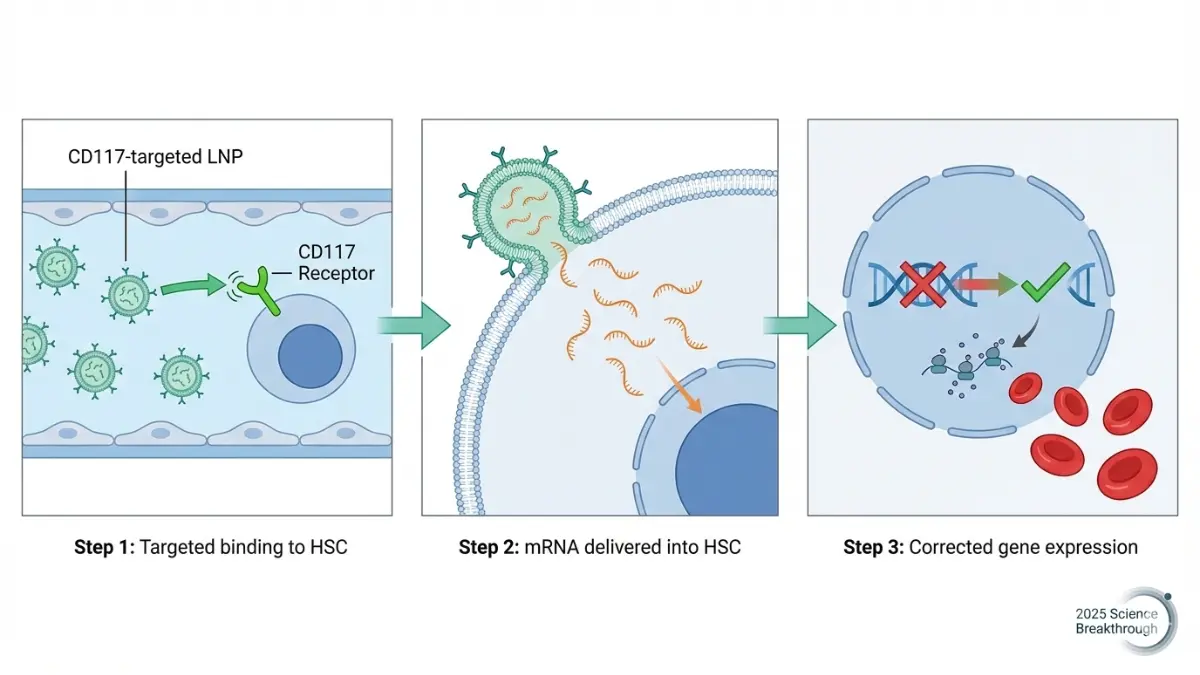
Breakthrough 3: In Vivo mRNA Gene Therapy Corrects Sickle Cell
Perhaps the most clinically significant advance: a research team developed CD117/LNP-mRNA — a novel lipid nanoparticle system that delivers gene-correcting mRNA directly to haematopoietic stem cells inside the body, without requiring their removal and external manipulation. Published in Science and now entering clinical translation, this system achieved near-complete correction of sickle haematopoietic cells in preclinical models.
🟢 Status: Published in Science; clinical translation advancing in 2025–2026
Breakthrough 4: New Understanding of the HSC Niche
In August 2025, a landmark Nature paper overturned 60 years of established biology by demonstrating that HSC numbers are regulated by both systemic AND local mechanisms simultaneously — not just by the local niche size as previously believed. This dual-control discovery reshapes how scientists understand bone marrow failure and clonal haematopoiesis, opening new therapeutic targets.
🟢 Status: Published and confirmed, Nature August 2025
Breakthrough 5: Depleting Old HSCs Rejuvenates Immunity (Human Trials Advancing)
Building on the 2024 Stanford Nature study mentioned in Section 3, research teams are now designing Phase I/II clinical trials to test whether selectively depleting myeloid-biased haematopoietic stem cells in elderly patients can restore immune function and reduce age-related disease risk. If successful, this would represent a paradigm shift in how we treat immune ageing.
🟡 Status: Phase I/II trial design stage, 2025–2026
Evidence Strength Pyramid
| Colour | Level | Examples from Above |
|---|---|---|
| 🟢 Confirmed & Translating | Published, entering clinical use | mRNA HSC gene therapy; niche dual-control biology |
| 🟡 Promising Preclinical | Strong lab data, human trials imminent | Ferroptosis inhibition; MYCT1 expansion; immune rejuvenation |
🔑 What This Means For You: If you or a family member has sickle cell disease, beta-thalassaemia, or a blood cancer — these breakthroughs are not speculative future science. They are happening right now in clinical centres across the US. Ask your haematologist specifically about eligibility for gene therapy trials involving haematopoietic stem cell modification.
For the latest updates on haematological health and related treatment advances, explore our Health Tips section and our detailed guide on stem cell therapy and real-world results.
A Doctor Said “Stem Cell Transplant” — Here’s Exactly What Happens Next
Hearing those words is overwhelming. Most patients leave their haematologist’s office with an avalanche of information and no clear mental map of what the process actually involves. This section gives you that map — clearly, compassionately, and in plain English.
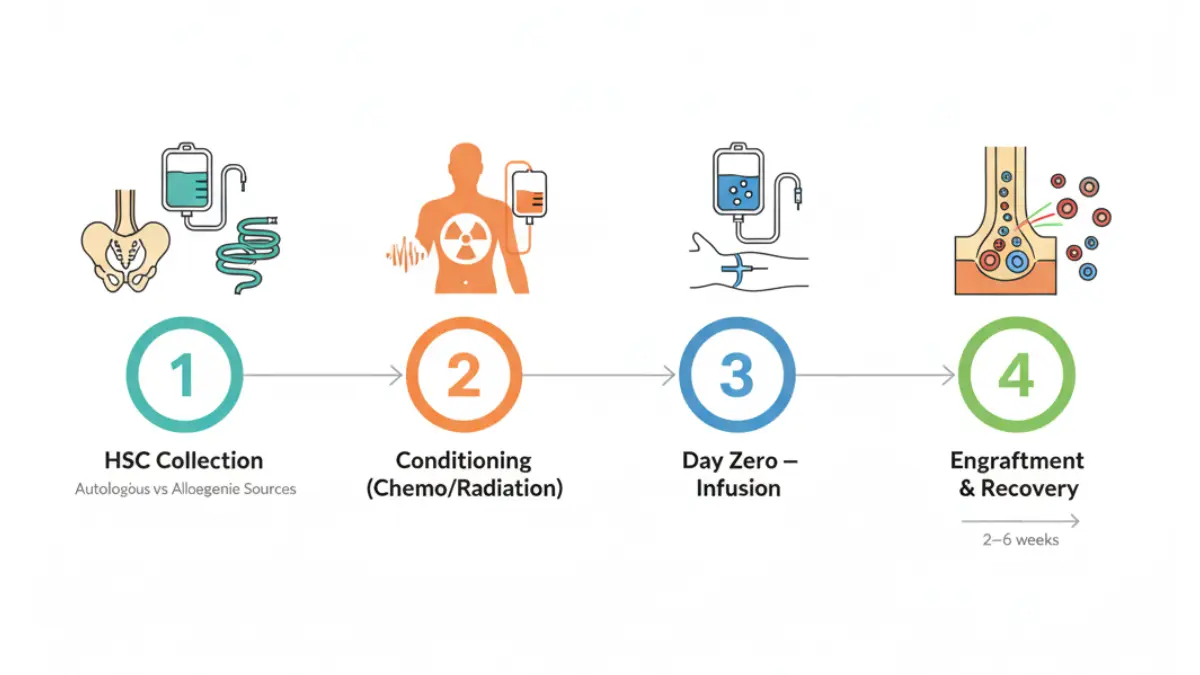
The 4 Stages of Haematopoietic Stem Cell Transplantation
Stage 1 — Evaluation and Eligibility (2–4 weeks)
Your transplant team will assess your overall fitness, organ function, and HLA (human leukocyte antigen) tissue type. HLA matching is the genetic compatibility test that determines whether a donor’s haematopoietic stem cells will be accepted by your immune system. A perfect 10/10 HLA match is ideal — but haploidentical (half-matched) transplants are now feasible, dramatically expanding the donor pool.
Stage 2 — Conditioning (1–9 days before transplant)
You receive high-dose chemotherapy and/or radiation therapy. This serves three purposes:
- Destroys remaining cancer or diseased cells
- Suppresses your immune system to prevent rejection
- Creates physical space in the bone marrow niche for incoming haematopoietic stem cells
Stage 3 — Infusion (Day Zero)
Haematopoietic stem cells are delivered intravenously — like a blood transfusion. The process is painless. You remain awake. This is the transplant itself — a moment that typically takes hours but whose effects last a lifetime.
Stage 4 — Engraftment and Recovery (2–6 weeks)
The transplanted haematopoietic stem cells migrate to the bone marrow niche and begin producing new blood cells. Full engraftment is confirmed when red and white blood cell counts stabilise. This is the most critical window — infection risk is highest during this phase.
Key Risks to Discuss With Your Haematologist
| Risk | Who Is Affected | What to Know |
|---|---|---|
| Graft-versus-Host Disease (GVHD) | Allogeneic transplant only | Donor immune cells attack recipient tissues; manageable but serious |
| Infection | All transplant types | Immune suppression window creates vulnerability; preventive antibiotics used |
| Graft failure | All types (rare) | Stem cells fail to engraft; requires repeat procedure |
| Organ toxicity | All types | Conditioning therapy can stress heart, liver, kidneys; monitored closely |
3 Critical Questions to Ask Your Transplant Team
- “Am I a candidate for autologous or allogeneic transplant — and what drives that decision in my specific case?”
- “What is the HLA matching strategy, and how does a haploidentical donor option change my timeline and risk profile?”
- “Are there active gene therapy trials involving haematopoietic stem cell modification that I might qualify for?”
Post-Transplant Recovery Timeline
| Milestone | Approximate Timeframe |
|---|---|
| Initial engraftment | 2–6 weeks post-transplant |
| Discharge from transplant centre | When ANC ≥ 500/mm³ and no fever for 24–48 hours |
| Near-normal blood counts | 2–6 months |
| Full immune reconstitution | 6–12 months or longer |
| Re-vaccination programme begins | Typically 6–12 months post-transplant |
Managing post-transplant medications can be complex. Our Pill Identifier tool helps you verify and identify medications during your recovery period. For patients navigating the broader landscape of cancer treatment options, our guide to immunotherapy and how it works provides important context on how haematopoietic stem cell approaches compare with other modern therapies.
For a deeper understanding of the entire transplant journey from a patient perspective, the NIH National Heart, Lung, and Blood Institute’s Molecular Hematopoiesis research page provides world-class background on how these cells are studied and translated into clinical care.
🔑 What This Means For You: The transplant process is demanding — but it is structured, monitored, and supported by dedicated specialists at every stage. Knowledge is your most powerful tool going in.
Frequently Asked Questions — Haematopoietic Stem Cells
1. What are haematopoietic stem cells in simple terms?
Haematopoietic stem cells are rare bone marrow cells that produce every type of blood cell in the body. They self-renew and can differentiate into red cells, white cells, and platelets throughout your entire life.
2. Where are haematopoietic stem cells found in the body?
Primarily in the red bone marrow of flat bones (pelvis, sternum, vertebrae). Smaller numbers circulate in peripheral blood and are also found in umbilical cord blood.
3. What is the difference between haematopoietic and mesenchymal stem cells?
Haematopoietic stem cells produce blood and immune cells. Mesenchymal stem cells produce structural tissues — bone, cartilage, fat, and muscle. Both live in bone marrow but serve entirely different biological roles.
4. How many blood cells do haematopoietic stem cells produce per day?
The average adult produces approximately 500 billion blood cells every day through haematopoiesis — all originating from haematopoietic stem cells in the bone marrow.
5. What diseases are treated with haematopoietic stem cell transplants?
Over 15 conditions including acute myeloid leukemia, sickle cell disease, aplastic anaemia, multiple myeloma, lymphoma, thalassaemia, and severe combined immunodeficiency (SCID).
6. What is graft-versus-host disease (GVHD)?
GVHD occurs when donor haematopoietic stem cells produce immune cells that recognise the recipient’s body as foreign and attack it. It is managed with immunosuppressive medications and is a risk specific to allogeneic transplants.
7. Can haematopoietic stem cells be used for gene therapy?
Yes — and this is one of the fastest-growing areas in medicine. In 2025, CD117/LNP-mRNA delivery systems successfully corrected sickle cell haematopoietic stem cells in vivo, without removing cells from the body — a major clinical advance.
8. What is the difference between autologous and allogeneic transplant?
Autologous uses your own haematopoietic stem cells. Allogeneic uses a donor’s cells. Autologous carries lower rejection risk; allogeneic offers a potential graft-versus-tumour effect that can eliminate residual cancer.
9. How long does haematopoietic stem cell transplant take to work?
Initial engraftment takes 2–6 weeks. Full immune reconstitution typically takes 6–12 months. Complete recovery from the transplant process may take 1–2 years.
10. Can cord blood replace bone marrow as an HSC source?
Yes. Cord blood is an established alternative HSC source, particularly valuable when a fully matched bone marrow donor cannot be found. Cord blood units are now banked globally and can be accessed by patients without matched family donors.
11. What is clonal haematopoiesis and should I be concerned?
Clonal haematopoiesis occurs when a single haematopoietic stem cell with a somatic mutation expands and dominates blood cell production. It increases with age and raises the risk of blood cancers and cardiovascular disease. If detected incidentally on a CBC, discuss significance with your haematologist — it requires monitoring but not always treatment.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.