On This Page – Quick Medical Summary
Understanding Your T-Score -2.5 Diagnosis
What Does a T-Score of -2.5 Actually Mean?
A T-score of -2.5 on your bone density scan indicates that your bone mineral density is 2.5 standard deviations below the average peak bone mass of a healthy 30-year-old adult. This specific threshold marks the clinical diagnosis of osteoporosis according to the World Health Organization’s criteria.
When Maria received her DEXA scan results showing a T-score of -2.5 at her lumbar spine, she felt overwhelmed. Like many patients, she wondered: “Does this mean my bones will definitely break?”
The answer is more nuanced than a simple yes or no. Your T-score represents a snapshot of bone density at a specific moment, but it doesn’t predict your future with absolute certainty. Think of it as a warning light on your dashboard—it signals that action is needed, but the outcome depends on what you do next.
How T-Scores Are Calculated and Why -2.5 Matters
Your DEXA scan measures bone mineral density at critical fracture sites—typically your hip, spine, and sometimes your forearm. The machine compares your results against two benchmarks, which is where understanding the difference between diagnostic testing approaches becomes important.
The calculation works like this: If peak bone density equals 0, each point below represents one standard deviation of bone loss. According to research from Johns Hopkins Medicine, fracture risk approximately doubles with each 1-point drop in T-score.

T-Score Classification Table:
| T-Score Range | Diagnosis | Fracture Risk Level |
|---|---|---|
| -1.0 or higher | Normal bone density | Low baseline risk |
| -1.0 to -2.5 | Osteopenia (low bone mass) | Moderate risk (1.5-2x) |
| -2.5 or lower | Osteoporosis | High risk (4x or more) |
| -2.5 with prior fracture | Severe osteoporosis | Very high risk (6-10x) |
The Difference Between T-Score and Z-Score
While your doctor focuses on T-scores for diagnosis, you might also see a Z-score on your report. The Z-score compares your bone density to people of your same age, sex, and ethnicity.
If your Z-score is significantly low (below -2.0), it suggests something beyond normal aging is causing bone loss. This might trigger additional testing to rule out secondary causes like vitamin D deficiency, thyroid disorders, or medication effects. Understanding your complete health picture, including factors you can track with tools like a BMI calculator, helps contextualize your bone health.
Your Fracture Risk at -2.5: What the Numbers Tell You
Here’s what studies from the National Institutes of Health reveal: A T-score of -2.5 increases your fracture risk by approximately 4 to 5 times compared to someone with normal bone density. But this is a statistical average—your individual risk depends on multiple factors.
Key Risk Multipliers Beyond T-Score:
- Previous fracture history (triples risk)
- Age over 65 (doubles risk per decade)
- Family history of hip fracture
- Current smoking status
- Low body weight (BMI under 19)
- Chronic steroid use
- Frequent falls (2+ per year)
Dr. Sarah Chen, an endocrinologist treating osteoporosis for 15 years, explains: “I’ve seen patients with a T-score of -2.6 remain fracture-free for decades with proper treatment, while others at -2.3 fracture within a year. The T-score is just one piece of the puzzle.”
Is -2.5 Always Osteoporosis? When Other Conditions Matter
Not every low T-score means primary osteoporosis. Sometimes bone density readings can be affected by arthritis, previous fractures, or bone deformities that make the scan less accurate. More seriously, conditions like osteomalacia (vitamin D deficiency), multiple myeloma, or hyperparathyroidism can mimic osteoporosis.
When Additional Testing Is Critical:
- Unexpectedly low T-score in men under 50
- Young premenopausal women with no risk factors
- Rapid bone loss over 1-2 years
- Severe back pain with vertebral compression
- Lab abnormalities in calcium or vitamin D
Your healthcare provider may order blood work including calcium levels, vitamin D (25-hydroxyvitamin D), thyroid function, and kidney function tests to rule out secondary causes. This comprehensive approach, similar to how doctors evaluate other complex diagnostic results, ensures you receive the right treatment.
What This Means For You: A T-score of -2.5 is a diagnosis that demands attention but offers tremendous opportunity for intervention. With modern treatments and lifestyle modifications, most people can significantly reduce fracture risk and even improve bone density over time.
Immediate Next Steps After Your -2.5 Diagnosis
What Happens Next: Your First 30 Days After Diagnosis
The 30 days following your osteoporosis diagnosis are crucial for establishing a treatment foundation. Research shows that patients who take immediate action reduce their fracture risk by 25-40% compared to those who delay treatment.
Your Week-by-Week Action Plan:
Week 1: Information Gathering
- Schedule a comprehensive follow-up appointment with your primary care physician or endocrinologist
- Request copies of your complete DEXA scan report
- Document all current medications and supplements
- Begin a fall diary to track any balance issues
Week 2-3: Medical Evaluation
- Complete recommended blood work
- Discuss FRAX score calculation
- Review medication options
- Schedule specialist consultation if needed
Week 4: Treatment Initiation
- Start prescribed medications
- Implement dietary changes
- Begin supervised exercise program
- Set up follow-up appointment schedule
Critical Questions to Ask Your Doctor Today
Walking into your doctor’s office prepared transforms a passive appointment into an active partnership. These questions, developed through consultation with osteoporosis specialists and patient advocates, ensure you don’t miss critical information.
About Your Diagnosis:
- “What was my exact T-score at each measured site (spine, hip, forearm)?”
- “How does my T-score compare to my last scan, if I had one?”
- “What is my absolute fracture risk over the next 10 years?”
- “Are there any secondary causes we should rule out?”
About Treatment Options: 5. “Which medication do you recommend and why?” 6. “What are realistic expectations for bone density improvement?” 7. “How will we monitor treatment effectiveness?” 8. “What are the alternatives if I can’t tolerate the first-line treatment?”
Studies from Stanford University Medical Center show that patients who ask detailed questions have 60% better medication adherence and superior outcomes.
Additional Tests You May Need
Beyond your DEXA scan, comprehensive osteoporosis evaluation includes several laboratory tests. According to guidelines from the National Institute on Aging, these tests identify treatable causes of bone loss.
Essential Lab Work:
Calcium Metabolism:
- Serum calcium (normal: 8.5-10.5 mg/dL)
- 25-hydroxyvitamin D (optimal: >30 ng/mL)
- Parathyroid hormone (PTH)
- 24-hour urine calcium
Bone Turnover Markers:
- CTX (bone resorption marker)
- P1NP (bone formation marker)
Secondary Cause Screening:
- Complete blood count (CBC)
- Comprehensive metabolic panel
- Thyroid stimulating hormone (TSH)
- Testosterone (for men)
- Celiac disease screening if indicated
Jennifer, 58, discovered her T-score of -2.7 was partly due to undiagnosed celiac disease. After treating the underlying condition and starting bone-building medication, her follow-up scan two years later showed improvement to -2.3—a remarkable reversal.
FRAX Score Calculation: Understanding Your 10-Year Fracture Risk
The FRAX (Fracture Risk Assessment Tool) converts your T-score and risk factors into a personalized prediction. Developed by the World Health Organization, this calculator estimates your 10-year probability of hip fracture and major osteoporotic fracture.
FRAX Input Variables:
- Age, sex, weight, and height (consider checking your ideal weight calculator for context)
- Previous fracture
- Parental hip fracture history
- Current smoking
- Glucocorticoid use
- Rheumatoid arthritis
- Secondary osteoporosis
- Alcohol intake
- Femoral neck bone mineral density
Treatment Thresholds According to National Osteoporosis Foundation:
- Hip fracture risk ≥3%: Consider treatment
- Major osteoporotic fracture risk ≥20%: Consider treatment
- T-score ≤-2.5 at any site: Treatment recommended
Access the official FRAX calculator through the University of Sheffield to understand your individualized risk profile.
When to See an Endocrinologist vs. Primary Care
Most osteoporosis cases can be effectively managed by primary care physicians, but certain situations warrant specialist referral.
Endocrinologist Referral Indicated When:
- T-score below -3.5 (severe osteoporosis)
- Men under 50 or premenopausal women with osteoporosis
- Suspected secondary causes requiring complex management
- Fracture despite appropriate treatment
- Multiple prior fractures
- Contraindications to standard medications
- Complex medication history
- Chronic kidney disease stage 4-5
Primary Care Appropriate For:
- Straightforward postmenopausal osteoporosis
- No complicating medical conditions
- Standard medication candidates
- Good response to initial treatment
Creating Your Personalized Treatment Timeline
Evidence-based osteoporosis management follows a structured timeline that balances urgency with thoughtful decision-making.
Treatment Timeline Table:
| Timepoint | Action | Purpose |
|---|---|---|
| Day 1-7 | Initial evaluation, labs ordered | Baseline assessment |
| Week 2 | Lab results review | Rule out secondary causes |
| Week 2-3 | Treatment decision | Medication selection |
| Month 1 | Treatment start | Begin bone protection |
| Month 3 | Side effect assessment | Ensure tolerance |
| Month 6 | Clinical check-in | Assess adherence, adjust plan |
| Year 1-2 | Follow-up DEXA scan | Measure treatment response |
| Every 2 years | Ongoing monitoring | Track long-term progress |
Insurance Coverage and Cost Considerations
Understanding the financial aspects of osteoporosis treatment helps prevent delays due to cost concerns. Medicare and most private insurance plans cover DEXA scans and medications, but specifics vary.
Medicare Coverage (2025):
- DEXA scan: Covered once every 24 months (or more frequently if medically necessary)
- Oral bisphosphonates: Typically $4-$40/month
- IV zoledronic acid: Covered as Part B at 80% after deductible
- Denosumab injections: Part B coverage, but check specific plan
Cost Comparison Without Insurance:
- Generic alendronate: $10-$30/month
- Brand-name Fosamax: $200-$300/month
- Denosumab (Prolia): $1,800-$2,000 per injection (twice yearly)
- Teriparatide (Forteo): $3,500-$4,000/month
- Romosozumab (Evenity): $4,000-$4,500/month
Financial Assistance Resources:
- Manufacturer patient assistance programs
- NeedyMeds.org for medication discount programs
- State pharmaceutical assistance programs
- Medicare Extra Help for low-income beneficiaries
What This Means For You: Taking immediate, organized action in your first 30 days sets the foundation for successful long-term bone health management. Most patients find that once the initial steps are complete, ongoing management becomes routine.
Evidence-Based Medication Strategies for Osteoporosis
First-Line Treatments: Bisphosphonates
Bisphosphonates remain the gold standard first-line therapy for osteoporosis, backed by decades of research and millions of patient-years of safety data. These medications work by slowing the bone-dissolving cells (osteoclasts) while allowing bone-building cells (osteoblasts) to catch up.
How Bisphosphonates Work:
Think of your bones as a constantly remodeling building. Old, worn sections are demolished (resorption) while new, strong sections are constructed (formation). In osteoporosis, demolition outpaces construction. Bisphosphonates apply the brakes to demolition crews, giving construction teams time to rebuild.
According to Harvard Medical School research, bisphosphonates reduce vertebral fracture risk by 40-70% and hip fracture risk by 40-50% over 3 years.
Primary Bisphosphonate Options:
Alendronate (Fosamax):
- Dosing: 70mg once weekly or 10mg daily
- Administration: Take on empty stomach with 8oz water, remain upright 30 minutes
- Efficacy: Increases spine BMD by 5-7% over 3 years
- Cost: $10-$30/month (generic)
- Best for: Patients who can follow strict dosing requirements
Risedronate (Actonel):
- Dosing: 35mg once weekly or 150mg once monthly
- Administration: Similar to alendronate but 30-minute wait
- Efficacy: Comparable to alendronate
- Advantage: May have slightly better gastrointestinal tolerability
Ibandronate (Boniva):
- Dosing: 150mg once monthly or 3mg IV every 3 months
- Hip data: Less robust than alendronate/risedronate
- Best for: Patients wanting less frequent dosing
Zoledronic Acid (Reclast):
- Dosing: 5mg IV infusion once yearly
- Administration: 15-minute infusion in clinic
- Efficacy: Superior adherence due to annual dosing
- Cost: $1,200-$2,000/infusion
- Best for: Patients with absorption issues or poor oral medication adherence
Managing Bisphosphonate Side Effects
David, age 62, stopped his alendronate after two weeks due to heartburn. His doctor switched him to monthly risedronate taken with dinner (after a 4-hour fast), which he tolerated perfectly. Understanding side effect management prevents unnecessary treatment discontinuation.
Common Side Effects and Solutions:
Gastrointestinal Issues (10-20% of patients):
- Symptoms: Heartburn, nausea, abdominal pain
- Solutions: Switch to different bisphosphonate, try weekly vs. daily dosing, consider IV formulation
- Prevention: Strict adherence to dosing instructions, avoid NSAIDs when possible
Flu-Like Symptoms with IV Bisphosphonates (10-30% first infusion):
- Symptoms: Fever, muscle aches, fatigue lasting 2-3 days
- Solutions: Premedicate with acetaminophen, schedule on Friday for weekend recovery
- Note: Rarely occurs with subsequent infusions
Rare But Serious (Risk <1 in 10,000):
- Atypical femoral fractures (risk increases after 5+ years)
- Osteonecrosis of the jaw (mostly in cancer patients on high doses)
- Regular dental care and drug holidays mitigate these risks
Alternative Medications: When Bisphosphonates Aren’t Suitable
Approximately 20% of patients cannot tolerate or have contraindications to bisphosphonates. Modern alternatives provide excellent options.
Denosumab (Prolia):
Denosumab is a twice-yearly injection that works differently than bisphosphonates by targeting a protein called RANKL that signals bone destruction.
Key Features:
- Dosing: 60mg subcutaneous injection every 6 months
- Efficacy: Reduces spine fractures by 68%, hip fractures by 40%
- BMD gains: 9-13% at spine over 3 years
- Advantages: No GI side effects, no kidney restrictions
- Cautions: Cannot stop abruptly (risk of rebound vertebral fractures), requires calcium/vitamin D supplementation
Critical Denosumab Consideration: If you start denosumab, work with your doctor on a long-term plan. Stopping without transitioning to another medication can cause rapid bone loss and vertebral fractures within 6-12 months.
Anabolic Agents: Building New Bone
For patients with severe osteoporosis (T-score ≤-3.0), history of multiple fractures, or those who fracture despite bisphosphonate therapy, anabolic agents actively build new bone rather than just slowing loss.
Teriparatide (Forteo):
- Mechanism: Synthetic parathyroid hormone fragment
- Dosing: Daily subcutaneous injection for up to 2 years
- Efficacy: Reduces spine fractures by 65%, non-spine by 53%
- BMD gains: 9-13% at spine (superior to bisphosphonates)
- Cost: $3,500-$4,000/month
- Limitation: 2-year lifetime maximum use
Abaloparatide (Tymlos):
- Mechanism: PTH-related protein analog
- Dosing: Daily injection for up to 2 years
- Efficacy: Similar to teriparatide with fewer cardiac concerns
- Advantage: May have better non-vertebral fracture protection
Romosozumab (Evenity):
- Mechanism: Monoclonal antibody blocking sclerostin
- Unique feature: Both builds bone AND slows resorption simultaneously
- Dosing: Monthly injections for 12 months only
- Efficacy: Reduces spine fractures by 73%, hip by 38%
- BMD gains: 13% at spine in first year (fastest gains available)
- Caution: Cardiovascular warning—not for patients with MI/stroke in past year
- Cost: $4,000-$4,500/month
Anabolic Therapy Sequential Treatment:
Research from the Mayo Clinic emphasizes that anabolic agents must be followed by antiresorptive therapy (bisphosphonate or denosumab) to maintain gains. Without this, bone density improvements are lost within 1-2 years.
Recommended Sequence:
- Anabolic agent (1-2 years)
- Transition to bisphosphonate or denosumab
- Continue antiresorptive long-term
Medication Comparison Table
| Medication Class | Efficacy | Administration | Best Candidate | Major Considerations |
|---|---|---|---|---|
| Oral Bisphosphonates | ↑ BMD 5-7% | Weekly/monthly pills | Standard osteoporosis | GI side effects, strict dosing |
| IV Bisphosphonates | ↑ BMD 5-7% | Annual infusion | Poor adherence, GI issues | Flu-like symptoms first dose |
| Denosumab | ↑ BMD 9-13% | Injection every 6mo | Kidney disease, can’t take oral | Cannot stop abruptly |
| Teriparatide | ↑ BMD 9-13% | Daily injection x2yr | Severe osteoporosis, prior fracture | Expensive, time-limited |
| Romosozumab | ↑ BMD 13% | Monthly injection x1yr | Very severe, imminent fracture risk | CV warning, expensive |
Drug Holidays: When and Why
Long-term bisphosphonate use carries small risks of atypical fractures and jaw osteonecrosis. After 3-5 years of treatment, some patients may benefit from a “drug holiday.”
Guidelines for Drug Holidays:
Consider Drug Holiday After:
- 5 years of oral bisphosphonates OR
- 3 years of IV zoledronic acid
IF Patient Meets Low-Risk Criteria:
- T-score improved to ≥-2.5
- No fractures during treatment
- No new risk factors
Duration: Typically 1-3 years with monitoring
Continue Treatment Without Holiday If:
- T-score still ≤-2.5
- Prior hip or spine fracture
- New fractures during treatment
- High FRAX scores (hip ≥3%, major ≥20%)
What This Means For You: Modern osteoporosis medications are remarkably effective when properly selected and used. Working with your healthcare team to choose the right medication for your specific situation—and maintaining that treatment consistently—can reduce your fracture risk by 40-70%.
Proven Lifestyle Changes to Strengthen Your Bones
Nutrition for Bone Health: Beyond Calcium
When Robert, 66, was diagnosed with a T-score of -2.6, he assumed taking calcium supplements would fix everything. Six months later, his repeat labs showed he was still vitamin D deficient, and his dietary analysis revealed he was eating only 0.6g protein per kg body weight—far below the recommended amount for bone health.
Optimal bone nutrition requires a comprehensive approach that extends well beyond just calcium supplementation.
Calcium Requirements: Sources Beyond Dairy
According to the National Institutes of Health Office of Dietary Supplements, adults over 50 need 1,200mg of calcium daily for women and 1,000-1,200mg for men. However, more isn’t always better—excessive calcium intake (>2,000mg/day) may increase cardiovascular risks.
Best Calcium Sources (% Daily Value per serving):
Dairy Options:
- Plain yogurt (8oz): 400mg (31%)
- Milk (8oz): 300mg (23%)
- Swiss cheese (1oz): 220mg (17%)
- Cottage cheese (1 cup): 125mg (10%)
Non-Dairy Options:
- Fortified almond milk (8oz): 450mg (35%)
- Cooked collard greens (1 cup): 268mg (21%)
- Canned sardines with bones (3oz): 325mg (25%)
- Firm tofu (1/2 cup): 253mg (19%)
- Cooked kale (1 cup): 177mg (14%)
- White beans (1 cup): 161mg (12%)
Calcium Absorption Considerations:
Your body absorbs only 500mg of calcium at one time, making divided doses throughout the day more effective than a single large supplement. Additionally, calcium carbonate requires stomach acid for absorption (take with meals), while calcium citrate absorbs well regardless of food intake.
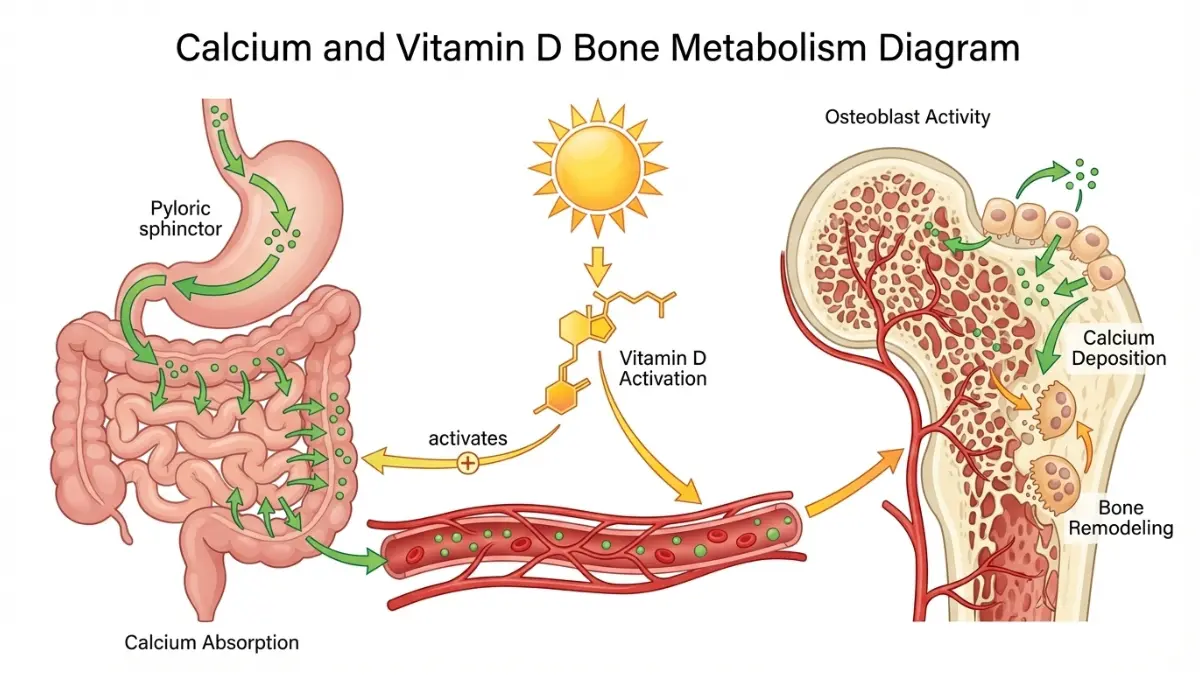
Vitamin D Optimization: The Critical Co-Factor
Vitamin D deficiency affects an estimated 40% of Americans and directly impairs calcium absorption, regardless of intake. Studies from Harvard School of Public Health demonstrate that optimal vitamin D levels (30-50 ng/mL) significantly reduce fracture risk.
Vitamin D Testing and Targets:
- Test: 25-hydroxyvitamin D blood test
- Deficient: <20 ng/mL
- Insufficient: 20-29 ng/mL
- Optimal: 30-50 ng/mL
- Upper safe limit: <100 ng/mL
Vitamin D Sources:
Sunlight Synthesis:
- 10-30 minutes of midday sun exposure on arms/legs 2-3x/week
- Varies by latitude, skin tone, season
- Less effective north of 37°N latitude (San Francisco, Richmond VA) from November-March
Dietary Sources:
- Salmon, wild (3oz): 570 IU
- Fortified milk (8oz): 100 IU
- Fortified orange juice (8oz): 100 IU
- Egg yolk: 40 IU
Supplementation:
- Most patients need 1,000-2,000 IU daily
- Some require 4,000-5,000 IU to reach optimal levels
- Always test before high-dose supplementation
Protein Intake: The Forgotten Bone Builder
Protein comprises 50% of bone volume and approximately 30% of bone mass. Inadequate protein intake accelerates bone loss and impairs fracture healing. Research published by Tufts University shows that adults over 50 should consume 1.0-1.2g protein per kg body weight daily for bone health.
Protein Calculation Example:
- Person weighing 150 lbs (68 kg)
- Target: 68-82g protein daily
- Use a protein intake calculator to determine your personalized needs
High-Quality Protein Sources:
- Chicken breast (3oz): 26g
- Greek yogurt (6oz): 17g
- Salmon (3oz): 22g
- Lentils (1 cup): 18g
- Eggs (2 large): 12g
- Quinoa (1 cup): 8g
Foods That Help vs. Harm Bone Density
Bone-Supportive Foods:
- Leafy greens (vitamin K)
- Fatty fish (vitamin D, omega-3s)
- Nuts and seeds (magnesium, zinc)
- Prunes (boron, vitamin K)
- Berries (antioxidants)
Foods to Limit:
High Sodium (>2,300mg/day):
- Increases calcium excretion in urine
- Each 2,300mg sodium causes ~40mg calcium loss
Excessive Caffeine (>4 cups coffee/day):
- May increase calcium excretion
- Effect neutralized by adequate calcium intake
Foods High in Oxalic Acid:
- Spinach (ironically high in calcium but poorly absorbed)
- Swiss chard
- Rhubarb
- Better alternatives: kale, collards, bok choy
Excessive Alcohol (>2 drinks/day):
- Interferes with vitamin D metabolism
- Increases fall risk
- Directly toxic to bone-forming cells
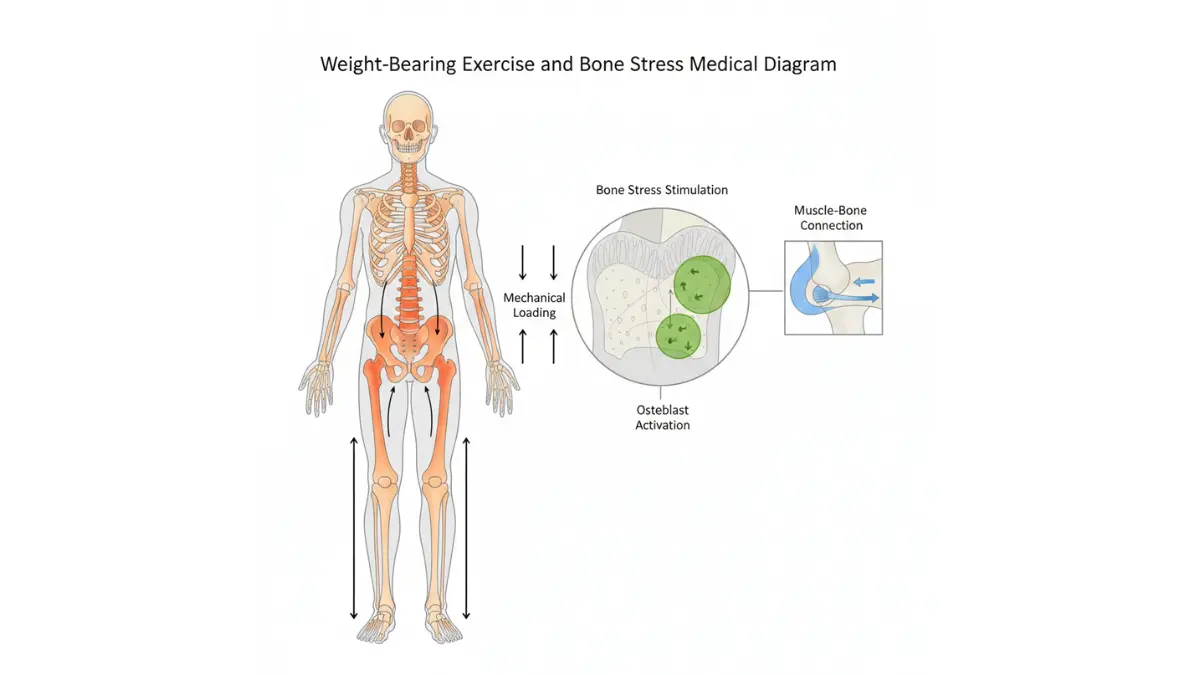
Weight-Bearing Exercise That Builds Bone
Exercise is non-negotiable for bone health. However, not all exercise equally benefits bones. Swimming and cycling, while excellent for cardiovascular fitness, provide minimal bone-building stimulus because they’re non-weight-bearing.
Evidence-Based Exercise Prescription:
According to CDC guidelines, bone-building exercise must be:
- Weight-bearing: Your bones support your body weight
- High-impact or moderate-impact: Provides bone-loading stimulus
- Progressive: Gradually increases intensity
- Consistent: At least 3-4x per week
Optimal Exercise Types:
High-Impact (if no prior fractures and doctor-approved):
- Jogging or running
- Jumping exercises
- Dance fitness
- Tennis
- Basketball
Moderate-Impact (suitable for most osteoporosis patients):
- Brisk walking
- Stair climbing
- Elliptical machine
- Low-impact aerobics
- Dancing
Resistance Training (Essential—2-3x/week):
- Squats
- Lunges
- Deadlifts (with proper form)
- Chest press
- Rows
- Overhead press
Weekly Exercise Schedule Example:
| Day | Activity | Duration | Bone Benefit |
|---|---|---|---|
| Monday | Brisk walking + resistance training | 30min + 30min | High |
| Tuesday | Balance exercises | 20min | Fall prevention |
| Wednesday | Brisk walking | 40min | Moderate |
| Thursday | Resistance training | 45min | High |
| Friday | Rest or gentle yoga | 30min | Recovery |
| Saturday | Stair climbing + walking | 45min | Moderate-High |
| Sunday | Recreation activity | 30-60min | Variable |
Exercises to Avoid:
According to the National Osteoporosis Foundation, patients with osteoporosis should avoid:
- High-impact activities if you have vertebral fractures
- Excessive forward spine flexion (toe touches, sit-ups)
- Twisting at the waist with resistance
- Trampolines or activities with fall risk
Balance and Fall Prevention Exercises
Falls cause 90% of hip fractures in people with osteoporosis. Balance training reduces fall risk by 24-35% according to research. Similar to how maintaining overall fitness through proper caloric balance supports health, balance work protects against the consequences of osteoporosis.
Daily Balance Routine (10 minutes):
Single-Leg Stands:
- Hold 30 seconds each leg
- Progress to eyes closed
- Repeat 3 times
Heel-to-Toe Walk:
- Walk straight line, heel touching toe
- 20 steps forward
- 2-3 repetitions
Chair Stands:
- Stand up from chair without using hands
- 10-15 repetitions
- Strengthens legs for stability
Tai Chi:
- Proven 47% reduction in falls
- Improves balance, coordination, confidence
Lifestyle Factors: Smoking, Alcohol, and Sleep
Smoking Cessation:
Smoking directly damages bone cells and impairs healing. Studies show smokers have 30-40% higher fracture rates and slower healing. Every cigarette reduces bone blood flow for 30-90 minutes.
Benefits of Quitting:
- Fracture risk begins declining within 6 months
- Bone formation improves progressively
- Returns to near-normal risk after 5-10 years
Alcohol Limits:
- Women: Maximum 1 drink/day
- Men: Maximum 2 drinks/day
- Heavy drinking (>3 drinks/day) increases fracture risk by 68%
Sleep and Bone Health:
Poor sleep disrupts bone remodeling hormones and increases fall risk. Aim for 7-9 hours nightly. Consider using a sleep calculator to optimize your sleep schedule for recovery and bone healing.
What This Means For You: Lifestyle modifications aren’t optional additions to medication—they’re foundational. The good news: every positive change you make compounds. Within 3-6 months of comprehensive lifestyle optimization, most patients report feeling stronger, more confident in movement, and empowered in their bone health journey.
Living Successfully with Osteoporosis
Home Safety Modifications to Prevent Falls
Falls represent the most immediate threat to people with osteoporosis. A comprehensive home safety assessment can reduce fall risk by 35-40% according to CDC fall prevention data.
Room-by-Room Safety Checklist:
Bathroom (Highest Risk Area):
- Install grab bars in shower/tub and near toilet
- Use non-slip mats in tub/shower
- Ensure adequate lighting (nightlight for evening)
- Remove floor rugs or secure with non-slip backing
- Keep towel bars separate from grab bars (weight-bearing difference)
- Consider raised toilet seat for easier standing
Bedroom:
- Position bed at proper height (feet touch floor when sitting)
- Keep pathway to bathroom clear and lit
- Install nightlights along walking path
- Secure or remove bedside rugs
- Use bed rails if balance is compromised
- Keep phone and flashlight within reach
Kitchen:
- Store frequently used items at waist-to-shoulder height
- Use non-slip floor mats
- Clean spills immediately
- Use step stool with handrail (never chair)
- Adequate lighting over work areas
- Avoid floor wax or polish that creates slippery surfaces
Living Areas:
- Remove throw rugs or secure firmly
- Ensure all walking paths are 36 inches wide
- Secure electrical cords against walls
- Remove low furniture and clutter
- Arrange furniture for clear pathways
- Install adequate lighting (especially stairs)
Stairways:
- Install sturdy handrails on both sides
- Ensure adequate lighting (top and bottom switches)
- Add non-slip treads to each step
- Paint edge of top step in contrasting color
- Never place objects on stairs
- Consider stairlift if stairs become too risky
Outdoor Spaces:
- Repair uneven walkways and cracked pavement
- Install handrails on all steps and porches
- Ensure adequate exterior lighting
- Remove ice and snow immediately
- Wear proper footwear (rubber soles, low heels)
- Consider motion-sensor lights
When to Repeat DEXA Scans
DEXA scan timing balances the need to monitor treatment effectiveness against the precision limitations of the test. The smallest change that exceeds measurement error is approximately 3-5% at most centers.
DEXA Scan Schedule:
| Clinical Situation | Timing | Rationale |
|---|---|---|
| Starting new medication | 1-2 years | Assess treatment response |
| Stable on long-term treatment | Every 2 years | Monitor maintenance |
| Treatment change | 1 year | Evaluate new medication |
| High fracture risk | Annually | Close monitoring |
| Drug holiday consideration | Before holiday, then 1-2 years | Safety assessment |
| Post-fracture | 1 year | Evaluate treatment intensification |
Interpreting Follow-Up Scans:
Successful Treatment:
- Stable BMD (no further loss)
- BMD increase of 3-10%
- No new fractures
Inadequate Response:
- BMD decline >3-5%
- New fragility fracture
- Triggers medication change or investigation
Martha, diagnosed at age 61 with a T-score of -2.7, followed her treatment plan diligently. Her 2-year follow-up scan showed improvement to -2.3—a 6% increase in spine BMD. This validated her consistent bisphosphonate therapy, calcium intake, and exercise regimen.
Tracking Your Progress: What Metrics Matter
Monitoring Checklist:
Monthly:
- Medication adherence tracking
- Falls or near-falls log
- Pain or new symptoms
- Exercise consistency
Every 3-6 Months:
- Clinical check-in with provider
- Weight assessment
- Blood work if indicated
- Side effect evaluation
Annually:
- Comprehensive bone health assessment
- Review treatment plan
- Update fracture risk assessment
- Dental examination
Every 1-2 Years:
- DEXA scan
- Vitamin D level check
- Medication regimen review
Managing Fear and Anxiety About Fractures
The psychological impact of an osteoporosis diagnosis cannot be understated. Studies show that 40-60% of patients develop some degree of kinesiophobia (fear of movement) after diagnosis, which paradoxically increases fall risk by reducing activity levels and muscle strength.
Strategies to Manage Fracture Anxiety:
1. Education Reduces Fear: Understanding that treatment dramatically reduces risk (by 40-70%) helps contextualize the diagnosis. You’re not fragile; you’re managing a treatable condition.
2. Confidence-Building Exercise: Working with a physical therapist to learn safe movement patterns rebuilds confidence. Many patients report that supervised exercise reduces anxiety more than any other intervention.
3. Focus on What You Control:
- Daily medication adherence
- Nutritious eating
- Regular exercise
- Home safety improvements
- Social connections
4. Professional Support When Needed: If anxiety interferes with daily life, consider speaking with a therapist. Cognitive-behavioral therapy has proven particularly effective for health-related anxiety.
5. Connect With Others: Support groups (in-person or online) connect you with people managing similar challenges. The National Osteoporosis Foundation offers resources for finding local support groups.
Sexual Health and Intimacy Considerations
Many patients hesitate to discuss how osteoporosis affects intimate relationships, but these concerns are valid and addressable. Fear of fracture during sexual activity affects 30-40% of people with osteoporosis.
Practical Guidance:
Communication is Essential:
- Discuss concerns openly with your partner
- Explain what movements cause discomfort
- Explore positions that minimize stress on vulnerable areas
Modifications for Spine Protection:
- Avoid excessive flexion (forward bending)
- Use pillows for support
- Consider positions that minimize spinal twisting
- Side-lying positions often work well
When to Seek Medical Guidance:
- Persistent pain during intimacy
- Severe anxiety affecting relationships
- Questions about specific limitations
- Need for professional counseling
Healthcare providers recognize these concerns as legitimate and can provide practical, personalized guidance.
Travel and Activity Modifications
Having osteoporosis doesn’t mean giving up travel or hobbies—it means being thoughtful about preparations.
Travel Safety Tips:
Before Travel:
- Bring adequate medication supply (plus extra)
- Pack vitamin supplements
- Wear supportive, rubber-soled shoes
- Research medical facilities at destination
- Carry medication list and doctor contact
During Travel:
- Use luggage with wheels
- Request wheelchair assistance at airports if needed
- Stay hydrated (bone health connection)
- Maintain medication schedule across time zones
- Be cautious on unfamiliar terrain
Activity Modifications:
- Golf: Use cart instead of walking entire course
- Gardening: Use raised beds, knee pads, proper tools
- Hiking: Choose established trails, use trekking poles
- Swimming: Excellent low-impact exercise
- Biking: Consider stationary bike (less fall risk)
Building Your Support System
Successful long-term osteoporosis management requires a team approach. Understanding how different specialists contribute helps you build the right support network, much like how patients benefit from comprehensive approaches to other complex health conditions.
Your Osteoporosis Care Team:
Primary Care Physician:
- Coordinates overall care
- Prescribes and monitors medications
- Orders follow-up testing
- Manages related health conditions
Endocrinologist:
- Manages complex cases
- Evaluates secondary causes
- Optimizes hormonal factors
- Guides treatment transitions
Physical Therapist:
- Designs safe exercise programs
- Teaches proper body mechanics
- Improves balance and strength
- Reduces fall risk
Registered Dietitian:
- Optimizes nutritional intake
- Plans calcium/vitamin D sources
- Addresses dietary restrictions
- Monitors protein adequacy
Pharmacist:
- Reviews medication interactions
- Provides dosing guidance
- Manages side effects
- Ensures proper administration
Occupational Therapist:
- Home safety assessment
- Adaptive equipment recommendations
- Activity modification strategies
- Energy conservation techniques
Insurance Navigation and Financial Assistance
Medicare Coverage Specifics:
- Part B covers DEXA scans (80% after deductible)
- Part D covers oral medications
- Part B covers injectable/infused medications (80%)
- Extra Help available for low-income beneficiaries
Manufacturer Assistance Programs:
- Most drug manufacturers offer patient assistance
- Income-based eligibility
- Can reduce costs significantly
- Contact drug manufacturer directly or ask pharmacist
Generic Options:
- Generic alendronate: $10-$30/month
- Generic risedronate: $15-$40/month
- Generic ibandronate: $20-$50/month
What This Means For You: Living well with osteoporosis means integrating bone health into your daily life without letting it define you. With proper modifications, support systems, and consistent management, most people maintain active, fulfilling lives while significantly reducing fracture risk.
Advanced Insights and Special Considerations
Secondary Osteoporosis: When Other Conditions Are to Blame
Approximately 30% of postmenopausal women and 50-80% of men with osteoporosis have secondary causes contributing to bone loss. Identifying these conditions is critical because treating the underlying cause often improves bone density more effectively than osteoporosis medications alone.
Common Secondary Causes:
Endocrine Disorders:
- Hyperthyroidism (increases bone turnover)
- Hyperparathyroidism (mobilizes calcium from bone)
- Cushing’s syndrome (excess cortisol)
- Hypogonadism (low sex hormones)
- Type 1 diabetes (impaired bone formation)
Gastrointestinal Conditions:
- Celiac disease (calcium malabsorption)
- Inflammatory bowel disease (Crohn’s, ulcerative colitis)
- Post-gastric bypass surgery
- Chronic liver disease
Kidney Disease:
- Chronic kidney disease stage 3-5
- Kidney stones with hypercalciuria
Rheumatologic Conditions:
- Rheumatoid arthritis
- Systemic lupus erythematosus
- Ankylosing spondylitis
Medication-Induced:
- Glucocorticoids (>5mg prednisone for >3 months)
- Aromatase inhibitors (breast cancer treatment)
- Androgen deprivation therapy (prostate cancer)
- Some seizure medications
- Proton pump inhibitors (long-term, high-dose)
- Selective serotonin reuptake inhibitors
Red Flags for Secondary Osteoporosis:
- Osteoporosis in men under 50
- Premenopausal women with fragility fractures
- T-score <-3.0 without obvious risk factors
- Rapid bone loss (>3-5% per year)
- Elevated bone turnover markers
- Abnormal lab values (calcium, PTH, vitamin D, TSH)
Osteoporosis in Men: Different Considerations
Men represent 20-25% of osteoporosis cases but suffer disproportionately higher mortality rates after hip fracture (30% vs. 17% in women). Unfortunately, men are vastly underdiagnosed and undertreated.
Unique Considerations in Men:
Secondary Causes More Common:
- 50-80% of male osteoporosis has identifiable secondary cause
- Hypogonadism (low testosterone) affects 30-40%
- Alcohol abuse more frequent contributor
- Glucocorticoid use more common
Different Fracture Patterns:
- Hip fractures occur 5-10 years later than in women
- Higher vertebral fracture rate than recognized
- Often more severe when fractures occur
Testosterone and Bone Health:
Low testosterone contributes to male osteoporosis, but testosterone replacement’s bone benefits remain controversial. According to National Institute on Aging research, testosterone therapy may benefit men with symptomatic hypogonadism, but risks must be carefully weighed.
Treatment Considerations:
- Bisphosphonates equally effective in men
- Less data on other medications in male populations
- Address underlying causes (especially testosterone, alcohol)
- Resistance exercise particularly important
Premenopausal Women and Younger Adults
Osteoporosis in premenopausal women or young adults always warrants investigation for secondary causes. Normal aging doesn’t explain bone loss in these populations.
Common Causes in Younger Patients:
Women:
- Amenorrhea or irregular periods (low estrogen)
- Eating disorders (anorexia nervosa, bulimia)
- Female athlete triad (energy deficit, amenorrhea, bone loss)
- Celiac disease
- Inflammatory bowel disease
- Pregnancy and lactation-associated osteoporosis (rare)
Both Sexes:
- Genetic disorders (osteogenesis imperfecta, Ehlers-Danlos)
- Cystic fibrosis
- Inflammatory conditions
- Malabsorption syndromes
- Medication effects
- Idiopathic juvenile osteoporosis
Treatment Cautions: Most osteoporosis medications haven’t been extensively studied in premenopausal women due to pregnancy concerns. Bisphosphonates remain in bone for years, raising theoretical fetal risks. Treatment focuses on:
- Correcting underlying causes
- Optimizing calcium, vitamin D, protein
- Weight-bearing exercise
- Addressing amenorrhea/hypogonadism
- Medication only for severe cases or high fracture risk
Chronic Kidney Disease and Bone Health
Chronic kidney disease (CKD) creates complex bone metabolism disorders. As kidney function declines, phosphate retention and vitamin D deficiency trigger secondary hyperparathyroidism, leading to unique bone problems distinct from typical osteoporosis.
CKD-Mineral Bone Disorder (CKD-MBD):
Patients with CKD stages 3-5 develop abnormal calcium, phosphate, parathyroid hormone, and vitamin D metabolism. This causes:
- Bone disease (renal osteodystrophy)
- Vascular calcification
- Increased fracture risk
- Increased cardiovascular risk
Treatment Considerations:
- Standard DEXA T-scores less reliable in CKD
- Bisphosphonates contraindicated in advanced CKD (GFR <30)
- Denosumab can be used with caution (hypocalcemia risk)
- Phosphate binders often needed
- Active vitamin D analogs replace standard vitamin D
Management requires nephrology consultation to balance bone health with other CKD complications.
Medication-Induced Bone Loss: Glucocorticoids
Glucocorticoid-induced osteoporosis (GIOP) represents the most common cause of secondary osteoporosis. Even moderate doses (≥5mg prednisone daily) cause rapid bone loss, with most damage occurring in the first 6-12 months.
Glucocorticoid Effects on Bone:
- Decreases bone formation
- Increases bone resorption
- Reduces calcium absorption
- Increases urinary calcium loss
- Reduces sex hormone production
- Causes muscle weakness (increases falls)
Prevention Strategies:
For All Patients Starting Glucocorticoids:
- Use lowest effective dose
- Consider alternate-day dosing when possible
- Inhaled glucocorticoids (asthma) less problematic
- Optimize calcium (1,200mg) and vitamin D (800-1,000 IU)
- Initiate weight-bearing exercise
- Assess baseline fracture risk
Medication Prevention: According to American College of Rheumatology guidelines, consider bisphosphonates or denosumab for patients:
- Taking ≥7.5mg prednisone for ≥3 months
- Age >40 with moderate fracture risk
- Any age with prior fracture
- Postmenopausal women or men >50 on any dose
Emerging Treatments and Clinical Trials
Bone research continues advancing, with several promising treatments in development.
2024-2025 Research Highlights:
Novel Medications in Development:
- Abaloparatide transdermal patch (avoiding daily injections)
- Combination anabolic/antiresorptive therapies
- Cathepsin K inhibitors (more selective bone protection)
- Extended-release formulations
Technology Advances:
- High-resolution peripheral quantitative CT (HR-pQCT) for bone microarchitecture assessment
- Artificial intelligence prediction models for fracture risk
- Wearable technology for fall detection and prevention
- Bone turnover marker optimization for treatment guidance
Emerging Understanding:
- Gut microbiome influence on bone health
- Senescent cell removal (senolytics) for bone aging
- Mechanical loading optimization studies
- Personalized medicine approaches based on genetics
Latest Research Findings (2024-2025)
Key 2024 Publications:
Research from the National Osteoporosis Foundation in 2024 confirmed that sequential anabolic-then-antiresorptive therapy provides superior fracture prevention compared to bisphosphonates alone for severe osteoporosis—fracture reduction improved from 40% to 68%.
Protein and Bone Health Study (2024): A large prospective cohort study demonstrated that protein intake >1.2g/kg body weight in older adults reduced hip fractures by 23% compared to intake <0.8g/kg, independent of calcium intake.
Exercise Intensity Research (2025): New data suggests that progressive resistance training with loads 70-80% of one-repetition maximum provides superior bone density improvements compared to lower intensities, though both benefit balance and fall prevention.
Vitamin K2 Emerging Data: While vitamin K1 (leafy greens) is well-established for bone health, vitamin K2 (fermented foods, natto) shows promise for directing calcium to bones rather than arteries, though more research is needed.
What the Future Holds: New Treatment Modalities
The next decade promises exciting advances in osteoporosis management:
Personalized Medicine:
- Genetic testing to predict fracture risk
- Identification of treatment responders vs. non-responders
- Targeted therapies based on specific bone metabolism patterns
Less Frequent Dosing:
- Annual or less frequent medication administration
- Long-acting formulations improving adherence
Combination Therapies:
- Simultaneous anabolic and antiresorptive treatment
- Synergistic approaches for maximum benefit
Regenerative Medicine:
- Stem cell therapies for bone regeneration
- Gene therapy approaches
- Tissue engineering for severe cases
What This Means For You: Understanding special circumstances ensures you receive appropriate, personalized care. Whether you have secondary causes, are younger than typical osteoporosis patients, or have complicated medical conditions, modern medicine offers increasingly sophisticated approaches to protect your bone health.
Frequently Asked Questions (FAQs) about T-score
1. Can I reverse a T-score of -2.5 back to normal?
While complete reversal to normal bone density is uncommon, significant improvements are possible. Most patients on treatment can expect 5-13% bone density increases over 2-3 years, which might improve a T-score from -2.5 to -2.1 or -2.2. This represents meaningful fracture risk reduction. Focus on stabilization and risk reduction rather than achieving normal T-scores.
2. How long will I need to take osteoporosis medication?
Treatment duration varies by medication and individual circumstances. Bisphosphonates typically continue for 3-5 years before considering a drug holiday. Denosumab usually continues indefinitely as stopping causes rapid bone loss. Anabolic agents are limited to 1-2 years, followed by transition to antiresorptive therapy. Your doctor reassesses treatment needs based on follow-up scans and fracture risk.
3. Will I definitely break a bone with a -2.5 T-score?
No. A T-score of -2.5 increases fracture risk but doesn’t guarantee a fracture will occur. Your absolute risk depends on multiple factors including age, prior fractures, medications, and lifestyle. With appropriate treatment, you can reduce fracture risk by 40-70%. Many patients with osteoporosis never experience fractures.
4. Can I still exercise if I have osteoporosis?
Yes—exercise is essential for bone health. Weight-bearing and resistance exercises strengthen bones and muscles while improving balance. Avoid high-impact activities if you have spine fractures, and skip exercises involving excessive forward bending or twisting. Work with a physical therapist to develop a safe, effective program.
5. What’s the difference between -2.4 and -2.5 T-score?
Clinically, the difference is minimal. The -2.5 cutoff represents a somewhat arbitrary threshold where fracture risk becomes high enough to warrant medical treatment. A T-score of -2.4 is osteopenia (low bone mass), while -2.5 is osteoporosis. Your doctor considers overall fracture risk using FRAX scores, not just T-scores, when making treatment decisions.
6. Do I need medication if my T-score is exactly -2.5?
Usually yes, especially for postmenopausal women and men over 50. However, the decision considers your entire clinical picture: age, prior fractures, family history, medications, and calculated fracture risk. Some patients with -2.5 T-scores but very low FRAX scores might start with lifestyle modifications and close monitoring rather than immediate medication.
7. How often should I get rescanned?
Typically every 1-2 years initially when starting or changing treatment, then every 2 years once stable on therapy. More frequent scanning doesn’t provide additional useful information due to the test’s precision limitations. Your doctor schedules scans based on your specific treatment plan and risk factors.
8. Can diet alone improve my T-score?
Diet alone rarely improves T-scores significantly, though it may prevent further bone loss. Optimal nutrition (adequate calcium, vitamin D, protein) combined with exercise provides the foundation, but patients with T-scores of -2.5 typically need medication to actively rebuild bone density and reduce fracture risk meaningfully.
9. What if I can’t tolerate bisphosphonates?
Multiple alternatives exist. Denosumab injections work differently and avoid gastrointestinal side effects. IV bisphosphonates bypass the stomach entirely. For severe cases, anabolic agents like teriparatide or romosozumab offer excellent options. Work with your doctor to find a medication you can tolerate—effective treatment options exist for virtually every patient.
10. Does osteoporosis mean I’m aging faster?
Osteoporosis represents accelerated bone aging, but it doesn’t reflect overall body aging. Many people with osteoporosis remain otherwise healthy and active. Think of it as one system requiring extra attention, similar to someone needing glasses—it’s a specific condition requiring management, not a sign of general decline.
11. Will my children inherit osteoporosis?
Genetics influence bone density, but heredity isn’t destiny. Children of parents with osteoporosis have modestly increased risk, but lifestyle factors (nutrition, exercise, avoiding smoking) substantially influence outcomes. Encourage your children to build strong bones during childhood and young adulthood through calcium-rich diets and weight-bearing activities. Peak bone mass in the 20s-30s largely determines later osteoporosis risk.
Final Thoughts: Your Path Forward
Receiving a T-score of -2.5 marks a critical turning point—not an endpoint. Modern osteoporosis treatment is remarkably effective, reducing fracture risk by 40-70% when patients remain engaged with their care plan.
Your immediate priorities are simple but powerful:
- Understand your complete fracture risk through FRAX calculation and discussion with your healthcare team
- Start appropriate treatment within 30 days of diagnosis
- Optimize nutrition with adequate calcium, vitamin D, and protein
- Engage in regular weight-bearing and resistance exercise at least 3-4 times weekly
- Modify your home environment to prevent falls
- Monitor progress through follow-up testing and ongoing communication with your care team
Remember: osteoporosis is a treatable condition. With consistent management, most patients maintain active, fulfilling lives while significantly reducing fracture risk. You’ve taken the essential first step by seeking information—now continue forward with confidence, knowing that effective treatments and supportive healthcare providers are ready to guide you.
Take action today. Your bones—and your future self—will thank you.
Medical Disclaimer: This article provides educational information about osteoporosis management and should not replace professional medical advice. Always consult qualified healthcare providers for diagnosis, treatment decisions, and personalized medical guidance specific to your individual health circumstances.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.