On This Page – Quick Medical Summary
Meet Emily, a 38-year-old marketing executive who discovered something unsettling during her annual physical. Her TSH test came back at 3.8 mIU/L—technically “normal” according to standard lab ranges. Yet she felt exhausted, gained 12 pounds despite exercising regularly, and struggled with concentration. Her doctor dismissed her concerns, saying her thyroid was fine. But was it really?
Here’s what you need to know right now: The normal TSH range for adults is 0.4 to 4.0 mIU/L, but groundbreaking 2023 research involving 134,346 participants reveals that optimal TSH levels for cardiovascular health fall between 1.5 and 2.8 mIU/L (the 60-80th percentile). This means millions of Americans with “normal” results may not be functioning at their healthiest levels.
Quick Reference: TSH Ranges at a Glance
| TSH Level (mIU/L) | Status | Action Needed |
|---|---|---|
| Below 0.4 | Low (Hyperthyroidism) | Medical evaluation required |
| 0.4 – 1.5 | Normal (Lower range) | Monitor if symptomatic |
| 1.5 – 2.8 | Optimal for heart health | Ideal target range |
| 2.8 – 4.0 | Normal (Upper range) | Consider optimization |
| 4.0 – 10.0 | Subclinical hypothyroidism | Individual assessment needed |
| Above 10.0 | Overt hypothyroidism | Treatment typically recommended |
TSH, or thyroid-stimulating hormone, acts as your body’s thermostat for metabolism. Produced by your pituitary gland, TSH tells your thyroid how much hormone to make. When thyroid hormone levels drop, TSH rises to stimulate more production. When levels are too high, TSH decreases. This feedback loop keeps your metabolism balanced—affecting everything from heart rate to body temperature, weight, and energy levels.
Why this matters now: Unlike other medical tests where “normal” equals healthy, TSH reference ranges have been based purely on statistical distribution rather than health outcomes. Recent evidence from multiple international studies published in The Lancet Diabetes & Endocrinology suggests we may need to rethink what “optimal” really means for long-term cardiovascular health and mortality risk.
Understanding your TSH levels can be life-changing. Whether you’re experiencing unexplained symptoms, managing a known thyroid condition, or simply want to optimize your health, this comprehensive guide will help you interpret your results and take informed action.
Medical Disclaimer: This article provides educational information about TSH levels and thyroid health. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your healthcare provider about your specific TSH levels and treatment options.
Comprehensive TSH Levels Chart by Age & Condition
Standard TSH Reference Ranges by Age Group
TSH levels naturally change throughout life, with newborns having significantly higher levels that gradually decrease into adulthood. According to data from the National Institute of Diabetes and Digestive and Kidney Diseases, understanding age-appropriate ranges is crucial for accurate diagnosis.

| Age Group | Normal TSH Range (mIU/L) | Clinical Notes |
|---|---|---|
| Newborns (0-5 days) | 0.7 – 15.2 | Elevated at birth, drops rapidly |
| Infants (6-90 days) | 0.72 – 11.0 | Continues to normalize |
| Babies (4-12 months) | 0.73 – 8.35 | Approaching childhood levels |
| Children (1-6 years) | 0.7 – 5.97 | Stable pediatric range |
| Children (7-11 years) | 0.6 – 4.84 | Pre-adolescent levels |
| Adolescents (12-20 years) | 0.51 – 4.3 | Adult-like ranges emerging |
| Adults (21-79 years) | 0.4 – 4.0 | Standard reference range |
| Elderly (80+ years) | 0.5 – 6.0 | Age-related increase accepted |
The upper limit of normal increases with age, particularly after 60. Research published by Johns Hopkins School of Medicine suggests that what’s considered “high” for a 30-year-old may be physiologically normal for an 80-year-old.
The Optimal Health Range: What 2023 Research Reveals
This is where conventional medicine is being revolutionized. A massive meta-analysis published in The Lancet tracked 134,346 participants for an average of 11.5 years, examining the relationship between TSH levels and cardiovascular disease mortality. The findings challenge everything we thought we knew about “normal” thyroid function.
Groundbreaking Discovery: The study divided normal TSH ranges into percentiles and found that individuals with TSH in the 60-80th percentile (approximately 1.5-2.8 mIU/L) had the lowest risk of cardiovascular events and death. Those in the upper range—even within “normal” limits—faced significantly increased risks.
| TSH Percentile | Approximate TSH (mIU/L) | 10-Year Cardiovascular Risk |
|---|---|---|
| 20-40th (Optimal Free T4) | 1.3 – 1.9 | Lowest baseline risk |
| 60-80th (Optimal TSH) | 1.5 – 2.8 | Lowest risk zone |
| 80-100th (High-normal TSH) | 2.8 – 4.0+ | 34% increased mortality risk |
| 0-20th (Low TSH) | Below 1.0 | 20% increased cardiac death |
What this means clinically: Having a TSH of 3.8 mIU/L—like Emily from our opening story—places you in the 80-100th percentile, associated with a 34% higher risk of all-cause mortality and 57% higher risk of cardiovascular death compared to the optimal range. For women over 70, having free T4 above the 85th percentile increased absolute 10-year cardiovascular risk by more than 5%.
TSH Levels During Pregnancy: Trimester-Specific Guidelines
Pregnancy dramatically affects thyroid function due to rising levels of human chorionic gonadotropin (hCG), which stimulates the thyroid gland. According to the American Thyroid Association, maintaining optimal TSH levels is critical for fetal brain development.
| Trimester | TSH Range (mIU/L) | Why It Changes |
|---|---|---|
| First (0-12 weeks) | 0.18 – 2.99 | hCG stimulation lowers TSH |
| Second (13-26 weeks) | 0.11 – 3.98 | Gradual normalization |
| Third (27-40 weeks) | 0.48 – 4.71 | Returns toward baseline |
Women with hypothyroidism typically need to increase their levothyroxine dose by 30-50% during pregnancy. If you’re planning to conceive, aim for TSH below 2.5 mIU/L before conception. Use our pregnancy due date calculator and fetal growth percentile calculator to track your pregnancy alongside thyroid monitoring.
Special Populations: When Standard Ranges Don’t Apply
Certain medical conditions and treatments require different TSH targets. The Cleveland Clinic Endocrinology Department provides specific guidance for these situations:
Thyroid Cancer Survivors: TSH suppression therapy keeps levels between 0.1-0.5 mIU/L to prevent cancer recurrence by minimizing thyroid stimulation.
Patients on Thyroid Hormone Replacement: Target range is 0.5-3.0 mIU/L, narrower than the general population to ensure adequate replacement without overtreatment.
Elderly Patients (65+): Mild TSH elevation (4.0-6.0 mIU/L) may not require treatment if asymptomatic. Recent guidelines suggest using “age divided by 10” as the upper TSH limit in mIU/L (e.g., 7.0 for a 70-year-old).
Subclinical Hypothyroidism: TSH 4.5-10.0 mIU/L with normal free T4 requires individualized assessment. Treatment is typically recommended if TSH exceeds 10.0 mIU/L or if thyroid antibodies are positive.
Understanding Your TSH Test Results
What High TSH Levels Mean (Hypothyroidism)
When Maria, a 52-year-old teacher, finally got tested after months of fatigue, her TSH came back at 8.2 mIU/L. Her doctor diagnosed subclinical hypothyroidism and started her on levothyroxine. Within three months, her TSH dropped to 2.1 mIU/L, and she regained her energy, lost the 15 pounds she’d gained, and her brain fog lifted. Her story illustrates why understanding TSH severity matters.
High TSH indicates your thyroid isn’t producing enough hormone—a condition called hypothyroidism. Your pituitary gland responds by releasing more TSH, trying to stimulate the underperforming thyroid. The higher the TSH, the more severe the deficiency.
| TSH Level (mIU/L) | Classification | Free T4 Status | Typical Symptoms |
|---|---|---|---|
| 4.5 – 10.0 | Subclinical hypothyroidism | Normal | Mild fatigue, slight weight gain, cold sensitivity |
| 10.0 – 20.0 | Mild hypothyroidism | Low-normal to low | Above symptoms plus hair thinning, constipation, depression |
| 20.0 – 50.0 | Moderate hypothyroidism | Low | Above plus significant weight gain, severe fatigue, memory issues |
| Above 50.0 | Severe hypothyroidism | Very low | All above plus myxedema risk, muscle weakness, cognitive impairment |
Subclinical hypothyroidism deserves special attention. With TSH between 4.5-10.0 mIU/L but normal free T4 levels, you may have minimal symptoms or none at all. Research from the National Institutes of Health shows that 2-5% of people with subclinical hypothyroidism progress to overt disease annually, with the risk increasing if thyroid antibodies are present.
What Low TSH Levels Mean (Hyperthyroidism)
Low TSH indicates your thyroid is producing too much hormone—hyperthyroidism—so your pituitary gland shuts down TSH production to slow things down. This condition accelerates body functions, creating a cascade of symptoms that, if left untreated, can lead to serious complications like atrial fibrillation and osteoporosis.

| TSH Level (mIU/L) | Classification | Free T4/T3 Status | Key Symptoms |
|---|---|---|---|
| 0.1 – 0.4 | Subclinical hyperthyroidism | Normal | Mild anxiety, slight weight loss, increased heart rate |
| 0.01 – 0.1 | Mild hyperthyroidism | Elevated | Above plus tremors, insomnia, heat intolerance |
| Below 0.01 | Severe hyperthyroidism (suppressed) | Very high | Above plus significant weight loss, rapid heart rate, risk of thyroid storm |
According to data from the University of California San Francisco Medical Center, women over 60 with subclinical hyperthyroidism have triple the risk of developing atrial fibrillation compared to those with normal TSH.
When TSH Doesn’t Tell the Complete Story
TSH is highly sensitive, but it’s not infallible. Several conditions can produce misleading results, which is why endocrinologists often order additional tests like free T4, free T3, and thyroid antibodies. Understanding these scenarios prevents misdiagnosis and inappropriate treatment.
Central (Secondary) Hypothyroidism: Low TSH with low free T4 indicates a pituitary or hypothalamic problem rather than a thyroid issue. The pituitary fails to produce adequate TSH, so the thyroid doesn’t receive proper stimulation. This rare condition affects only 1 in 20,000-80,000 people according to Stanford Medicine.
T3 Thyrotoxicosis: Low TSH with normal free T4 but elevated free T3 can occur in early Graves’ disease or with toxic nodules. About 5% of hyperthyroid patients have this pattern.
Non-Thyroidal Illness Syndrome: Severe illness, fasting, or major surgery can temporarily suppress TSH without true thyroid dysfunction. TSH typically normalizes once the acute illness resolves.
Medication Interference: Biotin supplements (often in multivitamins and hair growth formulas) can falsely lower TSH results. Discontinue biotin 2-3 days before testing. Other medications affecting TSH include lithium, amiodarone, and high-dose glucocorticoids.
What This Means For You: If your TSH seems inconsistent with your symptoms, request a complete thyroid panel including free T4, free T3, thyroid peroxidase antibodies (TPO), and thyroglobulin antibodies. Consider using our symptom checker to document patterns before your doctor visit.
Cardiovascular & Mortality Risk—The Game-Changing Research
The Optimal TSH Sweet Spot for Longevity
For decades, doctors have treated thyroid function like a binary switch—either you’re hypothyroid (high TSH), hyperthyroid (low TSH), or normal. But what if “normal” isn’t good enough? A paradigm-shifting 2023 study published in The Lancet Diabetes & Endocrinology tracked over 134,000 adults for more than a decade, revealing that TSH levels within the traditional “normal” range have dramatically different implications for cardiovascular health and lifespan.
The research, conducted by the Thyroid Studies Collaboration and analyzed by researchers at Johns Hopkins Bloomberg School of Public Health, found a J-shaped curve for cardiovascular risk. Both very low and high-normal TSH levels increased mortality, with a clear “sweet spot” in the middle providing maximum protection.
The Optimal Zone: TSH levels between 1.5-2.8 mIU/L (the 60-80th percentile of normal range) were associated with the lowest risk of:
- Cardiovascular disease events (heart attack, stroke, heart failure)
- Cardiovascular mortality
- All-cause mortality over 10 years
Evidence Pyramid: Strength of TSH-Mortality Relationship
HIGHEST EVIDENCE
▲ Meta-analysis (134,346 participants)
▲▲ Multiple cohort studies
▲▲▲ Individual studies
▲▲▲▲ Expert opinion

| TSH Percentile | TSH Range (mIU/L) | 10-Year Composite Risk vs. Optimal |
|---|---|---|
| 60-80th (Optimal) | 1.5 – 2.8 | Baseline (lowest risk) |
| 80-100th (High-normal) | 2.8 – 4.0+ | +34% all-cause mortality, +57% CVD death |
| 40-60th | 1.0 – 1.5 | +8% increased risk |
| 0-20th (Low) | Below 1.0 | +20% CVD mortality, +9% all-cause death |
Age and Gender: Why Your Risk Profile Matters
The relationship between TSH and cardiovascular outcomes isn’t uniform across all populations. The same research revealed critical age and gender differences that should inform treatment decisions, particularly for older adults.
Women Over 70: Those with free T4 levels above the 85th percentile of normal range had an absolute 10-year cardiovascular risk exceeding 5%—a clinically significant threshold. High-normal thyroid hormone levels appear particularly dangerous in older women, potentially accelerating atherosclerosis and cardiac stress.
Men Over 70: Similar increased risk appeared at the 75th percentile of free T4, suggesting men have slightly more tolerance for higher thyroid hormone levels but still face elevated mortality risk in the upper ranges.
Younger Adults (Under 50): The mortality associations were less pronounced, though subclinical hypothyroidism with TSH 4-10 mIU/L still correlated with increased cardiovascular risk factors including elevated blood pressure, higher cholesterol, and increased body mass index.
Patients with Diabetes: A separate NHANES study found a U-shaped mortality curve for TSH in diabetic patients. Both low-normal (0.39-1.30 mIU/L) and high-normal (2.09-4.60 mIU/L) TSH levels increased cardiovascular and all-cause mortality compared to mid-normal levels. This suggests diabetic patients may benefit from tighter TSH targets around 1.5-2.0 mIU/L.
Why Most Doctors Don’t Know This Yet
Here’s the uncomfortable truth: the 2023 Lancet study represents cutting-edge research that hasn’t yet penetrated mainstream medical practice. Most clinical laboratories still report 0.4-4.0 mIU/L as the reference range without mentioning optimal targets. Current treatment guidelines from major endocrinology societies haven’t fully incorporated these findings into official recommendations.
The paradigm shift: Traditional reference ranges were established by testing healthy populations and defining “normal” as the middle 95% (2.5th-97.5th percentile). This statistical approach ignores whether those “normal” values predict good health outcomes. It’s like defining normal cholesterol based on population averages rather than heart disease risk—which medicine moved away from decades ago for that very reason.
Real-world example: John, a 62-year-old accountant with TSH of 3.9 mIU/L, was told his thyroid was “perfectly normal.” After learning about the optimal range research, he discussed it with his endocrinologist. Together they optimized his TSH to 2.2 mIU/L using low-dose levothyroxine. His calculated 10-year cardiovascular mortality risk dropped by an estimated 5.2% based on the Lancet data—equivalent to the benefit of statin therapy in many patients.
What This Means For You: Bring this research to your doctor’s attention. The 2023 Lancet meta-analysis (PMID: 37696273) provides evidence that “normal” TSH may not be optimal, particularly if you have cardiovascular risk factors, metabolic syndrome, or a family history of heart disease. While not yet standard of care, optimizing TSH to the 60-80th percentile (1.5-2.8 mIU/L) may provide cardiovascular benefits worth discussing with your healthcare provider.
Symptoms, Causes & When to Get Tested
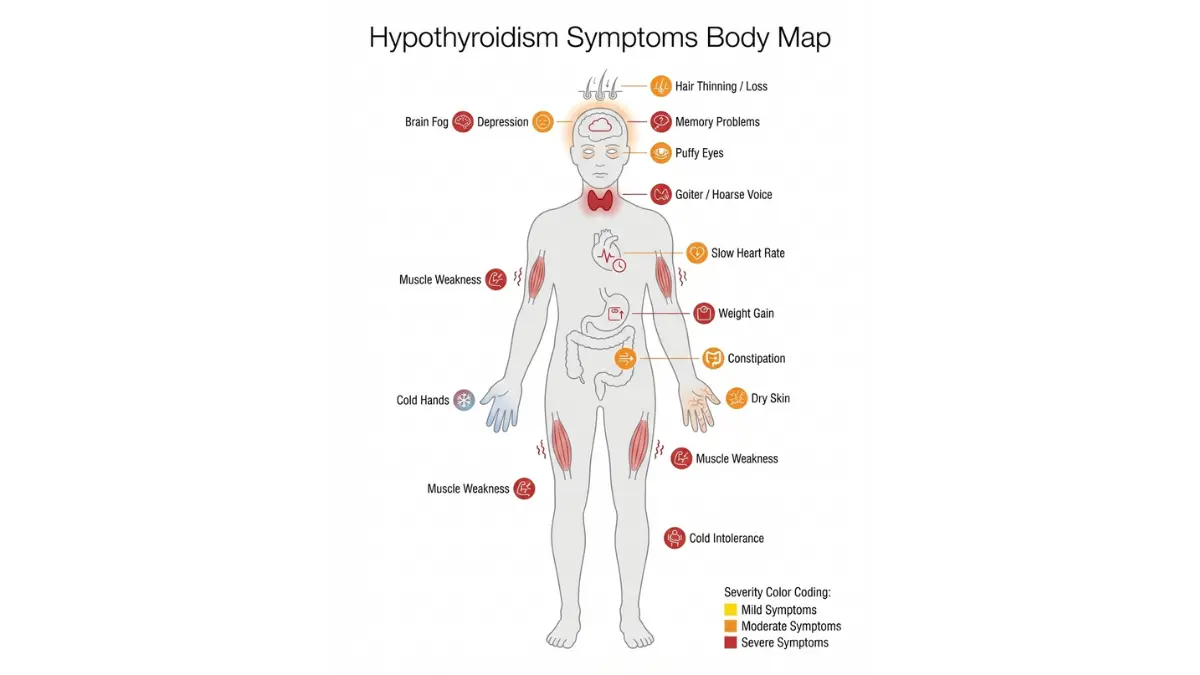
Hypothyroidism Symptoms: Recognizing an Underactive Thyroid
Hypothyroidism often develops gradually, with symptoms so subtle they’re easily dismissed as stress, aging, or other conditions. According to the American Thyroid Association, about 5% of Americans have hypothyroidism, but nearly 60% of those affected don’t know they have it.
Early Signs (TSH 4-10 mIU/L):
- Persistent fatigue despite adequate sleep
- Unexplained weight gain of 5-10 pounds
- Increased sensitivity to cold temperatures
- Mild depression or mood changes
- Slightly dry skin and brittle nails
- Heavier or irregular menstrual periods
Moderate Symptoms (TSH 10-20 mIU/L):
- Above symptoms plus marked fatigue
- Weight gain of 10-20 pounds without dietary changes
- Hair thinning, particularly outer third of eyebrows
- Chronic constipation
- Memory problems and “brain fog”
- Muscle weakness and joint pain
- Puffy face, especially around eyes
Advanced Symptoms (TSH >20 mIU/L):
- All above symptoms intensified
- Severe cognitive impairment affecting work/daily life
- Significant muscle weakness
- Slowed heart rate (bradycardia)
- Very dry, flaky skin
- Hoarse voice
- Myxedema (severe cases): life-threatening condition with confusion, hypothermia, and coma
Real patient insight: “I thought I was just getting older at 45,” shares Jennifer, whose TSH was 12.4 mIU/L. “The weight gain, exhaustion, and memory issues felt like early menopause. After starting levothyroxine and getting my TSH to 2.3, it was like someone turned the lights back on. I had no idea how poorly I’d been functioning.”
Hyperthyroidism Symptoms: Signs of an Overactive Thyroid
Hyperthyroidism affects about 1% of Americans, with symptoms that can be mistaken for anxiety disorders, excessive caffeine intake, or panic attacks. Because the condition accelerates metabolism, symptoms often appear more suddenly than hypothyroidism.
Mild Hyperthyroidism (TSH 0.1-0.4 mIU/L):
- Nervousness, anxiety, or irritability
- Unintentional weight loss despite normal eating
- Increased heart rate or palpitations
- Heat intolerance and excessive sweating
- Difficulty sleeping
- More frequent bowel movements
- Trembling hands
Moderate to Severe (TSH <0.1 mIU/L):
- All above symptoms intensified
- Rapid heartbeat (tachycardia) exceeding 100 bpm at rest
- Significant weight loss (10-20+ pounds)
- Muscle weakness, especially in upper arms and thighs
- Bulging eyes (Graves’ ophthalmopathy)
- Irregular menstrual periods or absence of periods
- Fine, brittle hair with hair loss
- Warm, moist skin
Critical warning: Untreated severe hyperthyroidism can lead to thyroid storm—a life-threatening condition with fever above 104°F, delirium, and cardiac arrhythmias requiring immediate hospitalization. Use our heart rate calculator to track resting heart rate trends.
Who Should Get Their TSH Tested?
The U.S. Preventive Services Task Force doesn’t recommend universal screening for asymptomatic adults, but multiple medical organizations advocate for targeted testing in high-risk groups.
Definite Testing Recommendations:
- Women over 60: One in ten has hypothyroidism, often with minimal symptoms
- Anyone with symptoms suggesting thyroid dysfunction
- Pregnant women or those planning pregnancy
- First-degree relatives of people with thyroid disease (7x increased risk)
- Autoimmune conditions: Type 1 diabetes, celiac disease, rheumatoid arthritis, lupus
- After radiation to head, neck, or chest
- Taking medications affecting thyroid: lithium, amiodarone, interferon, immune checkpoint inhibitors
- Unexplained infertility or recurrent miscarriage
- Every 5 years after age 35 per American Thyroid Association guidance
Frequency of testing:
- Untreated: Every 6-12 months if borderline abnormal
- Starting medication: Every 6-8 weeks until stable
- Stable on medication: Every 6-12 months
- Pregnancy: Every 4 weeks (thyroid needs change rapidly)
- After dose changes: 6-8 weeks
Root Causes of TSH Abnormalities
Understanding why TSH becomes abnormal helps guide treatment and monitor for associated conditions.
High TSH (Hypothyroidism) Causes:
Hashimoto’s Thyroiditis (90% of hypothyroidism): Autoimmune attack on thyroid tissue causes gradual destruction. Diagnosed by elevated thyroid peroxidase (TPO) antibodies in 90% of cases, according to research from the National Institutes of Health.
Iodine Deficiency: Still affects 2 billion people globally, though rare in the U.S. due to iodized salt. Excessive iodine intake can also trigger hypothyroidism.
Treatment-Related: Radioactive iodine therapy, thyroid surgery, or external beam radiation to the neck permanently reduces thyroid function.
Medications: Lithium (used for bipolar disorder) directly impairs thyroid hormone synthesis. Amiodarone (heart medication) contains high iodine content.
Low TSH (Hyperthyroidism) Causes:
Graves’ Disease (70% of hyperthyroidism): Autoimmune antibodies mimic TSH, overstimulating the thyroid. More common in women ages 30-50. Diagnosed by TSH receptor antibodies (TRAb).
Toxic Nodular Goiter: Thyroid nodules autonomously produce hormone independent of TSH regulation. Prevalence increases with age.
Thyroiditis: Temporary inflammation (often post-viral or postpartum) causes stored hormone to leak out, creating transient hyperthyroidism followed by hypothyroidism. Typically resolves within 6-12 months.
Excessive Thyroid Medication: Over-replacement with levothyroxine suppresses TSH. Requires dose adjustment.
The Testing Process: What to Expect
TSH testing requires a simple blood draw, typically performed at a laboratory or doctor’s office. The process takes less than five minutes, and results are usually available within 1-3 days.
Preparation tips:
- Timing matters: TSH has circadian variation, peaking between 2-4 AM and reaching its lowest point in late afternoon. Test consistently in the morning for comparability.
- Fasting unnecessary: Unlike cholesterol or blood sugar testing, TSH doesn’t require fasting, though some doctors prefer it if ordering a complete metabolic panel simultaneously.
- Medication timing: If taking levothyroxine, some endocrinologists recommend waiting to take it until after the blood draw to avoid artificially lowered TSH.
- Biotin warning: Stop biotin supplements 2-3 days before testing—they interfere with immunoassays used to measure TSH, potentially causing falsely low results.
What gets tested:
- Initial screening: TSH alone is usually sufficient
- Abnormal TSH: Follow-up with free T4
- Comprehensive panel: Free T3, thyroid antibodies (TPO, thyroglobulin, TSH receptor)
- Monitoring treatment: TSH and free T4 every 6-8 weeks until stable
When to retest: If TSH is mildly abnormal (4-10 mIU/L) with no symptoms, retest in 2-3 months before starting treatment. TSH can temporarily fluctuate due to illness, stress, or non-thyroidal factors.
Treatment, Lifestyle Optimization & Your Action Plan
Treatment Options for Abnormal TSH Levels
Treatment decisions depend on TSH level, symptoms, age, and overall health status. The goal is optimizing thyroid hormone levels to relieve symptoms and reduce long-term cardiovascular risk—not just normalizing a number on paper.
Hypothyroidism Treatment (High TSH):
Levothyroxine (Synthroid, Levoxyl): The gold standard treatment is synthetic T4 taken once daily on an empty stomach. According to the FDA’s thyroid medication guidance, levothyroxine is the seventh most prescribed medication in America with over 100 million prescriptions annually.
Starting dose: Typically 1.6 mcg per kg body weight (e.g., 112 mcg for a 70 kg/154 lb person). Elderly patients or those with heart disease start at 25-50 mcg to avoid cardiac stress.
Dose adjustments: Every 6-8 weeks based on TSH until reaching target of 0.5-2.5 mIU/L for most patients, or 1.5-2.8 mIU/L if targeting optimal cardiovascular range.
Critical timing: Take levothyroxine 60 minutes before breakfast or at bedtime (3+ hours after last meal) for maximum absorption. Avoid taking within 4 hours of calcium, iron, fiber supplements, or antacids—they reduce absorption by 30-50%.
Treatment Decision Matrix:
| TSH Level | Free T4 | Typical Treatment | Exceptions |
|---|---|---|---|
| >10.0 mIU/L | Low or normal | Treat with levothyroxine | None—universal treatment |
| 7-10 mIU/L | Normal | Usually treat | Consider in elderly without symptoms |
| 4.5-7 mIU/L | Normal | Individualized | Treat if: positive antibodies, pregnant, symptomatic |
| <0.4 mIU/L | High | Antithyroid drugs or RAI | Surgery if large goiter |
| <0.1 mIU/L | Very high | Immediate treatment | Risk of atrial fibrillation, osteoporosis |
Hyperthyroidism Treatment (Low TSH):
Antithyroid Medications: Methimazole (preferred) or propylthiouracil (PTU) block thyroid hormone production. Used as primary treatment or before radioactive iodine.
Radioactive Iodine (I-131): Permanent solution that destroys overactive thyroid tissue. Most patients become hypothyroid and require lifelong levothyroxine—an acceptable trade-off for uncontrolled hyperthyroidism.
Beta-Blockers: Propranolol or atenolol rapidly control symptoms (palpitations, tremors, anxiety) while awaiting definitive treatment effects.
Surgery (Thyroidectomy): Reserved for large goiters, suspicious nodules, or inability to tolerate other treatments. Complications include vocal cord nerve damage (1-2%) and hypoparathyroidism (1-5%).
The Subclinical Hypothyroidism Controversy
This remains one of endocrinology’s most debated topics. With TSH 4.5-10.0 mIU/L and normal free T4, should you treat?
Arguments FOR treatment:
- Prevents progression to overt hypothyroidism
- May improve fatigue, weight, and cognitive symptoms
- Reduces cardiovascular risk in younger adults
- Essential if thyroid antibodies positive (progression rate 4-5% annually)
Arguments AGAINST treatment:
- Limited evidence for benefit in adults 65+
- Overtreatment risks: atrial fibrillation, osteoporosis, anxiety
- TSH often returns to normal spontaneously
- Age-specific reference ranges suggest higher TSH may be physiologically appropriate in elderly
2023 Evidence Update: A randomized controlled trial of 737 adults over 65 with subclinical hypothyroidism published in the New England Journal of Medicine found no improvement in quality of life or thyroid symptoms with levothyroxine treatment versus placebo. This challenges routine treatment in older adults with mild TSH elevation.
Current expert consensus:
- Definitely treat if: TSH >10, positive antibodies, pregnancy, age <65 with symptoms
- Consider treating if: TSH 7-10, strong symptoms, cardiovascular risk factors, age <65
- Monitor without treatment if: TSH 4.5-7, age 65+, no symptoms, no antibodies
- Always retest in 2-3 months before committing to lifelong treatment
Lifestyle Strategies to Optimize Thyroid Function
While medication treats thyroid dysfunction, lifestyle factors significantly influence thyroid health and can optimize TSH levels naturally.
Nutritional Optimization:
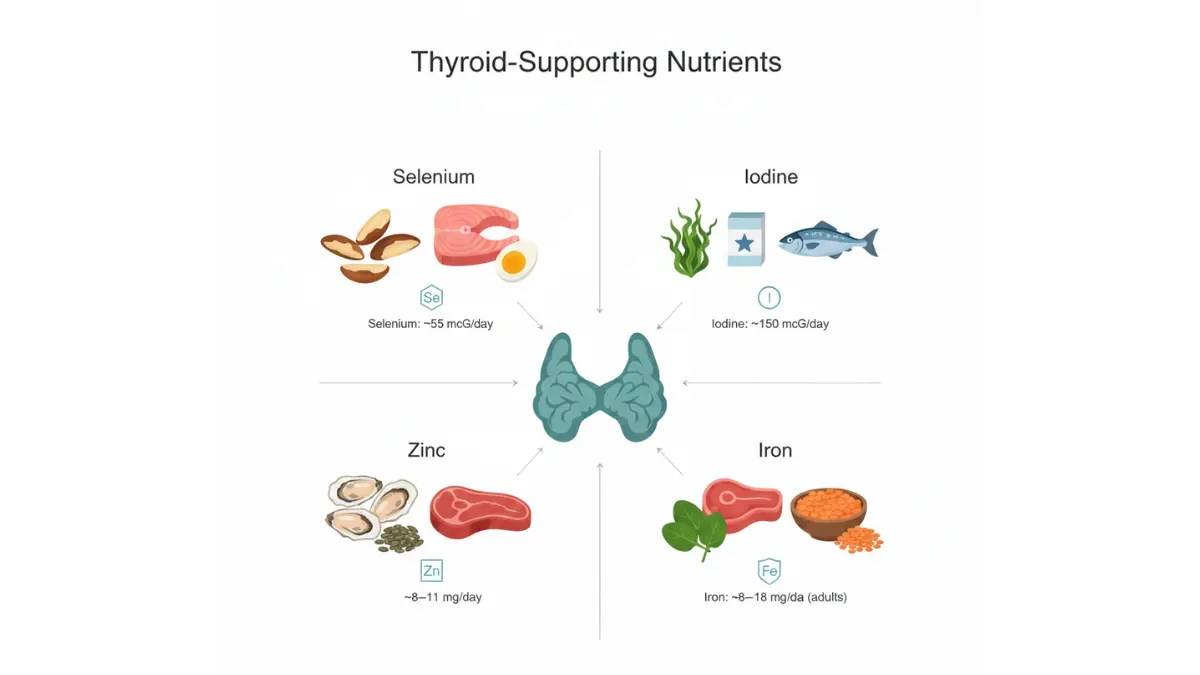
Selenium (55 mcg daily): Essential for converting T4 to active T3. Best food sources include Brazil nuts (just 2 provide daily needs), tuna, halibut, and grass-fed beef. Research from the NIH Office of Dietary Supplements shows selenium supplementation may reduce thyroid antibodies in Hashimoto’s by 40%.
Iodine (150 mcg daily): Required for thyroid hormone synthesis but excessive amounts (>500 mcg daily) can trigger or worsen thyroid dysfunction. Adequate but not excessive intake through iodized salt and seafood is ideal.
Zinc (8-11 mg daily): Supports TSH production and thyroid hormone activation. Found in oysters, beef, pumpkin seeds, and lentils.
Iron: Deficiency impairs thyroid hormone synthesis. Especially important for women with heavy periods. Check ferritin levels alongside TSH.
Vitamin D: Deficiency correlates with higher rates of Hashimoto’s thyroiditis. Aim for blood levels of 30-50 ng/mL through sunlight, fortified foods, or supplementation.
Stress Management Reduces Cortisol Impact:
Chronic stress elevates cortisol, which interferes with thyroid hormone conversion and can suppress TSH. Research published by Harvard Medical School demonstrates that psychological stress impairs hypothalamic-pituitary-thyroid axis function.
Evidence-based stress reducers:
- Mindfulness meditation (20 minutes daily reduces cortisol 15-20%)
- Regular exercise (particularly moderate-intensity cardio)
- Adequate sleep (7-9 hours—poor sleep quality elevates TSH)
- Adaptogenic herbs (ashwagandha may lower TSH in subclinical hypothyroidism)
Exercise Optimization:
Moderate exercise supports healthy thyroid function, but excessive training (>10 hours weekly) can suppress TSH temporarily. Balance is key. Combine cardiovascular exercise with strength training for optimal metabolic health and weight management.
Gut Health Connection:
Your microbiome influences thyroid hormone metabolism and autoimmunity. Research indicates that 20% of T4 to T3 conversion occurs in the gut. Inflammatory bowel conditions and dysbiosis may impair thyroid function.
Gut-supporting strategies:
- Probiotic-rich foods (yogurt, kefir, sauerkraut, kimchi)
- Prebiotic fiber (feeds beneficial bacteria)
- Limit processed foods and excess sugar
- Consider testing for celiac disease (10x higher in Hashimoto’s patients)
Environmental Toxins to Minimize:
Endocrine-disrupting chemicals can interfere with thyroid function. Limit exposure to:
- BPA (plastics, can linings)
- Perchlorate (drinking water contaminant)
- Polychlorinated biphenyls/PCBs (persistent environmental pollutants)
- Excessive fluoride (found in some drinking water)
- Mercury (large fish like swordfish, tilefish)
Monitoring and Optimization: Your Personalized Action Plan
Step 1: Know Your Current Status Get a baseline TSH test if you haven’t had one. If you’re over 35 or have risk factors, request TSH along with your next annual physical. Ask for a copy of your results with reference ranges.
Step 2: Compare to Age-Appropriate and Optimal Ranges Don’t just accept “normal” without knowing the number. If your TSH is 3.5 mIU/L, it’s technically normal but in the high-risk zone for cardiovascular outcomes according to 2023 research.
Step 3: Document Your Symptoms Use our comprehensive symptom checker to track patterns. Rate severity on a 1-10 scale monthly to objectively measure improvement with treatment.
Step 4: Assess Additional Risk Factors Calculate cardiovascular risk using established tools. If you have metabolic syndrome, diabetes, family history of heart disease, or elevated cholesterol, optimizing TSH to the 1.5-2.8 range may provide extra benefit.
Step 5: Partner With Your Healthcare Provider Bring this research (specifically the 2023 Lancet meta-analysis, PMID: 37696273) to your appointment. Discuss whether targeting optimal ranges rather than just “normal” makes sense for your situation.
Step 6: Implement Lifestyle Optimizations Even if medication isn’t indicated, nutrition, stress reduction, and exercise support thyroid health. Track your water intake, ensure adequate protein consumption, and maintain healthy body composition with our BMI calculator.
Step 7: Retest Strategically
- Initial borderline results: 2-3 months
- Starting medication: 6-8 weeks after each dose change
- Stable on treatment: Every 6-12 months
- Pregnancy: Every 4 weeks
Step 8: Adjust and Refine Treatment isn’t one-size-fits-all. Your optimal TSH target may differ from the population average. Some people feel best at 1.0 mIU/L, others at 2.5 mIU/L. Work with your doctor to find your personal optimal range based on how you feel, not just lab values.
What This Means For You:
Understanding TSH empowers you to advocate for your health. Whether you’re investigating unexplained symptoms, managing known thyroid disease, or optimizing wellness, remember that “normal” isn’t necessarily optimal. The difference between TSH of 3.8 and 2.2 mIU/L might not seem significant, but it could translate to meaningful reductions in cardiovascular risk and improvements in energy, weight, mood, and cognitive function.
Take charge of your thyroid health today. Request your TSH level, compare it to both standard and optimal ranges, and discuss targeted optimization with your healthcare provider. Your heart—and your energy levels—will thank you.
Key Takeaways: ✓ Normal TSH range is 0.4-4.0 mIU/L, but optimal for cardiovascular health is 1.5-2.8 mIU/L
✓ High TSH (>4.0) indicates hypothyroidism; low TSH (<0.4) indicates hyperthyroidism
✓ Age-specific ranges matter—TSH naturally increases with age
✓ Subclinical hypothyroidism (TSH 4.5-10) requires individualized treatment decisions
✓ Lifestyle factors including nutrition, stress, and sleep significantly impact thyroid function
✓ Regular monitoring ensures optimal thyroid health and cardiovascular protection
This comprehensive guide provides educational information about TSH levels and thyroid health. Always consult your healthcare provider for personalized medical advice, diagnosis, and treatment decisions based on your specific health situation and laboratory results.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.