On This Page – Quick Medical Summary
Your CMP electrolytes, explained — start here
A red “H” beside your potassium, or an “L” beside your sodium, can turn an ordinary afternoon into a search for the worst possible answer. This page explains what those numbers mean — and what they usually don’t.
Start where your result is:
- Your potassium is flagged. Go to the potassium section. This is the number people fear most, and it is the one where the reason behind it matters more than the value itself.
- Your sodium is flagged. Go to the sodium section. A high sodium result is almost never about how much salt you eat.
- Your chloride is flagged. Go to the chloride section. Chloride is rarely the problem on its own — it is usually telling your provider something about the other numbers.
- You are reading a parent’s or partner’s results. Go straight to the emergency section, which lists the symptoms that matter more than any number on the page.
One out-of-range electrolyte is not a diagnosis. It is the opening of a conversation with the clinician who ordered the test, and this page exists to prepare you for it. For the full picture, see your complete comprehensive metabolic panel results; if several markers are flagged at once, what an abnormal CMP result actually means explains how providers read them together.
ℹ️ Medical Disclaimer: The reference ranges, severity thresholds, medication effects, dietary figures, and emergency criteria in this article are drawn from the cited authorities and are general education only. They cannot interpret your individual result. An electrolyte value is read in the context of your kidney function, your medications, your symptoms, how fast the value changed, and the reference range printed on your own report — one out-of-range number is not a diagnosis, and no article can triage you. Speak with the primary care provider or clinician who ordered your test before acting on anything here, and seek emergency care immediately for the red-flag symptoms listed in the emergency section below.
What the electrolytes on a CMP actually measure
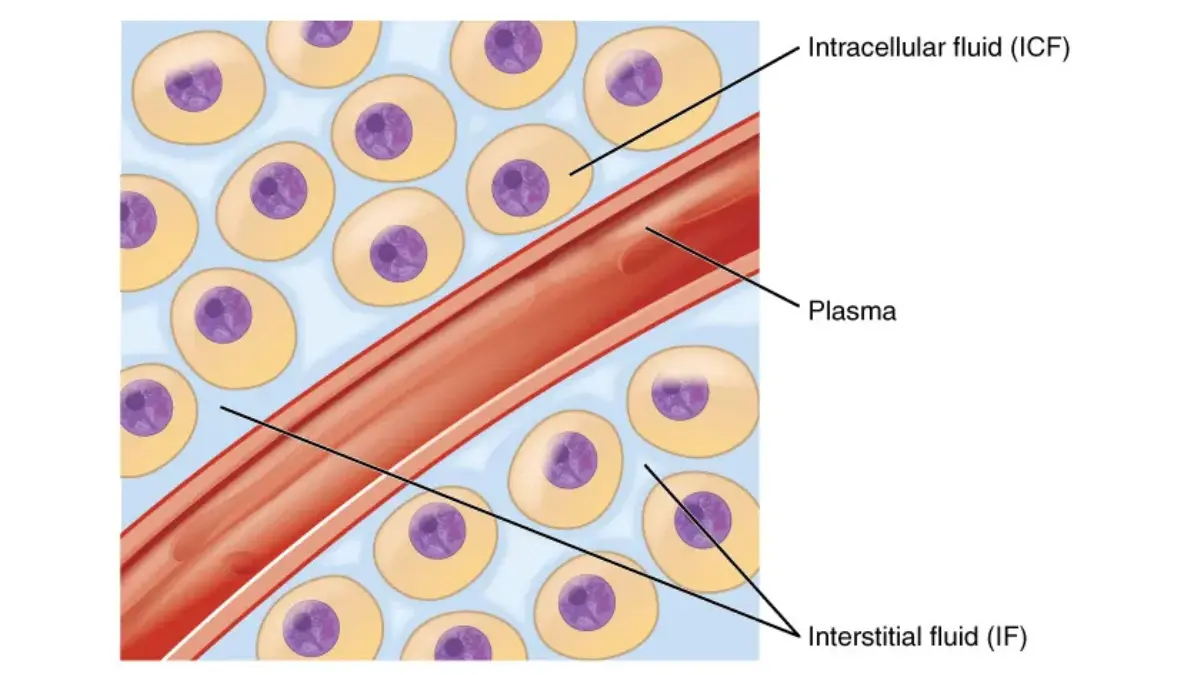
The electrolytes on a comprehensive metabolic panel are sodium, potassium, chloride and bicarbonate — four electrically charged minerals that control the amount of fluid in your body, hold your acid–base (pH) balance steady, and carry the signals that run your nerves, muscles and heart.
A CMP measures 14 substances in total. These four are the electrolyte group; the rest cover blood sugar, kidney function, liver function, proteins and calcium, all of which are broken down in our guide to the 14 components of a CMP.
The four electrolytes on your panel
- Sodium (Na) — controls how much fluid your body holds, and supports nerve and muscle function.
- Potassium (K) — keeps your cells, heart and muscles working properly.
- Chloride (Cl) — works alongside sodium to manage fluid, blood volume and blood pressure.
- Bicarbonate (CO₂) — maintains the balance between acids and bases in your blood.
These four roles are described by the National Library of Medicine’s overview of the electrolyte panel, which is the reference this article uses throughout.
Why they are read together, never alone
Your provider does not read these as four separate verdicts. They move in relation to one another, so a shift in one is often the fingerprint of something happening elsewhere — which is why a single flagged electrolyte is rarely acted on by itself.
If a complete blood count was drawn at the same visit, that is a different test measuring different things; how a CBC differs from a CMP explains why both are often ordered together.
Sodium on your CMP: what high and low really mean
Normal blood sodium runs 135 to 145 mEq/L, according to MedlinePlus, and the range varies slightly between laboratories. Below 135 is called hyponatremia; above 145 is called hypernatremia.
What a low sodium result means
Low sodium is the most common electrolyte abnormality seen in patients arriving at emergency departments, according to American Family Physician (2023) — which also means most low readings turn up in people who feel completely well.
📊 Clinical Data Point: Hyponatremia is classified as mild at 130–134 mEq/L, moderate at 125–129 mEq/L, and severe below 125 mEq/L. Severe or fast-falling hyponatremia can cause confusion, impaired consciousness, unsteadiness and seizures. (Source: American Family Physician, “Diagnosis and Management of Sodium Disorders,” 2023.) NIH clinical reference literature adds that people above 125, or whose level fell gradually over more than 48 hours, generally have few or no symptoms.
What a high sodium result means
High sodium almost always reflects a shortage of water, not a surplus of salt. NIH clinical reference literature describes hypernatremia as arising from net water loss, and notes it is most common in infants and in older adults whose thirst is blunted or who cannot get to a drink unaided.
🔬 How It Works: Your sodium result measures a ratio — how much sodium there is relative to how much water it is dissolved in. Lose water and the same sodium looks concentrated; take on excess water and it looks diluted. That is why sodium is best understood as a water number wearing a salt costume.
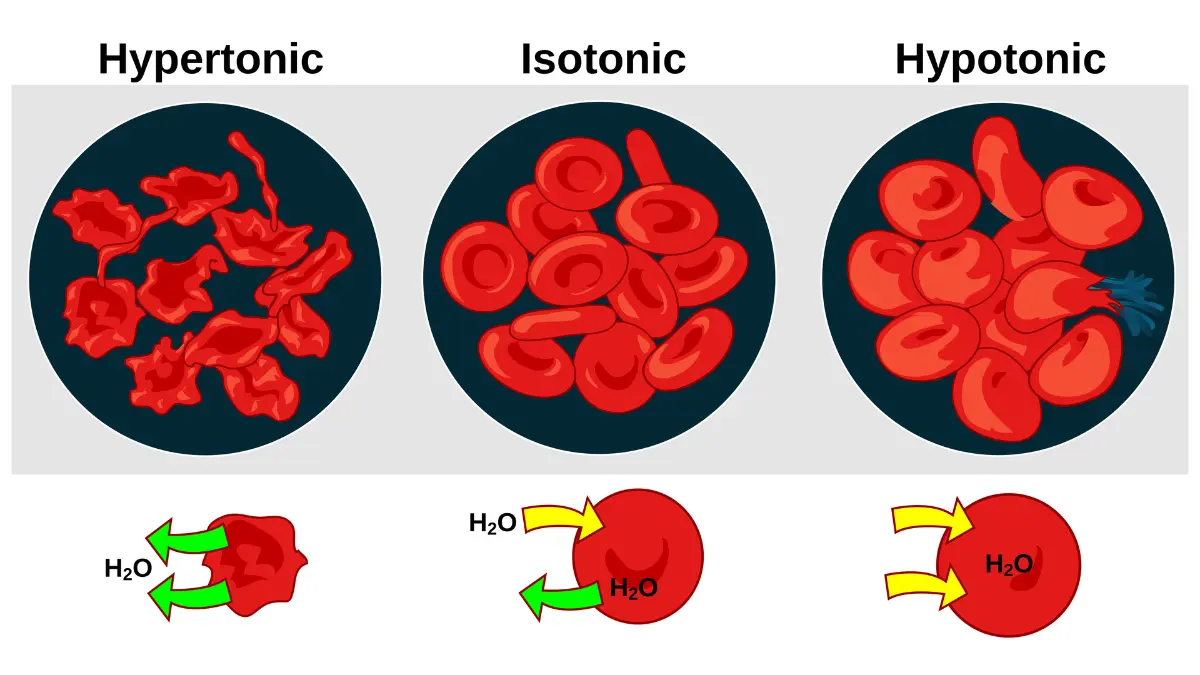
Adapted from Wikimedia Commons Osmotic pressure on blood cells diagram, licensed under Public Domain.
Does eating too much salt cause high sodium?
For most people with a working thirst response and access to water, no. Dietary salt drives blood pressure, not your serum sodium reading — the CDC’s sodium and health overview reports Americans average more than 3,300 mg of sodium a day against a federal recommendation of under 2,300 mg, and the American Heart Association sets an optimal goal of 1,500 mg for most adults.
Those numbers are worth acting on for your heart. They are not the explanation for the number on your panel, and cutting salt will not correct an abnormal sodium result.
✅ Patient Action: Ask the primary care provider who ordered the test: “Is this sodium change new compared with my last panel, how fast did it move, and could any of my medications be causing it?” If you are simply looking at your everyday hydration, our daily water intake calculator gives a general adult estimate — but drinking more water is not a treatment for an abnormal sodium result, and overdrinking is itself a recognised cause of low sodium.
Potassium on your CMP: what high and low mean
Hyperkalemia — high potassium — is generally defined as a level above 5.0 to 5.5 mEq/L, and symptoms usually appear only above 6.0 mEq/L. But the most useful thing published in the NIH’s clinical reference literature is this: how fast your potassium rose matters more than the number it reached.
The normal range — and why yours may differ
The reference range published by MedlinePlus is 3.7 to 5.2 mEq/L. The NIH Office of Dietary Supplements describes normal serum potassium as roughly 3.6 to 5.0 mmol/L. Both are correct — see the next section for why that matters more than it sounds.
What a high potassium result means
According to MedlinePlus, medications that raise potassium include ACE inhibitors, ARBs, the potassium-sparing diuretics spironolactone, amiloride and triamterene, and beta blockers. Reduced kidney function is the other major driver, which is why potassium is always read alongside your kidney markers on the same panel.
What it is almost certainly not is your diet. The NIH Office of Dietary Supplements is explicit that in people with normal kidney function, a high dietary potassium intake carries no health risk, because the kidneys simply excrete the surplus.
Is a potassium of 5.3 dangerous?
That question has no honest answer from a webpage, and any site that gives you one is guessing. Clinical reference literature on hyperkalemia records that mild elevations are frequently asymptomatic, that someone with long-standing kidney impairment may sit at a raised level without symptoms, and that a fast rise can cause serious effects at a lower number.
🩺 Physician Note: A common point of confusion is treating potassium as a pass/fail line. Clinicians weigh four things together — the value, the rate of change, your kidney function, and your medications. The same 5.3 means something different in a healthy 30-year-old than in someone on spironolactone with reduced kidney function.
What a low potassium result means
Hypokalemia is a potassium below 3.5 mmol/L. NIH clinical reference literature classifies it as mild at 3.0–3.4, moderate at 2.5–3.0, and severe below 2.5 mmol/L, with symptoms that may include muscle weakness, fatigue, cramping, palpitations and constipation.
Diuretics and gastrointestinal losses do most of the damage here — severe or chronic diarrhoea is the single most common non-kidney cause. Poor diet alone rarely does it, because healthy kidneys clamp down on potassium excretion when intake drops.
The magnesium connection
Low magnesium frequently travels with low potassium and makes it worse, and the two together raise the risk of dangerous heart rhythms. It is the reason a potassium level sometimes refuses to come back up until the magnesium is addressed — and a reasonable thing to ask about.
🔬 How It Works: Almost all your potassium lives inside your cells. The blood test measures only the small fraction floating outside them, which is why serum potassium is a poor guide to your total body stores — and why a single reading is a snapshot, not an inventory.
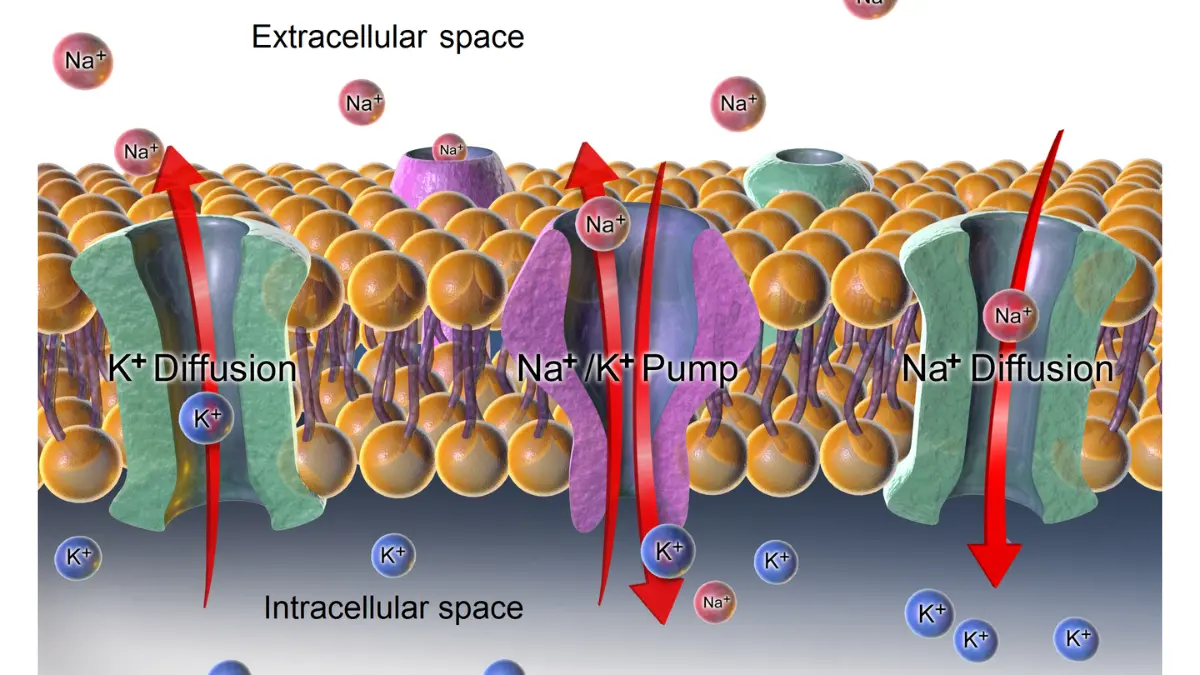
Adapted from Wikimedia Commons Sodium-potassium pump and diffusion, licensed under CC BY-SA 4.0.
✅ Patient Action: If your potassium is flagged high, contact the clinician who ordered the test the same day and ask: “Given my kidney function and my current medications, is this level new — and should it be repeated before we act on it?” Do not adjust any medication yourself.
Chloride and the anion gap: the numbers nobody explains
Chloride is the electrolyte patients skip and providers use. MedlinePlus gives a typical normal chloride range of 98 to 107 mEq/L, with variation between laboratories — but chloride’s real job on the report is arithmetic.
What high and low chloride suggest
Per MedlinePlus’s chloride blood test reference, a higher-than-normal chloride (hyperchloremia) may be linked to kidney disease, metabolic acidosis, diarrhoea, renal tubular acidosis, ketoacidosis, or salicylate toxicity such as an aspirin overdose.
A lower-than-normal chloride (hypochloremia) may be linked to vomiting, dehydration, excessive sweating, burns, congestive heart failure, metabolic alkalosis, or SIADH. Note the direction of travel — dehydration and vomiting push chloride down, which is the opposite of what most people assume.
What is the anion gap on a CMP?
The anion gap is a value your lab calculates rather than measures:
Anion gap = sodium − (chloride + bicarbonate)
A normal anion gap runs roughly 4 to 12 mmol/L, according to NIH clinical reference literature, and it shifts with your albumin and phosphate levels. Its main use is sorting out what kind of acid–base problem a person has.
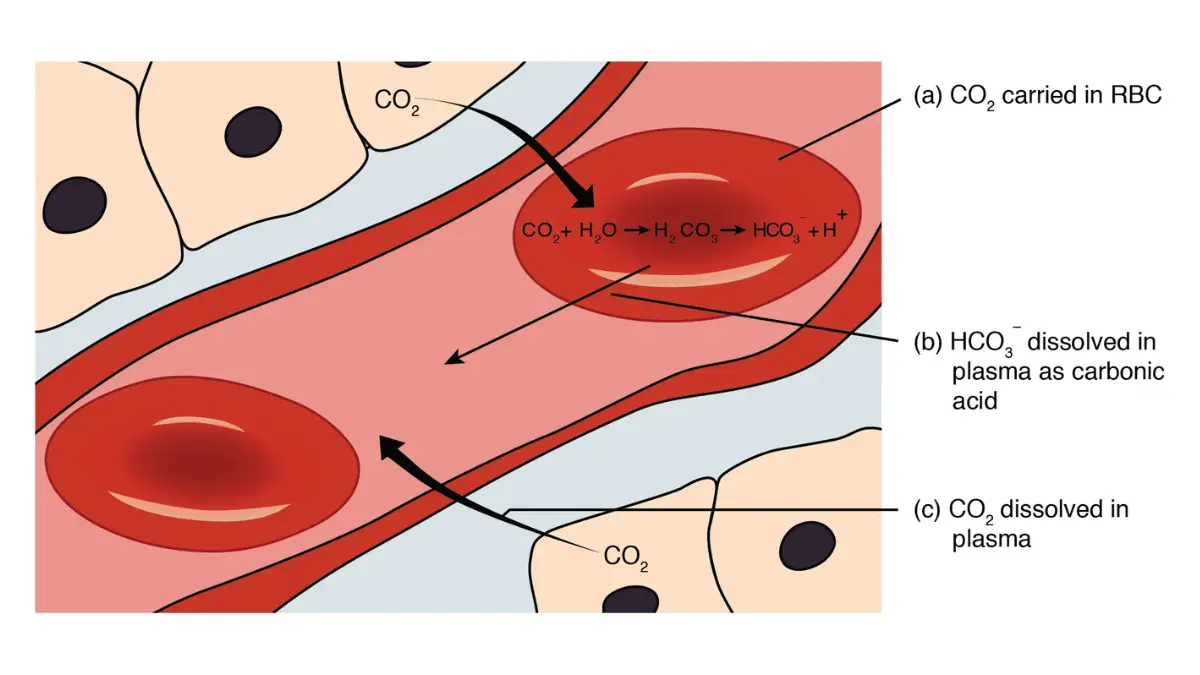
Adapted from OpenStax Gas Transport, licensed under CC BY 4.0.
🔬 How It Works: Take an ordinary panel — sodium 140, chloride 105, bicarbonate 26. The gap is 140 − 131 = 9, comfortably normal. If that gap were wide, it would tell your provider that something acidic and unmeasured is circulating in the blood, and send them looking for it. Chloride’s value is that it makes this sum possible.
Reading the whole report line by line is a skill worth having; our guide to reading your CMP results walks through every line of the printout.
Why your electrolyte result may not mean what it says
Yes — a blood test can report a falsely high potassium. MedlinePlus states it directly: if it is difficult to get the needle into the vein, injury to the red blood cells can release potassium into the sample and produce a falsely elevated result.
When a high potassium is not real
NIH clinical reference literature calls this pseudohyperkalemia — a spurious elevation caused by the collection, the handling, hemolysis of the sample, or a very high platelet count. It is common enough that a repeat draw is a routine next step, not a sign anyone is dismissing you.
Why different labs print different normal ranges
This is the part almost nobody explains, and it changes how you should read your own report.
| Electrolyte | MedlinePlus (NIH) range | URMC Health Encyclopedia range | Key clinical detail |
|---|---|---|---|
| Sodium | 135–145 mEq/L | 136–145 mEq/L | A 135 is normal by one reference, borderline by the other |
| Potassium | 3.7–5.2 mEq/L | 3.5–5.0 mEq/L | A 3.6 is low by MedlinePlus and normal by URMC — and a 5.1 flips the other way |
| Chloride | 98–107 mEq/L | 98–106 mmol/L | The upper limit differs by a full point |
Ranges as published by MedlinePlus, National Library of Medicine (NIH), reviewed 2025, and by the University of Rochester Medical Center Health Encyclopedia — the reference set used in our own CMP normal range guide. Neither source is wrong. Laboratories set their intervals from their own analyzers and their own tested population, which is why the range printed on your report is the only one that applies to your result.
What can shift a result before you reach the lab
A missed fasting instruction, dehydration on the day, or a medication you take routinely can all move these numbers — how to prepare for a CMP covers what actually matters. If the result looks out of character, when a blood test result is wrong and needs a retest explains how a recheck is decided.
⚠️ Clinical Warning: MedlinePlus is unambiguous on this point: many medicines interfere with blood test results, and you should not stop or change any medication before a test without speaking to your provider first. Stopping a diuretic, an ACE inhibitor or a potassium-sparing drug on your own to “clean up” a result is more dangerous than the flagged number that prompted it.
When an electrolyte result is an emergency
A number on a screen cannot tell you whether you are safe. Symptoms can. Seek emergency care now — do not wait for a callback — if you or the person whose results you are reading has any of the following:
- Heart palpitations, a racing heart, or a heartbeat that feels like it is skipping. Severe potassium abnormalities in either direction can cause life-threatening heart rhythm disturbances.
- Severe muscle weakness or paralysis, including weakness that makes it hard to grip, stand, or breathe.
- Confusion, disorientation, or a marked drop in alertness.
- A seizure, or loss of consciousness.
⚠️ Clinical Warning: Severe hyperkalemia can cause fatal arrhythmias, and severe hypokalemia can cause fatal arrhythmias or paralysis of the breathing muscles, according to NIH clinical reference literature. Severe or rapidly developing low sodium can cause seizures. These are the reasons this section exists — and the reason no article, including this one, should ever tell you a specific value is safe to sit on.
✅ Patient Action: If none of the above applies, contact the clinician who ordered your test — usually your primary care provider — and ask: “Which electrolyte is out of range, by how much, and does it need a repeat draw or a change to anything I am taking?” Bring the printed report with its own reference ranges.
Common questions about CMP electrolyte results
1. What do electrolytes mean on a CMP?
The CMP electrolytes are sodium, potassium, chloride and bicarbonate. These four charged minerals control your body’s fluid balance, keep your blood’s acid–base balance steady, and carry the electrical signals your nerves, muscles and heart depend on. They are four of the 14 substances a comprehensive metabolic panel measures, and they are read as a set rather than individually.
2. What is a normal sodium level on a blood test?
MedlinePlus gives a normal blood sodium range of 135 to 145 mEq/L, with slight variation between laboratories. Below 135 is hyponatremia; above 145 is hypernatremia. Compare your result to the reference range printed on your own report rather than to a figure from another lab, and ask the clinician who ordered the test to interpret it.
3. What is a normal potassium level?
MedlinePlus publishes 3.7 to 5.2 mEq/L, while the NIH Office of Dietary Supplements describes roughly 3.6 to 5.0 mmol/L. Both are legitimate. This is why a potassium of 3.6 can be flagged at one lab and normal at another — your own report’s printed range is the one that applies to you.
4. What does high potassium mean on a blood test?
Hyperkalemia is generally a potassium above 5.0 to 5.5 mEq/L. Common drivers are reduced kidney function and medications — ACE inhibitors, ARBs, potassium-sparing diuretics and beta blockers, per MedlinePlus. It is rarely caused by diet in people with normal kidney function. Contact the clinician who ordered the test the same day for interpretation.
5. Is a potassium level of 5.3 dangerous?
No webpage can answer that for you. NIH clinical reference literature notes that mild elevations are frequently asymptomatic and that symptoms generally appear above 6.0 mEq/L — but that the rate of change matters more than the value. Your provider weighs the number against your kidney function and medications. Ask them the same day.
6. What does low sodium mean on a blood test?
Hyponatremia is a sodium below 135 mEq/L, classified as mild at 130–134, moderate at 125–129 and severe below 125 mEq/L. Many people with mild, slowly developing low sodium have no symptoms at all. Severe or fast-falling levels can cause confusion and seizures. Have the clinician who ordered your test interpret it.
7. Does eating too much salt cause high sodium on a blood test?
Usually not. High blood sodium reflects a shortage of water rather than an excess of salt, and it appears most often in people whose thirst is blunted or who cannot drink freely. Dietary salt matters enormously for blood pressure — but cutting salt will not correct an abnormal sodium result.
8. What does high chloride mean?
Per MedlinePlus, hyperchloremia may be associated with kidney disease, metabolic acidosis, diarrhoea, renal tubular acidosis, ketoacidosis or salicylate toxicity. It is seldom meaningful on its own — chloride is usually interpreted alongside your sodium and bicarbonate. Ask the clinician who ordered your panel what pattern they are seeing across the four electrolytes.
9. What is the anion gap on a CMP?
The anion gap is calculated, not measured: sodium minus the sum of chloride and bicarbonate. NIH clinical reference literature puts the normal gap at roughly 4 to 12 mmol/L, varying with albumin and phosphate. Its purpose is to help a clinician classify what kind of acid–base disturbance may be present.
10. Can a blood test show a falsely high potassium?
Yes. MedlinePlus states that a difficult blood draw can injure red blood cells, releasing potassium into the sample and producing a falsely high reading. NIH literature calls this pseudohyperkalemia and links it to collection, handling, hemolysis and high platelet counts. This is why a repeat draw is often the very next step.
11. When is an electrolyte result an emergency?
Symptoms, not values, are what you can act on at home. Seek emergency care for palpitations or an irregular heartbeat, severe muscle weakness or difficulty breathing, confusion, or a seizure. Severe potassium abnormalities can cause fatal heart rhythms, and severe low sodium can cause seizures. Otherwise, contact the clinician who ordered the test.
What to do next with your electrolyte results
You now know more about your electrolytes than the flagged letter beside them told you. The single most useful thing you can do is not more reading — it is one specific question, asked of the person who ordered the test.
Take your printed report, with its own reference ranges, and ask: “Which electrolyte is out of range, by how much compared with my last panel, and does this need a repeat draw before we change anything?”
If other markers on the panel were also flagged, your full comprehensive metabolic panel results explains how the 14 numbers are read together — because that pattern, not any single value, is what your provider is actually looking at.
Disclosure: some links on this site are affiliate links, and we may earn a commission if you use them. At-home CMP and electrolyte panels are available if you want to recheck between provider visits. They are a convenience, not a substitute for the clinician interpreting your result, and we do not recommend acting on any at-home value without one.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.