On This Page – Quick Medical Summary
Your CMP flagged a liver marker — here’s what that means
Your comprehensive metabolic panel measures 14 substances, and six of them report on your liver: ALT, AST, ALP, bilirubin, albumin, and total protein.
One flagged number is not a diagnosis. What a clinician reads is the pattern — which markers moved together, and by how much.
Find your situation below, then read that section first.
The six liver markers on your CMP
- ALT or AST high, ALP normal → Sections 3 and 4
- Bilirubin high, ALT and AST normal → Section 5
- Taking medication or supplements, or trained hard before the draw → Section 6
- Yellowing eyes or skin, dark urine, pale stools, or new confusion → Section 7, now
Why one number out of range is usually not the answer
ALT and AST are liver enzymes that leak out of injured cells. ALP and bilirubin track bile flow. Albumin and total protein show what your liver is still building — a different question entirely.
The National Library of Medicine notes that a CMP can find certain conditions before you have symptoms. That is why so many people discover an abnormal liver marker while feeling completely fine. For the other eight results on the same page, see what all 14 CMP results mean.
ℹ️ Medical Disclaimer: This article explains how liver markers are interpreted; it does not interpret your result. It is not a diagnosis, and it does not recommend, start, stop, or adjust any medication, supplement, procedure, or treatment. Reference ranges vary by laboratory, and a single value cannot be read without your full history. Bring your actual numbers to a board-certified primary care physician, gastroenterologist, or hepatologist before acting on anything here. If you have symptoms of acute liver injury — yellowing skin or eyes, dark urine, pale stools, abdominal swelling, unusual bruising, or confusion — seek medical care now rather than reading further.
What each liver marker actually measures
The six markers split into two groups that answer two different questions: what has been injured, and what your liver can still do.
| Marker | What it measures | Typical adult range | Key clinical detail |
|---|---|---|---|
| ALT | Enzyme concentrated in the liver | 4–36 U/L | The most liver-specific of the six |
| AST | Enzyme in liver, heart and muscle | 8–33 U/L | Can rise from muscle, not liver |
| ALP | Enzyme tied to bile ducts and bone | 20–130 U/L | Rises when bile flow is obstructed |
| Total bilirubin | Waste from red blood cell breakdown | 0.1–1.2 mg/dL | Backs up when the liver can’t clear it |
| Albumin | Main protein the liver makes | 3.4–5.4 g/dL | Falls in chronic, not acute, injury |
| Total protein | Albumin plus globulins | 6.0–8.3 g/dL | A synthesis marker, not an injury marker |
Reference values from the National Library of Medicine’s reference values for a CMP. MedlinePlus notes that normal ranges may vary slightly between laboratories, and some labs use different measurements — always read your own lab’s printed range.
ALT and AST: enzymes that leak when cells are injured
🔬 How It Works: Healthy liver cells hold these enzymes inside them. When a cell is damaged, its membrane leaks and the enzymes spill into your blood. A high ALT does not mean your liver is “failing” — it means cells released their contents, which is a very different and often reversible event.
The critical asymmetry: AST is found mainly in the liver but also in your heart, muscles, and other tissues. ALT is far more liver-specific. That single fact drives Section 4.
ALP, bilirubin, albumin and total protein
ALP and bilirubin move when bile can’t drain. Albumin and total protein fall only when the liver has been struggling for a long time — which is why a normal albumin alongside a high ALT is genuinely reassuring.
MedlinePlus advises no food or drink for at least 8 hours before a CMP; see whether you need to fast for a CMP. The kidney half of the same panel is read on completely different logic.
How high is too high? The ALT threshold your lab may not use
Your lab prints a range. A specialty guideline prints a different, lower one — and the gap between them is the most decision-relevant fact on this page.
📊 Clinical Data Point: A true healthy normal ALT is 29–33 IU/L in males and 19–25 IU/L in females, and levels above that should be assessed by a physician. — Source: American College of Gastroenterology, Evaluation of Abnormal Liver Chemistries (Kwo, Cohen & Lim, 2017), verified against the published guideline.
The lab’s “normal” versus the guideline’s “healthy”
Compare that to the 4–36 U/L range in Section 2. An ALT of 45 in a woman sits above the ACG threshold while sitting inside many labs’ printed ceiling — and would not be flagged at all.
The ACG guideline notes that ALT upper limits vary between laboratories, which is precisely how this gap opens. Full context on the other 13 markers is in the normal ranges for a CMP and how clinicians read the panel.
Why a normal ALT does not rule out liver disease
The guideline cuts both ways, and honesty requires saying so. The ACG states plainly that a normal ALT level may not exclude significant liver disease, and that ALT levels are higher in males than females. It also notes that an elevated ALT has been associated with increased liver-related mortality — a population-level association across large cohorts, not a prediction about any individual reader.
🩺 Physician Note: Current guidance emphasizes that these thresholds are a trigger for assessment, not a diagnosis. A common point of confusion: many labs have not adopted the lower ACG values, so a result inside your lab’s range may still be worth a conversation.
✅ Patient Action: Bring the exact number to a primary care physician and ask: “My ALT is ___. Is that above the healthy threshold the ACG guideline uses for my sex, and should we repeat it before deciding anything?”
Reading the pattern: which markers went up together
This is the step your clinician performs and most explainers skip. The pattern — not the individual number — narrows what is actually happening.
| Pattern | Marker signature | What it points toward | Key clinical detail |
|---|---|---|---|
| Hepatocellular | ALT and AST up, ALP relatively normal | Injury to liver cells themselves | The most common pattern on a routine CMP |
| Cholestatic | ALP up, ALT and AST relatively normal | Impaired bile flow | ALP also comes from bone — context matters |
| Mixed | Both elevated | Overlapping processes | Can shift as the condition evolves |
| Isolated bilirubin | Bilirubin up, everything else normal | Often benign — see Section 5 | A recognized pattern in its own right |
Pattern definitions verified against the American College of Gastroenterology guideline and the NIH’s overview of how clinicians classify the injury pattern.
The ACG defines hepatocellular injury as a disproportionate rise in AST and ALT compared with alkaline phosphatase, and cholestatic injury as the reverse.
🔬 How It Works: Clinicians quantify this with the R ratio: ALT divided by its upper limit of normal, divided by ALP divided by its upper limit of normal. Above 5 is hepatocellular; below 2 is cholestatic; 2 to 5 is mixed. It is a triage tool that narrows the list — it does not name the disease, and it is not a home diagnostic.
What the AST-to-ALT ratio hints at
An AST higher than ALT is the one combination worth naming specifically.
⚠️ Clinical Warning: The ACG guideline advises that men consuming more than 210 grams of alcohol per week, and women more than 140 grams per week, who show a higher AST than ALT should be considered at risk for alcohol-related liver disease and counselled on cessation. This is a threshold for clinical assessment — not a self-diagnosis, and not a reason to stop anything abruptly without medical supervision.
The ACG also describes a linear relationship between ALT level and BMI, which is why metabolic causes lead the differential; you can check your BMI for context. If your markers are elevated and a dedicated liver panel was ordered, decoding LFT numbers goes deeper than a CMP can.
High bilirubin with normal ALT and AST
If bilirubin is your only flagged value, there is a specific, common and mostly harmless explanation that almost nobody leads with.
📊 Clinical Data Point: Gilbert syndrome is estimated to affect 3 to 7 percent of Americans, and roughly 30% of people who have it have no signs or symptoms at all — they are discovered only when a routine blood test shows elevated unconjugated bilirubin. — Source: MedlinePlus Genetics, National Library of Medicine.
Gilbert syndrome: common, harmless, found by accident
That second figure describes the exact situation you may be in right now. Gilbert syndrome is an inherited variation in how efficiently the liver processes bilirubin, not a disease of liver damage.
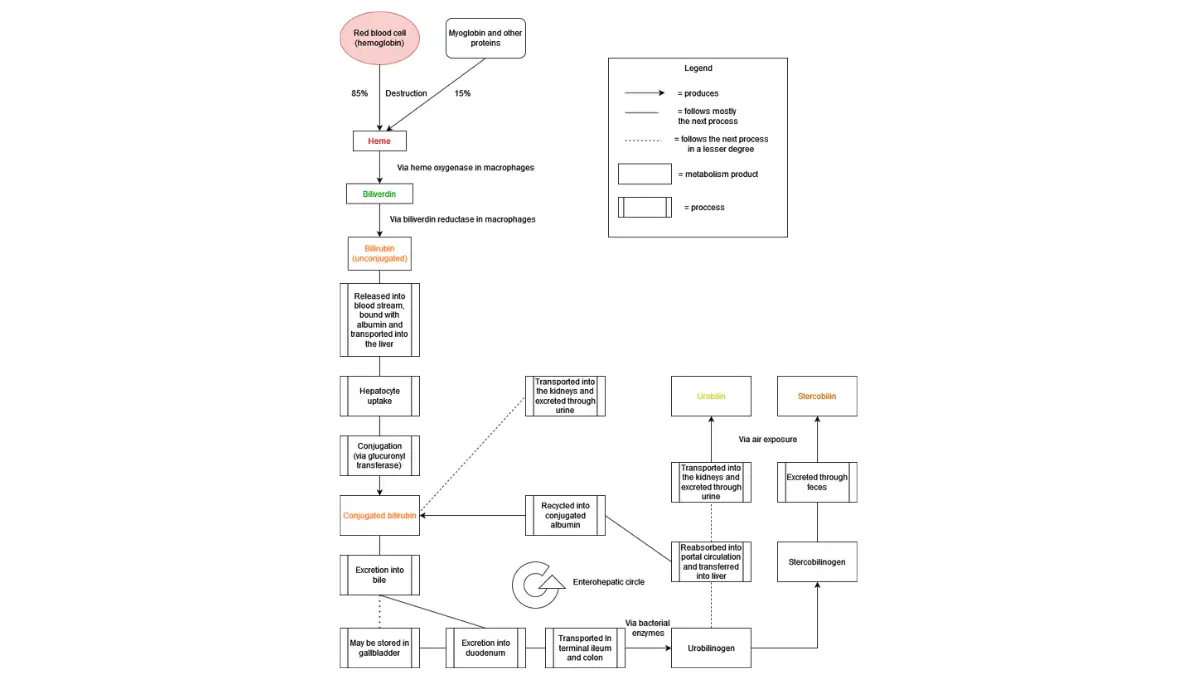
🔬 How It Works: The liver converts toxic unconjugated bilirubin into a water-soluble form it can excrete. In Gilbert syndrome that conversion enzyme runs at roughly 30% of normal capacity, so bilirubin backs up mildly. Episodes are typically triggered by dehydration, prolonged fasting, illness, vigorous exercise, or menstruation — including the overnight fast before your blood draw.
When a high bilirubin does need a closer look
The distinction that matters is which bilirubin. The ACG notes that most bilirubin circulates in the unconjugated form, and that an elevated conjugated — “direct” — bilirubin implies hepatocellular disease or cholestasis. Total bilirubin alone cannot tell you which you have.
Only a clinician can diagnose Gilbert syndrome, and only by excluding the alternatives.
✅ Patient Action: Ask your primary care physician: “Was my direct (conjugated) bilirubin measured, and what was it?” That single question separates the benign pattern from the one needing a workup.
Medications, supplements and habits that move these numbers
Before assuming disease, account for what you were already doing. The most common movers are ordinary.
Acetaminophen: the one hiding inside your other medicines
Acetaminophen is the one worth naming, because you may be taking it without knowing. The FDA notes that more than 600 prescription and over-the-counter medicines contain it, often abbreviated as APAP on labels.
⚠️ Clinical Warning: The FDA’s consumer guidance on acetaminophen states that taking too much can cause liver failure and death, that you should ask a health care professional before using it if you have liver disease, and that severe liver damage may occur if you have three or more alcoholic drinks per day while using it. Read the Drug Facts label on every product you take — we are not a dosing authority and will not give you a number.
Supplements, alcohol, and hard workouts
Because AST also lives in muscle, a hard training session before a blood draw can raise it without your liver being involved at all. Alcohol in the days before a test, and dietary supplements — which are not regulated the way medicines are — belong in the same conversation.
✅ Patient Action: Take your complete list — prescriptions, over-the-counter products, and every supplement — to a pharmacist. Ask: “Can you review all of this for anything that could raise my liver enzymes?” A pharmacist is free, walk-in, and is the right professional for this. Never stop a prescribed medication on your own.
When an abnormal liver marker needs urgent attention
Almost always, the answer is a repeat blood test in a few weeks. These symptoms change that.
Seek medical care now if you have:
- Jaundice — yellowing of the skin or the whites of the eyes
- Changes in the color of your stool or urine — dark urine, or pale, clay-colored stools
- Swelling of the abdomen or legs
- Bruising or bleeding easily
- Confusion or new problems thinking clearly
- A suspected acetaminophen overdose — the FDA directs you to get medical help or contact Poison Help at 1-800-222-1222 right away
Symptom list verified against the National Library of Medicine’s liver disease overview and its cirrhosis reference page (MedlinePlus). The same source notes that liver disease sometimes causes no symptoms at all — which is why the blood test exists.
What your clinician will likely do next
For a mild elevation with none of the above, expect a repeat draw, a review of your medications and alcohol intake, and possibly an ultrasound. Because viral hepatitis is part of the standard workup for a hepatocellular pattern, hepatitis panel results may be ordered alongside it.
✅ Patient Action: If none of the red flags apply, ask your primary care physician: “When should we repeat this, and what would make you refer me to a gastroenterologist?” If any red flag applies, go now — do not wait for a callback. Our symptom checker is not a substitute for urgent care.
Liver markers on a CMP: common questions
1. What are the liver markers on a CMP?
Six of the 14 results on a comprehensive metabolic panel report on your liver: ALT, AST, ALP, total bilirubin, albumin, and total protein. ALT, AST and ALP are enzymes; bilirubin is waste from red blood cell breakdown; albumin and total protein show what your liver is still producing. They are interpreted together, never one at a time.
2. What is a normal ALT level on a CMP?
Your lab most likely prints a range around 4–36 U/L. The American College of Gastroenterology’s 2017 guideline sets a true healthy normal ALT at 29–33 IU/L for males and 19–25 IU/L for females, and says levels above that should be assessed by a physician. The two are not the same number. Bring your exact result to your clinician.
3. Is an ALT of 45 dangerous?
An ALT of 45 sits inside many labs’ printed range but above the ACG’s healthy threshold for both sexes, so it is worth assessing rather than ignoring. It is not, on its own, an emergency. What matters is whether AST, ALP and bilirubin also moved, and whether the elevation persists on a repeat draw. Ask your primary care physician to interpret it in context.
4. What does a high AST with a normal ALT mean?
AST is found in the heart and muscles as well as the liver, while ALT is far more liver-specific. A high AST with a normal ALT therefore often points away from the liver — toward muscle, for example, including a hard workout before your blood draw. Your clinician will consider non-liver sources before assuming liver injury.
5. What does an AST-to-ALT ratio above 2 suggest?
The ACG guideline advises that people drinking above defined thresholds — more than 210 grams of alcohol weekly for men, 140 for women — who show a higher AST than ALT should be considered at risk for alcohol-related liver disease and counselled on cessation. It is a signal for clinical assessment, not a diagnosis. Discuss it honestly with your physician.
6. What causes high bilirubin when ALT and AST are normal?
This is called isolated hyperbilirubinemia, and it is a recognized pattern. The most common explanation is Gilbert syndrome, an inherited variation affecting an estimated 3–7% of Americans. The key follow-up question is whether your direct (conjugated) bilirubin was elevated, because that points toward a liver or bile-duct problem instead. Ask your clinician which was measured.
7. Can Gilbert syndrome show up on a routine CMP?
Yes — that is usually exactly how it is found. Roughly 30% of people with Gilbert syndrome have no symptoms whatsoever and are discovered only when a routine blood test shows elevated unconjugated bilirubin. Levels typically fluctuate with dehydration, fasting, illness or hard exercise. Only a clinician can confirm the diagnosis, by excluding other causes.
8. Which medications can raise liver enzymes?
Many can, which is why this needs a person rather than a list. Acetaminophen is the one most worth knowing about, because the FDA notes it appears in over 600 prescription and over-the-counter products, often abbreviated as APAP. Take your full medication and supplement list to a pharmacist for review, and never stop a prescribed medicine on your own.
9. Can exercise or fasting change my liver markers?
Yes. AST is present in muscle as well as liver, so vigorous exercise before a blood draw can raise it independently of any liver problem. In Gilbert syndrome, bilirubin rises with prolonged fasting, dehydration and vigorous exercise — including the overnight fast before the test. Mention recent hard training or illness to your clinician.
10. Do I need to fast before a CMP?
MedlinePlus advises no food or drink for at least 8 hours before a comprehensive metabolic panel. Fasting mainly protects the accuracy of the glucose result rather than the liver markers, though a prolonged fast can nudge bilirubin upward in some people. Follow the specific instructions your ordering clinician or lab gives you.
11. When is a high liver marker an emergency?
Not by number — by symptom. Yellowing skin or eyes, dark urine, pale or clay-colored stools, abdominal or leg swelling, easy bruising, or new confusion all warrant immediate medical care, as does a suspected acetaminophen overdose. Without those, a mildly elevated liver marker is almost always managed with a repeat blood test. Contact your clinician the same day if you are unsure.
What to do with your result this week
Write your six numbers down side by side. Ask which pattern they form, whether the direct bilirubin was measured, and what your ALT looks like against the ACG’s healthy threshold rather than only your lab’s ceiling. Those three questions will get you further than any article can.
Take a full medication and supplement list to a pharmacist. If a red flag from Section 7 applies, go today. For everything else on the panel, see what an abnormal CMP result means and the full CMP guide.
We can tell you how these markers are read. We cannot tell you what yours mean — your clinician has your history, and we do not.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.