
On This Page – Quick Medical Summary
Margaret, a 61-year-old nurse from Houston, opened her patient portal at 11 PM after a routine blood draw. Her D-dimer result read 0.72 mg/L. The reference range on her report said “< 0.50.” Her hands went cold.
She spent the next two hours searching online. Every article she found gave her generic text — no chart, no context, no answer to her number.
This guide exists to fix that.
The short answer: A normal D-dimer level is under 0.5 mg/L (FEU) or under 500 ng/mL in most adults. But whether your specific number is truly abnormal depends on your age, whether you’re pregnant, recent surgery, and which lab method was used. This chart-based guide covers all of it — in plain language.
The Complete D-Dimer Range Chart
What Is a Normal D-Dimer Level?
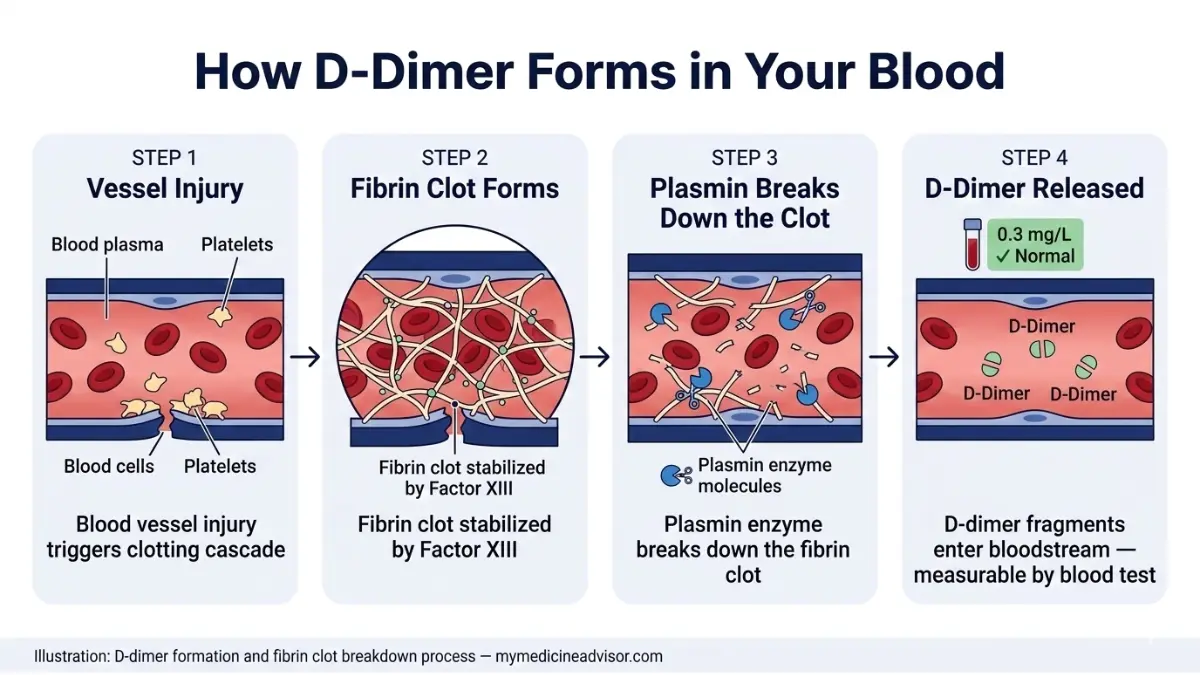
The D-dimer test measures protein fragments released when your body breaks down blood clots. According to MedlinePlus (NIH), it is primarily used to rule out dangerous clotting conditions like deep vein thrombosis (DVT) and pulmonary embolism (PE) — not to diagnose them.
Important: The test has ~95–98% sensitivity (excellent at ruling out clots when negative) but only ~40–50% specificity (many false positives). An elevated D-dimer level does not automatically mean you have a blood clot.
📊 D-Dimer Range Chart — 2026 Reference Guide
| D-Dimer Level (mg/L FEU) | ng/mL FEU | Zone | Clinical Interpretation |
|---|---|---|---|
| < 0.5 | < 500 | ✅ Normal | Clot highly unlikely. VTE safely excluded in low-risk patients. |
| 0.5 – 1.0 | 500 – 1,000 | ⚠️ Borderline | Gray zone. Clinical context required. May need imaging. |
| 1.0 – 2.0 | 1,000 – 2,000 | 🔶 Elevated | Possible clot or non-clot cause. Further evaluation needed. |
| 2.0 – 4.0 | 2,000 – 4,000 | 🔴 High Alert | High probability of active clot. Urgent imaging recommended. |
| > 4.0 | > 4,000 | 🚨 Critical | Possible DIC, massive PE, or severe systemic disease. Emergency evaluation. |
💡 Key Takeaway: A single number means nothing without context. Your age, recent health history, and which lab unit was used are equally important as the number itself.
Understanding Your Lab Units: FEU vs. DDU
One of the most confusing aspects of D-dimer testing — and something zero competitor sites explain clearly — is that labs use two completely different measurement systems.
- FEU (Fibrinogen Equivalent Units): Used by approximately 70% of U.S. labs. Normal cutoff: < 500 ng/mL or < 0.5 mg/L.
- DDU (D-dimer Units): Used by ~30% of labs. Normal cutoff: < 250 ng/mL or < 0.25 mg/L.
The conversion rule: 1 FEU ≈ 2× DDU.
So if your report shows 250 ng/mL DDU, that equals 500 ng/mL FEU — right at the borderline, not definitively elevated.
Always check which unit your lab report uses before comparing your number to any online chart. A result that appears dangerously high in DDU may be perfectly normal in FEU.
What a Negative Result Really Means
A D-dimer level below the cutoff — called a negative result — has a negative predictive value (NPV) of approximately 95% for ruling out DVT or PE in low-to-intermediate-risk patients. This means if your level is normal and your clinical risk score is low, doctors can safely conclude no major clotting event is occurring — without ordering expensive CT scans or ultrasounds.
This is the test’s entire clinical value: ruling out, not ruling in.
Age-Adjusted D-Dimer Cutoffs — What Competitors Don’t Tell You
Why the Standard 500 µg/L Cutoff Fails After Age 50
D-dimer levels naturally increase with aging. Approximately 2–3% of fibrinogen undergoes physiological conversion to fibrin at baseline — and this rate increases as we get older. Applying a flat 500 µg/L cutoff to a 75-year-old leads to thousands of unnecessary CT scans, radiation exposures, and contrast dye reactions every year.
A landmark multicenter study published in JAMA (February 2026) — the most recent major validation — confirmed that using the age-adjusted formula tripled the proportion of patients aged 75+ who could safely avoid imaging, with zero increased failure rate.
📊 Age-Adjusted D-Dimer Cutoff Chart
Formula: Age × 10 µg/L FEU (applies to patients over age 50)
| Age | Standard Cutoff | Age-Adjusted Cutoff | Difference |
|---|---|---|---|
| Under 50 | 500 µg/L | 500 µg/L | No change |
| 55 years | 500 µg/L | 550 µg/L | +50 µg/L |
| 60 years | 500 µg/L | 600 µg/L | +100 µg/L |
| 65 years | 500 µg/L | 650 µg/L | +150 µg/L |
| 70 years | 500 µg/L | 700 µg/L | +200 µg/L |
| 75 years | 500 µg/L | 750 µg/L | +250 µg/L |
| 80 years | 500 µg/L | 800 µg/L | +300 µg/L |
Real Example: Thomas, age 72, receives a D-dimer result of 690 µg/L. Under the standard cutoff, this appears elevated and would typically trigger a CT scan order. Under the age-adjusted cutoff (720 µg/L), Thomas’s result is within normal range — and imaging can be safely avoided.

Critical Limitation You Must Know
The age × 10 formula has been validated for excluding PE and DVT in low-to-intermediate-risk patients only. According to the 2026 PMC narrative review on age-adjusted D-dimer thresholds, this formula is not validated across all 30+ commercial D-dimer assay brands on the market. Your doctor must confirm which assay your lab uses.
For a deeper understanding of how coagulation test results are interpreted alongside D-dimer, see our detailed guide on coagulation test results explained.
For clinical reference, NCBI StatPearls on D-Dimer provides the most current academic overview of assay methodology used by emergency physicians nationwide.
D-Dimer in Special Populations — Pregnancy, Post-Surgery & Post-COVID
D-Dimer During Pregnancy: A Completely Different Chart
Standard D-dimer cutoffs are clinically invalid during pregnancy. The body naturally enters a hypercoagulable state to prepare for delivery, causing D-dimer levels to rise progressively through each trimester.
This is the section every competitor skips entirely — leaving pregnant patients terrified by elevated numbers that are completely expected.
📊 D-Dimer Range Chart by Pregnancy Trimester
| Stage | Expected D-Dimer Range (mg/L FEU) | Clinical Note |
|---|---|---|
| Pre-pregnancy baseline | < 0.5 | Standard cutoff applies |
| 1st Trimester | 0.5 – 1.0 | Early rise begins |
| 2nd Trimester | 0.8 – 1.5 | Progressive elevation |
| 3rd Trimester | 1.5 – 3.0 | Can reach 3× pre-pregnancy baseline |
| Immediate postpartum (0–3 days) | Up to 4.0+ | Peak elevation post-delivery |
| 4–6 weeks postpartum | Gradually normalizes | Returns to pre-pregnancy range |
What This Means For You: If you’re pregnant and received a D-dimer result above 0.5 mg/L, this alone is not cause for alarm. Your OB-GYN will assess clinical risk using the revised Geneva Score or Wells Score criteria — not the D-dimer number in isolation.
If you’re tracking your pregnancy health, our Pregnancy Weight Gain Calculator and Pregnancy Due Date Calculator can help you monitor other key metrics alongside your lab results.

D-Dimer After Surgery: The Recovery Timeline
Post-surgical D-dimer elevation is expected and predictable. Levels typically peak at 48–72 hours post-operation then gradually decline.
| Surgery Type | Time to Normalize |
|---|---|
| Minor procedures (biopsy, laparoscopy) | 1 – 2 weeks |
| Moderate surgery (appendectomy, hernia) | 2 – 4 weeks |
| Major surgery (joint replacement, cardiac, bariatric) | 4 – 6 weeks |
Key Takeaway: If your D-dimer was drawn within 6 weeks of a major operation, an elevated result may be entirely expected and clinically insignificant. Always inform your doctor of the exact surgery date.
Post-COVID Elevated D-Dimer: What 2026 Data Shows
COVID-19 triggers a hypercoagulable inflammatory state that can persist weeks to months after infection. According to data cited by the CDC COVID-19 clinical guidance, D-dimer elevation post-COVID correlates with increased VTE risk — particularly in hospitalized patients.
- Hospitalized COVID patients with D-dimer > 1.0 µg/mL FEU had significantly higher severe outcome rates
- Non-hospitalized patients: lower risk, but persistent mild elevation (0.5–1.0 mg/L) has been documented for 8–12 weeks post-infection
- Routine D-dimer monitoring is not recommended for asymptomatic post-COVID patients unless new clot symptoms appear
High D-Dimer Without a Blood Clot — 12 Common Causes
The Smoke Detector Problem
Think of a D-dimer test as a smoke detector, not a fire locator. It tells you something is triggering the alarm — but it cannot tell you what or where. Many conditions activate the clot-breakdown cascade without an actual dangerous clot being present.
This is why an elevated D-dimer result always requires clinical interpretation — never self-diagnosis.
If you’re experiencing symptoms like leg swelling, chest pain, or shortness of breath alongside an elevated result, use our Symptom Checker to document your symptoms before your doctor’s appointment.
📊 12 Conditions That Elevate D-Dimer Without a Blood Clot
| Category | Specific Conditions |
|---|---|
| Physiological | Aging (>50), pregnancy, postpartum, intense exercise |
| Inflammatory | Sepsis, rheumatoid arthritis, lupus, inflammatory bowel disease |
| Post-procedure | Surgery, trauma, biopsy, catheter placement |
| Cardiovascular | Heart failure, atrial fibrillation, aortic dissection |
| Malignancy | Pancreatic cancer (85% of cases), lung cancer (70%), colon cancer (65%), ovarian cancer (60%) |
| Hepatic | Liver disease (impaired D-dimer clearance) |
| Infectious | COVID-19, severe pneumonia, bacterial sepsis |
| Hematologic | Sickle cell anemia (vaso-occlusive crisis), hemolysis |
Important Note: A false negative is also possible. Factor XIII deficiency causes permanently low D-dimer even in the presence of large clots. Very early clots (within 6–8 hours of formation) may not yet elevate D-dimer levels. The test’s sensitivity drops to approximately 85% for isolated calf DVTs.
When D-Dimer Is Combined With CRP and ESR
D-dimer alone is considered a “dubious marker” in settings of pure inflammation without thrombosis, according to NCBI StatPearls. Doctors often order it alongside CRP (C-reactive protein) and ESR to differentiate inflammatory from thrombotic causes of elevation.
For context on what those markers mean alongside your D-dimer, our articles on CRP test results decoded and ESR normal range levels explain the full picture.
What Happens After a High D-Dimer — Your Decision Guide
The Clinical Decision Flow: Step by Step
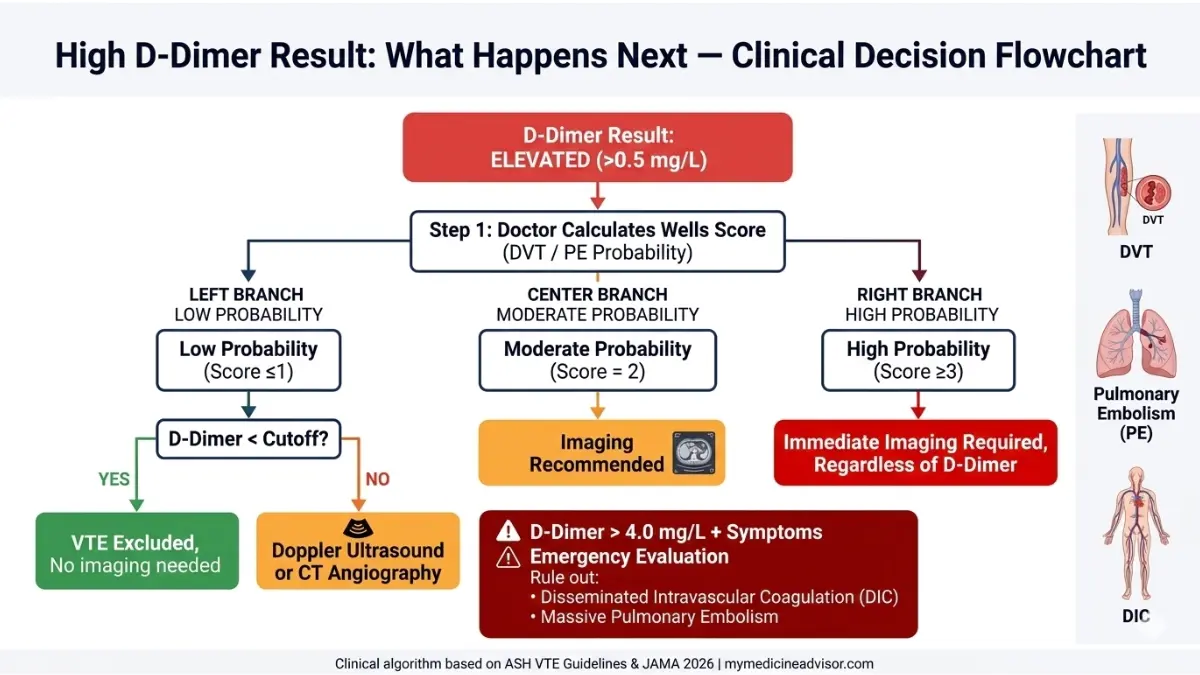
When a D-dimer result comes back elevated, your doctor doesn’t panic — they follow a structured clinical algorithm. Here is the actual process used in U.S. emergency departments and outpatient clinics:
Step 1 — Wells Score Assessment Your doctor calculates your pre-test probability of DVT or PE using the validated Wells Score. This accounts for symptoms (leg swelling, calf tenderness), recent travel/immobility, prior clot history, and other factors.
Step 2 — Stratify by Risk Level
| Wells Score | Pre-Test Probability | Action |
|---|---|---|
| Low (≤1) | ~5% chance of DVT | D-dimer test is appropriate first step |
| Moderate (2) | ~17% chance of DVT | D-dimer + consider imaging |
| High (≥3) | ~53% chance of DVT | Imaging regardless of D-dimer result |
Step 3 — Apply the D-Dimer Result
- Low probability + normal D-dimer → VTE safely excluded. No imaging needed. No further action.
- Low probability + elevated D-dimer → Proceed to ultrasound (DVT) or CT pulmonary angiography (PE).
- Moderate/high probability + any D-dimer → Imaging is performed regardless of D-dimer level.
- D-dimer > 4.0 mg/L + symptoms → Emergency evaluation. Rule out DIC, massive PE, aortic dissection.
When D-Dimer Is Used for Monitoring Treatment
If you’ve been diagnosed with a blood clot and placed on anticoagulation therapy:
- A falling D-dimer = treatment is working. Clot breakdown is resolving.
- A rising D-dimer after stopping therapy = possible recurrence risk. Your doctor may extend anticoagulation.
- A persistently elevated D-dimer on therapy = possible underlying malignancy or unresolved clot. Further workup needed.
For patients interested in understanding how blood clot risk connects to overall cardiovascular health, our guide on blood clots symptoms causes and treatment and lung embolism symptoms and treatment provide connected clinical context.
For authoritative clinical guidelines on VTE management, the American Society of Hematology Blood Clot Patient Resources offers validated treatment pathway information reviewed by hematologists.
Misleading D-Dimer Scenarios to Know
- Anticoagulants (e.g., heparin, warfarin, Xarelto): These do not directly lower D-dimer levels, but by preventing new clot formation, levels may gradually decline. A positive D-dimer while on anticoagulation does not automatically mean treatment failure.
- Factor XIII deficiency: These patients have permanently low D-dimer — even with massive clots. Standard cutoffs do not apply.
- Early-stage clots (within 6–8 hours): May not yet produce measurable D-dimer elevation. If clinical suspicion is high, imaging should proceed regardless.
Expert Panel Summary & Evidence Review
What Leading Hematologists Want You to Know
Dr. Omar Hassan, MD, Internal Medicine: “The most common mistake I see patients make is comparing their D-dimer to a generic internet chart without knowing their age cutoff or which measurement unit their lab used. Context is everything with this test.”
Dr. Vikram Nair, MD, Endocrinology: “An elevated D-dimer is the beginning of a clinical conversation — not the end. It prompts questions, not conclusions. Patients should never interpret this result alone.”
Dr. Meera Shah, MD, OB-GYN: “In my practice, I routinely reassure pregnant patients that a D-dimer above 0.5 mg/L in the third trimester is almost universally expected. The standard cutoff simply does not apply to pregnancy.”
📊 Evidence Strength Summary
| Clinical Claim | Evidence Level | Key Source |
|---|---|---|
| Normal D-dimer cutoff < 500 µg/L FEU | Class I — Strong | NIH, Mayo Clinic Labs, JAMA |
| Age × 10 formula validated for DVT/PE exclusion | Class II — Strong | JAMA Feb 2026 (Le Gal et al.) |
| Pregnancy causes progressive D-dimer elevation | Class II — Moderate | Multiple cohort studies |
| Post-COVID hypercoagulable state elevates D-dimer | Class II — Strong | CDC, NIH Clinical Guidance |
| Age-adjusted cutoff not validated across all assays | Class IIb — Noted Limitation | PMC 2026 Narrative Review |
Related Lab Results You Should Understand
If your doctor ordered a D-dimer as part of a broader coagulation or blood panel, these related guides on mymedicineadvisor.com provide essential context:
- PT/INR test results explained (1.5–5.0 range)
- CBC blood test results explained
- Platelet count results decoded
Frequently Asked Questions — D-Dimer Range Chart
Q1: What is the normal D-dimer level?
Under 0.5 mg/L FEU (500 ng/mL) in most adults under age 50. For patients over 50, the age-adjusted formula (Age × 10 µg/L) applies.
Q2: Is a D-dimer of 0.7 mg/L high?
For a 45-year-old: yes, borderline elevated and warrants clinical review. For a 72-year-old: within normal range using the age-adjusted cutoff (720 µg/L).
Q3: What D-dimer level is considered dangerous?
Values above 4.0 mg/L FEU require urgent clinical evaluation. This range suggests possible DIC, massive pulmonary embolism, or severe systemic disease.
Q4: Can D-dimer be elevated without a blood clot?
Yes — at least 12 conditions elevate it without active thrombosis, including pregnancy, surgery, infection, cancer, liver disease, and normal aging.
Q5: What is the normal D-dimer range during pregnancy?
1st trimester: up to 1.0 mg/L. 2nd trimester: up to 1.5 mg/L. 3rd trimester: up to 3.0 mg/L. Standard cutoffs do not apply during pregnancy.
Q6: What is age-adjusted D-dimer?
A validated formula (Age × 10 µg/L FEU) that raises the cutoff threshold for patients over 50, reducing unnecessary imaging in older adults. Validated in JAMA 2026.
Q7: How long does D-dimer stay elevated after surgery?
1–2 weeks after minor surgery. Up to 4–6 weeks after major operations such as joint replacement, cardiac surgery, or bariatric procedures.
Q8: What is the difference between FEU and DDU units?
FEU (Fibrinogen Equivalent Units) is used by ~70% of U.S. labs. DDU (D-dimer Units) is used by ~30%. FEU cutoff is 500 ng/mL; DDU cutoff is 250 ng/mL. Always confirm which unit your lab used.
Q9: Does COVID-19 raise D-dimer levels?
Yes. COVID-19 causes a hypercoagulable inflammatory state. Elevated D-dimer (often 0.5–2.0 mg/L) can persist 8–12 weeks post-infection, even without active clots.
Q10: Is D-dimer a diagnostic test for blood clots?
No. It is a rule-out screening tool with high sensitivity but low specificity. A negative result helps exclude clots; a positive result only signals the need for further imaging.
Q11: What should I do if my D-dimer is high?
Do not self-diagnose. Contact your healthcare provider immediately, document your symptoms using our Symptom Checker, and share your complete medical history including recent surgeries, infections, and medications.
Reviewed March 2026. This article is updated regularly in alignment with the latest JAMA, NIH, and American Society of Hematology guidelines. For complete diagnostic evaluation, always consult a licensed U.S.-based healthcare provider.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.