On This Page – Quick Medical Summary
What Are Coagulation Test Results?
Your coagulation test results measure how quickly your blood forms clots. These tests—including PT (Prothrombin Time), INR (International Normalized Ratio), aPTT (Activated Partial Thromboplastin Time), and fibrinogen—identify bleeding disorders, monitor blood-thinning medications, and evaluate liver function before surgery.
When Marcus received his coagulation panel results after a routine pre-surgical screening, the INR value of 2.8 caught his attention. His doctor explained this elevated number indicated his blood was clotting slower than normal—critical information before his scheduled knee procedure.
Why You Received This Test
Doctors order coagulation studies for several urgent reasons:
- Medication Monitoring: If you’re taking warfarin (Coumadin), apixaban, or other anticoagulants
- Pre-Surgical Screening: Before any invasive procedure to assess bleeding risk
- Unexplained Bleeding: Frequent nosebleeds, easy bruising, or prolonged bleeding from minor cuts
- Liver Disease Evaluation: The liver produces most clotting factors
- Suspected Clotting Disorders: Family history of hemophilia, von Willebrand disease, or Factor V Leiden
Understanding your coagulation test results requires knowing what each number means and when abnormal values demand immediate medical attention. The National Heart, Lung, and Blood Institute emphasizes that proper interpretation prevents both dangerous bleeding and life-threatening clots.
Quick Visual Guide
| Result Zone | PT (seconds) | INR | What It Means |
|---|---|---|---|
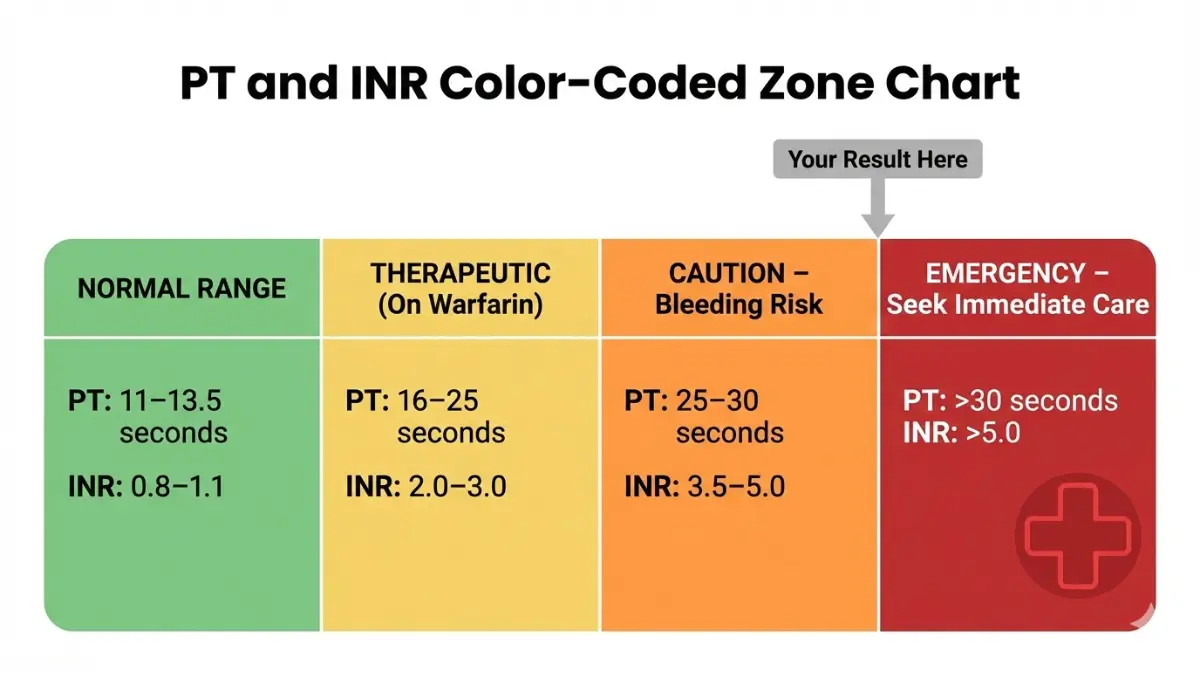
| Normal | 11-13.5 | 0.8-1.1 | Blood clots normally |
| Therapeutic | 16-25 | 2.0-3.0 | On blood thinners (target range) |
| Caution | >25 | >3.5 | High bleeding risk |
| Emergency | >30 | >5.0 | Immediate medical attention needed |
Decode Your Coagulation Test Results: Number by Number
Each component of your coagulation panel reveals specific information about your blood’s clotting ability. Here’s what every number actually means.
PT (Prothrombin Time): What Your Number Means
Normal Range (2026 Updated): 11-13.5 seconds
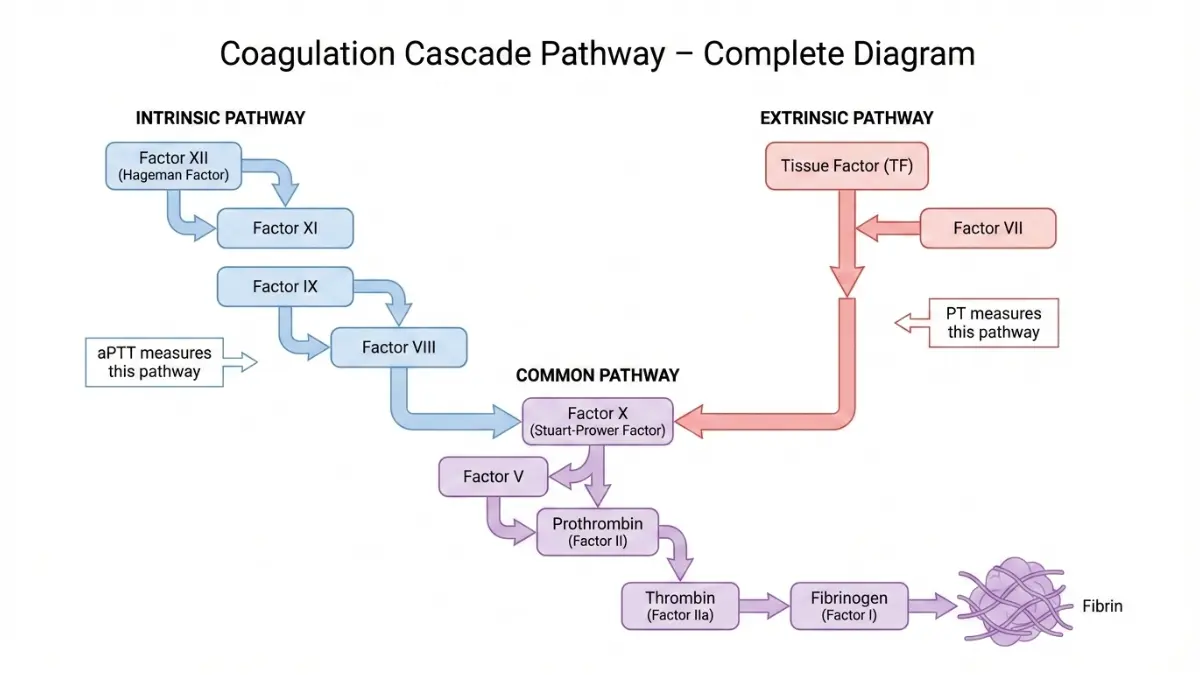
PT measures how long it takes your blood to clot through the extrinsic pathway. If your result shows PT 12.2 seconds, you’re within normal range—your clotting factors II, V, VII, and X are functioning properly.
Elevated PT (>15 seconds) suggests:
- Warfarin therapy (expected if prescribed)
- Vitamin K deficiency
- Liver disease affecting clotting factor production
- Rare inherited factor deficiencies
A 2025 study from the American Society of Hematology found that patients with PT values between 14-16 seconds had 3.2 times higher surgical bleeding risk compared to those with normal values.
INR (International Normalized Ratio): The Critical Measurement
Normal Range: 0.8-1.1 (not on anticoagulants)
Therapeutic Range: 2.0-3.0 (on warfarin for AFib, DVT, or PE)
High-Risk Range: 3.0-4.5 (mechanical heart valves)
The INR standardizes PT results across different laboratories, making it the gold standard for monitoring blood thinners. Think of INR as a universal translator—while PT varies by lab equipment, INR remains consistent.
Real Example: Jennifer’s INR was 3.8 while taking warfarin for atrial fibrillation. Her cardiologist reduced her dose by 1mg because values above 3.5 significantly increase bleeding risk without additional clot prevention benefit.
Patients managing chronic conditions often use tools like our Heart Rate Zone Calculator to monitor overall cardiovascular health alongside coagulation management.
aPTT (Activated Partial Thromboplastin Time) Explained
Normal Range: 25-35 seconds (lab-dependent—check your report’s reference range)
The aPTT evaluates the intrinsic clotting pathway, measuring factors VIII, IX, XI, and XII. This test is particularly important for patients on heparin therapy or those being evaluated for hemophilia.
What Abnormal aPTT Reveals:
- Prolonged (>40 seconds): Heparin therapy, hemophilia A or B, lupus anticoagulant, von Willebrand disease
- Shortened (<25 seconds): Rarely significant, but may indicate hypercoagulability or early-stage DIC
The National Institutes of Health reports that inherited bleeding disorders affect approximately 1 in 1,000 Americans, with aPTT being the primary screening tool.
Fibrinogen Levels: When They’re Tested
Normal Range: 200-400 mg/dL
Fibrinogen, produced by your liver, converts to fibrin during clot formation. Doctors check this level when PT and aPTT are both prolonged or when DIC (disseminated intravascular coagulation) is suspected.
Critical Fibrinogen Thresholds:
- <100 mg/dL: Severe bleeding risk; often requires fibrinogen replacement
- >500 mg/dL: Increased clotting risk; seen in inflammation, pregnancy, or acute infections
Platelet Count in Coagulation Panels
While not technically part of the coagulation cascade testing, platelet count often accompanies these studies. Normal platelet counts range from 150,000-400,000/μL. Our detailed guide on platelet count results explains when low or high values require intervention.
2026 Reference Range Updates
The American College of Pathologists updated therapeutic INR targets in late 2025 for specific conditions:
- Mechanical mitral valves: Now 2.5-3.5 (previously 3.0-4.0)
- Recurrent VTE on warfarin: 2.5-3.5
- AFib with low stroke risk: 2.0-2.5
Why Your Results May Be Abnormal
Abnormal coagulation test results don’t always indicate a bleeding disorder. Multiple factors—from medications to dietary choices—significantly impact these numbers.
Medications That Affect Your Coagulation Tests
Anticoagulants (Expected to Prolong Results):
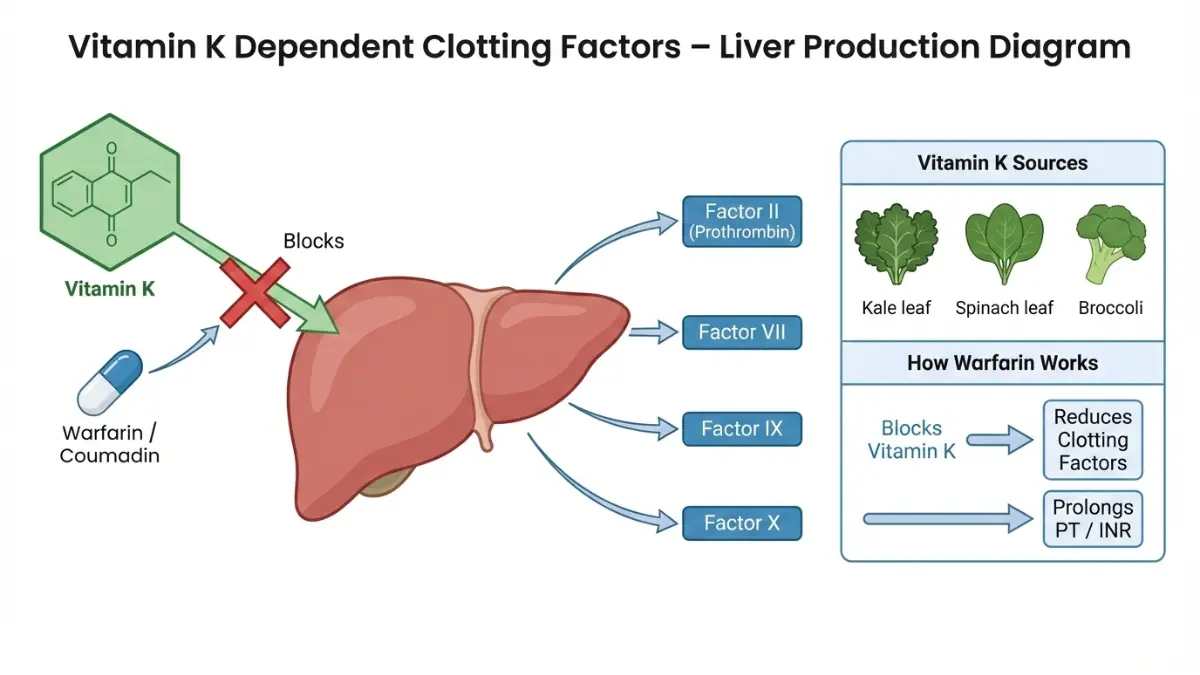
- Warfarin (Coumadin): Increases PT/INR by blocking vitamin K–dependent factors
- Heparin: Prolongs aPTT; monitored every 6 hours during IV therapy
- DOACs (Rivaroxaban, Apixaban, Edoxaban): Minimal PT/INR elevation; require specialized anti-Xa assays
Medications That Unexpectedly Affect Results:
- Antibiotics (especially fluoroquinolones): Can increase INR by 30-50% through gut bacteria disruption
- NSAIDs (ibuprofen, naproxen): Increase bleeding risk but don’t significantly alter PT/INR
- Aspirin: Affects platelet function, not coagulation tests directly
- Certain antifungals (fluconazole): May double INR values within 3-5 days
The FDA’s drug interaction database lists over 120 medications that interact with warfarin alone.
Medical Conditions Causing Abnormal Results
| Condition | PT/INR | aPTT | Fibrinogen | Common Cause |
|---|---|---|---|---|
| Liver Disease | ↑ | Normal/↑ | ↓ | Reduced clotting factor production |
| Vitamin K Deficiency | ↑ | Normal | Normal | Malabsorption, antibiotics |
| Hemophilia A | Normal | ↑↑ | Normal | Factor VIII deficiency |
| DIC | ↑↑ | ↑↑ | ↓↓ | Sepsis, trauma, cancer |
| Lupus Anticoagulant | Normal/↑ | ↑ | Normal | Autoimmune disorder |
Real Patient Case: David’s routine coagulation panel showed PT 18.5 seconds (elevated) and aPTT 32 seconds (normal). Further testing revealed early-stage cirrhosis—his liver couldn’t produce adequate clotting factors. His hepatologist started vitamin K supplementation and scheduled liver function tests every 3 months.
Lifestyle Factors Impacting Blood Clotting
Dietary Vitamin K (Major INR Variable):
- High Vitamin K Foods: Kale (1,062 mcg per cup), spinach (888 mcg), Brussels sprouts, broccoli
- Moderate Vitamin K: Green beans, asparagus, cabbage
- Impact: One kale salad can lower INR by 0.5-1.0 points within 24 hours
Patients on warfarin should maintain consistent vitamin K intake rather than avoiding it entirely. The National Library of Medicine recommends tracking green vegetable consumption weekly.
Other Lifestyle Factors:
- Alcohol: Heavy consumption (>3 drinks/day) can prolong PT by impairing liver function
- Supplements: Fish oil, vitamin E (>400 IU), garlic extract, ginkgo biloba all increase bleeding risk
- Dehydration: Concentrates clotting factors, potentially lowering PT/INR
Lab Timing and Collection Issues
Pre-Analytical Variables Affecting Accuracy:
- Underfilled tubes: Causes falsely prolonged PT/aPTT (citrate ratio incorrect)
- Hemolyzed samples: From difficult blood draws; requires redraw
- Delayed processing: Should reach lab within 4 hours; clotting factors degrade
- Recent heparin flush: If blood drawn from IV line; falsely elevates aPTT
Always request a redraw if your results seem inconsistent with symptoms. Quality labs follow CLSI collection guidelines strictly to ensure accuracy.
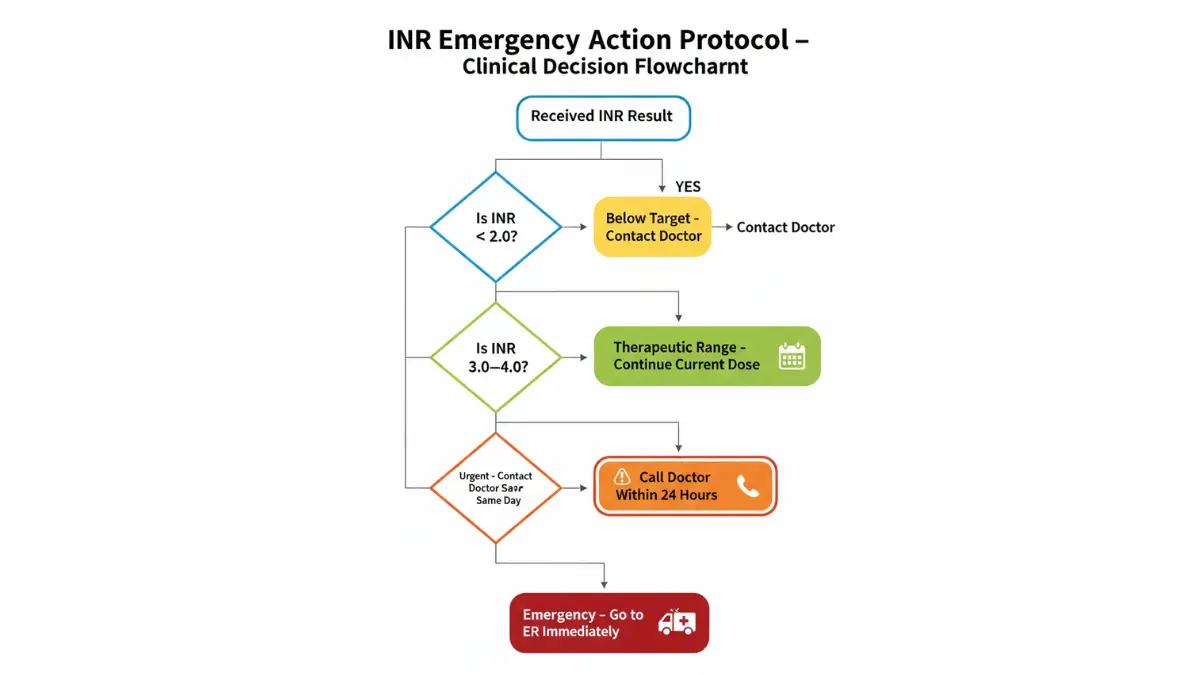
Red Flag Results: When Your Coagulation Numbers Need Urgent Attention
Certain coagulation test results require immediate medical intervention to prevent life-threatening bleeding or clotting events.
Critical INR Levels Requiring Emergency Care
IMMEDIATE ER VISIT (INR >6.0):
- Bleeding risk exceeds 20% within 48 hours
- Even minor trauma can cause severe hemorrhage
- Brain bleed risk increases 8-fold
URGENT DOCTOR CONTACT (INR 4.0-6.0):
- Dose adjustment needed within 24 hours
- Hold warfarin 1-2 doses typically
- Recheck INR in 24-48 hours
Case Study from 2025 Cleveland Clinic Data: Among 847 patients with INR >5.0, those who received vitamin K within 6 hours had 74% lower major bleeding rates compared to those who delayed treatment beyond 24 hours.
Dangerously Prolonged PT/aPTT: What To Do
Emergency Thresholds:
- PT >25 seconds (not on anticoagulants): Suggests severe liver disease, vitamin K deficiency, or rare bleeding disorder
- aPTT >60 seconds (not on heparin): Indicates significant factor deficiency or lupus anticoagulant
The Centers for Disease Control estimates that undiagnosed bleeding disorders affect 1 in 10,000 Americans, often discovered only after surgery or trauma when excessive bleeding occurs.
Symptom-Result Correlation Guide
Match your symptoms to likely test abnormalities:
Active Bleeding Symptoms + Abnormal Results:
- Spontaneous bruising (>2 inches diameter) → Check PT, aPTT, platelet count, fibrinogen
- Gum bleeding lasting >10 minutes → Often platelet disorder; coagulation tests may be normal
- Heavy menstrual bleeding (>7 days or flooding) → Von Willebrand screening (specialized aPTT)
- Persistent nosebleeds (>20 minutes) → If INR >3.0, emergency reversal may be needed
Use our Symptom Checker to assess bleeding patterns, but seek immediate care for uncontrolled bleeding regardless of previous test results.
When to Retest Your Coagulation Panel
2026 Clinical Protocol Timing:
- Warfarin initiation: Daily for 3 days, then weekly until stable, then monthly
- Dose adjustment: Recheck INR in 3-5 days (peak effect timing)
- Illness/antibiotics: Retest within 3-7 days; infections alter INR unpredictably
- Abnormal but asymptomatic: Repeat in 1-2 weeks to confirm; single abnormal test may be lab error
- Pre-surgical: Within 48 hours of procedure if on anticoagulants
Call Your Doctor Within 24 Hours If:
- INR 3.5-5.0 (on warfarin)
- New unusual bruising or petechiae (small red spots)
- Blood in urine or stool
- Severe headache (possible brain bleed warning)
Seek Emergency Care Immediately If:
- INR >6.0
- Active uncontrolled bleeding
- Severe headache with confusion
- Vomiting blood or coffee-ground material
- Black tarry stools (upper GI bleed)
Patients with blood clotting disorders require coordinated care between hematology and primary care providers to balance clot prevention against bleeding risk.
How to Prepare for Coagulation Testing (And What Comes After)
Proper preparation ensures accurate coagulation test results and prevents unnecessary retesting.
Pre-Test Preparation Checklist
Good News: Fasting Usually NOT Required
Unlike lipid panels or blood sugar tests, coagulation studies typically don’t require fasting. You can eat and drink normally before testing unless specifically instructed otherwise for concurrent tests.
Medication Timing Instructions:
- Take warfarin as prescribed: Don’t skip doses before testing; doctors need to see your actual therapeutic level
- Hold morning heparin dose: If on subcutaneous heparin, wait until after blood draw
- Report ALL supplements: Even “natural” products like fish oil affect results
What to Bring to Your Appointment:
- Complete medication list (including over-the-counter drugs and supplements)
- Previous coagulation test results for comparison
- List of recent dietary changes or illnesses
- Questions about result interpretation
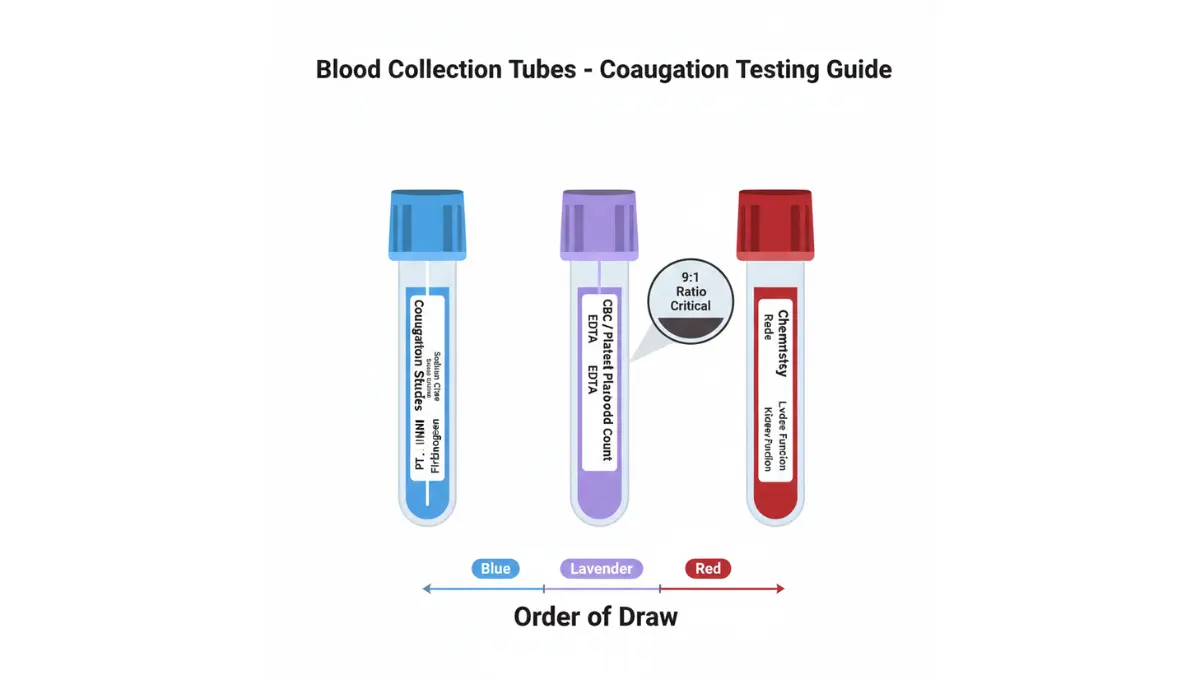
What to Expect During Blood Draw
The phlebotomist will collect blood from a vein, typically in your arm, into special blue-top tubes containing sodium citrate (an anticoagulant that preserves clotting factors). The entire process takes 2-3 minutes.
Why Blue-Top Tubes? The citrate binds calcium, preventing the blood from clotting in the tube while preserving the clotting factors needed for accurate PT/INR/aPTT measurement.
Staying properly hydrated using our Water Intake Calculator recommendations makes blood draws easier and reduces hemolysis (red blood cell breakdown that invalidates results).
How Long Until You Get Results
Standard Laboratory Timing:
- Hospital inpatient: 1-2 hours (stat orders for urgent decisions)
- Outpatient lab: 24-48 hours (non-urgent)
- Point-of-care INR: 2-5 minutes (fingerstick test at clinic or home)
2026 Technology Update: FDA-approved home INR monitors (CoaguChek, INRatio) now feature Bluetooth connectivity, automatically transmitting results to your physician’s portal. A University of Michigan study published in January 2025 showed patients using home monitoring had 42% fewer ER visits for bleeding complications.
Follow-Up Testing Protocols
After Initial Abnormal Result:
- Repeat within 1-2 weeks to rule out lab error
- Add specialized tests if pattern suggests specific disorder (Factor VIII, IX levels; lupus anticoagulant panel; von Willebrand antigen)
Routine Monitoring Schedules:
- Stable on warfarin: Monthly INR checks
- Warfarin dose changes: Weekly until two consecutive therapeutic values
- On heparin infusion: aPTT every 6 hours initially, then every 12-24 hours when stable
Insurance Coverage Notes
Most insurance plans, including Medicare Part B, cover coagulation testing when medically necessary:
- Anticoagulation monitoring: 100% covered (considered preventive)
- Pre-surgical screening: Covered with surgery authorization
- Unexplained bleeding evaluation: Requires documented symptoms
- Routine screening without symptoms: Usually not covered (out-of-pocket cost: $15-75)
Patients managing multiple chronic conditions should review our comprehensive CBC blood test guide to understand how different panels work together for complete health assessment.
Your Coagulation Test Questions Answered
Frequently Asked Questions About Coagulation Results
Q1: Can I eat before a coagulation test?
Yes—coagulation panels (PT, INR, aPTT) don’t require fasting. You can eat and drink normally beforehand. However, if your doctor ordered additional tests like lipid panels, fasting may be necessary for those.
Q2: How long do coagulation test results take?
Standard outpatient labs return results in 24-48 hours. Hospital stat orders take 1-2 hours. Point-of-care INR fingerstick tests provide results in 2-5 minutes at clinics or using home monitors.
Q3: What’s a dangerous INR level?
INR >5.0 indicates high bleeding risk requiring urgent medical attention. INR >6.0 is an emergency—seek immediate care. Even minor injuries can cause severe bleeding at these levels.
Q4: Can stress affect coagulation results?
Acute stress has minimal direct impact on PT/INR/aPTT. However, chronic stress may influence inflammatory pathways affecting fibrinogen levels. Stress doesn’t typically cause clinically significant changes requiring dose adjustments.
Q5: Do I need to stop medications before testing?
Never stop prescribed anticoagulants before testing without physician approval. Doctors need to see your actual therapeutic level. Do report all medications and supplements, as some (antibiotics, antifungals) significantly affect results.
Q6: What’s the difference between PT and INR?
PT measures clotting time in seconds; results vary by lab equipment. INR standardizes PT results using a mathematical formula, allowing accurate comparison across different laboratories—critical for warfarin management.
Q7: Can diet affect my coagulation results?
Yes—vitamin K-rich foods (kale, spinach, Brussels sprouts) can lower INR significantly. If you’re on warfarin, maintain consistent vitamin K intake rather than avoiding these healthy foods entirely.
Q8: How often should coagulation be monitored?
On warfarin: Weekly during initiation, monthly when stable. On heparin: Every 6 hours initially. DOACs (Eliquis, Xarelto): Routine coagulation monitoring not needed; specialized anti-Xa tests only if bleeding occurs.
Q9: Are home INR monitors accurate?
FDA-approved devices (CoaguChek, INRatio) show 95-98% accuracy when used correctly. The American College of Cardiology recommends home monitoring for stable patients on long-term warfarin therapy.
Q10: What causes both PT and aPTT to be high?
Common causes include liver disease (can’t produce clotting factors), vitamin K deficiency, DIC (disseminated intravascular coagulation), or certain anticoagulants. Requires urgent evaluation to determine underlying cause.
Q11: Can alcohol affect coagulation tests?
Heavy alcohol consumption (>3 drinks daily) can prolong PT/INR by impairing liver production of clotting factors. Binge drinking may cause temporary elevation. Avoid alcohol 24 hours before testing for accuracy.
For patients with hereditary clotting concerns, our Genetic Risk Assessment Tool helps evaluate family history patterns that may warrant specialized hematology consultation.
Final Takeaway: Your coagulation test results provide critical information about bleeding and clotting risks. While abnormal values require investigation, most can be managed effectively through medication adjustment, dietary consistency, and appropriate monitoring. Always discuss results with your healthcare provider for personalized interpretation and treatment planning.
Related Resources:
- Understanding iron studies abnormalities alongside coagulation testing
- Complete guide to CRP test results for inflammation assessment
- Comprehensive vitamin D level interpretation
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.