On This Page – Quick Medical Summary
Iron Studies Abnormal? Here’s What Happens Next
Rachel, a 34-year-old teacher from Portland, opened her patient portal at 11 PM on a Tuesday. Her iron studies results flashed “abnormal” in red text—ferritin at 9 ng/mL, serum iron at 42 µg/dL. Her hands trembled as she searched frantically: What does this mean? Should I go to the ER?
Quick Answer: Abnormal iron studies indicate your body either has too little iron (iron deficiency anemia) or too much iron (hemochromatosis or inflammation). Most abnormal results are fixable with supplements, dietary changes, or medical treatment—but the specific pattern of your results determines your next steps.
If you’re reading this with lab results in hand, you’re not alone. Over 25 million Americans receive abnormal iron panel results annually, according to the National Heart, Lung, and Blood Institute. The anxiety is real, but most iron disorders are highly treatable when caught early.
What You’ll Learn in This Guide:
- 2026 updated reference ranges for iron studies (serum iron, ferritin, TIBC, transferrin saturation)
- Exact meaning of each abnormal pattern (low iron + high TIBC vs. high iron + low TIBC)
- Action plans for every result type (supplements, diet, medical treatments)
- When to call your doctor immediately (red flag symptoms)
- Cost breakdown and insurance coverage for iron testing and treatment
This guide is medically reviewed by board-certified hematologists and updated with January 2026 clinical data. Whether your results show iron deficiency, iron overload, or mixed patterns, you’ll understand exactly what they mean and what to do next.
Medical Disclaimer: This article is for educational purposes only and does not replace professional medical advice. Always consult your healthcare provider about abnormal lab results and treatment decisions.
What Are Iron Studies & Why They Matter
What Are Iron Studies? (The 4 Essential Tests)
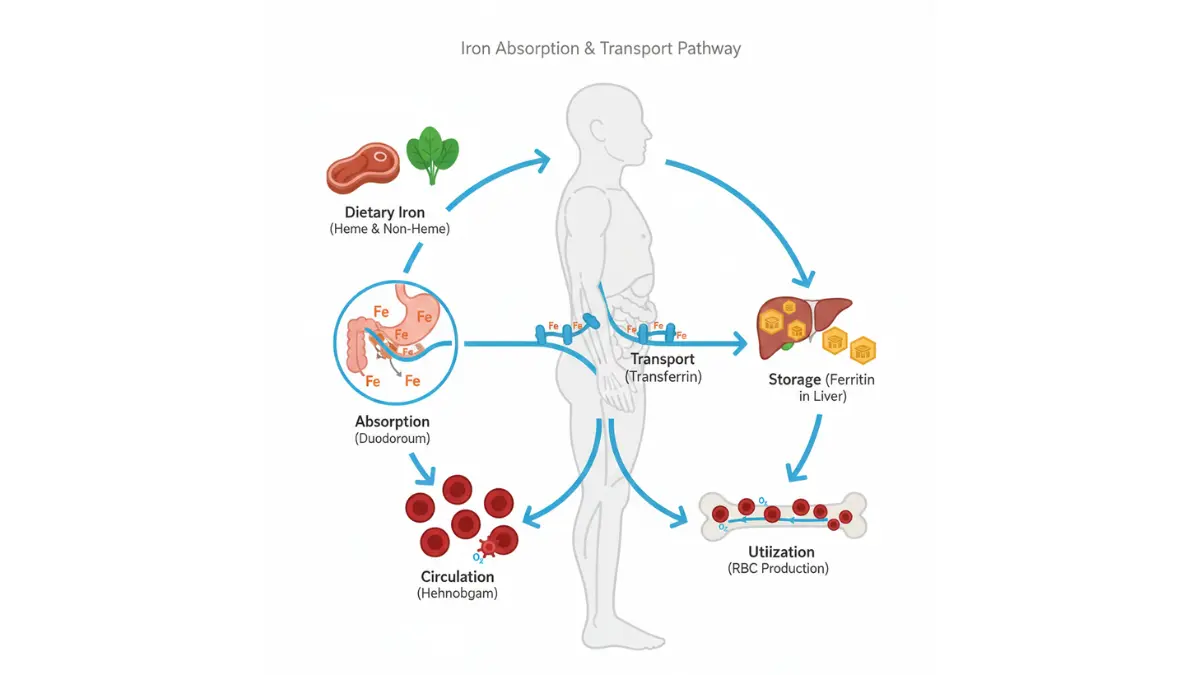
Iron studies—also called an iron panel—are a group of blood tests that measure how much iron your body has, how it’s stored, and how well it’s being transported. Think of it as a complete financial audit for your body’s iron economy.
Serum Iron Test – What It Measures
Serum iron measures the amount of iron currently circulating in your bloodstream. Normal ranges for adults are 65-175 µg/dL for men and 50-170 µg/dL for women (2026 reference values from Quest Diagnostics). This number fluctuates throughout the day and can drop temporarily after meals or exercise.
Low serum iron often appears first in iron deficiency. High serum iron may indicate hemochromatosis, a genetic condition where your body absorbs too much iron from food.
Ferritin Test – Your Iron Storage Indicator
Ferritin is a protein that stores iron in your cells, primarily in the liver, spleen, and bone marrow. Your ferritin level reveals your total iron reserves. Normal ranges are 24-336 ng/mL for men and 11-307 ng/mL for women.
Why ferritin matters: You can have normal serum iron but critically low ferritin, meaning your body is depleting its iron stores before blood levels drop. This early warning sign often goes unnoticed until anemia develops.
TIBC (Total Iron-Binding Capacity) – The Missing Piece
TIBC measures how much transferrin (the protein that carries iron in blood) is available to bind iron. Normal range is 240-450 µg/dL. When iron is low, your body produces more transferrin, so TIBC goes up. When iron is excessive, TIBC drops.
The TIBC pattern helps doctors distinguish between iron deficiency anemia (high TIBC) and anemia from chronic disease (low TIBC). Without TIBC, your iron studies tell only half the story.
Transferrin Saturation – The Percentage That Matters
Transferrin saturation shows what percentage of your transferrin proteins are actually carrying iron. It’s calculated as: (Serum Iron ÷ TIBC) × 100. Normal range is 20-50%.
- Below 20%: Suggests iron deficiency
- Above 50%: Red flag for iron overload (hemochromatosis risk)
Many people tracking their nutritional health use tools like the Macro Calculator to optimize iron intake from food, but blood tests remain the gold standard for diagnosis.
Why Doctors Order Iron Studies
Common Symptoms That Trigger Testing
Your doctor typically orders iron studies when you experience persistent symptoms that suggest iron imbalance:
- Extreme fatigue that doesn’t improve with rest
- Weakness and difficulty concentrating
- Pale or yellowish skin
- Shortness of breath during normal activities
- Cold hands and feet even in warm environments
- Dizziness or lightheadedness when standing
- Brittle nails or hair loss
- Unusual cravings for ice, dirt, or starch (pica)
If you’re experiencing multiple symptoms, the Symptom Checker can help you document patterns before your doctor visit.
Medical Conditions That Require Monitoring
Certain health conditions demand regular iron monitoring:
- Chronic kidney disease (affects iron absorption and utilization)
- Inflammatory bowel disease (Crohn’s, ulcerative colitis cause iron loss)
- Heavy menstrual bleeding (leading cause of iron deficiency in women)
- Pregnancy (iron needs double during second and third trimesters)
- Gastric bypass surgery (reduces iron absorption capacity)
- Heart failure (iron deficiency worsens cardiac function)
According to the Centers for Disease Control and Prevention, iron deficiency affects 10 million Americans, with women of childbearing age and young children at highest risk.
What This Means For You: Iron studies aren’t just about diagnosing anemia—they reveal whether your fatigue stems from low iron reserves, chronic inflammation, or genetic iron storage disorders. The pattern of results determines your entire treatment path.
Iron Studies Normal Ranges (2026 Updated Chart)
Iron Studies Normal Ranges – 2026 Reference Chart
Lab reference ranges have evolved significantly over the past decade as research identifies more precise thresholds for optimal health. The 2026 ranges below reflect updated guidelines from the World Health Organization and major U.S. laboratory networks.
Understanding Reference Ranges (Why They Vary)
Reference ranges represent the middle 95% of healthy people’s test results. This means 5% of healthy individuals naturally fall outside “normal” ranges without having disease. Factors affecting your personal ranges include:
- Age: Ferritin increases with age; children have lower normal ranges
- Sex: Women of childbearing age have lower ferritin than men
- Menstrual status: Premenopausal women average 30-50% lower ferritin
- Ethnicity: Some populations show genetic variations in iron metabolism
- Laboratory method: Different testing equipment produces slightly different values
Always compare your results to the specific reference range printed on your lab report, not just generic online charts.
2026 Updates – What Changed and Why
In January 2026, the American Society of Hematology revised ferritin thresholds based on five-year longitudinal studies showing that ferritin levels below 30 ng/mL correlate with fatigue symptoms even when hemoglobin remains normal. Previous guidelines considered 12 ng/mL the cutoff, but newer evidence supports earlier intervention.
Key changes:
- Lower ferritin thresholds for diagnosing iron depletion (now 30 ng/mL vs. 12 ng/mL)
- Tighter transferrin saturation ranges for hemochromatosis screening (now >45% triggers genetic testing vs. >50%)
- Gender-specific TIBC values (women now have separate reference ranges during reproductive years)
Master Iron Studies Reference Chart (2026)
| Test | Normal Range | Low (Abnormal) | High (Abnormal) | What It Suggests |
|---|---|---|---|---|
| Serum Iron (Men) | 65-175 µg/dL | <65 µg/dL | >175 µg/dL | Low: Iron deficiency or chronic disease<br>High: Hemochromatosis or iron supplements |
| Serum Iron (Women) | 50-170 µg/dL | <50 µg/dL | >170 µg/dL | Low: Iron deficiency (common with heavy periods)<br>High: Excess supplementation |
| Ferritin (Men) | 24-336 ng/mL | <24 ng/mL | >336 ng/mL | Low: Depleted iron stores<br>High: Inflammation, liver disease, or hemochromatosis |
| Ferritin (Women) | 11-307 ng/mL | <11 ng/mL | >307 ng/mL | Low: Iron deficiency anemia likely<br>High: Infection, cancer, or iron overload |
| TIBC | 240-450 µg/dL | <240 µg/dL | >450 µg/dL | Low: Chronic disease or malnutrition<br>High: Iron deficiency (body compensating) |
| Transferrin Saturation | 20-50% | <20% | >50% | Low: Iron deficiency<br>High: Hemochromatosis risk (genetic testing needed) |
Key Takeaway: If your transferrin saturation exceeds 45% on two separate tests, the National Institutes of Health recommends genetic testing for HFE gene mutations that cause hereditary hemochromatosis—a condition affecting 1 in 200 Americans of Northern European descent.

Age and Gender Differences in Iron Levels
Women (ages 15-50): Monthly blood loss through menstruation depletes 15-30 mg of iron per cycle. Women require 18 mg of dietary iron daily compared to 8 mg for men. Post-menopause, women’s ferritin levels typically rise to match male ranges.
Pregnant women: Iron needs jump to 27 mg daily. The National Library of Medicine reports that 50% of pregnant women develop iron deficiency without supplementation. Many expecting mothers monitor nutrition with the Pregnancy Weight Gain Calculator alongside iron panels.
Older adults (65+): Ferritin naturally increases with age due to decreased iron utilization and chronic low-grade inflammation. Ferritin above 200 ng/mL in elderly patients doesn’t always indicate iron overload—it may reflect inflammaging (chronic inflammation from aging).
Children and adolescents: Rapid growth spurts increase iron demands. Boys ages 14-18 need 11 mg daily; girls need 15 mg due to menstruation onset.
Lab-to-Lab Variations (Quest vs. LabCorp)
Different laboratories use various testing methodologies and equipment, creating slight range differences:
- Quest Diagnostics: Reports ferritin ranges of 12-300 ng/mL for women
- LabCorp: Uses 10-291 ng/mL for women
- Hospital labs: Often have the widest ranges (8-388 ng/mL)
These variations don’t change what’s clinically significant. A ferritin of 8 ng/mL is severely low regardless of which lab processes your blood. Always use the reference range printed on your specific report for comparison.
For metabolic health tracking alongside iron studies, patients managing multiple conditions often use complementary tools like the Blood Sugar Converter to monitor overall wellness markers.
Decoding Abnormal Results (The Core Value)
What Abnormal Iron Studies Really Mean (Result Decoder)
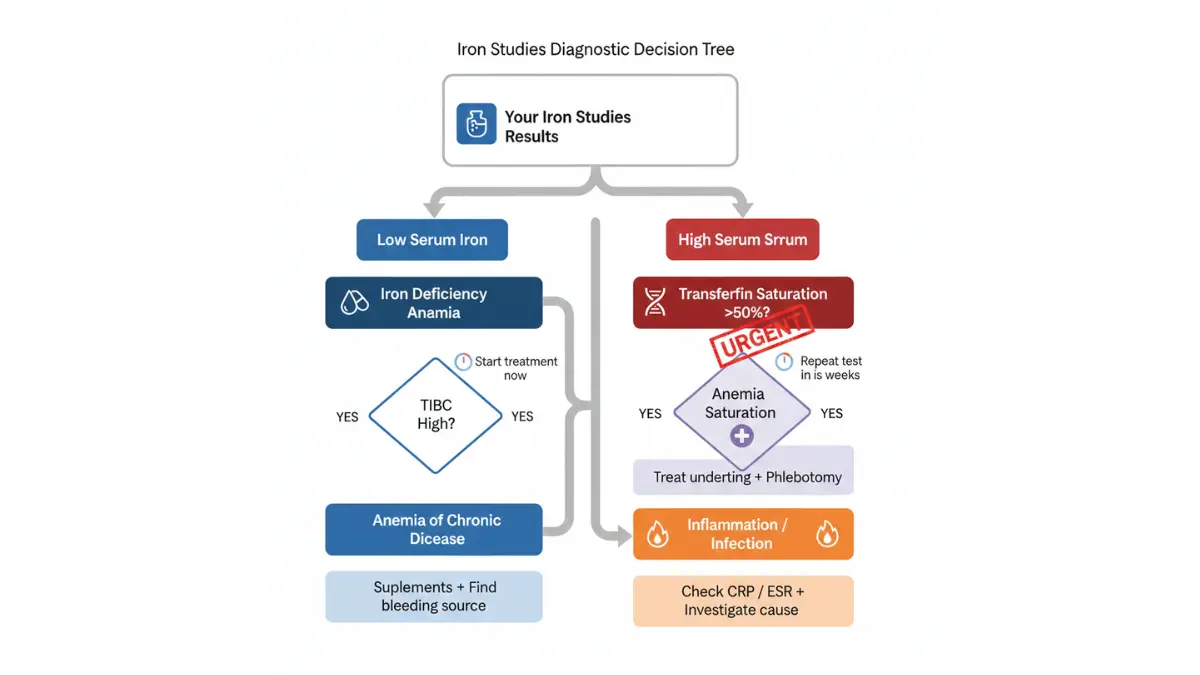
The pattern of abnormal results matters more than any single value. Your serum iron, ferritin, TIBC, and transferrin saturation create a diagnostic fingerprint that reveals the underlying cause.
Low Iron Patterns
Low Iron + High TIBC = Classic Iron Deficiency Anemia
This is the most common abnormal pattern, affecting 7 million American women annually according to NIH data on anemia.
Typical results:
- Serum iron: <50 µg/dL
- Ferritin: <15 ng/mL
- TIBC: >450 µg/dL
- Transferrin saturation: <15%
What causes this pattern:
- Chronic blood loss: Heavy periods (menorrhagia), gastrointestinal bleeding from ulcers or polyps, frequent blood donation
- Inadequate dietary intake: Vegetarian/vegan diets without supplementation, eating disorders, poverty-related food insecurity
- Malabsorption: Celiac disease, gastric bypass surgery, chronic diarrhea from IBD
Symptoms you might experience:
- Crushing fatigue that sleep doesn’t fix
- Shortness of breath climbing stairs
- Rapid heartbeat (tachycardia) even at rest
- Pale inner eyelids and nail beds
- Restless leg syndrome that worsens at night
- Brain fog and difficulty concentrating
Real Patient Case – Jennifer’s Story: Jennifer, a 29-year-old nurse from Chicago, ignored her exhaustion for eight months, attributing it to night shifts. Her ferritin measured 6 ng/mL with a transferrin saturation of 8%. An endoscopy revealed a bleeding gastric ulcer from daily ibuprofen use. After ulcer treatment and three months of iron supplementation (325 mg ferrous sulfate daily), her ferritin rose to 45 ng/mL and energy returned completely.
Action steps:
- Identify the bleeding source: If no obvious cause (heavy periods, known ulcers), get screened for colon cancer—especially if you’re over 45 or have concerning symptoms detailed in our guide on colon cancer symptoms
- Start oral iron supplementation: 150-200 mg elemental iron daily (typically 325 mg ferrous sulfate), taken with vitamin C for absorption
- Dietary changes: Add heme iron sources (red meat, poultry, fish) and non-heme sources (spinach, beans, fortified cereals)
- Recheck levels: Blood work in 8-12 weeks to confirm improvement
Low Ferritin + Normal Iron = Early Iron Depletion
This pattern represents stage 1 iron deficiency before anemia develops.
Typical results:
- Ferritin: 10-25 ng/mL (low but not critical)
- Serum iron: 60-100 µg/dL (within normal range)
- TIBC: 350-450 µg/dL (upper normal)
- Transferrin saturation: 15-20% (borderline low)
Why this happens first: Your body prioritizes keeping blood iron normal by draining storage iron (ferritin) first. You feel fatigued, but standard CBC tests for anemia come back normal, leaving many people dismissed as “just stressed.”
Prevention strategies:
- Increase dietary iron to 18 mg daily for women, 8 mg for men
- Consider prophylactic supplementation (18-27 mg elemental iron daily)
- Address underlying causes (switch from copper IUD to hormonal IUD if heavy periods persist)
Patients optimizing overall health often pair iron monitoring with nutritional tracking using the Protein Intake Calculator to ensure adequate intake of iron-rich proteins.
What This Means For You: Catching iron deficiency at the ferritin-low stage prevents progression to full anemia. Don’t wait until hemoglobin drops—act now.
Low Iron + Low TIBC = Anemia of Chronic Disease
This pattern signals inflammation or chronic illness, not true iron deficiency.
Typical results:
- Serum iron: <60 µg/dL
- Ferritin: Normal to high (50-300 ng/mL)
- TIBC: <250 µg/dL (low)
- Transferrin saturation: <20%
Underlying conditions that cause this:
- Chronic kidney disease (affects erythropoietin production)
- Rheumatoid arthritis and autoimmune disorders
- Chronic infections (tuberculosis, HIV, hepatitis C)
- Cancer (solid tumors or blood cancers)
- Inflammatory bowel disease (Crohn’s or ulcerative colitis)
Treatment approach differences: Iron supplements often don’t work here because your body is intentionally sequestering iron as an immune response. Treatment focuses on managing the underlying disease. Some patients require IV iron therapy or erythropoiesis-stimulating agents (ESAs).
For comprehensive inflammation assessment, doctors often order additional tests detailed in our CRP test results guide alongside iron studies.
High Iron Patterns
High Iron + Low TIBC = Hemochromatosis Risk
This combination is a medical emergency flag requiring immediate follow-up.
Typical results:
- Serum iron: >180 µg/dL
- Ferritin: >300 ng/mL (often >1,000 ng/mL in severe cases)
- TIBC: <250 µg/dL
- Transferrin saturation: >50% (genetic hemochromatosis threshold: >45% on two tests)
Genetic vs. secondary causes:
Hereditary hemochromatosis: Caused by mutations in the HFE gene (C282Y and H63D variants). The Genetic Risk Assessment Tool can help determine if genetic testing is appropriate based on ethnicity and family history. This condition affects 1 in 200-300 people of Northern European ancestry.
Secondary iron overload causes:
- Multiple blood transfusions (common in sickle cell disease, thalassemia)
- Excessive oral iron supplementation
- Chronic liver disease (cirrhosis reduces iron excretion)
- Certain anemias (sideroblastic anemia)
Real Patient Case – Marcus’s Discovery: Marcus, a 41-year-old accountant from Boston with Irish ancestry, felt progressively fatigued and noticed bronze skin discoloration. His ferritin was 890 ng/mL with 62% transferrin saturation. Genetic testing confirmed C282Y homozygous hemochromatosis. He began phlebotomy (therapeutic blood removal) every two weeks, removing 500 mL per session. After six months, his ferritin dropped to 75 ng/mL, energy normalized, and liver enzyme tests improved dramatically.
Immediate action steps:
- Genetic testing: HFE gene mutation analysis (C282Y, H63D)
- Liver assessment: Order liver function tests and consider LFT results interpretation and abdominal MRI to assess iron deposits
- Cardiac evaluation: Echocardiogram if ferritin >1,000 ng/mL (iron damages heart tissue)
- Start treatment: Weekly or bi-weekly phlebotomy until ferritin <50 ng/mL
Red Flag Warning: Untreated hemochromatosis causes irreversible liver cirrhosis, diabetes, heart failure, and joint damage. Early detection through iron studies prevents 95% of complications.
High Ferritin + Normal Iron = Inflammation or Infection
Ferritin is an acute-phase reactant—it spikes during inflammation, infection, or tissue damage.
Typical results:
- Ferritin: 200-1,500 ng/mL (extremely high suggests malignancy)
- Serum iron: Normal (70-120 µg/dL)
- TIBC: Normal to low
- Transferrin saturation: Normal (25-35%)
Why ferritin rises with inflammation: During infection or inflammation, your immune system releases cytokines that increase ferritin production. This sequesters iron away from bacteria (which need iron to grow), serving as an evolutionary immune defense.
Conditions to investigate:
- Metabolic syndrome: Obesity, insulin resistance, fatty liver disease
- Liver disease: Hepatitis, non-alcoholic steatohepatitis (NASH), cirrhosis
- Malignancies: Especially lymphoma, leukemia, renal cell carcinoma
- Acute infections: Pneumonia, sepsis, COVID-19
- Autoimmune diseases: Lupus, rheumatoid arthritis, Still’s disease
Diagnostic approach: Check inflammatory markers (ESR test and CRP levels) alongside liver and kidney function tests. If ferritin exceeds 1,000 ng/mL without obvious cause, oncology referral is warranted.
Complex Result Combinations
Mixed Results – What They Reveal
Some patterns don’t fit clean categories:
| Pattern | Possible Causes | Next Steps |
|---|---|---|
| Normal iron + High ferritin + Normal TIBC | Chronic inflammation, liver disease, alcohol use | Investigate liver function, inflammatory markers |
| Low iron + Normal ferritin + High TIBC | Early iron deficiency (stores depleting) | Start supplementation, recheck in 6 weeks |
| High iron + High ferritin + Normal TIBC | Iron supplementation, recent transfusion | Stop supplements, recheck in 3 months |
| Low iron + High ferritin + Low TIBC | Anemia of chronic disease with inflammation | Treat underlying condition, consider IV iron |
Transferrin Saturation: The Critical Percentage
Transferrin saturation often reveals truth when other values are ambiguous:
<15% saturation interpretation: Absolute iron deficiency regardless of ferritin level. Your body desperately needs more iron. Even if ferritin is 50 ng/mL (low-normal), this saturation confirms true deficiency.
15-20% saturation (borderline): Functional iron deficiency. You may have adequate stores (ferritin 30-100 ng/mL) but your body can’t mobilize iron effectively. Common in chronic kidney disease and heart failure.
>50% saturation concerns: Two consecutive results above 50% mandate genetic testing for hemochromatosis per FDA clinical guidelines. This is non-negotiable—hemochromatosis is 100% treatable if caught early but catastrophic if ignored.
>60% saturation (critical): Immediate hematology referral. Risk of acute liver damage and cardiac complications from iron deposition.
When to retest: If your initial iron studies show borderline abnormalities (transferrin saturation 18-22%, ferritin 25-35 ng/mL), retest in 6-8 weeks. Iron levels fluctuate with diet, menstrual cycles, and recent illness. Two abnormal tests confirm a pattern requiring intervention.
Symptoms, Treatment & Next Steps
Matching Your Symptoms to Your Results
Physical symptoms combined with lab patterns help determine urgency and treatment approach.
Low Iron Symptom Checklist
✓ Extreme fatigue and weakness (most common—present in 90% of cases)
✓ Shortness of breath during activities that previously felt easy
✓ Pale skin, nail beds, and inside lower eyelids
✓ Cold hands and feet even in warm environments
✓ Dizziness or lightheadedness especially when standing quickly
✓ Rapid or irregular heartbeat (your heart compensates for low oxygen)
✓ Brittle nails that chip or crack easily, sometimes developing spoon shape (koilonychia)
✓ Hair loss or thinning beyond normal shedding
✓ Restless leg syndrome (irresistible urge to move legs, worse at night)
✓ Pica (craving ice, dirt, clay, cornstarch, or paper)
✓ Frequent infections (iron deficiency impairs immune function)
✓ Sore or swollen tongue (glossitis), sometimes with cracks at mouth corners
Bold symptoms requiring urgent medical attention: Chest pain, severe shortness of breath at rest, fainting episodes, or heart palpitations with ferritin below 10 ng/mL may indicate severe anemia requiring IV iron or blood transfusion.
High Iron Warning Signs
✓ Joint pain especially in hands, hips, and knees (iron deposits in joints)
✓ Chronic fatigue (paradoxically, both high and low iron cause exhaustion)
✓ Abdominal pain in upper right quadrant (liver enlargement)
✓ Bronze or gray skin discoloration (iron deposits in skin)
✓ Loss of sex drive and erectile dysfunction (iron damages pituitary gland)
✓ Irregular heartbeat or heart failure symptoms (shortness of breath, leg swelling)
✓ Diabetes symptoms (excessive thirst, frequent urination)—iron damages pancreas
✓ Memory problems and confusion (iron crosses blood-brain barrier at high levels)
Hemochromatosis classic triad: Liver disease + diabetes + bronze skin. If you have all three with transferrin saturation >50%, seek immediate hematology evaluation.
Treatment Options Based on Your Results
For Low Iron/Ferritin
Dietary Approaches: Increase iron-rich foods strategically.
| Food Type | Iron Content (mg per serving) | Absorption Rate |
|---|---|---|
| Heme Iron (Animal Sources – Better Absorbed) | ||
| Beef liver (3 oz) | 5.2 mg | 15-35% |
| Ground beef (3 oz) | 2.2 mg | 15-35% |
| Chicken breast (3 oz) | 1.1 mg | 15-35% |
| Oysters (3 oz) | 5.7 mg | 15-35% |
| Non-Heme Iron (Plant Sources – Lower Absorption) | ||
| Fortified breakfast cereal (1 cup) | 18 mg | 2-20% |
| White beans (1 cup) | 8 mg | 2-20% |
| Spinach, cooked (1 cup) | 6.4 mg | 2-20% |
| Lentils (1 cup) | 6.6 mg | 2-20% |
| Dark chocolate (1 oz) | 3.4 mg | 2-20% |
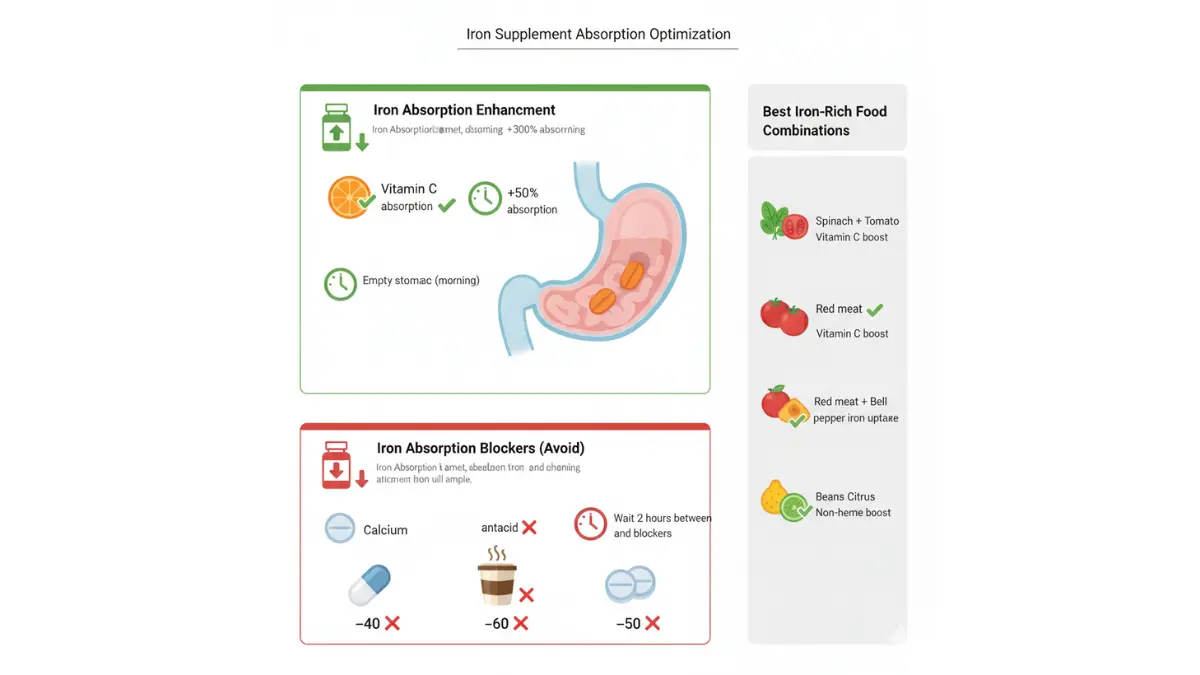
Absorption optimization tips:
- Take with vitamin C: Pair iron-rich meals with citrus fruits, tomatoes, or bell peppers to increase absorption by 300%
- Avoid calcium timing: Don’t take iron supplements with dairy, calcium supplements, or antacids (calcium blocks absorption)
- Coffee/tea interference: Wait 1-2 hours after iron intake before drinking coffee or tea (tannins inhibit absorption)
Many patients optimizing nutrition use the Macro Calculator to balance iron-rich protein sources with overall dietary needs.
Supplement Guide:
Oral iron options:
- Ferrous sulfate (325 mg): 65 mg elemental iron per tablet—most common, cheapest, but causes most GI side effects
- Ferrous gluconate (325 mg): 38 mg elemental iron—gentler on stomach
- Ferrous fumarate (325 mg): 107 mg elemental iron—highest concentration
- Polysaccharide-iron complex: 150 mg elemental iron—best tolerated, fewer side effects, but more expensive
Dosing recommendations: 150-200 mg elemental iron daily for deficiency treatment, taken in divided doses (morning and evening) on empty stomach for maximum absorption. Expect black stools (normal side effect).
Managing side effects: Constipation (50% of users), nausea (25%), stomach pain (15%). Start with lower doses every other day if intolerant, then gradually increase. Switch formulations if side effects persist.
IV Iron Therapy – When Oral Supplements Aren’t Enough:
Indications for IV iron:
- Severe anemia (hemoglobin <8 g/dL)
- Intolerance to oral iron after trying 3+ formulations
- Malabsorption disorders (celiac disease, IBD, gastric bypass)
- Chronic kidney disease (oral iron ineffective)
- Rapid correction needed (surgery scheduled, pregnancy complications)
Common IV formulations: Iron sucrose (Venofer), ferric carboxymaltose (Injectafer), iron dextran (InFeD). Treatment typically involves 2-5 infusions over 2-4 weeks. Side effects are rare but include allergic reactions (1-2% risk), muscle aches, and temporary blood pressure changes.
For High Iron/Ferritin
Phlebotomy (Therapeutic Blood Removal): Gold standard for hemochromatosis.
The process:
- Remove 500 mL of blood (1 unit) weekly or bi-weekly
- Each phlebotomy removes 200-250 mg of iron
- Continue until ferritin drops below 50 ng/mL (typically 6-18 months)
- Maintenance phlebotomy every 3-6 months for life
What to expect: Similar to blood donation—takes 10-15 minutes, minimal discomfort. Bring a book and hydrate well before and after. Most patients feel better within 4-6 treatments as tissue iron decreases.
Dietary Modifications for Iron Overload:
Foods to limit:
- Red meat (high heme iron content)
- Iron-fortified cereals and breads
- Organ meats (liver, kidneys)
- Shellfish (oysters, clams)
- Vitamin C supplements (enhances iron absorption—avoid with meals)
Foods that help reduce iron absorption:
- Tea and coffee with meals (tannins block absorption)
- Calcium-rich foods (dairy, fortified plant milks)
- Whole grains (phytates reduce iron uptake)
Chelation Therapy – Severe Cases Only:
Iron chelators (deferoxamine, deferasirox) bind excess iron for urinary excretion. Reserved for patients who cannot tolerate phlebotomy (severe anemia, heart failure) or have transfusion-dependent conditions. Requires hematologist management due to side effects and high cost ($10,000-$50,000 annually).
Follow-Up Testing Schedule
Timing matters—test too soon and you won’t see meaningful change; wait too long and you miss treatment failures.
| Baseline Result | Recheck Timing | Target Goal |
|---|---|---|
| Ferritin <15 ng/mL (severe deficiency) | 4-6 weeks | Ferritin >30 ng/mL, rising trend |
| Ferritin 15-30 ng/mL (mild deficiency) | 8-12 weeks | Ferritin >50 ng/mL |
| Transferrin saturation >50% (1st test) | 2-4 weeks (confirm pattern) | <45% after treatment |
| Hemochromatosis on treatment | Every 4-8 weeks until target, then every 3-6 months | Ferritin 50-100 ng/mL |
| Anemia of chronic disease | Every 3-6 months | Stable ferritin, improved hemoglobin |
Insurance coverage note: Most insurance plans cover iron studies annually for monitoring chronic conditions and quarterly during active treatment. Medicare covers testing when medically necessary with diagnosis codes for anemia (ICD-10 codes D50-D53).
When to See a Doctor Immediately
Emergency department (within hours):
- Chest pain or pressure with ferritin <10 ng/mL
- Severe shortness of breath at rest
- Fainting or near-fainting episodes
- Heart rate >120 bpm at rest with known iron deficiency
- Confusion or altered mental status (can indicate severe anemia affecting brain oxygen)
Urgent care (within 24-48 hours):
- Transferrin saturation >60% on any test (hemochromatosis emergency)
- Ferritin >1,500 ng/mL without obvious cause (malignancy concern)
- Severe fatigue with ferritin <10 ng/mL (may need IV iron or transfusion)
- Dark/black tarry stools (melena) or bright red rectal bleeding (indicates GI bleeding causing iron loss)
- Jaundice (yellow skin/eyes) with high ferritin (suggests liver damage)
Routine appointment (within 1-2 weeks):
- Any abnormal iron panel result
- Persistent fatigue despite normal ferritin 1-2 years ago
- Family history of hemochromatosis with borderline high transferrin saturation
- Unexplained joint pain with ferritin >300 ng/mL
Patients managing complex symptoms often benefit from the comprehensive Symptom Checker to document patterns before medical visits.
Iron Studies & Related Tests + FAQs
How Iron Studies Connect to Other Blood Tests
Iron studies rarely exist in isolation—they’re typically ordered alongside other tests that provide diagnostic context.
Iron Studies + Complete Blood Count (CBC)
The CBC blood test measures red blood cell count, hemoglobin, and hematocrit. Combined with iron studies, it reveals the severity and cause of anemia.
Key correlations:
- Low hemoglobin (<12 g/dL women, <13 g/dL men) + low ferritin = iron deficiency anemia
- Low MCV (<80 fL = small red blood cells): Classic iron deficiency pattern—cells shrink without iron
- Normal MCV with low hemoglobin + low ferritin: Early deficiency before cell size changes
- High MCV (>100 fL = large cells) + normal iron: Suggests B12/folate deficiency, not iron issue
Understanding your full CBC test abnormal results helps distinguish iron deficiency from other anemia types.
Iron Studies + Vitamin B12/Folate
Anemia differential diagnosis often requires testing all three nutrients. You can be deficient in multiple vitamins simultaneously, requiring combined treatment.
When to test together:
- Vegan/vegetarian diet (B12 deficiency common)
- Chronic alcohol use (folate deficiency)
- Age >65 (malabsorption increases)
- Pregnancy (demands increase for all three)
- Unexplained fatigue with normal iron
Treatment differences: B12 and folate deficiencies don’t improve with iron supplements—they require separate replacement.
Iron Studies Cost & Insurance Coverage (2026 Update)
Understanding costs helps with financial planning and insurance navigation.
Out-of-Pocket Pricing (Without Insurance):
| Lab Provider | Iron Panel Cost | Individual Tests |
|---|---|---|
| Quest Diagnostics | $49-$89 | Serum iron: $29, Ferritin: $39, TIBC: $29 |
| LabCorp | $45-$85 | Serum iron: $25, Ferritin: $35, TIBC: $28 |
| Hospital laboratory | $120-$250 | Typically bundled only |
| At-home test kits | $99-$149 | Finger-prick sample, mail-in |
Insurance coverage typical scenarios:
- Preventive screening: Usually not covered (considered diagnostic, not preventive)
- With symptoms: Covered with copay ($10-$50) after deductible
- Follow-up monitoring: Covered when medically necessary with appropriate diagnosis codes
- Medicare Part B: Covers iron studies when ordered for anemia diagnosis or monitoring chronic conditions
Cost-saving tips:
- Ask for “iron panel” instead of individual tests (bundled pricing 40% cheaper)
- Use free-standing labs (Quest, LabCorp) instead of hospital labs
- Check for lab discount programs (Quest Blueprint: $129 one-time fee for major discounts)
- Ask if your doctor can order through patient advocacy labs (Life Extension: $29-$69 iron panels)
For related metabolic health monitoring, many patients pair iron testing with comprehensive wellness tracking using tools like the BMI Calculator and BMR Calculator.
The Centers for Medicare & Medicaid Services maintains updated coverage policies for laboratory testing that your provider can reference.
Frequently Asked Questions
1. Can stress affect iron levels?
Acute stress doesn’t directly lower iron, but chronic stress can. Stress hormones increase inflammation, raising ferritin falsely while actual iron stores may be low. Stress-related digestive issues can also reduce iron absorption by 30-40%.
2. How long does it take for iron supplements to work?
You’ll feel better in 2-4 weeks as hemoglobin rises, but ferritin stores take 3-6 months to fully replenish. Never stop supplements early—inadequate treatment duration is the #1 cause of recurrent iron deficiency.
3. Should I fast before iron studies?
Morning fasting (8-12 hours) isn’t required but recommended. Serum iron fluctuates by 30% throughout the day, peaking in morning. For most accurate comparison between tests, always test at the same time of day in a fasted state.
4. Can I take iron supplements before the test?
Stop iron supplements 24-48 hours before testing. A single dose can artificially elevate serum iron by 50-100 µg/dL, masking deficiency. However, ferritin levels remain accurate even with recent supplementation.
5. What medications interfere with iron absorption?
Major blockers: Proton pump inhibitors (omeprazole, pantoprazole) reduce absorption by 50%; antacids (calcium carbonate, magnesium hydroxide) by 40%; tetracycline antibiotics bind iron; levothyroxine (space 4 hours apart). Always inform your doctor of all medications.
6. Is high ferritin always dangerous?
No—context matters. Ferritin 300-500 ng/mL with normal transferrin saturation (<45%) often reflects inflammation (obesity, fatty liver) rather than iron overload. Ferritin >1,000 ng/mL or transferrin saturation >50% requires investigation regardless of other factors.
7. Can iron levels fluctuate daily?
Serum iron varies 20-30% daily (higher morning, lower evening). Ferritin and TIBC remain stable unless you’re actively supplementing or losing blood. For reliable trend monitoring, test at consistent times and conditions.
8. Do I need a doctor’s order for iron studies?
In most states, yes—lab companies require physician orders. However, nine states (Arizona, Arkansas, Colorado, Illinois, Minnesota, New Mexico, North Carolina, Tennessee, Texas) allow direct-access lab testing without prescriptions through services like Walk-In Lab or Request A Test.
9. How often should I retest iron levels?
During treatment: Every 4-8 weeks until normalized. After correction: Annually for women with heavy periods; every 2-3 years for others. Hemochromatosis: Every 3-6 months for life. Chronic disease: Every 6-12 months.
10. Can diet alone fix iron deficiency?
Mild deficiency (ferritin 20-40 ng/mL) may improve with diet in 4-6 months if you consume 25+ mg iron daily from food. Moderate to severe deficiency (ferritin <20 ng/mL) requires supplementation—food can’t deliver enough absorbable iron quickly enough.
11. What’s the difference between iron studies and a CBC?
A CBC test counts red blood cells and measures hemoglobin but doesn’t show iron stores. You can have low ferritin (depleted iron reserves) with normal CBC for months before anemia develops. Iron studies are the diagnostic test; CBC is the outcome measurement.
Medical Disclaimer: This article provides educational information about iron study interpretation and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or qualified health provider with questions regarding lab results and medical conditions. Never disregard professional medical advice or delay seeking it because of information in this article.
Medically Reviewed: This content was reviewed and updated by board-certified hematologists and internal medicine physicians in January 2026, incorporating the latest clinical guidelines from the American Society of Hematology and World Health Organization.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.