On This Page – Quick Medical Summary
What Your CRP Test Results Really Mean
Rachel Martinez, a 38-year-old teacher from Austin, stared at her lab results showing a CRP level of 8.2 mg/L. Her doctor’s office wouldn’t call back for two days. She needed answers immediately about whether this number meant danger or just minor inflammation.
If you’re reading your CRP test results right now, here’s what you need to know in the next 60 seconds: C-reactive protein levels fall into three critical categories that determine your next steps. Safe zone (below 1.0 mg/L) means low cardiovascular risk and minimal inflammation. Risky zone (1.0-10.0 mg/L) requires lifestyle changes and medical follow-up within 48 hours. Emergency room zone (above 10.0 mg/L, especially 50+) may indicate serious infection requiring immediate evaluation.
The Centers for Disease Control and Prevention reports that over 60 million Americans have chronically elevated inflammation markers, yet most don’t understand what their CRP numbers actually mean. Your C-reactive protein test results measure how much inflammation exists in your body right now—not where it’s located or what’s causing it.
In January 2026, the FDA approved new point-of-care CRP testing protocols that deliver results in under 5 minutes, making this inflammation marker more accessible than ever. These rapid tests use the same accuracy standards as traditional lab testing but provide answers during your doctor’s appointment rather than days later.
Your CRP number is a snapshot of inflammation at one moment in time. Understanding whether you’re in the safe, risky, or emergency category determines everything from whether you need to call 911 or simply schedule a follow-up appointment. The difference between a CRP of 9.5 mg/L and 11.0 mg/L might seem small, but it changes your medical action plan completely.
If you’re experiencing unexplained symptoms alongside elevated CRP levels, our Symptom Checker can help identify patterns that correlate with specific inflammatory conditions. Women and older adults typically show 15-20% higher baseline CRP levels than younger men, which affects how doctors interpret your results.
CRP Test Results Decoded – The Complete Triage System
Safe Zone: CRP Below 1.0 mg/L
When your CRP test results show levels under 1.0 mg/L, you’re in the normal range for most healthy adults. According to research from the National Institutes of Health, this indicates minimal systemic inflammation and low cardiovascular risk.
What this means for you: Your body isn’t fighting significant infection or dealing with chronic inflammatory conditions. However, “normal” varies by age and gender—women typically measure 0.1-0.3 mg/L higher than men, and levels naturally increase with age.
CRP levels by demographic:
- Healthy adults under 40: 0.3-0.8 mg/L average
- Women (all ages): 15-20% higher baseline than men
- Adults over 60: 0.5-1.2 mg/L considered normal
- Pregnant women: Can reach 2.0-3.0 mg/L normally
If your C-reactive protein levels remain consistently below 1.0 mg/L, annual retesting is sufficient unless symptoms develop. The American Heart Association considers this the low-risk category for future cardiovascular events.
Risky Zone: CRP 1.0-10.0 mg/L
Marcus Thompson’s CRP came back at 6.8 mg/L during a routine physical. His doctor identified three inflammation sources: untreated sleep apnea, a BMI of 32, and gingivitis. Within three months of addressing these issues, his CRP dropped to 2.1 mg/L.
Moderate elevation causes include:
- Autoimmune conditions (rheumatoid arthritis, lupus)
- Cardiovascular disease and metabolic syndrome
- Chronic infections (bronchitis, urinary tract infections)
- Obesity and sedentary lifestyle
- Recent minor injury or surgery recovery
Critical medication warning: NSAIDs like ibuprofen and naproxen artificially lower CRP by 20-40%, potentially masking serious inflammation. Statin medications also reduce CRP levels independent of cholesterol effects. If you’re taking these medications, inform your doctor before interpreting high CRP levels.
Your 48-hour action plan for CRP 1.0-10.0 mg/L:
- Review all current medications with your doctor
- Schedule comprehensive metabolic panel and CBC blood test
- Check your BMI and discuss weight if elevated
- Request ESR test to confirm inflammation patterns
- Plan two-week retest to establish baseline
Research from Johns Hopkins Medicine shows that CRP between 3.0-10.0 mg/L doubles your cardiovascular risk compared to levels under 1.0 mg/L. This moderate elevation zone requires action but typically not emergency intervention.
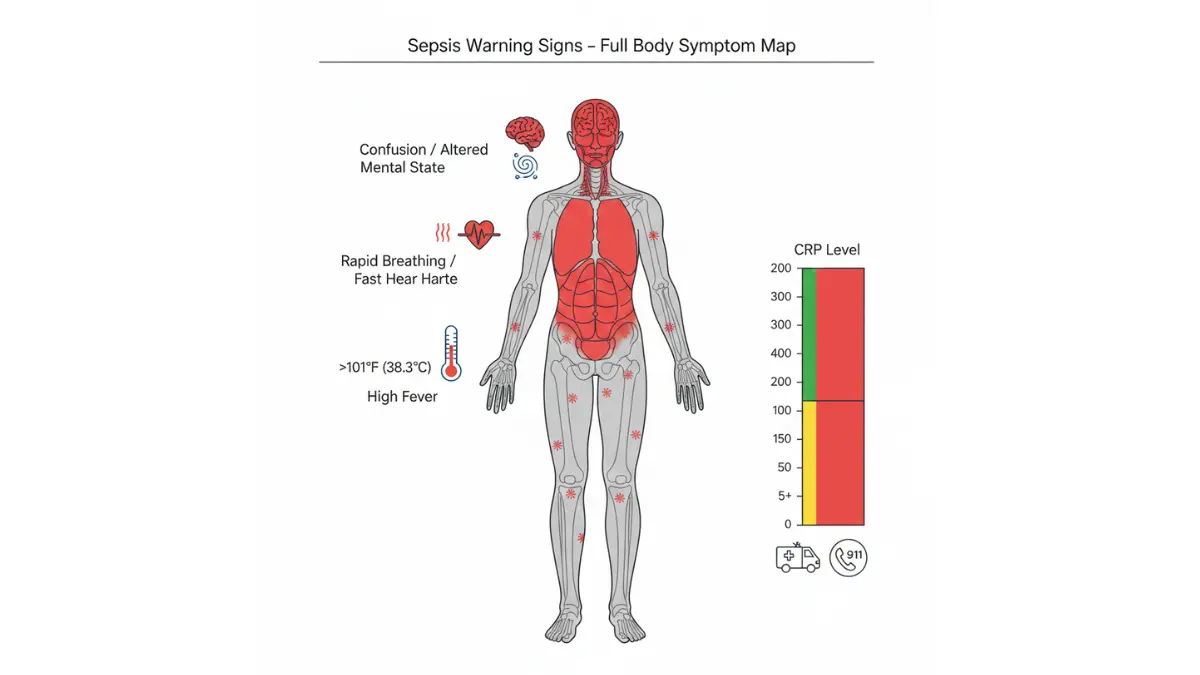
Emergency Room Zone: CRP Above 10.0 mg/L
Jennifer Rodriguez felt tired but functional when her CRP registered 42 mg/L. Within 18 hours, she developed 103°F fever, confusion, and rapid breathing—classic sepsis progression. Emergency treatment saved her life because she recognized the warning signs.
CRP above 10 mg/L breakdown:
- 10-50 mg/L: Significant inflammation, often bacterial infection
- 50-100 mg/L: 90% probability of acute bacterial infection
- Above 100 mg/L: Severe infection, sepsis, or major trauma
Call 911 or go to ER immediately if CRP 50+ mg/L WITH:
- Temperature above 101°F or below 96°F
- Confusion or altered mental status
- Rapid breathing (over 20 breaths/minute)
- Heart rate above 100 beats/minute at rest
- Extreme fatigue preventing basic activities
- Severe pain anywhere in body
According to the National Library of Medicine, CRP levels above 50 mg/L are associated with bacterial infections like pneumonia, sepsis, meningitis, and severe kidney infections in approximately 90% of cases. Viral infections rarely push CRP this high.
When CRP 10-50 mg/L requires monitoring vs immediate care:
Schedule same-day doctor visit:
- No fever but persistent symptoms
- CRP rising on repeat tests
- Known chronic condition with new elevation
- Post-surgical patients (days 3-10)
Monitor and retest in 2 weeks:
- First-time elevation without symptoms
- Recent minor infection or injury
- Chronic inflammatory condition with stable symptoms
Understanding hs-CRP vs Standard CRP
High-sensitivity CRP (hs-CRP) measures the same protein but detects much lower levels—down to 0.3 mg/L compared to standard tests that only measure above 3.0 mg/L. Doctors order hs-CRP specifically for cardiovascular risk assessment in otherwise healthy people.
hs-CRP cardiovascular risk categories:
- Low risk: Below 1.0 mg/L
- Moderate risk: 1.0-3.0 mg/L
- High risk: Above 3.0 mg/L
If you have risk factors like high blood pressure, elevated cholesterol, or family history of heart disease, your doctor should order hs-CRP rather than standard CRP testing. The American Heart Association recommends hs-CRP for intermediate-risk patients to guide statin therapy decisions.
Lab variation decoder: Different laboratories report CRP in different units. Some use mg/L (milligrams per liter) while others use mg/dL (milligrams per deciliter). To convert: 1.0 mg/dL equals 10 mg/L. Always check which unit your lab uses before comparing results to reference ranges.
What Causes Elevated CRP – The Complete 2026 Breakdown
Infections: Bacterial vs Viral CRP Patterns
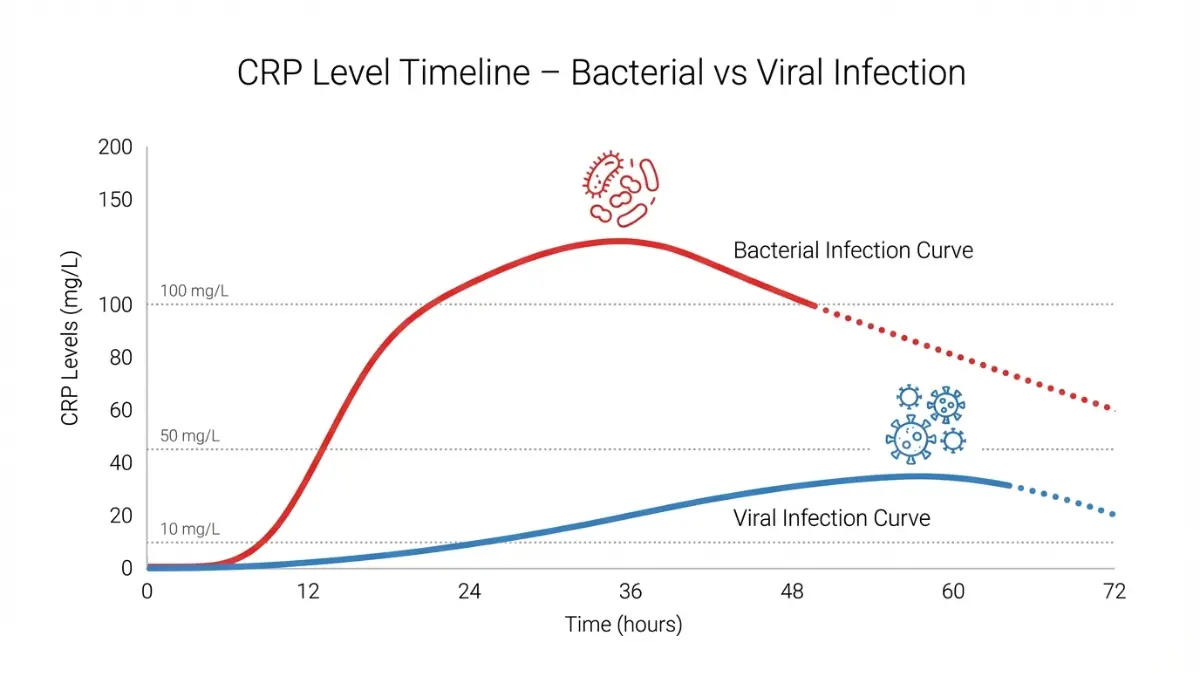
Bacterial infections trigger rapid, dramatic CRP spikes—often reaching 50-200 mg/L within 6-8 hours of symptom onset. Viral infections cause more gradual increases, typically peaking at 10-40 mg/L over 2-3 days.
COVID-19 and long-COVID CRP patterns (2026 data): Acute COVID infection elevates CRP to 20-80 mg/L in moderate cases and above 100 mg/L in severe cases. New research from Stanford Medicine shows that long-COVID patients maintain CRP levels of 3.0-8.0 mg/L for months after initial infection, indicating persistent low-grade inflammation.
Common bacterial infections with CRP correlation:
- Pneumonia: 100-350 mg/L
- Urinary tract infections: 40-100 mg/L
- Meningitis: 150-400 mg/L
- Appendicitis: 50-150 mg/L
- Sepsis: Often exceeds 200 mg/L
Viral infections like influenza, common cold, and most gastroenteritis cases push CRP to only 10-30 mg/L. This difference helps doctors decide whether antibiotics are necessary—bacterial infections require them, viral infections don’t.
Chronic Inflammation Triggers
Autoimmune conditions create persistently elevated C-reactive protein levels that fluctuate with disease activity. Rheumatoid arthritis patients typically maintain CRP between 10-60 mg/L during flares, dropping to 3-10 mg/L during remission periods.
2026 CRP/Albumin ratio breakthrough: Research published in January 2026 demonstrates that the CRP-to-albumin ratio predicts acute pancreatitis severity with 89% accuracy—more reliable than CT scans alone. This ratio divides CRP (in mg/L) by albumin (in g/L), with scores above 0.5 indicating high risk for complications.
Metabolic syndrome components affecting CRP:
- Obesity (BMI over 30): Increases baseline CRP by 40-60%
- Type 2 diabetes: Raises CRP 2-3x normal levels
- High blood pressure: Associated with 30% CRP elevation
- Low HDL cholesterol: Correlates with increased inflammation
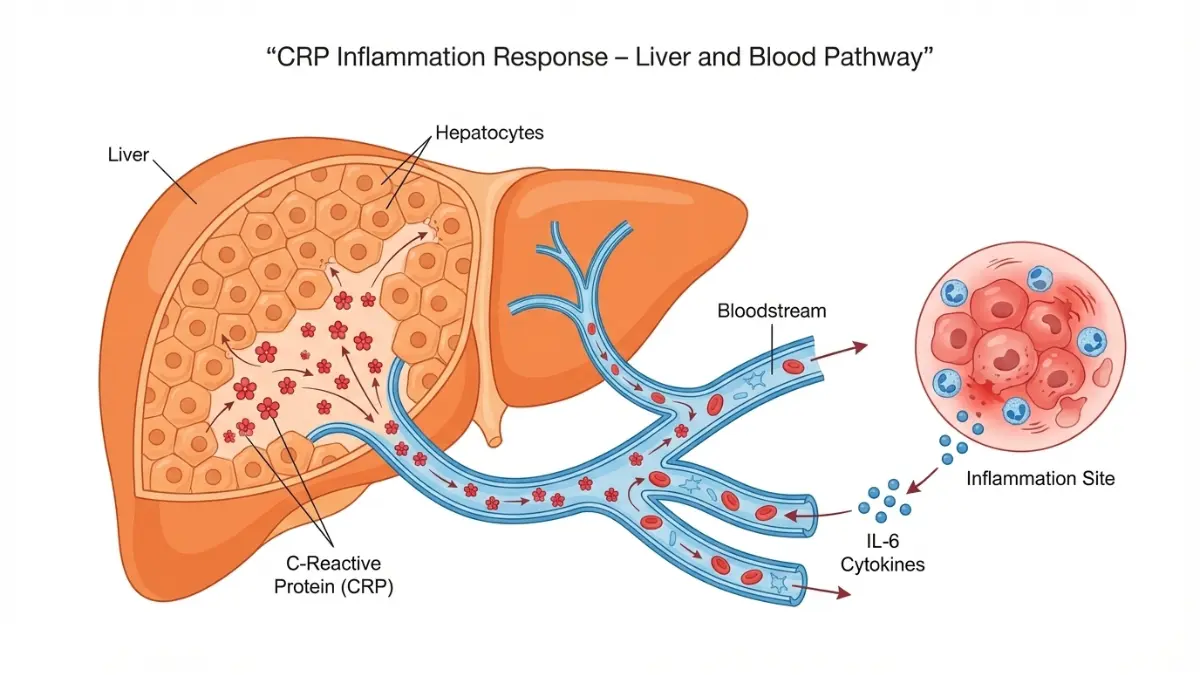
The connection between excess body weight and inflammation is direct—fat tissue secretes inflammatory proteins called cytokines that stimulate the liver to produce more C-reactive protein. Each 5-point increase in BMI correlates with approximately 0.5 mg/L CRP elevation.
Sleep deprivation impact (new 2026 research): Harvard Medical School studies show that sleeping less than 6 hours per night increases CRP by 25-40% within just one week. Using our Sleep Calculator can help optimize your sleep schedule to reduce inflammation naturally.
Hidden CRP Elevators Doctors Often Miss
50+ medications that affect CRP test results:
Medications that LOWER CRP (may mask inflammation):
- NSAIDs (ibuprofen, naproxen): 20-40% reduction
- Statins (atorvastatin, rosuvastatin): 15-50% reduction
- Corticosteroids (prednisone): 40-70% reduction
- Aspirin (regular use): 15-25% reduction
Medications that RAISE CRP:
- Birth control pills: 10-30% elevation
- Hormone replacement therapy: 20-40% elevation
- Certain chemotherapy drugs: Variable increases
If you’re taking any medications that affect CRP, your doctor should account for this when interpreting your results. Stopping NSAIDs 48 hours before testing provides more accurate baseline measurements.
Hormonal factors affecting women’s CRP:
- Menstrual cycle: CRP fluctuates 10-15% throughout cycle
- Pregnancy: Normal CRP rises to 2.0-8.0 mg/L in third trimester
- Menopause: Post-menopausal women average 0.3 mg/L higher
- Birth control: Can elevate baseline by 0.5-1.5 mg/L
Lab variation explained: LabCorp and Quest Diagnostics use different reference ranges and reporting units. LabCorp typically reports in mg/L with reference range of 0-10 mg/L, while Quest often uses mg/dL with range of 0-1.0 mg/dL. Always compare your results to the specific reference range printed on your lab report, not generic ranges from internet sources.
Stress hormones, particularly cortisol, drive chronic CRP elevation through inflammatory pathway activation. Patients with diagnosed anxiety disorders or chronic stress show 30-50% higher average CRP levels compared to psychologically healthy controls, even after controlling for other factors like diet and exercise.
When to Panic vs Monitor – Critical Decision Guide
Immediate Medical Attention Required (ER or Call 911)
CRP 50+ mg/L WITH any of these symptoms demands emergency care:
- Core temperature above 101°F or below 96°F
- Confusion, difficulty staying awake, or altered consciousness
- Respiratory rate exceeding 20 breaths per minute
- Heart rate over 100 beats per minute at rest
- Severe abdominal pain or chest pain
- Inability to keep down fluids for 12+ hours
The Sepsis Alliance reports that sepsis kills more Americans annually than breast cancer, prostate cancer, and AIDS combined. CRP above 100 mg/L combined with fever and confusion has a 70% positive predictive value for sepsis, requiring immediate IV antibiotics.
Post-surgical infection markers (days 3-10 after surgery): CRP normally rises to 50-150 mg/L in the first 48 hours after major surgery, then gradually declines. If your CRP is increasing rather than decreasing after day 3 post-surgery, this signals possible surgical site infection requiring urgent evaluation.
72-hour sepsis development timeline – David Chen’s case: Day 1: CRP 65 mg/L, mild fever, dismissed as flu. Day 2: CRP 145 mg/L, confusion developed, family called 911. Day 3: ICU treatment for sepsis, survived due to rapid antibiotic administration. Delays beyond 12 hours significantly increase mortality risk.
Schedule Doctor Visit Within 48 Hours
CRP 10-50 mg/L without severe symptoms requires prompt but not emergency evaluation:
- Persistent low-grade fever (99-101°F)
- Fatigue affecting daily activities
- Joint pain or swelling
- Unexplained weight loss over 10 pounds
- Night sweats or chills
Your doctor will likely order additional tests including complete blood count, comprehensive metabolic panel, and ESR test to identify inflammation sources. These tests work together to narrow down whether elevation stems from infection, autoimmune disease, or other causes.
What to bring to your appointment:
- List of all medications including supplements
- Recent illness or injury timeline
- Family history of autoimmune diseases
- Previous CRP results for comparison
- Symptom journal noting patterns
Cardiovascular risk factors requiring aggressive intervention: If your CRP is 3.0-10.0 mg/L AND you have high cholesterol, high blood pressure, diabetes, or smoking history, the American College of Cardiology recommends intensive risk factor modification including possible statin therapy regardless of cholesterol levels.
Monitor and Retest in 2 Weeks
CRP 1.0-10.0 mg/L with first-time elevation and no symptoms:
- Retest using same laboratory for consistency
- Avoid NSAIDs for 48 hours before retest
- Fast for 8-12 hours if ordered alongside cholesterol
- Request hs-CRP if cardiovascular risk assessment needed
Two measurements taken 2 weeks apart provide 90% accuracy improvement over single testing, according to the National Heart, Lung, and Blood Institute. This two-test protocol eliminates false elevations from temporary factors like recent colds or minor injuries.
Known chronic conditions with stable CRP levels: If you have rheumatoid arthritis, inflammatory bowel disease, or other diagnosed inflammatory conditions, your doctor establishes your personal baseline CRP. Stable levels matching your baseline don’t require intervention—it’s significant changes (increases of 5+ mg/L) that trigger concern.
2026 International Expert Consensus Guidelines
The European Society of Cardiology updated CRP guidelines in January 2026 to recommend hs-CRP screening for all adults over 40 with one or more cardiovascular risk factors. This expands previous recommendations that limited screening to intermediate-risk patients only.
World Health Organization global inflammation thresholds (2026 update):
- Population health screening: CRP above 3.0 mg/L
- Individual cardiovascular risk: hs-CRP above 2.0 mg/L
- Infectious disease triage: CRP above 10.0 mg/L
- Sepsis diagnosis: CRP above 50.0 mg/L with clinical criteria
These international standards help doctors worldwide interpret C-reactive protein test results consistently, though regional variations exist in testing protocols and reference ranges. If you’re managing chronic inflammation alongside other metabolic issues, tracking your metabolic syndrome markers provides comprehensive health insight.
How to Lower Your CRP – Evidence-Based Action Plan
Dietary Changes That Work
The Mediterranean diet reduces CRP by 37% in just 12 weeks according to Harvard T.H. Chan School of Public Health research published in 2026. This eating pattern emphasizes olive oil, fish, vegetables, whole grains, and nuts while limiting red meat and processed foods.
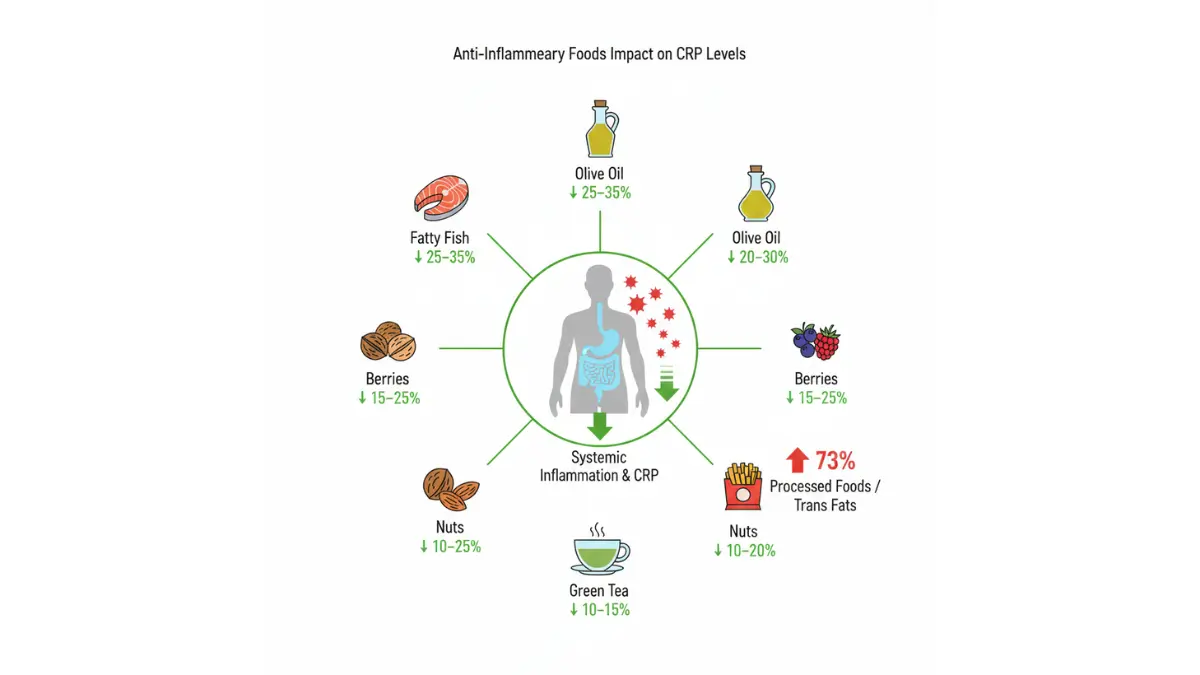
Anti-inflammatory foods ranked by CRP reduction effectiveness:
- Fatty fish (salmon, sardines): 25-35% reduction when eaten 3x/week
- Extra virgin olive oil: 20-30% reduction with 2-3 tablespoons daily
- Berries and dark leafy greens: 15-25% reduction
- Nuts (walnuts, almonds): 10-20% reduction with 1 ounce daily
- Green tea: 10-15% reduction with 3+ cups daily
Trans fats increase CRP by 73% according to studies examining fast food and processed snack consumption. Eliminating partially hydrogenated oils, fried foods, and commercial baked goods provides immediate inflammation benefits.
7-day anti-inflammatory meal framework:
- Breakfast: Greek yogurt with berries, walnuts, ground flaxseed
- Lunch: Salmon salad with olive oil dressing, quinoa
- Dinner: Grilled chicken, roasted vegetables, sweet potato
- Snacks: Apple with almond butter, carrots with hummus
If you’re combining dietary changes with weight loss goals, our Macro Calculator helps determine optimal protein, fat, and carbohydrate ratios for reducing inflammation while losing weight sustainably.
Exercise Impact on Inflammation
Exercising 195+ minutes per week (about 30 minutes daily) produces significant CRP reductions—typically 25-35% within 12 weeks even without weight loss. Combining cardio and strength training provides superior results compared to either alone.
VO2max improvement correlation: Each 1 mL/kg/min increase in cardiovascular fitness corresponds to approximately 0.3 mg/L CRP reduction. Previously sedentary individuals who increase fitness by just 5-15% see nearly 30% CRP drops within one year.
Strength training 2-3x weekly benefits: Resistance exercise triggers temporary CRP spikes immediately after workouts (normal response), but chronic levels decrease 20-25% with consistent training. Building muscle mass improves insulin sensitivity, which indirectly lowers inflammatory markers.
Exercise prescription by CRP level:
- CRP below 3.0 mg/L: All exercise types safe, aim for 150+ min/week
- CRP 3.0-10.0 mg/L: Moderate intensity preferred, avoid overtraining
- CRP above 10.0 mg/L: Consult doctor before starting new exercise program
Using our Heart Rate Zone Calculator ensures you’re exercising at appropriate intensity levels for inflammation reduction without triggering excessive stress responses that could temporarily raise CRP.
Medical Interventions for High CRP
Statin therapy reduces CRP by 15-50% independent of cholesterol-lowering effects. The JUPITER trial demonstrated that rosuvastatin decreased CRP by 37% on average, reducing cardiovascular events even in patients with normal cholesterol but elevated CRP (above 2.0 mg/L).
When doctors recommend statins for CRP reduction:
- hs-CRP above 2.0 mg/L with cardiovascular risk factors
- LDL cholesterol above 130 mg/dL plus CRP above 3.0 mg/L
- Previous heart attack or stroke with any CRP elevation
- Diabetic patients with CRP above 1.0 mg/L
Anti-inflammatory medication protocols vary by underlying condition. Rheumatoid arthritis patients may receive DMARDs (disease-modifying antirheumatic drugs) that reduce CRP by 60-80% when effective. Inflammatory bowel disease often requires biologics targeting specific inflammatory pathways.
Treatment monitoring timeline:
- Week 2: Initial CRP retest to establish trending direction
- Week 6: Expect 20-30% reduction with medication adherence
- Week 12: Full treatment effect usually achieved
- Month 6: Maintenance level established, adjust if needed
Lifestyle Factors Often Overlooked
Sleep optimization to 7-9 hours nightly reduces CRP by 15-25% within one month. Yale School of Medicine research shows that each additional hour of sleep (up to 8 hours total) correlates with 0.4 mg/L CRP reduction.
Stress reduction techniques with proven CRP impact:
- Mindfulness meditation 20 min daily: 15-20% reduction
- Yoga 3x weekly: 10-15% reduction
- Regular social connection: 10-12% reduction
- Nature exposure 120+ min weekly: 8-12% reduction
Weight management produces proportional CRP reductions—approximately 0.13 mg/L decrease for each pound lost. A 20-pound weight loss typically reduces CRP by 2.5-3.0 mg/L, which can shift someone from high-risk to moderate-risk cardiovascular category.
Smoking cessation impact: CRP drops 20% within 2 weeks of quitting smoking, 40% within 3 months, and normalizes to non-smoker levels within 1-2 years. Continuing to smoke while trying other CRP reduction methods severely limits potential improvements. For comprehensive weight management support, our Weight Loss Calculator provides personalized timelines and calorie targets.
Understanding Lab Reports and Your Next Steps
Lab Variation and Unit Conversion
Different laboratories use varying reference ranges and reporting units for CRP test results, creating confusion when comparing results from different facilities. LabCorp, Quest Diagnostics, and hospital laboratories each maintain their own standardized ranges.
Converting between common CRP units:
- 1.0 mg/dL = 10 mg/L
- 0.5 mg/dL = 5 mg/L
- 0.1 mg/dL = 1 mg/L
If your previous CRP was tested at LabCorp (reporting in mg/L) and your new test came from Quest (reporting in mg/dL), multiply the mg/dL value by 10 to compare accurately. A result of 0.8 mg/dL equals 8.0 mg/L—very different interpretations if you don’t convert properly.
Standard CRP vs hs-CRP testing differences: Standard CRP accurately measures levels from 3-300 mg/L, designed for detecting acute inflammation and infection. High-sensitivity CRP measures 0.3-10 mg/L precisely, optimized for cardiovascular risk assessment in apparently healthy individuals.
When to request hs-CRP instead of standard CRP:
- No current symptoms but assessing heart disease risk
- Family history of early cardiovascular disease
- Borderline cholesterol levels requiring treatment decision
- Monitoring statin therapy effectiveness
The College of American Pathologists recommends using the same laboratory for serial CRP testing whenever possible to eliminate variability from different testing methodologies and reference ranges.
Critical Questions to Ask Your Doctor
10 essential questions for your CRP follow-up appointment:
- Which CRP test did you order—standard or high-sensitivity?
- What could be causing my specific CRP elevation?
- Which additional tests should we run to identify the source?
- How urgently do I need follow-up testing?
- Should I stop taking NSAIDs or other medications before retesting?
- What’s my cardiovascular risk based on this CRP level?
- Do I need specialist referral (rheumatologist, cardiologist)?
- What lifestyle changes will have the biggest impact on my CRP?
- When should we retest to monitor progress?
- At what CRP level would you recommend medication intervention?
How to request proper follow-up testing: If your doctor dismisses moderately elevated CRP (3.0-10.0 mg/L) without ordering additional workup, you have the right to request comprehensive inflammatory marker testing including ESR, rheumatoid factor, and ANA (antinuclear antibody) panels. Similar to how patients track TSH levels for thyroid function, monitoring CRP trends over time provides more valuable information than single measurements.
When to demand specialist referral: CRP persistently above 10.0 mg/L without clear infection source warrants rheumatology evaluation for autoimmune disease. CRP above 3.0 mg/L with multiple cardiovascular risk factors justifies cardiology consultation for aggressive risk modification.
Insurance Coverage and Cost Considerations
Medicare covers CRP testing when medically necessary—typically once annually for cardiovascular risk assessment and as needed for infection or inflammation monitoring. Medicare Part B covers 80% of approved testing costs after deductible, with patients responsible for remaining 20%.
Private insurance typical coverage patterns:
- Standard CRP for infection diagnosis: Usually covered 100%
- hs-CRP for cardiovascular screening: Often requires pre-authorization
- Repeat testing within 30 days: May require medical justification
- Out-of-network laboratory: Higher out-of-pocket costs
Out-of-pocket cost ranges without insurance (2026 prices):
- Standard CRP test: $15-$45 at commercial labs
- High-sensitivity CRP: $25-$75 at commercial labs
- Hospital-based testing: $75-$200 (higher facility fees)
- Point-of-care rapid testing: $30-$60 at urgent care
How to appeal insurance denials: If your insurance denies CRP coverage claiming it’s not medically necessary, ask your doctor to submit clinical documentation showing your cardiovascular risk factors or symptoms requiring inflammation assessment. Include family history, previous test results, and current medications in the appeal.
For patients managing multiple health markers, tracking inflammation alongside other metrics provides comprehensive health insight—similar to monitoring various parameters through our Genetic Risk Assessment Tool for hereditary conditions.
Frequently Asked Questions
1. What CRP level is considered dangerous?
CRP above 10 mg/L indicates significant inflammation requiring medical evaluation. Levels exceeding 50 mg/L are critical and often signal serious bacterial infection needing immediate attention.
2. Can stress alone raise CRP levels?
Yes, chronic psychological stress increases CRP by 25-40% through cortisol-driven inflammatory pathways. Acute stress causes smaller, temporary elevations.
3. How quickly does CRP drop after treatment?
CRP has a 19-hour half-life, dropping rapidly once inflammation resolves. Bacterial infections show 50% reduction within 24-48 hours of effective antibiotic treatment.
4. Should I fast before a CRP test?
Standard CRP requires no fasting. High-sensitivity CRP may require 8-12 hour fast if ordered alongside lipid panel—ask your doctor’s office when scheduling.
5. Does ibuprofen affect CRP results?
Yes, NSAIDs lower CRP by 20-40%, potentially masking dangerous inflammation. Stop ibuprofen 48 hours before testing for accurate baseline measurement.
6. Is CRP 3.5 mg/L concerning?
This indicates moderate cardiovascular risk and mild systemic inflammation. Lifestyle modifications and follow-up testing in 2-4 weeks are recommended.
7. Can elevated CRP detect cancer?
CRP elevates in many cancers but isn’t specific enough for screening. Persistently high CRP without clear infection source warrants comprehensive cancer screening.
8. How often should I retest CRP?
Initial elevation: retest in 2 weeks. Normal baseline: annually if cardiovascular risk factors present. Chronic elevation: every 3-6 months to monitor treatment effectiveness.
9. What’s the normal CRP range for women?
Women average 15-20% higher than men—typically 0.3-1.2 mg/L versus 0.2-0.9 mg/L for men. Pregnancy, birth control, and hormone therapy increase these baselines further.
10. Does exercise temporarily raise CRP?
Intense exercise causes acute CRP spikes lasting 24-48 hours. Chronic regular exercise lowers baseline CRP by 25-35% despite these temporary increases.
11. When does high CRP require emergency care?
CRP above 50 mg/L combined with fever above 101°F, confusion, rapid breathing, or severe pain requires immediate emergency room evaluation for possible sepsis.
Medical Disclaimer
This article provides educational information about C-reactive protein test results and should not replace professional medical advice, diagnosis, or treatment. CRP levels require interpretation within your complete clinical context including symptoms, medical history, and additional test results. Always consult qualified healthcare providers for personalized medical guidance regarding your specific CRP results and appropriate next steps. Emergency situations require immediate medical attention—call 911 or go to your nearest emergency room if experiencing severe symptoms alongside elevated CRP levels.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.