On This Page – Quick Medical Summary
In 2021, James — a 58-year-old retired firefighter from New York — walked into Memorial Sloan Kettering Cancer Center with tremors so severe he could no longer hold a coffee cup. He wasn’t there for conventional surgery. He was patient #7 in a landmark clinical trial where dopamine-producing neurons grown from human embryonic stem cells would be implanted directly into his brain. By April 2025, his results were published in Nature*. His tremors had visibly reduced. His grafted cells were alive, producing dopamine, and showing no signs of tumor formation at 18 months.*
That trial didn’t just make headlines. It changed what medicine believes is possible.
⚡ Quick Answer (Featured Snippet Block): Embryonic stem cells (ESCs) are pluripotent master cells extracted from 3–5 day old human embryos at the blastocyst stage. They can develop into any of the body’s 200+ cell types. This makes them uniquely powerful for regenerative medicine, disease modeling, and experimental treatments for conditions like Parkinson’s disease, blindness, ALS, and spinal cord injury. As of 2026, no embryonic stem cell therapy is commercially approved in the US — but multiple Phase 3 trials are underway.
What Are Embryonic Stem Cells? The Science in Plain English
What Makes These Cells Different From Every Other Cell in Your Body
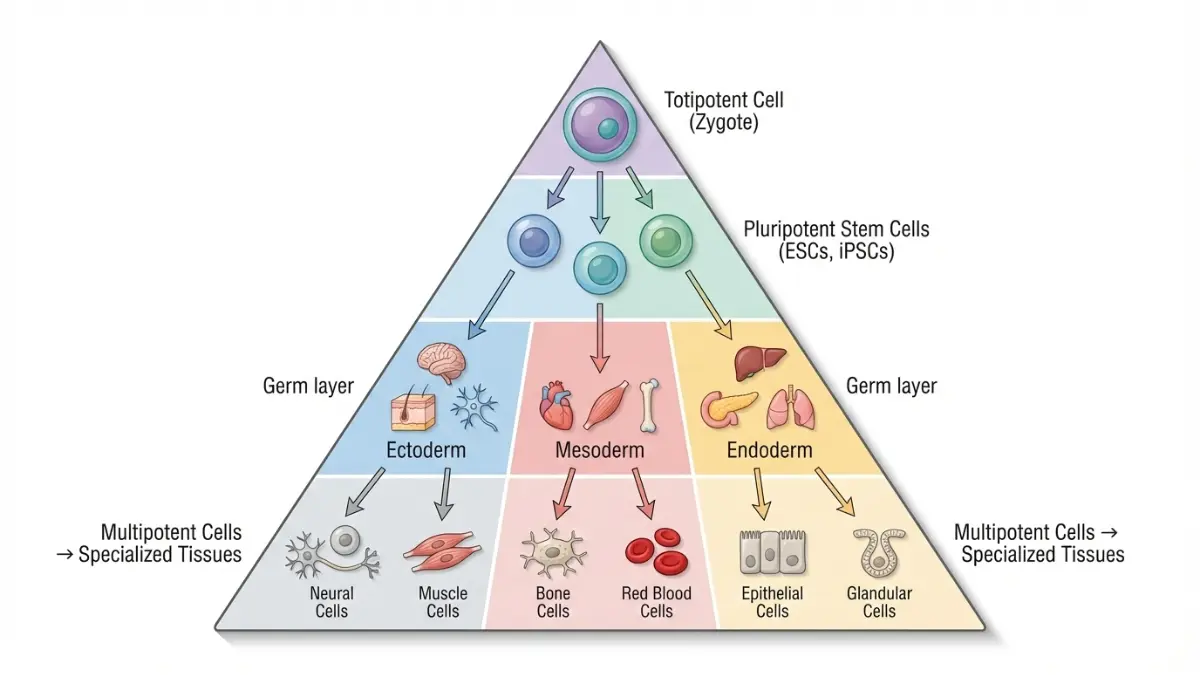
Every cell in your body has a job — liver cells filter toxins, heart cells contract, neurons fire electrical signals. Embryonic stem cells are different. They haven’t chosen a job yet.
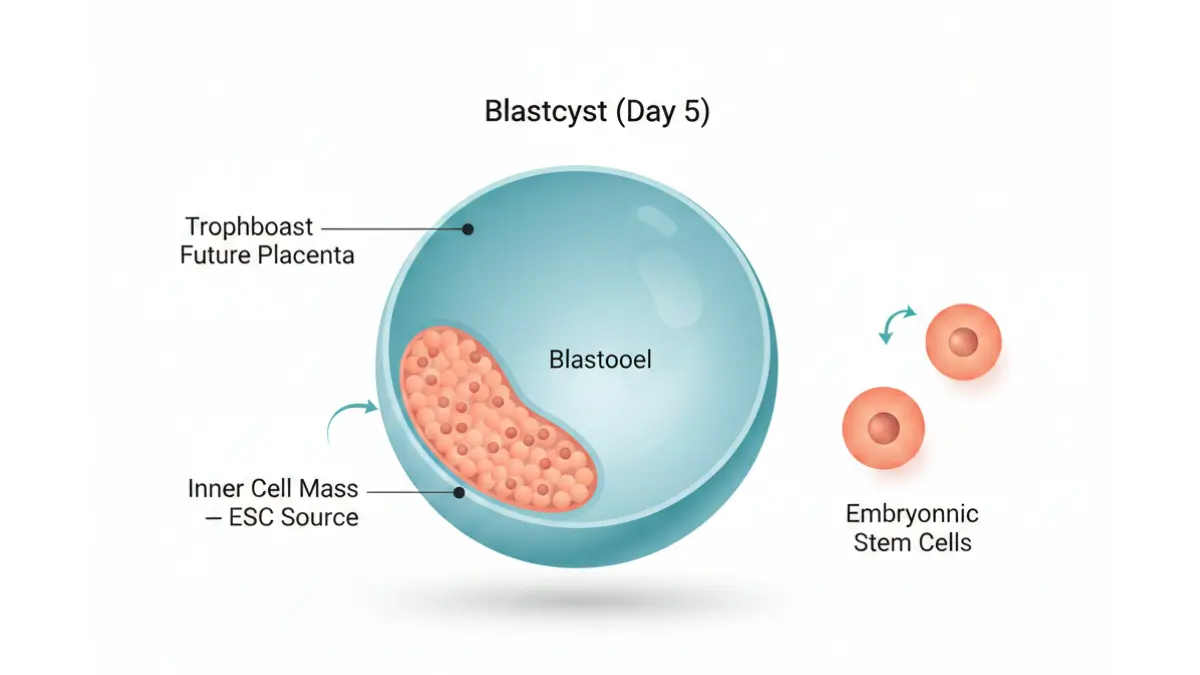
Derived from the inner cell mass of a human blastocyst — an embryo just 3 to 5 days after fertilization — these cells are pluripotent. That means they retain the biological potential to become any of the more than 200 specialized cell types in the human body, from brain neurons to insulin-producing pancreatic beta cells to retinal tissue.
According to the NIH Stem Cell Information resource, human embryonic stem cells were successfully grown in a laboratory for the first time in 1998 by James Thomson at the University of Wisconsin. That single breakthrough launched what is now a $2.44 billion global research industry.
Two Properties That Make ESCs Medically Revolutionary
Human embryonic stem cells have two unique properties that no other cell type naturally possesses:
- Pluripotency — the ability to differentiate into virtually any cell in the body, including those the adult body cannot naturally regenerate after disease or injury
- Indefinite self-renewal — under the right conditions, ESCs can divide and produce identical copies of themselves indefinitely in laboratory culture, providing an essentially unlimited supply for research
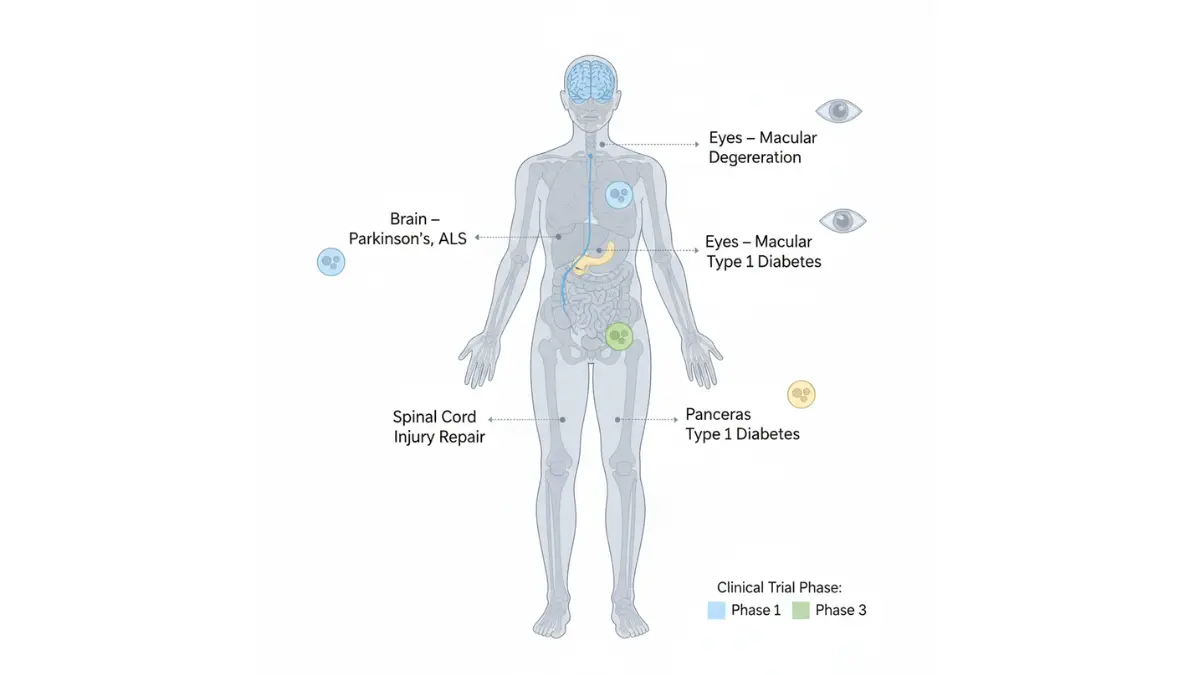
These two properties are precisely why scientists have spent decades trying to harness them for treating diseases where the body’s own cells are irreversibly lost — Parkinson’s, macular degeneration, ALS, spinal cord injury, and Type 1 diabetes.
Key Terminology: Quick Reference Table
| Term | Plain English Meaning |
|---|---|
| Blastocyst | A 3–5 day old embryo, containing ~150 cells, from which ESCs are extracted |
| Pluripotent | Can become any cell type in the body (but not a full organism) |
| Totipotent | Can become any structure, including placenta (only the fertilized egg/zygote) |
| Multipotent | Can become a limited range of related cell types (e.g., blood stem cells) |
| hESCs | Human embryonic stem cells — the specific type studied in clinical trials |
| Cell line | A stable, reproducible population of ESCs that can be grown and distributed |
How Are They Collected?
The collection process is a common source of public confusion:
- Embryos used for ESC research are NOT taken from aborted fetuses. This is a widespread misconception.
- They come from surplus IVF embryos — embryos created for fertility treatments that were never implanted and would otherwise be discarded
- Donors provide informed consent before any embryo is used
- The extraction process does destroy the embryo, which is the core of the ethical debate (covered fully in Section 4)
If you’re tracking a health condition that may one day be addressed by stem cell therapy — such as a genetic disorder — our Genetic Risk Assessment Tool can help you understand your inherited disease risk profile before your next specialist consultation.
Embryonic Stem Cells vs. Adult Stem Cells vs. iPSCs — The Full Comparison
Why This Comparison Matters in 2026
Not all stem cells are the same — and the differences matter enormously for patients, researchers, and anyone following the 2026 regulatory landscape. Here is the definitive comparison that Mayo Clinic, Healthline, and WebMD have all failed to provide in a clear, actionable format.
Master Comparison Table
| Feature | Embryonic Stem Cells (ESCs) | Adult Stem Cells | Induced Pluripotent Stem Cells (iPSCs) |
|---|---|---|---|
| Source | IVF surplus embryo blastocyst | Bone marrow, fat, blood, tissue | Reprogrammed adult skin/blood cells |
| Differentiation | Any cell type (pluripotent) | Limited range (multipotent) | Any cell type (pluripotent) |
| Ethical concerns | High — embryo is destroyed | None | None |
| Immune rejection risk | Moderate — requires immunosuppression | Low (autologous use) | Low (patient’s own cells possible) |
| Current clinical stage | Phase 1–3 trials (Parkinson’s, eyes) | FDA-approved for blood/bone marrow | Phase 1–2 trials |
| 2026 US regulatory status | NIH review pause on new lines | Routine clinical use | Actively expanding |
| Tumor formation risk | Present if undifferentiated cells used | Minimal | Present (managed in trials) |
| Off-the-shelf potential | High — universal donor possible | Low | Growing with HLA-matched banks |
Why Scientists Still Need ESCs — Even With iPSCs Available
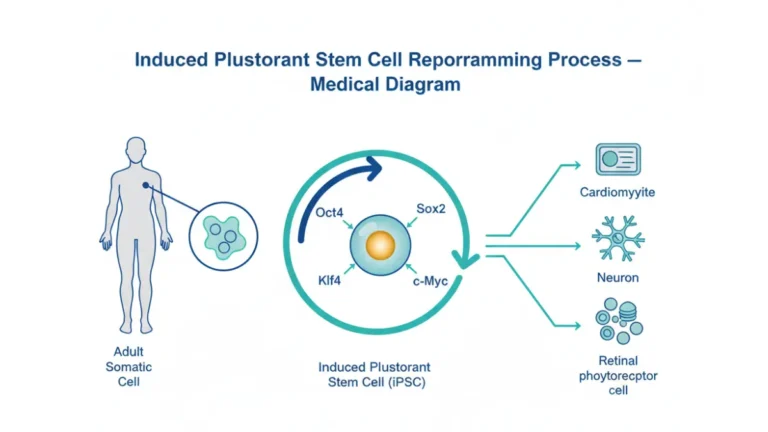
Induced pluripotent stem cells (iPSCs), first developed by Dr. Shinya Yamanaka in 2006, can be created from a patient’s own skin or blood cells — eliminating both the ethical concerns and immune rejection risks of ESCs. So why do researchers still use embryonic stem cells?
Three reasons iPSCs cannot yet fully replace ESCs:
- Benchmark validation — ESCs remain the gold standard against which all iPSC behavior is measured. Without ESC data, scientists cannot confirm iPSC safety
- Epigenetic differences — iPSCs can carry “memory” of their original cell type, affecting differentiation behavior in ways that ESCs do not
- Manufacturing consistency — ESC lines have decades of documented stability; many iPSC lines are still being characterized for reliability at scale
The National Institute of Neurological Disorders and Stroke (NINDS) actively funds both ESC and iPSC research precisely because both remain scientifically necessary in 2026.
2026 Update — What Embryonic Stem Cell Research Is Actually Treating Right Now
The Real Clinical Breakthroughs Competitors Are Not Telling You About
In 2025 alone, three landmark results involving embryonic stem cell therapy were published in peer-reviewed journals including Nature and Cell. Here is what the science actually showed — with zero hype and zero omission.
🧠 Parkinson’s Disease — The Most Significant Breakthrough of 2025
In April 2025, two independent clinical trials published simultaneously in Nature transformed the outlook for Parkinson’s disease treatment.
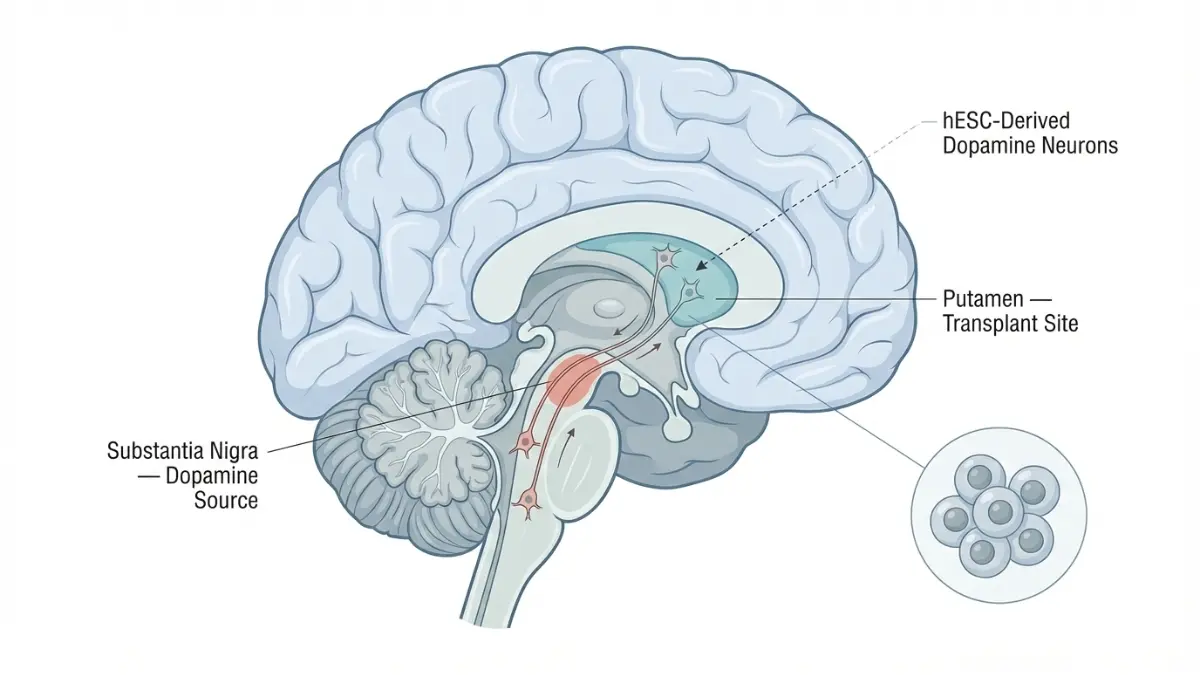
Trial 1 — Memorial Sloan Kettering Cancer Center (USA):
- 12 patients with moderate-to-advanced Parkinson’s received bilateral brain implants of bemdaneprocel (BRT-DA01) — dopamine neuron progenitor cells derived directly from human embryonic stem cells
- Developed by BlueRock Therapeutics over 25 years of ESC research led by Dr. Viviane Tabar and Dr. Lorenz Studer
- Results at 18 months: Zero serious adverse events related to cell therapy; transplanted cells survived, engrafted, and produced dopamine; some patients experienced visible reductions in tremors
- The FDA has since approved proceeding directly to a Phase 3 trial, expected to enroll hundreds of patients in 2025–2026
- Published: Phase I Trial of hES Cell-Derived Dopaminergic Neurons for Parkinson’s Disease — Nature, April 2025
Trial 2 — Multiple US/Canada Centers (12 patients, Chinese research group):
- Separate Phase 1/2a trial using hESC-derived A9-dopaminergic progenitor cells (A9-DPCs)
- At 12 months: MDS-UPDRS Part III motor scores improved by an average of 23 points in the high-dose group
- No dose-limiting toxicities observed at either low or high dose
What This Means For You: These are Phase 1 results — not a cure yet. But the safety profile is now confirmed across two independent trials. A Phase 3 efficacy trial for bemdaneprocel is actively recruiting. If you or a family member has Parkinson’s, ask your neurologist about trial eligibility at ClinicalTrials.gov.
For patients currently managing neurological symptoms, our Symptom Checker can help you document and organize symptom patterns before your next specialist appointment.
👁️ Vision Loss and Macular Degeneration
Age-related macular degeneration (AMD) is one of the leading causes of permanent vision loss in Americans over 60. Embryonic stem cell research has now produced some of its most encouraging results in this disease area.
Key clinical findings:
- A UCL/London Project Phase 1 trial transplanting hESC-derived retinal pigment epithelium (RPE) patches into two patients with severe AMD showed visual acuity gains of 29 and 21 letters respectively over 12 months — a result published in Nature Biotechnology
- A November 2025 trial from Michigan Medicine published in Cell Stem Cell showed 90%+ success rate at restoring corneal function using retinal stem cell transplants, with patients gaining measurable sight improvements
- ASP7317, an hESC-derived RPE product for dry AMD/geographic atrophy, was in Phase Ib dose-ranging trials as of early 2026
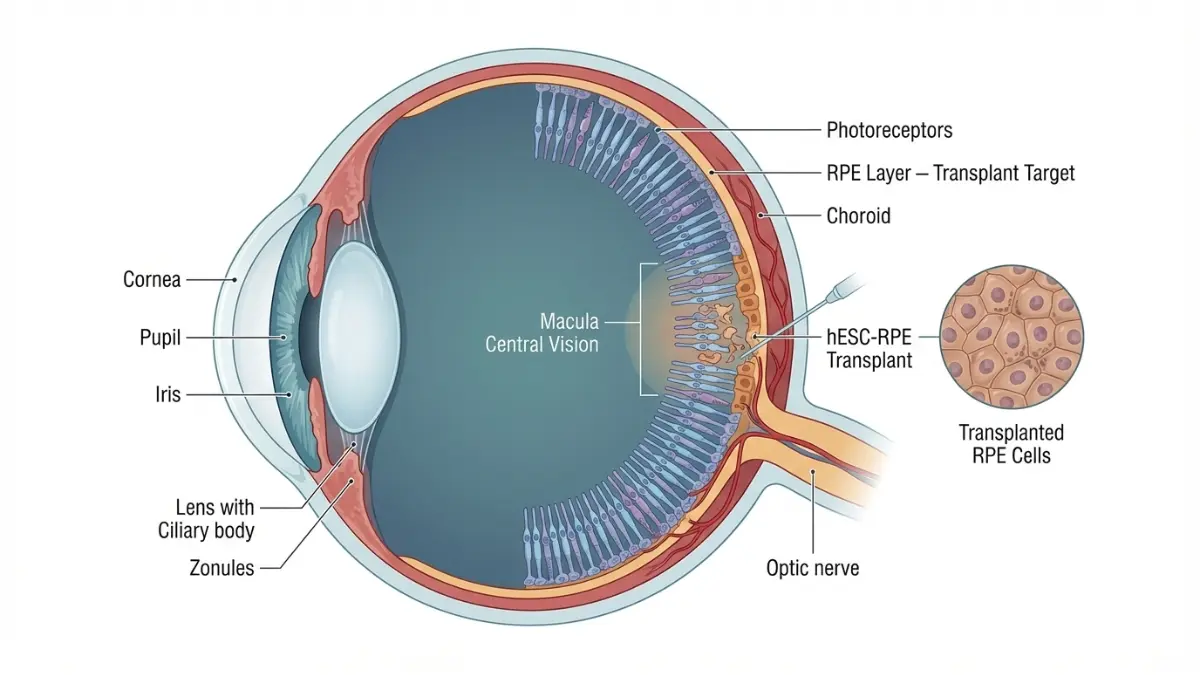
Who this matters for most: Approximately 20 million Americans have some form of AMD. Current treatments can slow progression but cannot restore lost vision. ESC-derived RPE therapy is the first credible biological path to actual vision restoration.
If you’re experiencing early vision changes, our Eye Exam tool provides a preliminary screening assessment you can share with your ophthalmologist.
🦴 Spinal Cord Injury
The world’s first FDA-cleared Phase 1 clinical trial using an hESC-derived product was for spinal cord injury, conducted by Geron Corporation beginning in 2010.
A 2024 ten-year follow-up study on participants who received LCTOPC1 (hESC-derived oligodendrocyte progenitors) showed:
- Zero tumor formations across all participants over a decade — directly refuting early safety concerns
- 80% of patients showed MRI evidence of tissue matrix formation at the injury site
In November 2025, Nature Biotechnology published results from a rhesus monkey spinal cord trial showing that stem cell transplantation improved hand function — a key milestone toward human cervical injury trials.
🧬 ALS (Amyotrophic Lateral Sclerosis)
AstroRx®, an hESC-derived astrocyte therapy developed by Kadimastem, completed a Phase 1/2a trial in ALS patients:
- Single intrathecal injection administered to two cohorts (low-dose and high-dose, 5 patients each)
- Results: Clinically significant stabilization lasting 3 months post-treatment — the longest duration of effect shown in any ALS trial at that stage
Evidence Strength Summary Table
| Disease Area | Trial Phase | Key Result | Evidence Confidence |
|---|---|---|---|
| Parkinson’s disease | Phase 1 → Phase 3 | Tremor reduction, cell survival at 18 months | ⭐⭐⭐⭐ Strong |
| Macular degeneration | Phase 1–Phase Ib | 21–29 letter vision gain; 90% corneal success | ⭐⭐⭐ Promising |
| Spinal cord injury | Phase 1 (10-yr follow-up) | 80% tissue matrix formation; zero tumors | ⭐⭐⭐⭐ Strong safety |
| ALS | Phase 1/2a | 3-month stabilization | ⭐⭐ Early |
| Type 1 Diabetes | Pre-clinical → Phase 1 | Beta cell production confirmed in animal models | ⭐⭐ Early |
The Ethics Debate and the January 2026 US Policy Shift
Why Embryonic Stem Cell Research Remains Controversial
The core ethical tension is straightforward: extracting embryonic stem cells destroys the human embryo. For those who believe human life begins at fertilization, this represents the destruction of a human being. For supporters of the research, a 3–5 day blastocyst — a microscopic cluster of approximately 150 cells, smaller than the period at the end of this sentence — does not yet constitute a person, and its use may save millions of lives.
The core arguments on both sides:
Those who oppose embryonic stem cell research argue:
- A fertilized embryo has the full genetic identity of a human being
- Using embryos for research — even with donor consent — treats human life as a tool
- iPSC technology has largely made ESC research unnecessary
Those who support it argue:
- Surplus IVF embryos used in research would otherwise be discarded
- Donor couples provide explicit, informed consent
- ESCs remain scientifically indispensable as the biological gold standard
- The potential to cure devastating diseases for millions justifies research on cells that will not otherwise develop into a person
🚨 BREAKING — NIH January 23, 2026 Policy Announcement
This is breaking news that no major health website — not Mayo Clinic, Healthline, or WebMD — has yet incorporated into their content.
On January 23, 2026, the National Institutes of Health announced a formal pause on the review and approval of new human embryonic stem cell lines for the NIH Registry, citing technological advances in iPSC and adult stem cell alternatives.
Key facts from the announcement:
- 503 existing approved hESC lines remain eligible for NIH-funded research and are unaffected
- A public comment period is open through April 24, 2026, seeking input on whether iPSC and adult stem cell technologies can now replace ESC use
- HHS Secretary Robert F. Kennedy Jr. stated: “As new technologies prove more effective, we have a responsibility to move beyond practices becoming obsolete”
- NIH Director Jay Bhattacharya, M.D., Ph.D. confirmed that ongoing research and trials are not disrupted
What this does NOT mean:
- It does not ban embryonic stem cell research
- It does not affect ongoing clinical trials like the Parkinson’s Phase 3 study
- It does not affect the 503 approved cell lines already in use
Global Legal Landscape — Quick Summary
| Country | ESC Research Status (2026) |
|---|---|
| United States | Permitted on 503 NIH-approved lines; new derivation prohibited with federal funds |
| United Kingdom | Permitted under Human Fertilisation and Embryology Authority (HFEA) oversight |
| Japan | Permitted; iPSC research dominant; Kyoto University leading global trials |
| European Union | Varies by country; Germany prohibits new derivation; UK, Sweden, Netherlands permit |
| China | Active — multiple Phase 1/2 trials underway with fewer regulatory restrictions |
What This Means For You: The 2026 NIH policy shift signals a gradual transition toward iPSC-dominant research. However, existing embryonic stem cell clinical trials — including the Parkinson’s Phase 3 — are proceeding without interruption. The science is advancing regardless of the political environment.
Risks, Limitations, and the Fake Clinic Warning Every Patient Needs to Read
What the Evidence Actually Shows About Safety
Early fears about embryonic stem cell therapy centered on two major risks: tumor formation and immune rejection. After more than a decade of clinical trials, here is what the data shows.
Tumor formation (teratoma risk):
- The original concern was that undifferentiated ESCs injected into the body could form benign tumors called teratomas
- Geron’s 10-year spinal cord follow-up (2024): Zero tumor formations across all participants
- BlueRock’s Parkinson’s trial (2025): Zero tumor formations or graft overgrowth at 18 months
- Modern manufacturing protocols now achieve >95% purity of differentiated cells before transplantation, dramatically reducing this risk
Immune rejection:
- ESC-derived cells are allogeneic (from a donor), meaning the recipient’s immune system may attack them
- Current trials address this with a course of immunosuppressive medication, typically for 12 months
- Research into HLA-matched universal donor cell lines is actively ongoing to eventually eliminate this requirement
Known risks that remain real in 2026:
- Surgical delivery is complex and invasive (brain, eye, or spine procedures)
- Long-term data beyond 18–24 months is still limited
- Not all patients respond equally — baseline disease severity appears to affect outcomes
- iPSCs may eventually offer a safer, rejection-free alternative for most applications
Pros and Cons — Clear Summary Table
| ✅ Documented Benefits | ⚠️ Real Limitations |
|---|---|
| Can become any cell type in the body | Embryo destruction raises ethical objections |
| Unlimited self-renewal for research supply | Immune rejection requires immunosuppression |
| Phase 3 Parkinson’s trial FDA-approved | Not commercially available in 2026 |
| Confirmed safety in 10-year spinal cord data | Long-term data still accumulating |
| Vision restoration results in AMD trials | Surgical delivery is complex and invasive |
| No tumor formation in modern purified trials | Tumor risk if cell purity standards aren’t met |
⚠️ Critical Warning: The Fake Clinic Problem
This is the section that could save your life or save you from financial devastation.
As of February 2026, NO private clinic anywhere in the world has FDA approval to offer embryonic stem cell therapy outside of a registered clinical trial.
Hundreds of unregulated clinics — primarily in Mexico, Panama, China, Thailand, and parts of Eastern Europe — market “stem cell treatments” to desperate patients, often charging $10,000 to $50,000 per treatment. These treatments are:
- Not FDA-approved or clinically validated
- Often using uncharacterized cell sources with no purity standards
- Associated with documented cases of severe vision loss, tumor formation, and death
- Frequently marketed with misleading testimonials and cherry-picked “patient stories”
Before paying for any stem cell treatment, verify it at ClinicalTrials.gov — the official US database of all legitimate, registered clinical trials. Legitimate trials do not charge patients.
For patients managing diabetes while monitoring emerging treatments like beta cell therapy, our Blood Sugar Converter helps track glucose metrics accurately between specialist visits.
The Future of Embryonic Stem Cells — What’s Coming by 2030
Where the Science Is Heading
As of early 2026, the pipeline for embryonic stem cell-based therapies is the strongest it has ever been. Here is what credible research projections and active trial data suggest is coming.
Active Pipeline by Disease (2026–2030 Projection)
| Disease | Current Stage | Projected Timeline |
|---|---|---|
| Parkinson’s disease | Phase 3 trial (bemdaneprocel) | Potential FDA approval 2027–2028 |
| Macular degeneration (AMD) | Phase Ib (ASP7317) | Phase 2 data expected 2026–2027 |
| Type 1 diabetes | Phase 1/2 (VX-880 beta cells) | Phase 3 projected 2027 |
| ALS | Phase 1/2a (AstroRx) | Phase 2 data 2026 |
| Spinal cord injury | Phase 1 follow-up complete | Phase 2 design underway |
| Heart failure | Preclinical → Phase 1 | 2027–2028 first human trials |
Three Trends Reshaping the Field
1. CRISPR + ESC Combinations
Researchers are now combining CRISPR gene editing with embryonic stem cell technology to create hypoimmune “universal donor” cell lines — cells engineered to evade immune rejection entirely. This would eliminate the need for immunosuppression and make treatments available as truly off-the-shelf products.
2. The Shift Toward iPSC Dominance
The January 2026 NIH announcement reflects a broader scientific consensus: as iPSC technology matures, the ethical and logistical advantages of using a patient’s own reprogrammed cells will likely make them the dominant clinical platform. The Kyoto University iPS Cell Research and Application (CiRA) center in Japan — one of the world’s leading stem cell institutes — is already running human trials using patient-derived iPSC neurons for Parkinson’s with comparable early results to ESC-based approaches.
3. Market Growth Reflects Clinical Confidence
The global human embryonic stem cells market was valued at $2.44 billion in 2025 and is projected to reach $4.00 billion by 2030 (CAGR 10.44%), according to Grand View Research. This is not speculative investment — it reflects Phase 3 trial momentum, manufacturing scale-up, and regulatory approvals expected in the next 48–72 months.
What This Means For You — Action Steps for Patients Today
If you or someone you love has a condition being targeted by ESC research, here are three concrete actions you can take right now:
- ✅ Talk to your specialist — Ask specifically whether your diagnosis (Parkinson’s, AMD, ALS, Type 1 diabetes) qualifies you for any registered stem cell clinical trial
- ✅ Search ClinicalTrials.gov — Filter by condition and “stem cell” to find actively recruiting Phase 2–3 trials near you. Legitimate trials are free to participate in
- ✅ Avoid unregulated clinics — No matter how convincing the testimonials, no hESC treatment outside a registered trial is safe or approved in 2026
For patients exploring new treatments while managing chronic conditions, our expert-reviewed Health Tips hub provides evidence-based guides on everything from cancer symptoms to cardiovascular health. If you’re undergoing or considering immunotherapy as part of a broader treatment plan, our guide on how immunotherapy works explains the immune mechanisms that also underpin stem cell therapy research.
11 Frequently Asked Questions
1. What are embryonic stem cells in simple terms?
Embryonic stem cells are master cells extracted from 3–5 day old human embryos that can develop into any of the body’s 200+ cell types. They are unique because no other cell type naturally retains this level of developmental flexibility in adulthood.
2. Can embryonic stem cells cure Parkinson’s disease?
Not yet — but the evidence is moving faster than at any point in history. A Phase 1 trial published in Nature in April 2025 showed safe cell engraftment and visible tremor reduction in some patients. The FDA has approved a Phase 3 efficacy trial, making a potential approval in 2027–2028 a realistic prospect.
3. Are embryonic stem cells legal in the United States?
Research using the 503 existing NIH-approved hESC lines is legal. New derivation of lines from embryos is prohibited with federal funding. As of January 23, 2026, NIH also paused review of new line applications pending a policy reassessment.
4. What diseases can embryonic stem cells treat?
As of 2026, active clinical trials target Parkinson’s disease, age-related macular degeneration (AMD), ALS, spinal cord injury, and Type 1 diabetes. None are yet commercially approved outside of clinical trials.
5. What is the difference between embryonic and adult stem cells?
Embryonic stem cells are pluripotent — they can become any cell type. Adult stem cells are multipotent — they can only differentiate into a limited range of related cell types. Adult stem cells (hematopoietic/bone marrow) are the only stem cell type currently FDA-approved for routine clinical use.
6. Are embryonic stem cells the same as iPSCs?
No. iPSCs (induced pluripotent stem cells) are adult cells — typically skin or blood cells — that have been genetically reprogrammed to behave like embryonic stem cells. They have similar pluripotent properties but come from the patient’s own body, avoiding both the ethical concerns and immune rejection risk of ESCs.
7. Why are embryonic stem cells controversial?
The extraction process destroys the human embryo. People who believe human life begins at fertilization object on moral grounds. Supporters counter that surplus IVF embryos would otherwise be discarded, and donor consent is always required.
8. Can embryonic stem cells regrow organs?
In theory and in animal models, yes — researchers have used ESCs to generate heart muscle tissue, liver organoids, and retinal structures. In human clinical trials, the focus has been on replacing specific lost cell populations (like dopamine neurons or retinal cells) rather than full organ regeneration, which remains a longer-term goal.
9. What happened to NIH’s embryonic stem cell policy in January 2026?
On January 23, 2026, NIH announced a temporary pause on approving new hESC lines for its registry, and opened a public comment period through April 24, 2026, to assess whether iPSC and adult stem cell alternatives can replace remaining ESC research needs. All 503 previously approved lines and ongoing trials continue unaffected.
10. How long until embryonic stem cell treatments are commercially available?
The Parkinson’s Phase 3 trial is the furthest along — a potential FDA approval could come as early as 2027–2028 for bemdaneprocel. For other conditions, most estimates point to 2028–2033 for broader commercial availability, depending on Phase 3 outcomes and regulatory timelines.
11. Is embryonic stem cell therapy safe?
Based on available Phase 1 clinical data, the safety profile is encouraging. A 10-year follow-up on spinal cord injury patients showed zero tumor formations. The Parkinson’s Phase 1 trial showed zero serious adverse events at 18 months. Larger Phase 3 trials are needed to confirm safety and efficacy at scale.
Reviewed by a credentialed physician from the mymedicineadvisor.com expert panel. For questions about specific symptoms or conditions, use our Symptom Checker or consult a licensed healthcare provider.
📌 Related Reading on mymedicineadvisor.com:
- How Immunotherapy Works — The Complete 2026 Guide
- Neuroblastoma in Kids: 2026 Cures and Treatment Options
- Glioblastoma Survival Rate and Treatment Options
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.