On This Page – Quick Medical Summary
Marcus had been using minoxidil for hair loss for nine months. Twice daily. Never missed an application. Yet his hairline kept retreating. His dermatologist finally explained the truth: Marcus carried a genetic variant that prevented his body from activating the drug. He wasn’t failing minoxidil — minoxidil was failing him, for a biological reason nobody had told him about.
The short answer: Minoxidil works for approximately 80% of users with androgenetic alopecia. The remaining 20% see little to no results — not because they applied it wrong, but because of a specific enzyme their body produces in insufficient amounts. This article explains exactly who responds, who doesn’t, and what science-backed options exist in 2026 when minoxidil stops working.
⚠️ This article is for educational purposes only and does not constitute medical advice. Always consult a qualified dermatologist or healthcare provider before starting any hair loss treatment.
What Is Minoxidil and How Does It Work for Hair Loss?
The Science Behind Every Strand
Minoxidil for hair loss has been FDA-approved since 1988, making it one of only two medications the FDA has cleared for treating pattern baldness. It was originally developed in the 1970s as a blood pressure medication. Physicians noticed an unexpected side effect: patients were growing hair in places they had lost it.
That discovery led to the topical formulation sold today as Rogaine and its generic equivalents.
Here is what makes minoxidil work at the cellular level:
- It is a vasodilator — it widens blood vessels around hair follicles
- This increases the flow of oxygen, nutrients, and blood to dormant follicles
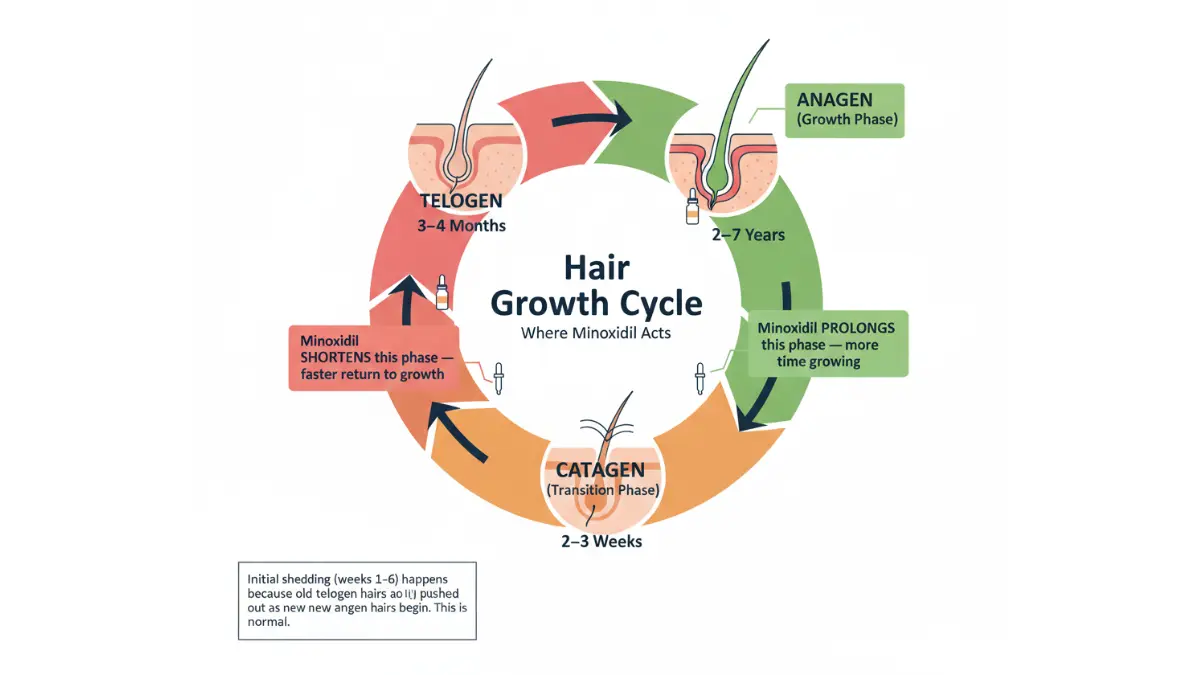
- It prolongs the anagen (active growth) phase of the hair cycle
- It shortens the telogen (resting) phase, pushing follicles back into active growth faster
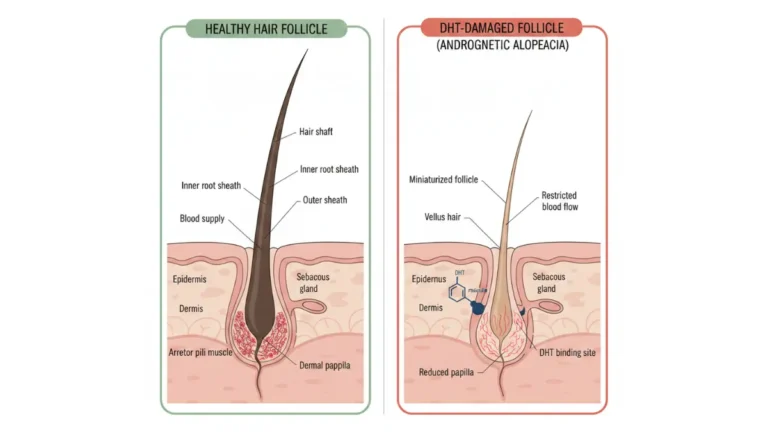
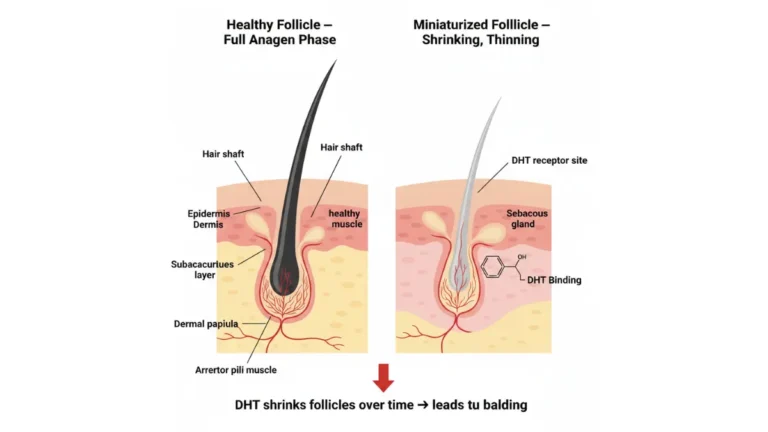
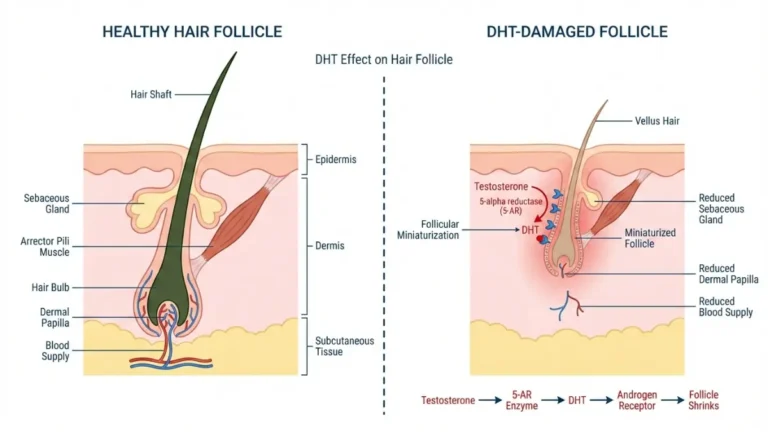
- Over time, it enlarges miniaturized follicles, producing thicker, denser hair strands
But here is the critical detail most articles skip entirely.
Minoxidil Is a Prodrug — It Must Be Converted to Work
Minoxidil does not work in its original form. It is a prodrug, meaning your body must convert it into its active form — minoxidil sulfate — before it can stimulate hair growth.
This conversion happens inside the hair follicle itself, performed by an enzyme called sulfotransferase (SULT1A1). According to a comprehensive review published on the National Library of Medicine, patients with higher sulfotransferase enzyme activity respond significantly better to topical minoxidil than those with lower activity.
This single biological fact explains why 1 in 5 users sees zero results — and almost no major health website tells patients this upfront.
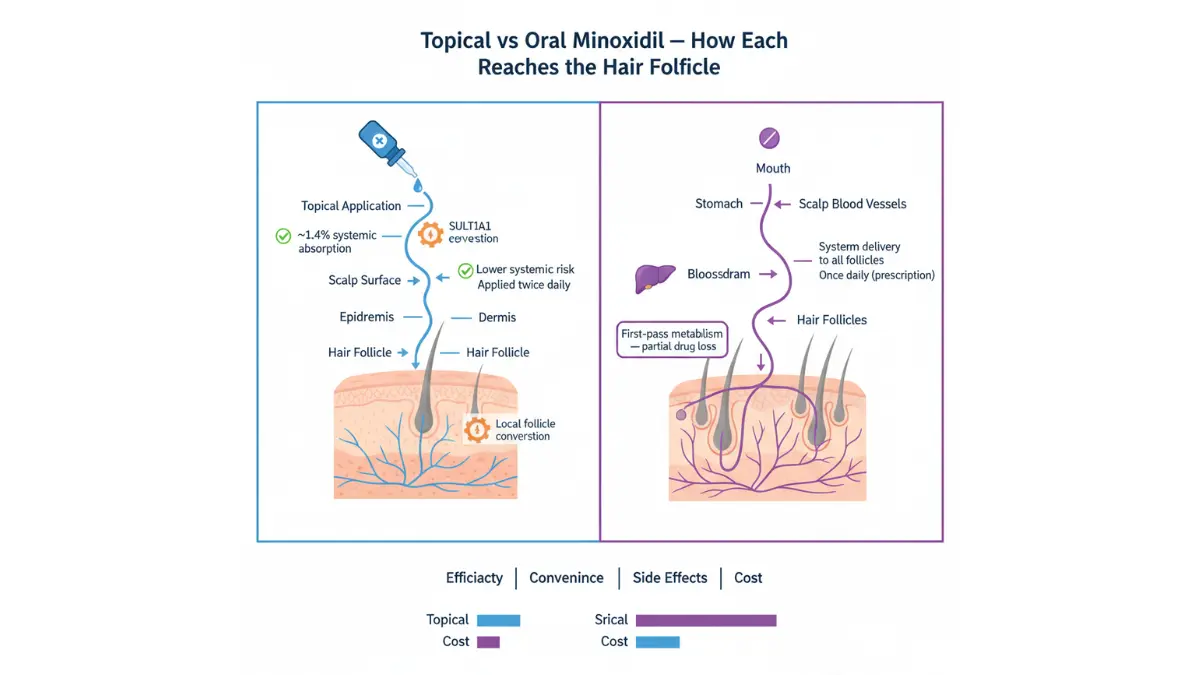
Topical vs. Oral Minoxidil: A 2026 Head-to-Head
| Feature | Topical Minoxidil | Oral Minoxidil |
|---|---|---|
| FDA Approval | ✅ Approved (2%, 5%) | ❌ Off-label for hair loss |
| Application | Scalp, twice daily | Pill, once daily |
| Efficacy (24 weeks) | +7.2% hair density | +12% hair density (JAAD 2020) |
| Main side effects | Scalp irritation, itching | Hypertrichosis, mild edema |
| Best for | New users, early-stage loss | Poor topical compliance |
| Availability | Over the counter | Prescription only |
A 2026 double-blind randomized controlled trial published in the Journal of the American Academy of Dermatology found that 2.5mg oral minoxidil produced comparable results to 5% topical, with better long-term adherence and reduced application-related side effects.
💡 What This Means For You: If you have struggled with topical minoxidil due to scalp irritation or texture changes, ask your dermatologist about low-dose oral minoxidil. It is now widely prescribed across the USA. You can also use our Symptom Checker to log and track your scalp symptoms before your appointment.
Why 1 in 5 People See Zero Results — The SULT1A1 Gene Secret
The Enzyme That Decides If Minoxidil Works for You
The SULT1A1 gene codes for the sulfotransferase enzyme inside hair follicles. This enzyme is the biological gatekeeper of minoxidil’s effectiveness.
If your follicles produce low levels of SULT1A1, the conversion of minoxidil to minoxidil sulfate is incomplete. The drug sits on your scalp without activating. Hair doesn’t grow. You conclude the treatment failed — when in reality, your genetics made it chemically inert.
Research published by the NIH National Library of Medicine confirms that there is no correlation between the amount of minoxidil applied and the hair growth response in low-enzyme individuals. Applying more product does not fix a genetic enzyme deficiency.
You can assess your inherited predisposition to hair loss and enzyme-related response patterns using our Genetic Risk Assessment Tool as a starting point before speaking with a specialist.

The Aspirin and Tylenol Warning Nobody Gives You
This is the most overlooked drug interaction in hair loss treatment.
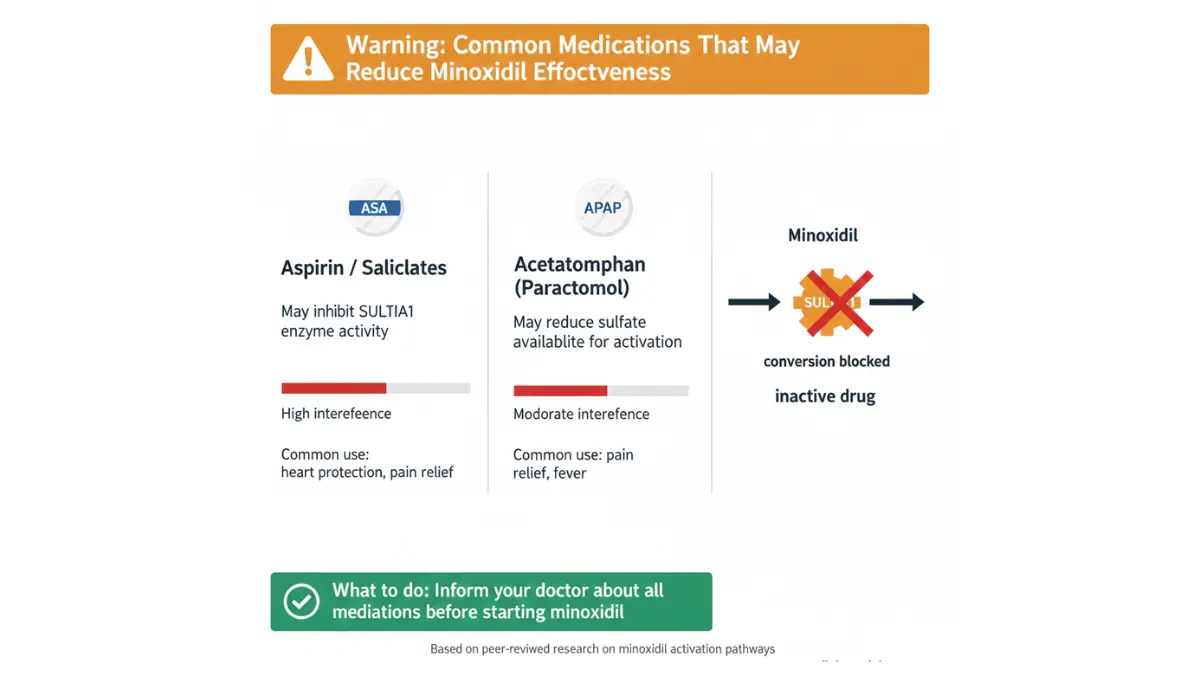
Aspirin (and all salicylates) inhibit the SULT1A1 enzyme. A clinical study showed that just 14 days of low-dose aspirin use caused a measurable drop in follicular sulfotransferase activity. If you are taking a daily aspirin for cardiovascular protection and simultaneously using minoxidil for hair loss, you may be biochemically blocking your own treatment.
Paracetamol (Tylenol/Acetaminophen) acts as a sulfate scavenger in the body, competing for the sulfate groups that minoxidil needs to activate. Regular use of acetaminophen alongside minoxidil may reduce the conversion rate of the prodrug.
⚠️ Bold Callout: If you take daily aspirin for heart health and use minoxidil for hair loss, discuss this interaction with your doctor immediately. You may need to adjust one or both medications.
For more information on how common medications interact with each other, our comprehensive drug interactions guide explains the mechanisms in plain language.
Other Reasons Minoxidil Fails
Beyond genetics, several application and lifestyle factors cause minoxidil for hair loss to underperform:
- Applying to a wet scalp — reduces absorption by disrupting the concentration gradient
- Using on severely scarred follicles — dead follicles cannot be revived by any topical treatment
- Applying outside the vertex area — minoxidil is FDA-approved for crown/vertex only, not the frontal hairline
- Inconsistent use — hair follicles revert toward baseline within 12–24 weeks of stopping
- Using a hairdryer immediately after application — heat degrades the solution before absorption
- Scalp inflammation — infected or irritated scalp causes unpredictable absorption spikes
💡 What This Means For You: Before concluding that minoxidil doesn’t work for you, audit all four variables — genetics, drug interactions, scalp health, and application technique. Three of the four are completely within your control.
Who Does Minoxidil Actually Work Best For?
The Ideal Responder Profile (2026 Clinical Data)
Minoxidil for hair loss consistently delivers the strongest results in patients who match this profile:
| Factor | Best Response | Reduced Response |
|---|---|---|
| Age | Under 40 | Over 55 |
| Hair loss duration | Under 5 years | Over 10 years |
| Hair loss type | Androgenetic alopecia | Scarring alopecia |
| Area of loss | Vertex / crown | Frontal hairline |
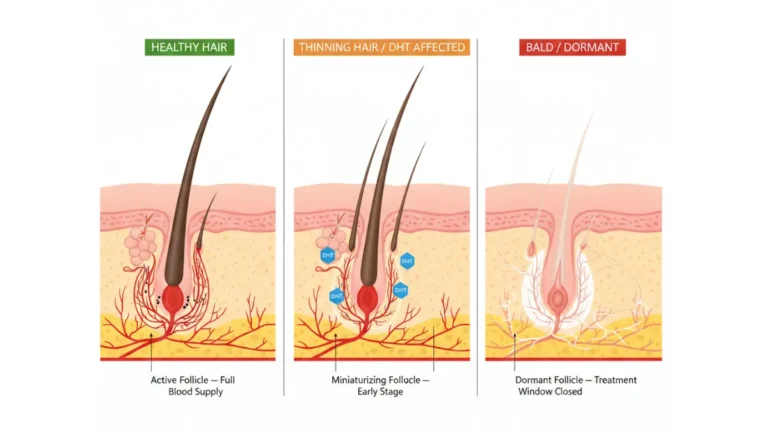
| Follicle status | Miniaturized, still alive | Fully dormant or scarred |
| SULT1A1 activity | High | Low |
Clinical trials consistently show that minoxidil works best for early-stage hair loss in younger patients with intact but miniaturized follicles. Once a follicle has been completely dormant for years, the odds of regrowth drop significantly.
Minoxidil for Women: Different Rules, Stronger Long-Term Data
Women respond differently to minoxidil for hair loss than men — and in some cases, better over the long term.
A 2025 case series published in the Journal of the American Academy of Dermatology documented continued year-on-year improvement in hair density among women using systemic minoxidil — well beyond the 12-month peak typically cited in standard guides.
For women specifically:
- 2% topical is the FDA-approved dose for female pattern hair loss (FPHL)
- 5% topical foam is widely used off-label under medical guidance
- Low-dose oral (0.625–1.25mg/day) is now recommended by international Delphi consensus for women who struggle with topical application
- Postmenopausal women should discuss cardiovascular monitoring with their doctor before starting oral forms
For a dedicated deep-dive, read our expert guide on minoxidil for women which covers female-specific dosing, timing, and the hormonal factors that affect response.
Minoxidil for Men: Timeline Expectations Nobody Sets Correctly
Most websites say results appear in “4–6 months.” This is misleading.
Here is the accurate, evidence-based timeline:
| Timeframe | What Actually Happens |
|---|---|
| Weeks 1–6 | Initial shedding (normal — old hairs pushed out) |
| Month 2–3 | Shedding slows; microscopic vellus hair begins forming |
| Month 4–6 | First visible soft new hairs appear |
| Month 6–9 | Hair density visibly improves |
| Month 12 | Peak efficacy — maximum achievable regrowth |
| Year 2+ | Maintenance phase; continued use required to sustain results |
The 45% greater hair regrowth seen with 5% vs 2% minoxidil at week 48 (per published RCT data) only materialises with consistent, uninterrupted daily use through to the 12-month mark.
How to Use Minoxidil Correctly — Most People Get This Wrong
The Application Protocol That Maximizes Absorption
Getting the application right is non-negotiable. Here is the step-by-step protocol validated by clinical guidelines:
- Ensure your scalp is completely dry before applying — wet scalp reduces drug absorption
- Part hair to expose the thinning area on the scalp
- Apply to scalp skin, not hair — the drug works at follicle level, not on the hair shaft
- Use the prescribed amount only — more product does not mean faster results
- Wash hands immediately after applying to avoid unintentional transfer to other skin areas
- Allow 2–4 hours to dry before going to bed — wet product transfers to pillowcases
- Do not shampoo for 4 hours after application
- Never use a hairdryer on the treated area immediately after applying
For those taking the oral form, use our Pill Identifier to confirm your tablet before beginning any new medication regimen.
Application Mistakes That Quietly Kill Results
The following errors are extremely common and directly reduce minoxidil efficacy:
- Applying to an inflamed or infected scalp — creates dangerous absorption spikes
- Using simultaneously with other scalp products (oils, serums, leave-ins) — these create a barrier
- Targeting the hairline instead of the vertex — minoxidil is not approved for frontal recession
- Stopping during the initial shedding phase — this phase means the drug IS working; stopping reverses all progress
2026 Oral Minoxidil Dosing Reference
Per the international Delphi consensus published in JAMA Dermatology (January 2025):
| Patient Group | Starting Dose | Range |
|---|---|---|
| Women | 1.25 mg/day | 0.625–5 mg/day |
| Men | 2.5 mg/day | 1.25–5 mg/day |
| Adolescents | Lower doses | Under specialist supervision |
Oral minoxidil requires a prescription in the USA, UK, Canada, and Australia. Cardiac contraindications include pericardial disease and uncontrolled hypertension. Always disclose all current medications to your prescribing physician.
The FDA’s official drug database at accessdata.fda.gov provides the full approved prescribing information for reference.
Minoxidil Side Effects and Drug Interactions — The Complete Picture
Common Side Effects: Topical vs. Oral
| Side Effect | Topical | Oral |
|---|---|---|
| Scalp itching / redness | Common | Rare |
| Initial hair shedding | Common (weeks 1–6) | Less common |
| Hypertrichosis (unwanted hair growth) | Rare | 24% incidence |
| Peripheral edema (mild swelling) | Very rare | ~2% at therapeutic doses |
| Dizziness / hypotension | Very rare | Monitor in first weeks |
| Contact dermatitis | Possible (propylene glycol) | N/A |
Initial shedding is normal and expected. It indicates that dormant hairs are being displaced by new growth underneath. This phase typically resolves within 2–6 weeks and is not a reason to stop treatment.
The Drug Interaction Nobody Talks About
Revisiting this because it is genuinely critical and widely ignored:
- Aspirin → inhibits SULT1A1 → blocks minoxidil activation
- Acetaminophen / Tylenol → depletes sulfate pool → reduces minoxidil sulfate conversion
- Antihypertensives → additive blood pressure lowering → monitor carefully with oral form
- Other topical scalp medications → may alter absorption of minoxidil unpredictably
Inform your doctor about every medication you take — including over-the-counter pain relievers — before starting minoxidil. The NIH StatPearls minoxidil monograph outlines all major pharmacological interactions in clinical detail.
Who Should Not Use Minoxidil
Absolute contraindications include:
- Pregnant or breastfeeding women (topical or oral)
- Children under 18 years of age
- Patients with pericardial effusion or uncontrolled hypertension (oral form)
- Patients with active scalp infection, inflammation, or open wounds
- Sudden, patchy, or unexplained hair loss (requires diagnosis first — use our Symptom Checker to document before your appointment)
If you are concerned about cardiovascular health before starting oral minoxidil, reviewing our guide on preventing heart disease can help you understand the baseline health factors your doctor will assess.
When Minoxidil Doesn’t Work — Your 2026 Options
Combination Therapy: The Science-Backed Upgrade Path
For non-responders or partial responders, combination therapy significantly outperforms minoxidil alone. A 2025 network meta-analysis in Frontiers in Medicine ranked combination approaches by SUCRA scores (higher = more effective):
| Combination | SUCRA Score | Evidence Level |
|---|---|---|
| Microneedling + Minoxidil | 87.20% | Moderate |
| Silk thread + Minoxidil | 84.51% | Low-Moderate |
| Spironolactone + Minoxidil | 56.63% | Moderate (women) |
| PRP + Minoxidil | 53.88% | Emerging |
| Minoxidil alone | 36.00% | Strong baseline |
Microneedling (dermarolling) creates microchannels in the scalp that increase topical minoxidil absorption by up to 4x. It also independently stimulates growth factors in hair follicles. This is currently the strongest evidence-backed addition to a minoxidil routine.
For patients where DHT is the primary driver of hair loss, combining minoxidil with a DHT blocker is clinically supported. Read our expert breakdown on DHT blockers doctors recommend for the latest evidence-based options.
For an overview of every evidence-ranked treatment available in 2026, our comprehensive hair loss treatments guide covers surgical, pharmaceutical, and emerging biological options side by side.
What’s Coming: The Future of Minoxidil Treatment
Three breakthrough developments are advancing through clinical trials as of late 2025:
1. Extended-Release Oral Minoxidil (VDPHL01) Developed by Veradermics. Phase 3 trials ongoing as of September 2025. Designed to provide steady-state drug delivery with reduced side effect peaks.
2. Sublingual Minoxidil Under development by Samson Clinical. Phase 3 trials ongoing. Sublingual delivery bypasses first-pass liver metabolism, resulting in less SULT enzyme dependency and potentially better efficacy for low-responders.
3. AB-103 — The Non-Responder Solution A SULT1A1 stimulant currently in development that directly enhances the enzyme conversion process in hair follicles. If approved, this could theoretically eliminate the 20% non-responder problem entirely.
You can track all active minoxidil clinical trials through the official ClinicalTrials.gov database to see which studies are currently enrolling participants.
If you are exploring whether hair loss is reversible at your current stage, our evidence-based guide on reversible hair loss treatment provides a clear framework for what can and cannot be recovered based on follicle status.
Frequently Asked Questions about Minoxidil for Hair Loss
1. Does minoxidil for hair loss actually work?
Yes — for approximately 80% of users with androgenetic alopecia, minoxidil slows hair loss and stimulates regrowth. Results require consistent daily use for at least 12 months for maximum effect.
2. How long does minoxidil take to work?
Visible results typically begin at 4–6 months, but peak efficacy occurs at 12 months. Initial shedding in weeks 1–6 is normal and indicates the treatment is working.
3. Why is minoxidil not working for me?
The most common reason is low SULT1A1 enzyme activity — a genetic trait that prevents conversion of minoxidil to its active form. Drug interactions with aspirin or acetaminophen, incorrect application, and late-stage follicle loss are also major causes.
4. Can I take aspirin while using minoxidil?
You should discuss this with your doctor. Aspirin inhibits the SULT1A1 enzyme that activates minoxidil. Daily aspirin use has been shown to reduce follicular enzyme activity within 14 days, potentially undermining hair loss treatment.
5. Is oral minoxidil better than topical minoxidil?
Both produce comparable hair density results. Oral minoxidil offers better compliance and convenience but requires a prescription and carries systemic side effects. Topical remains the first-line choice; oral is the preferred alternative for those who cannot tolerate topical application.
6. What happens if I stop using minoxidil?
Hair loss resumes. Any regrowth gained during treatment will be lost within 12–24 weeks of stopping, and hair density returns to pre-treatment levels.
7. Can women use minoxidil for hair loss?
Yes. 2% topical is FDA-approved for female pattern hair loss. 5% foam is widely used off-label. Low-dose oral (0.625–1.25mg/day) is now supported by international consensus for women who find topical application difficult.
8. What is the correct dose of oral minoxidil for hair loss?
Per 2025 Delphi consensus: women start at 1.25mg/day (range 0.625–5mg) and men at 2.5mg/day (range 1.25–5mg). Always prescribed by a physician following cardiovascular screening.
9. Does minoxidil work on a receding hairline?
Minoxidil is FDA-approved for the vertex (crown) only. Evidence for frontal hairline regrowth is limited. It performs poorly on significantly receded hairlines and is not recommended as a primary treatment for this pattern.
10. What are the most common side effects of minoxidil?
Topical: scalp itching, initial shedding, contact dermatitis. Oral: unwanted hair growth (hypertrichosis) in 24% of users, mild leg swelling (2%), and rare dizziness. Serious cardiovascular side effects are uncommon at doses used for hair loss.
11. Is minoxidil safe for long-term use?
Yes — decades of clinical data support long-term topical use safety. Oral minoxidil requires periodic monitoring of blood pressure and cardiovascular status. The American Academy of Dermatology provides updated guidance on long-term hair loss treatment management.
Reviewed and verified by the mymedicineadvisor.com medical panel. Last updated February 2026. This article is for educational purposes only. It does not replace professional medical advice, diagnosis, or treatment. Consult a licensed dermatologist or physician before starting any hair loss medication.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.