On This Page – Quick Medical Summary
Quick Answer: A receding hairline — caused by DHT attacking frontal scalp follicles — can be stopped and partially reversed with the right treatment. In 2026, dermatologists recommend a combination of finasteride and minoxidil as the gold standard. Early treatment at Norwood Stage 1–3 delivers the best outcomes. Read on for the complete, evidence-based guide.
Marcus, 31, noticed his temples had pulled back nearly half an inch in 18 months. His doctor started him on an oral finasteride-minoxidil combination in early 2025. By month 9, his dermatologist documented measurable density regrowth along the hairline — not a miracle, but real clinical progress. The key? He started before his follicles were permanently scarred.
If your hairline is receding, you are not alone. Approximately 50 million men and 30 million women in the United States are affected by androgenetic alopecia — the most common cause of hairline loss worldwide. The good news: 2026 has brought clearer evidence, better combination protocols, and breakthrough drugs in the pipeline that could transform treatment within two years.
What this guide covers:
- Why your receding hairline is happening (and how fast it will progress)
- Every FDA-approved and clinically proven treatment — ranked by evidence
- The 2026 combination protocol that outperforms all single treatments
- What’s new this year that competitors haven’t covered
- A dedicated section for women
- Exactly when and why you need to see a dermatologist — now
⚠️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified, board-certified dermatologist or healthcare provider before starting any hair loss treatment.
What Causes a Receding Hairline — And How Fast Will It Progress?
The DHT–Follicle Connection
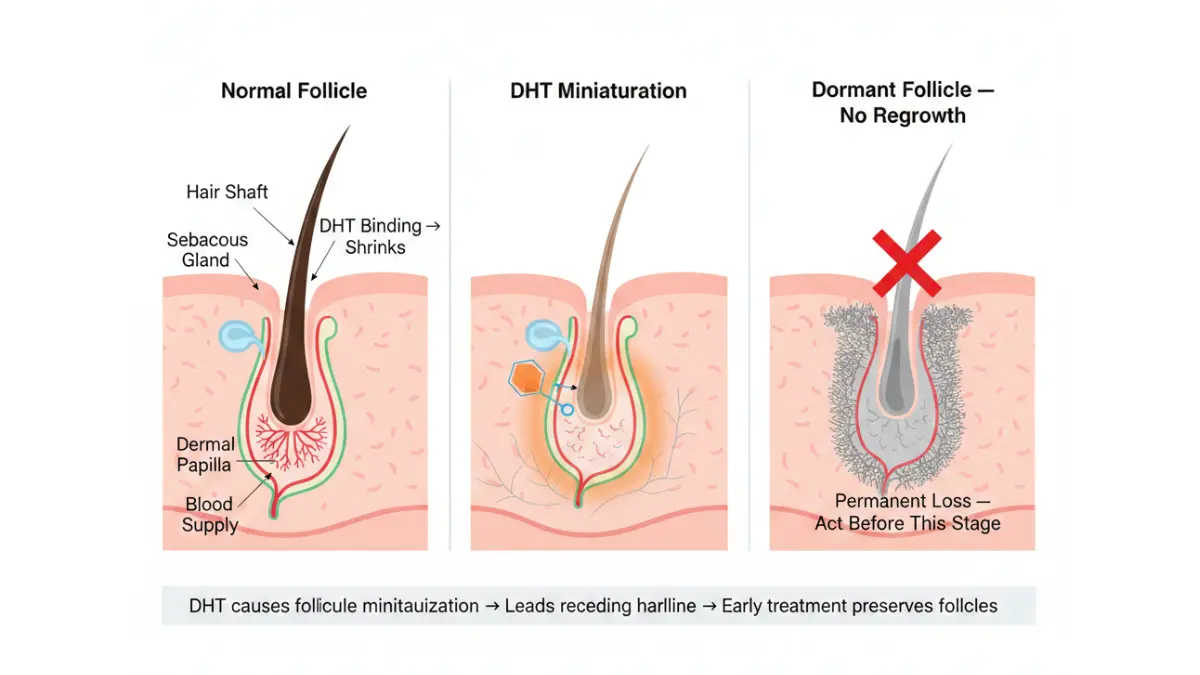
A receding hairline is not random. It follows a predictable biological pathway driven by a hormone called dihydrotestosterone (DHT).
DHT is a potent byproduct of testosterone. In people genetically predisposed to androgenetic alopecia, DHT binds to androgen receptors in the scalp’s frontal and temple follicles, causing them to miniaturize progressively. Each hair growth cycle produces a thinner, shorter hair — until the follicle goes dormant entirely.
The frontal hairline is typically the first target because androgen receptor density is highest at the temples. Once a follicle scars over, it cannot be revived by any current treatment — which is why the timing of intervention matters enormously.
You can use our Genetic Risk Assessment Tool to evaluate your hereditary hair loss risk before your first dermatology appointment.
Who Develops a Receding Hairline?
The data is unambiguous:
- 65% of men show visible hairline recession by age 35
- 85% of men have significantly thinner hair by age 50
- 33–50% of women experience some form of pattern hair loss by age 50–70
- Men whose fathers are bald are 5–6 times more likely to develop a receding hairline
- Genetics account for roughly 80% of androgenetic alopecia susceptibility, according to the American Academy of Dermatology
The Norwood Scale — Where Is Your Hairline Right Now?
The Norwood Scale classifies male hairline recession into 7 stages. Knowing your stage determines which treatments are appropriate and what outcomes are realistic.
| Norwood Stage | Description | Treatment Response |
|---|---|---|
| Stage 1 | No visible recession | Preventative options; excellent response |
| Stage 2 | Slight temporal recession | Strong response to finasteride + minoxidil |
| Stage 3 | Deeper temporal recession, M-shape forming | Good response; combination therapy recommended |
| Stage 4 | Significant frontal loss + crown thinning | Moderate response; combination + possible PRP |
| Stage 5 | Frontal and crown loss merging | Reduced medication response; transplant evaluation |
| Stage 6 | Only side/back hair remains | Primarily surgical options |
| Stage 7 | Minimal remaining hair | Hair transplant or scalp micropigmentation |
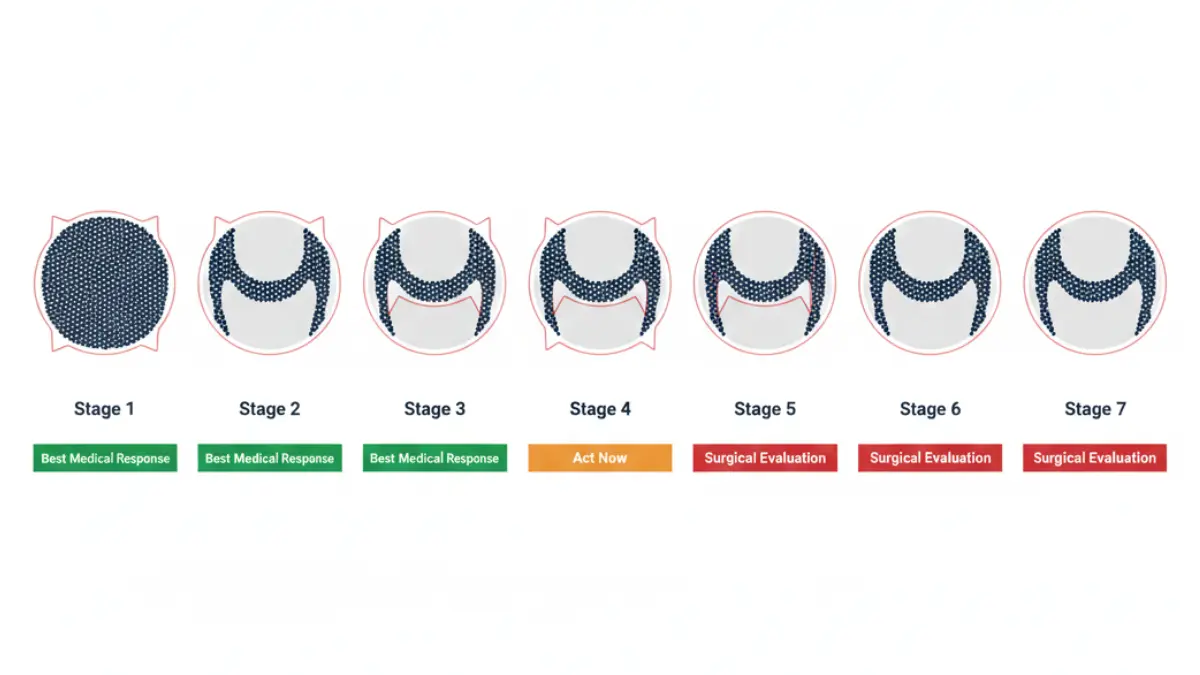
Key insight: Every stage you delay treatment costs active follicles you cannot get back. Stages 1–4 respond meaningfully to medical therapy. Stages 5–7 generally require surgical intervention.
If you notice hair-related symptoms beyond typical pattern loss, our Symptom Checker can help you identify whether a broader health issue may be contributing.
FDA-Approved Receding Hairline Treatments — Ranked by 2025 Evidence
What the Evidence Hierarchy Actually Shows
Only two treatments hold full FDA approval for androgenetic alopecia: oral finasteride and topical minoxidil. Everything else is off-label or emerging. Here is what the current clinical data says about each — with no marketing bias.
Finasteride — The Hairline Specialist
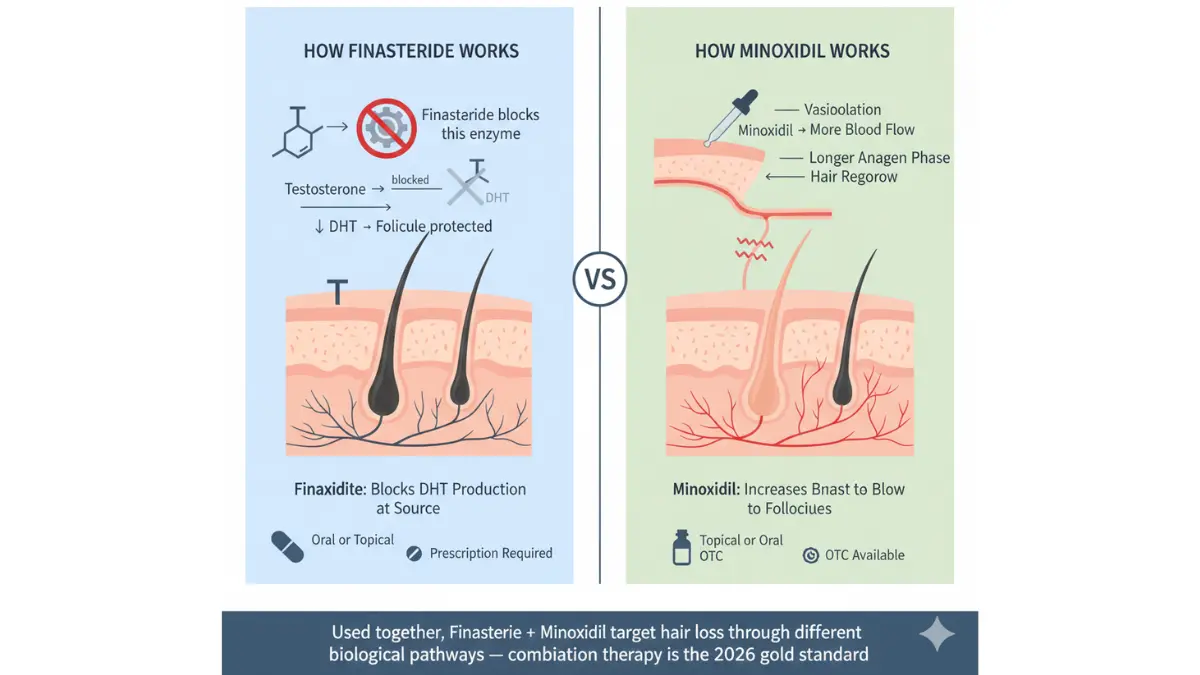
Finasteride (brand name Propecia) works by blocking the Type II 5-alpha-reductase enzyme, reducing scalp DHT levels by approximately 70%.
It is particularly effective for frontal hairline recession — more so than minoxidil alone. Clinical phase III data from 1,879 men shows:
- 66% showed improvement in hair growth at 2 years
- 83% of finasteride users had no further hairline loss at 2 years vs. 28% of placebo users
- Finasteride slows further hair loss in 80–90% of men who take it, per the American Academy of Dermatology’s male pattern hair loss guide
Side effects: Fewer than 2% of men experience sexual side effects (decreased libido, erectile changes). These are generally reversible within approximately one week of stopping the medication.
Important 2025 update: An October 2025 commentary flagged the need for closer psychiatric monitoring in younger male patients — specifically around depression risk. Always disclose your mental health history to your prescribing physician before starting finasteride.
Topical finasteride is now available as a spray formulation. A Phase III randomized controlled trial published on PubMed demonstrated similar efficacy to oral finasteride with markedly lower systemic DHT reduction — meaning fewer potential side effects for those concerned about systemic exposure.
For a deeper look at how DHT blockers work, read our expert guide on DHT Blockers — What Doctors Reveal.
Minoxidil — Topical vs. Oral in 2026
Minoxidil increases blood flow to follicles and extends the anagen (active growth) phase. However, its specific effect on the frontal hairline is weaker than finasteride when used alone.
Topical minoxidil (5%):
- Best documented for crown thinning
- Some evidence for stabilizing hairline recession
- Available OTC without prescription
- Foam form preferred: dries faster, less scalp irritation than solution
Oral minoxidil (2.5mg) — the 2026 game-changer:
Oral minoxidil is the fastest-growing prescription option in dermatology. A landmark 2025 meta-analysis of 2,933 patients across 27 studies published in Frontiers in Pharmacology showed:
- 35% of patients experienced significant symptom improvement
- 47% showed meaningful improvement
- 82% total responder rate across all alopecia types
- Oral minoxidil reaches the hairline systemically — an advantage over topical formulations
The main side effect is hypertension at higher doses; at 2.5mg, incidence was minimal with no study withdrawals.
For more detail on minoxidil’s mechanisms and dosing, see our in-depth guide on Minoxidil for Hair Loss.
Dutasteride — The More Potent Option
Dutasteride is a second-generation 5-alpha-reductase inhibitor. It is:
- 3x more potent than finasteride at blocking Type I enzyme
- 100x more potent at blocking Type II enzyme
- Off-label in the US but FDA-approved in South Korea for androgenetic alopecia
A 2025 network meta-analysis ranked dutasteride 0.5mg/day as the single most effective pharmacological agent for androgenetic alopecia — surpassing finasteride monotherapy.
If finasteride has not delivered satisfactory results after 12 months, ask your dermatologist about dutasteride before considering surgical options.
| Treatment | FDA Status (US) | Evidence Strength | Best For |
|---|---|---|---|
| Finasteride 1mg oral | ✅ Approved (men) | High — Phase III RCTs | Hairline recession, crown |
| Minoxidil 5% topical | ✅ Approved | High | Crown, early hairline |
| Oral Minoxidil 2.5mg | ⚠️ Off-label | High — 2025 meta-analysis | Both patterns |
| Dutasteride 0.5mg oral | ⚠️ Off-label (US) | High — 2025 NMA | Resistant or advanced AGA |
| Topical Finasteride | ⚠️ Off-label | Moderate-High — Phase III | Side effect-sensitive patients |
The 2026 Combination Protocol — What Dermatologists Are Actually Prescribing
Why Monotherapy Is No Longer Optimal
Using one treatment alone is increasingly considered suboptimal by leading dermatologists. The reason is mechanistic: finasteride attacks DHT production while minoxidil stimulates follicular blood flow independently. They work via entirely different pathways — making them highly complementary.
Finasteride + Minoxidil — The Gold Standard Combination
A 2025 systematic review and meta-analysis published in Frontiers in Medicine, analyzing seven randomized controlled trials across five countries (Thailand, India, Italy, Pakistan, and Indonesia) involving 396 male AGA patients, confirmed that the finasteride + minoxidil combination achieves a SUCRA ranking of 80.18% — the most effective treatment combination for men with a receding hairline.
You can read the full 2025 Frontiers in Medicine meta-analysis on combination therapy directly.
The “All-in-One” Pill — University of Bristol, January 2025
A collaborative study from the University of Bristol and Imperial College London evaluated a single oral pill combining:
- Low-dose minoxidil (2.5mg)
- Finasteride (1mg)
The rationale: topical regimens suffer from poor adherence. A once-daily combined pill eliminates the compliance barrier, maintains equivalent efficacy, and reduces individual drug dosing. This protocol is already being prescribed by forward-thinking dermatologists in the US and UK.
PRP + Growth Factors — The Highest-Efficacy Option Available Now
A comprehensive 2025 network meta-analysis published in Frontiers in Medicine analyzed 20 treatment groups and found that PRP combined with basic fibroblast growth factor (bFGF) achieved a SUCRA ranking of 93.06% — the highest efficacy rating of any combination analyzed.
Key results:
- Mean increase of +35.12 hairs/cm² compared to minoxidil alone
- Non-surgical, in-clinic procedure
- Typically 3–6 sessions, spaced 4–6 weeks apart
- Best suited for Norwood Stages 2–4
PRP is not covered by most US insurance plans, but it represents the most clinically advanced non-surgical option currently available. For a detailed guide on outcomes, see our PRP Therapy Results article.
The “Big 4” At-Home Protocol
For patients who cannot afford or access PRP, dermatologists increasingly recommend a structured at-home combination approach:
- Finasteride (oral 1mg/day or topical spray) — blocks DHT at the follicle
- Minoxidil (foam 5% twice daily or oral 2.5mg once daily) — stimulates follicular blood flow
- Dermaroller (0.5mm) — weekly microneedling stimulates follicular repair via controlled micro-injury
- Ketoconazole 2% shampoo — shown in clinical studies to block DHT locally; used 2–3x/week
Realistic patient timeline:
| Timeframe | What to Expect |
|---|---|
| Month 1 | Possible initial shedding (normal — weak hairs cycling out) |
| Month 3 | Shedding stops; follicles stabilizing |
| Month 6 | First visible density improvement in most patients |
| Month 12 | Full assessment of treatment response |
| Ongoing | Treatment must continue indefinitely to maintain results |

Since hair is made largely of keratin protein, nutritional support matters. Use our Protein Intake Calculator to ensure you are meeting your daily protein targets to support hair shaft health.
2026 Breakthrough Treatments — What Most Guides Have Not Covered
The Treatments Changing Everything in the Next 2 Years
The next wave of receding hairline treatments does not just improve on existing options — it targets hair follicle biology at a completely different level. None of these replace finasteride or minoxidil today, but by 2027, the landscape may look significantly different.
PP405 — TIME Magazine’s Best Invention of 2025
Pelage Pharmaceuticals’ PP405 is the most talked-about development in hair loss science. Unlike finasteride (which blocks hormones) or minoxidil (which increases blood flow), PP405 works at the cellular metabolic level.
How it works:
- PP405 is a mitochondrial pyruvate carrier (MPC) inhibitor
- It causes pyruvate buildup in hair follicle stem cells, increasing lactate production
- This metabolic shift reactivates dormant follicle stem cells — effectively switching dormant follicles back on
Phase 2a clinical data (June 2025):
- 31% of men with advanced baldness achieved greater than 20% hair density increase after just 8 weeks
- Results were particularly strong in men with higher degrees of hair loss — the patients who respond least to existing treatments
Current status: Phase 3 clinical trials are planned for launch in 2026. If successful, commercial availability is projected for 2027–2029.
⚠️ Critical Warning: PP405 is not commercially available as of 2026. Any online seller claiming to offer PP405 is selling an unverified, potentially dangerous product. Do not purchase it.
Clascoterone (Breezula) — The Topical Anti-Androgen
Clascoterone is a topical DHT-blocking molecule with a unique advantage: it works at the receptor level without systemic hormonal effects.
- FDA and EU regulatory submission expected Spring 2026
- Particularly relevant for women with hairline recession — a safe alternative to oral finasteride (which carries teratogenic risk in premenopausal women)
- Early trials showed scalp DHT reduction comparable to topical finasteride with a cleaner side effect profile
Exosome Therapy — Regenerative Medicine at the Follicle
Exosome therapy delivers concentrated growth factors, cytokines, and signaling proteins directly into scalp follicles via injection. A 2025 systematic review published in the World Journal of Stem Cells confirmed regenerative potential in hair follicle restoration.
Key details:
- Combines well with microneedling and PRP
- Particularly effective for treatment-resistant cases and post-surgical shedding
- Currently available at specialist clinics; no standalone FDA approval yet
For more on regenerative approaches, explore our guide to Regenerative Medicine Results and Stem Cell Therapy Results.
Receding Hairline in Women — The Underserved Reality
Why Women Are Being Left Behind by Most Hair Loss Guides
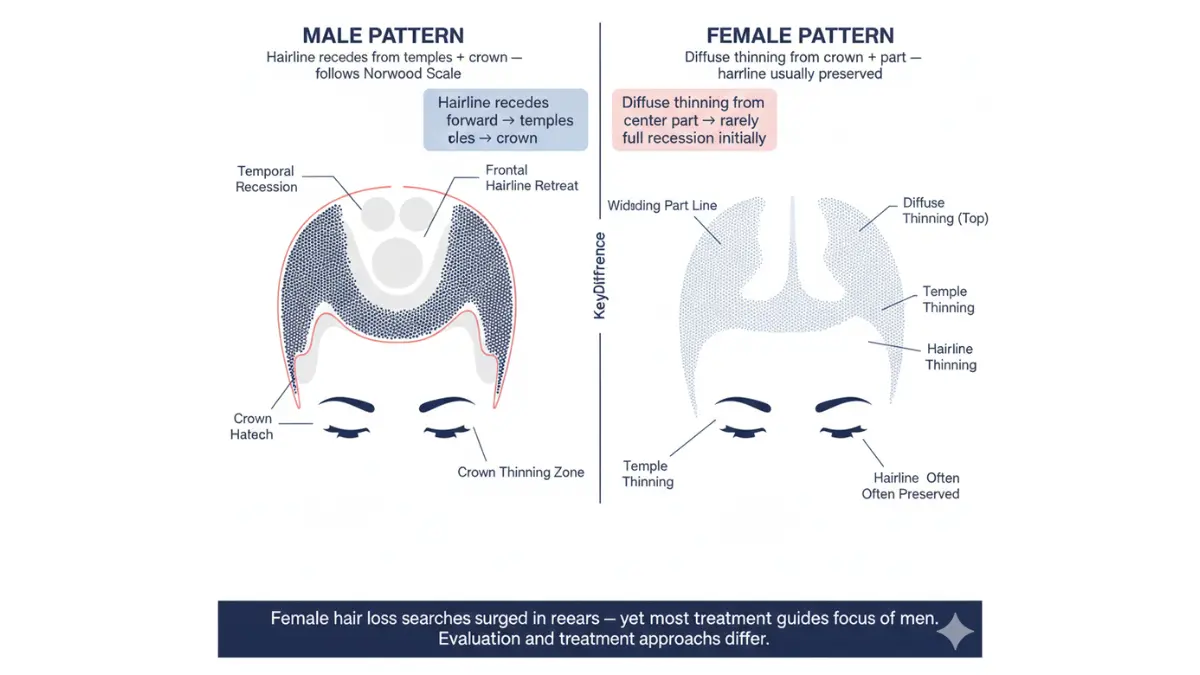
Female hair loss searches surged 125% in 2025 — yet the overwhelming majority of online resources, including top-ranking competitors, are written almost entirely for men.
Women experience hairline changes differently, and the treatment options differ too.
How Female Receding Hairline Differs
Female pattern hair loss (FPHL) typically presents as:
- Widening part line at the crown
- Diffuse thinning across the top of the scalp
- Temple recession — less common but rising, particularly in perimenopausal women
Common triggers in women include:
- Hormonal shifts (perimenopause, postpartum, PCOS)
- Traction alopecia — from tight hairstyles (braids, extensions, ponytails)
- Nutritional deficiencies — iron, Vitamin D, zinc
- Chronic psychological stress
The American Academy of Dermatology’s female pattern hair loss guide confirms that FPHL is progressive without treatment — but highly treatable when caught early.
What Dermatologists Recommend for Women With a Receding Hairline in 2026
| Treatment | FDA Status | Notes for Women |
|---|---|---|
| Minoxidil 2% or 5% topical | ✅ FDA-Approved | First-line; approved for women |
| Oral Minoxidil 0.25–1mg | ⚠️ Off-label | Growing first-choice in dermatology |
| Spironolactone | ⚠️ Off-label | Anti-androgen; widely prescribed for FPHL |
| Clascoterone (Breezula) | 🔬 Pending (Spring 2026) | Expected to become preferred option |
| PRP Therapy | ⚠️ Off-label | Strong evidence; no hormonal impact |
| Finasteride | ⚠️ Not for premenopausal women | Teratogenic risk; avoid in women of childbearing age |
What this means for you (women): Do not follow male-directed hair loss guides. The medications, dosages, and priorities are different. Ask your dermatologist specifically about oral minoxidil and spironolactone — both are now commonly prescribed for women experiencing temple and hairline recession.
For a dedicated deep-dive, read our evidence-based guide to Minoxidil for Women.
When to See a Dermatologist — Decision Framework + Lifestyle Factors
See a Dermatologist Immediately If You Notice Any of These
Do not wait. Early intervention is the single most important variable in treatment success. According to AAD’s hair loss diagnosis and treatment guidance, treatment initiated early produces measurably superior outcomes.
See a dermatologist within 4 weeks if:
- Your hairline has receded visibly within the last 6 months
- You are experiencing patchy hair loss (not pattern-based) — this may indicate alopecia areata
- Hair loss is accompanied by itching, burning, or scalp pain
- You are a woman noticing temple recession before age 45
- You have tried OTC minoxidil consistently for 6 months with no result
- Hair loss is accompanied by fatigue, weight changes, or skin changes (possible thyroid issue)
Lifestyle Factors That Accelerate Hairline Loss
Medical treatment works best when lifestyle contributors are also addressed. Dermatologists consistently flag these factors:
- Smoking: Directly associated with early-onset androgenetic alopecia via oxidative stress and reduced scalp blood flow
- Nutritional deficiencies: Iron, Vitamin D, Zinc, and Biotin deficiencies all accelerate hair follicle cycling disruption. Get blood levels checked at your first dermatology appointment
- Chronic stress: Elevates cortisol → triggers telogen effluvium → accelerates androgenetic loss
- Poor sleep: Chronic sleep deprivation elevates cortisol and disrupts growth hormone release, both of which impair hair follicle cycling. Use our Sleep Calculator to optimize your nightly rest
- Tight hairstyles: Traction alopecia can mimic or worsen receding hairline — particularly in women
Your 3-Step Action Plan — Start Today
Step 1: Assess your Norwood stage using a mirror and the chart in Section 1. Take dated photos of your hairline from the same angle every 3 months.
Step 2: Book a dermatologist appointment. Bring at least 12 months of hairline photos. Ask specifically about finasteride, oral minoxidil, and whether combination therapy is appropriate for you.
Step 3 (if Norwood 1–3 and awaiting appointment): Consider starting OTC topical minoxidil 5% foam — it is FDA-approved, safe to self-start, and every week you delay is a week of potential follicle miniaturization.
What This Means For You: The biggest clinical mistake people make is waiting until Norwood 4–5 before seeking treatment. Every stage of progression represents follicles that no longer respond to medication. Act in Stage 1–3, and your statistical odds of meaningful regrowth are excellent.
For a comprehensive look at hair regrowth surgery options when medical therapy is insufficient, read our guide on Hair Growth Surgery.
Frequently Asked Questions about Receding Hairline
Q1: Can a receding hairline grow back?
Yes — if follicles have not permanently scarred. Norwood Stages 1–3 respond well to finasteride and minoxidil combinations, with measurable regrowth in up to 66% of men within 2 years. Earlier treatment = significantly better outcomes.
Q2: How long do receding hairline treatments take to work?
Finasteride typically shows results at 6 months, with full effect at 12 months. Oral minoxidil often stabilizes shedding within 3 months. PRP with growth factors can show density gains within 6–8 weeks in some patients.
Q3: Is minoxidil or finasteride better for a receding hairline?
Finasteride is generally superior for the frontal hairline specifically, as it directly blocks DHT at the follicle. Combining both is the 2026 gold standard — the 2025 meta-analysis of 396 patients confirmed their combination outperforms either drug alone.
Q4: What is the fastest treatment for a receding hairline?
PRP combined with basic fibroblast growth factor showed the highest overall efficacy in 2025 research (SUCRA 93.06%). For medications, oral minoxidil typically works faster than topical due to systemic delivery.
Q5: Can women use finasteride for a receding hairline?
Generally not recommended for premenopausal women due to birth defect risk. Dermatologists instead use oral minoxidil, spironolactone, or the upcoming clascoterone. Postmenopausal women may sometimes be prescribed finasteride off-label.
Q6: What is PP405 and when will it be available?
PP405 by Pelage Pharmaceuticals reactivates dormant hair follicle stem cells via cellular metabolism. TIME Magazine named it one of the Best Inventions of 2025. Phase 3 trials begin in 2026. Commercial launch projected for 2027–2029 pending FDA approval.
Q7: What happens if I stop taking finasteride or minoxidil?
Hair loss resumes — typically within 3–12 months — and can return to the point it would have reached without any treatment. Both medications require indefinite use to maintain results.
Q8: Which Norwood stage is too late for medication?
Norwood Stages 1–4 offer the best pharmacological response. Stages 5–7 can still benefit from halting further progression, but significant regrowth becomes unlikely without hair transplant surgery.
Q9: Is a receding hairline genetic?
Genetics account for approximately 80% of susceptibility to androgenetic alopecia. Sons of bald fathers are 5–6 times more likely to develop a receding hairline — but the gene can be inherited from either parent.
Q10: Does oral minoxidil work better than topical for the hairline?
Oral minoxidil distributes systemically, potentially reaching the frontal hairline more effectively than topical applications. The 2025 meta-analysis of 2,933 patients confirmed strong efficacy across alopecia types, making it an increasingly preferred option.
Q11: Do lifestyle changes actually slow a receding hairline?
Yes — significantly. Quitting smoking, correcting iron and Vitamin D deficiencies, managing chronic stress, optimizing sleep, and avoiding traction hairstyles all reduce the rate of follicle miniaturization alongside medical treatment.
Last reviewed: February 2026 | Expert panel: mymedicineadvisor.com | For personalized guidance, consult a board-certified dermatologist. This article is for educational purposes only.
Explore more evidence-based guides: Balding Treatment 2026 | Hair Loss Treatments 2026 | Is Hair Loss Reversible?
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.