On This Page – Quick Medical Summary
⚡ Quick Answer: Melasma is a chronic skin condition causing dark, symmetrical patches on the face triggered by UV exposure, hormonal changes, and genetics. It affects up to 50% of high-risk populations. While no permanent cure exists, consistent combination therapy — topical agents, sun protection, and in some cases oral medications — can significantly fade and control it.
Dark patches appearing on your cheeks, forehead, or upper lip — seemingly out of nowhere — can be alarming. For millions of Americans, especially women between 20 and 40, those patches have a name: melasma.
Priya, a 33-year-old nurse from Chicago, noticed symmetrical brown patches spreading across both cheekbones three months after starting oral contraceptives. Her dermatologist confirmed melasma in under five minutes — yet she had spent months buying expensive creams that made no difference.
That gap between what patients know and what actually works is exactly what this guide closes.
What Is Melasma? The Skin Condition Affecting Millions
Melasma is a common, acquired hyperpigmentation disorder in which overactive melanocytes — the pigment-producing cells in your skin — release excess melanin, creating blotchy, darkened patches. It is not a rash, infection, or sign of cancer.
According to StatPearls via the National Institutes of Health (NIH), melasma affects approximately 1% of the global general population, rising to 9–50% in higher-risk groups — particularly women with darker skin tones in sun-exposed regions.
In the United States alone, an estimated 5–6 million people are affected, with women accounting for 90% of cases.
What Does Melasma Actually Look Like?
Melasma presents as bilateral, symmetrical patches — meaning it appears on both sides of the face in a mirrored pattern. The patches are typically flat, not raised, and painless.
Most commonly affected areas include:
- Cheeks (malar pattern — most common)
- Forehead and nose bridge (centrofacial pattern)
- Jawline (mandibular pattern)
- Upper lip
- Less commonly: forearms, neck, shoulders (sun-exposed skin only)
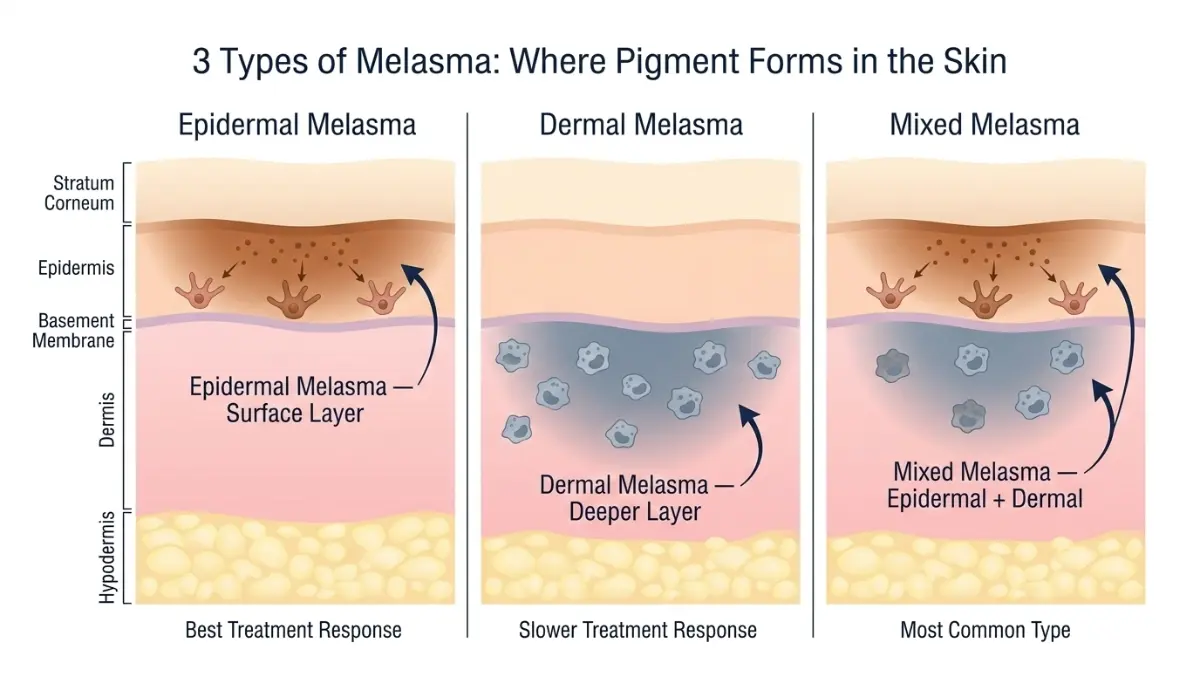
The 3 Types of Melasma Explained
Melasma is classified by how deeply the pigment penetrates the skin. This classification directly affects how it responds to treatment.
| Type | Skin Layer Affected | Colour Appearance | Treatment Response |
|---|---|---|---|
| Epidermal | Surface (epidermis) | Dark brown, well-defined borders | Best — responds well to topicals |
| Dermal | Deeper (dermis) | Blue-grey, blurry borders | Slower, may need procedures |
| Mixed | Both layers | Brown + grey combined | Requires combination approach |
Key Takeaway: Mixed melasma is the most common type. Most people need a combination of treatments — not just a single cream — because both skin layers are involved.
If you’re unsure whether your skin patches are melasma or another condition, use our Symptom Checker to identify possible causes and get guidance on next steps.
What Causes Melasma — And Why It Keeps Getting Worse
This is where competitors fail you completely. Understanding why melasma spreads is the key to stopping it.
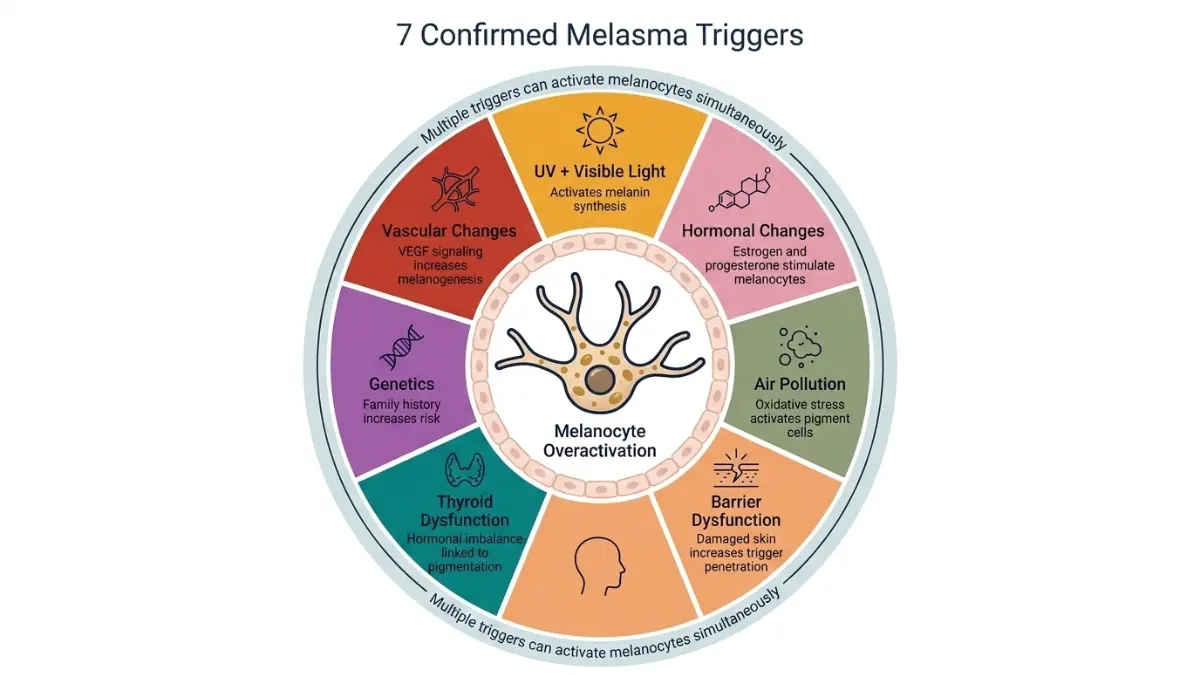
In 2025, dermatologist Dr. Mukta Sachdev presented the most comprehensive framework to date at the American Academy of Dermatology Annual Meeting, identifying seven distinct etiological pathways behind melasma development. No competitor covers this.
The 7 Confirmed Triggers of Melasma
1. UV and Visible Light Exposure UV radiation stimulates melanocytes to overproduce melanin. But here’s what most sunscreen labels won’t tell you: standard SPF sunscreens block UVA and UVB, but NOT visible light (400–700nm), which is a confirmed melanocyte trigger. This is why melasma can persist or worsen even in people who wear sunscreen religiously.
2. Hormonal Changes Estrogen and progesterone stimulate melanin synthesis. This explains why melasma surges during:
- Pregnancy (nicknamed “the mask of pregnancy”)
- Oral contraceptive use
- Hormone replacement therapy (HRT)
- Perimenopause
3. Genetic Predisposition Approximately 50% of melasma patients report a positive family history, according to NIH data. Identical twins have both been documented developing melasma under similar conditions.
4. Pollution — The Hidden Trigger Nobody Talks About This is a 2025 finding completely absent from Healthline, WebMD, and Mayo Clinic. Research presented at the AAD 2025 Annual Meeting confirmed that geographic areas with heavy air pollution show dramatically higher melasma incidence. Pollutant particles penetrate skin and trigger oxidative stress in melanocytes. Cleansers targeting pollution particles are now considered adjunct prevention tools.
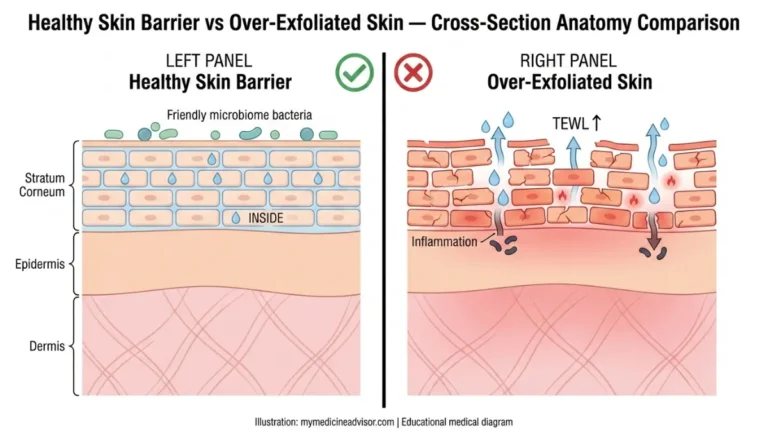
5. Barrier Dysfunction A compromised skin barrier allows greater UV penetration, inflammatory signals, and irritant exposure — all of which activate melanocytes. Harsh scrubs, chemical-heavy products, and over-exfoliation worsen melasma for this reason.
6. Thyroid Disease A frequently missed clinical link: elevated thyroid-stimulating hormone (TSH) and thyroid peroxidase antibodies are significantly more common in melasma patients. A 2025 meta-analysis confirmed this association. If you have melasma alongside fatigue, weight changes, or cold sensitivity, thyroid screening is clinically advisable. Our TSH test guide explains thyroid result interpretation in detail.
7. Vascular and Microbiome Changes Increased dermal blood vessel density and elevated vascular endothelial growth factor (VEGF) are consistently found in melasma skin — meaning blood vessel changes actively promote pigment production, not just UV damage alone.
Why Hormones Are the #1 Culprit in American Women
In the US, the hormonal trigger dominates. Between 15–50% of pregnant women develop melasma, with onset most common in the second and third trimesters. Women tracking hormonal cycles who notice face pigmentation changes can use our Ovulation Calculator to identify hormonal patterns linked to melasma flares.
Key Takeaway: Your melasma is almost certainly triggered by more than one factor simultaneously. Treating only one trigger — like using SPF but ignoring visible light — explains why so many treatments partially work but never fully clear the condition.
Melasma vs. Hyperpigmentation — How to Tell the Difference
This is the #1 People Also Ask question on Google — and no competitor answers it with a proper structured comparison.
Direct Comparison Table
| Feature | Melasma | Post-Inflammatory Hyperpigmentation (PIH) | Age Spots (Lentigines) | Freckles |
|---|---|---|---|---|
| Pattern | Symmetrical, bilateral | Asymmetrical, localized | Scattered, individual spots | Scattered, small |
| Primary trigger | Hormones + UV | Injury, acne, eczema | UV exposure only | Genetic |
| Typical location | Cheeks, forehead, upper lip | Where inflammation occurred | Hands, face | Face, shoulders |
| Fades in winter? | Partially | Sometimes | Rarely | Yes |
| Responds to topicals? | Yes (slowly) | Yes (faster) | Partially | N/A |
| Skin type most affected | Darker tones (Fitzpatrick III–VI) | Any skin type | Fairer skin tones | Fairer skin tones |
How Dermatologists Diagnose Melasma
A dermatologist typically diagnoses melasma using:
- Visual examination — symmetrical pattern is diagnostic in most cases
- Wood’s lamp — UV light device showing depth of pigment penetration
- Dermoscopy — magnified skin surface examination
- Skin biopsy — rarely needed; used to rule out other conditions
What This Means For You: If your dark patches are asymmetrical, appeared after a pimple or rash, or don’t match the bilateral pattern — it may be PIH, not melasma. The distinction matters because treatment protocols differ significantly.
If your skin changes concern you, this guide on skin cancer signs and warning symptoms can help you identify when to seek urgent dermatological evaluation.
How to Treat Melasma — The 2026 Dermatologist-Approved Guide
This is the section every competitor gets wrong. They list treatments without ranking evidence, explaining mechanisms, or differentiating by skin type.
The 2026 consensus from the American Academy of Dermatology (AAD) is clear: melasma requires multimodal combination therapy. Monotherapy — one cream, one procedure — consistently underdelivers.
Step 1: The Non-Negotiable Foundation — Sun Protection
No treatment works without this step. Every day. Rain or shine.
- SPF 50+ broad-spectrum sunscreen — mandatory baseline
- Iron oxide-containing tinted sunscreen — essential for blocking visible light (400–700nm), the trigger that standard SPF misses entirely
- Wide-brimmed hat — physical barrier reduces UV load significantly
- Avoid peak sun hours — 10 AM to 4 PM in the US
Sunscreens with zinc oxide and iron oxide offer the most comprehensive protection for melasma patients with darker skin tones.
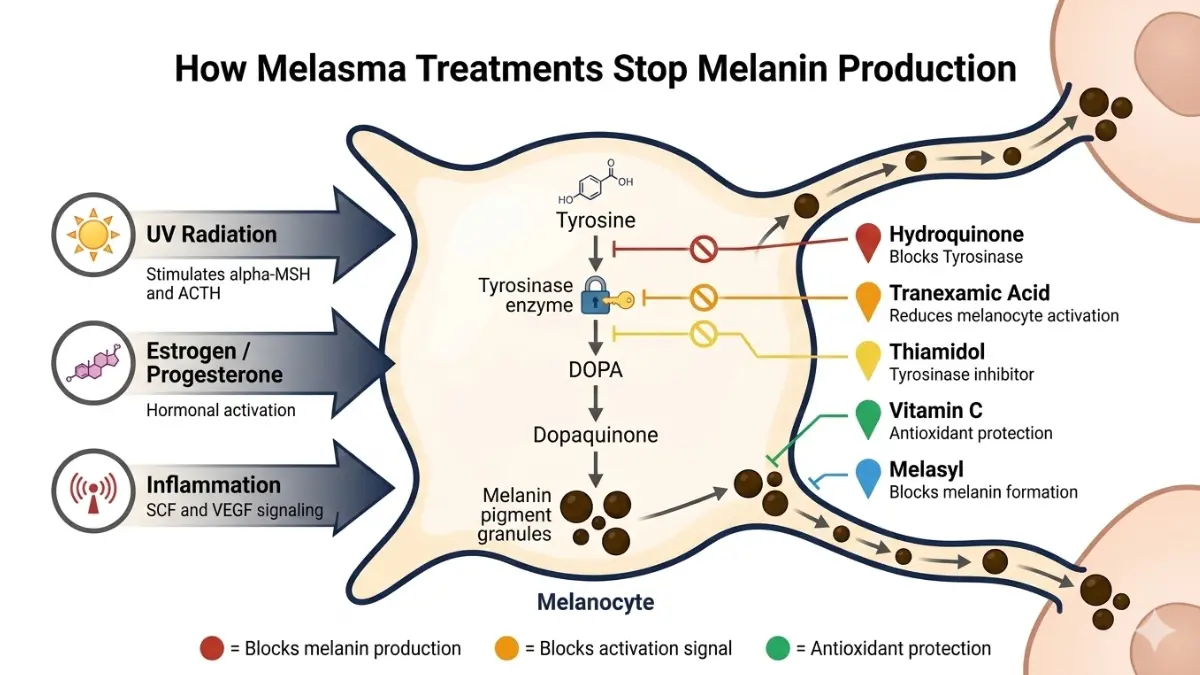
Step 2: Topical Treatments — Ranked by Clinical Evidence
| Treatment Agent | Mechanism | Evidence Level (2026) |
|---|---|---|
| Triple Combination Cream (hydroquinone + tretinoin + corticosteroid) | Multi-pathway depigmentation | ⭐⭐⭐⭐⭐ Strongest topical |
| Hydroquinone 4% | Tyrosinase enzyme inhibition | ⭐⭐⭐⭐⭐ Gold standard |
| Tranexamic Acid (topical) | Blocks UV-induced plasminogen → melanocyte activation | ⭐⭐⭐⭐ Strong — 2024–2025 RCT confirmed |
| Thiamidol | Next-generation tyrosinase inhibitor | ⭐⭐⭐⭐ Multiple 2023–2025 RCTs with strong MASI reduction |
| Azelaic Acid 15–20% | Anti-inflammatory + tyrosinase block | ⭐⭐⭐ Good safety profile, pregnancy-compatible |
| Vitamin C (ascorbic acid) | Antioxidant; tyrosinase suppression | ⭐⭐⭐ Best as maintenance agent |
| Melasyl (emerging 2025–2026) | Melanin polymerization inhibitor | ⭐⭐ Early clinical trials; promising combination data |
| Kojic Acid | Tyrosinase inhibition | ⭐⭐ Moderate evidence; often used adjunctively |
Important: Hydroquinone is no longer available over-the-counter in the US — a prescription is required. Do not use OTC “skin lightening” products with unregulated concentrations.
For those using prescription topicals, our Pill Identifier tool can help verify medications prescribed alongside your topical regimen.
Step 3: Oral Treatments (2025–2026 Evidence Update)
Oral Tranexamic Acid (TXA) is the most significant advance in melasma treatment in the past decade. A 2025 network meta-analysis published via PubMed/NIH comparing 15 different melasma treatments found TXA among the most effective combination options.
- Dosing studied: 250mg twice daily (most common protocol in RCTs)
- Mechanism: Inhibits the UV-induced plasminogen pathway that triggers melanocyte activation
- Results: Significant MASI (Melasma Area Severity Index) reduction in 12-week studies
- Requires: Dermatologist prescription and monitoring
Polypodium leucotomos — an oral fern extract — provides internal photoprotection and is used as a sun-protective adjunct in several US dermatology practices.
Step 4: In-Clinic Procedures
| Procedure | Best For | Caution |
|---|---|---|
| Chemical Peels (glycolic, lactic, Jessner’s) | Epidermal melasma | Avoid aggressive peels in Fitzpatrick IV–VI |
| Microneedling | Enhances topical penetration | Not standalone; combine with topicals |
| Pixel Er:YAG Laser | Epidermal type; strongest laser MASI reduction | Risk of post-inflammatory hyperpigmentation in dark skin |
| Q-Switched Nd:YAG (low fluence) | Asian and darker skin populations | Requires expert operator |
| PRP (Platelet-Rich Plasma) | Adjunct for resistant cases | Emerging; combine with TXA for best results |
Interested in how microneedling and laser treatments compare in real-world outcomes? Our in-depth microneedling guide and CO₂ laser treatment guide provide detailed procedure breakdowns.
Melasma Treatment for Darker Skin — Special Considerations
This is the most underserved guidance gap across every competitor.
The 2025 AAD consensus specifically states that Fitzpatrick skin types IV–VI require a modified treatment approach to avoid triggering post-inflammatory hyperpigmentation (PIH) — which can make melasma significantly worse.
For darker skin patients, dermatologists recommend:
- Triple combination cream as preferred first-line topical
- Oral tranexamic acid — systemically effective without skin surface trauma
- Microneedling — lower injury risk than ablative lasers
- Avoid: aggressive chemical peels, ablative laser as first-line treatment
- Use: tinted SPF 50+ with iron oxide — non-negotiable for this group
Key Takeaway: The 2026 AAD consensus confirms combination therapy outperforms any monotherapy for melasma — regardless of skin type. If one treatment hasn’t worked, the protocol, not the effort, likely needs updating.
Can Melasma Be Cured Permanently? Managing It Long-Term
The honest answer most medical sites avoid: no, melasma cannot be permanently cured in the conventional sense. But that doesn’t mean you’re stuck with it.
Dr. Mukta Sachdev of the AAD 2025 panel put it plainly: “Treat melasma like thyroid dysfunction — it’s a chronic condition that needs constant, ongoing management.”
Why Melasma Keeps Coming Back
Melasma recurs because:
- The dermal (deeper) component is not fully eliminated by most treatments
- The underlying triggers — UV exposure, hormones, pollution — continue to exist
- Melanocytes in previously affected areas remain “primed” and reactive
- Any sun exposure can reactivate pigmentation in treated areas
The Maintenance Protocol That Works
After achieving fading with active treatment, dermatologists recommend a long-term maintenance routine:
- Daily SPF 50+ iron-oxide sunscreen — no exceptions, including indoor days near windows
- Low-dose topical maintenance — rotating vitamin C in the morning, low-concentration retinoid at night
- Trigger management — reassess hormonal contraceptive use with your OB-GYN if melasma is severe
- Anti-pollution cleansers — now considered an evidence-based adjunct (2025 AAD update)
- Regular dermatology check-ins — every 3–6 months during active management
The Psychosocial Impact Competitors Never Acknowledge
A 2026 peer-reviewed study in Clinical, Cosmetic and Investigational Dermatology confirmed that melasma significantly impairs quality of life — particularly in the domains of emotional well-being, appearance confidence, and social interaction. This is not vanity. It is a clinically documented psychological burden.
If melasma is affecting your confidence or mental health, discussing this directly with your dermatologist opens access to more aggressive treatment pathways — and in some states, may influence insurance coverage considerations.
Poor sleep can elevate cortisol, which in turn activates stress-mediated melanocyte pathways. Use our Sleep Calculator to assess whether your rest patterns may be contributing to hormonal skin fluctuations.
When to See a Dermatologist Immediately
Schedule an appointment if:
- Patches appear suddenly or rapidly expand
- Pigmentation is asymmetrical or has irregular borders
- Patches have changed in texture or colour
- Over-the-counter treatments have shown zero improvement after 12 weeks
- Melasma appears alongside new systemic symptoms (fatigue, weight change, hair loss)
Melasma in Pregnancy and in Men — Two Groups Competitors Ignore
Melasma During Pregnancy (Chloasma)
Pregnancy-related melasma — clinically called chloasma — is one of the most common dermatological changes in pregnancy, affecting 15–50% of pregnant women in the US, according to NIH StatPearls.
It typically appears during the second or third trimester, coinciding with peak estrogen and progesterone surges. The good news: for many women, it partially or fully resolves within 3–6 months postpartum.
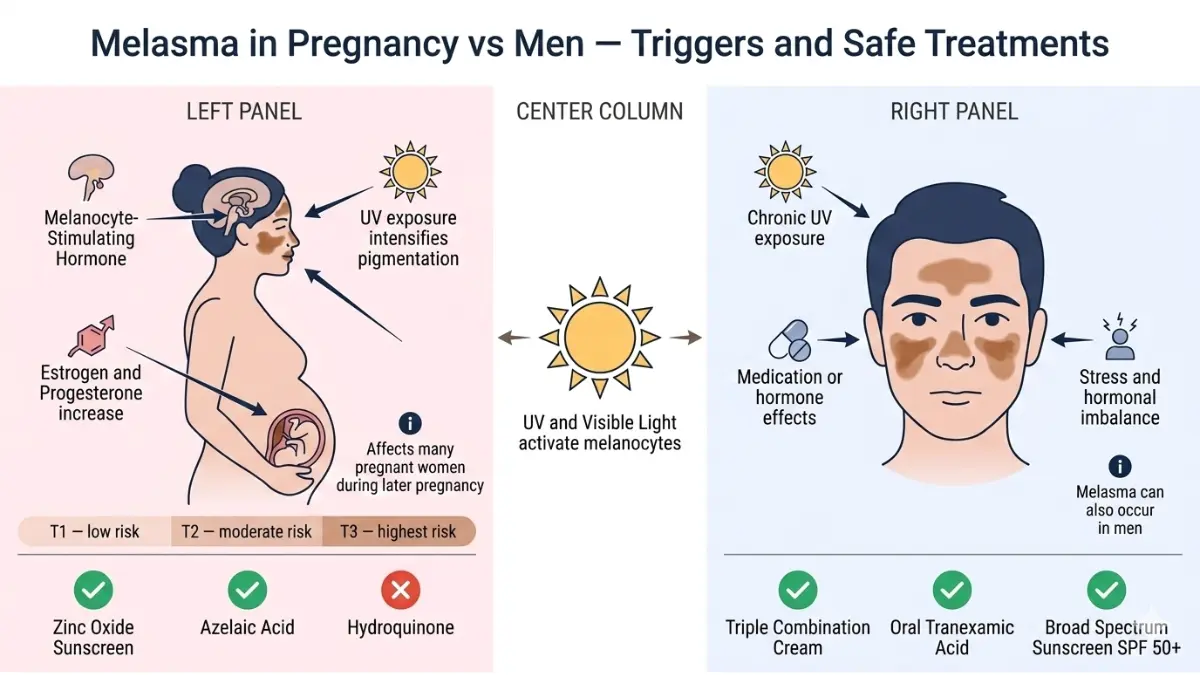
Safe management during pregnancy:
- Physical sunscreens only — zinc oxide and titanium dioxide are pregnancy-safe
- Avoid hydroquinone during pregnancy — insufficient safety data exists
- Azelaic acid — considered safe in pregnancy with physician guidance
- Gentle cleansing — avoid harsh exfoliants that compromise barrier function
- Hats and shade — non-pharmacological sun avoidance is your most powerful tool
If you’re monitoring your pregnancy timeline and noticing skin changes, our Pregnancy Due Date Calculator and Pregnancy Weight Gain Calculator can help you track key milestones while managing hormonal health holistically.
If melasma persists beyond 6 months postpartum, it has transitioned from chloasma to chronic melasma and requires active dermatological treatment.
Melasma in Men — More Common Than You Think
Approximately 10% of all melasma cases occur in men — a figure that remains dramatically underdiagnosed because men are far less likely to seek dermatological care for cosmetic skin concerns.
Key differences in male melasma:
- Trigger profile differs — sun exposure is the dominant trigger, not hormones
- Finasteride link — men using finasteride for hair loss have shown increased melasma incidence in emerging case reports (2024–2025)
- Location — typically centrofacial and malar, same as in women
- Treatment response — same principles apply; oral tranexamic acid and triple combination cream are effective
What This Means For You (Men): If you have dark facial patches and use finasteride or spend significant time outdoors, discuss melasma screening with your dermatologist. Early intervention produces significantly better outcomes than treating established, widespread pigmentation.
Men exploring hair loss treatments — some of which may influence melasma risk — can find evidence-based information in our DHT blocker guide and minoxidil treatment overview.
Most-Asked Questions About Melasma
1. What is melasma?
Melasma is a chronic skin condition causing symmetrical dark patches on the face due to excess melanin from overactive melanocytes, triggered by UV, hormones, and genetics.
2. Does melasma go away on its own?
Sometimes — pregnancy-related melasma often fades within months postpartum. But persistent melasma requires active treatment to fade effectively.
3. Is melasma dangerous or a sign of cancer?
No. Melasma is benign and not a cancer risk. However, rapidly changing or asymmetrical pigmentation should always be evaluated by a dermatologist.
4. What triggers melasma to spread?
UV and visible light exposure, hormonal changes, air pollution, stress, barrier damage, thyroid dysfunction, and certain medications can all worsen melasma.
5. Can melasma be cured permanently?
No permanent cure currently exists. However, consistent combination therapy with ongoing sun protection can maintain long-term remission effectively.
6. What is the best treatment for melasma in 2026?
The AAD 2026 consensus recommends triple combination cream (hydroquinone + tretinoin + corticosteroid) alongside SPF 50+ iron-oxide sunscreen as the strongest evidence-based starting protocol.
7. Is there a link between melasma and thyroid disease?
Yes. Research confirms elevated TSH and thyroid peroxidase antibodies are significantly more common in melasma patients. Thyroid screening is clinically recommended for persistent cases.
8. Can men get melasma?
Yes — men account for approximately 10% of cases, predominantly triggered by chronic sun exposure rather than hormones. Finasteride use may also be a contributing factor.
9. What sunscreen is best for melasma?
SPF 50+ tinted sunscreen containing iron oxide is the clinical recommendation — it blocks both UV and visible light, which standard SPF sunscreens do not adequately address.
10. How long does melasma treatment take to show results?
Most topical treatments show measurable fading within 8–12 weeks of daily consistent use. Oral tranexamic acid may show improvement from week 4 onward.
11. Does stress worsen melasma?
Yes. Elevated cortisol from chronic stress activates melanocyte-stimulating pathways. Stress management, adequate sleep, and hormonal regulation are all part of a comprehensive melasma management plan.
⚠️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. Melasma is a YMYL (Your Money or Your Life) health condition. Always consult a board-certified dermatologist for diagnosis and individualized treatment planning.
For more health guides, visit mymedicineadvisor.com/health/
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.