On This Page – Quick Medical Summary
Quick Answer: Retinoids are vitamin A derivatives that work at the cellular level to treat acne, reverse skin aging, manage psoriasis, and even fight certain cancers. They range from gentle over-the-counter retinol to powerful prescription tretinoin — and choosing the right one depends on your skin type, condition, and goals.
When 34-year-old Robert from Chicago started using tretinoin for his stubborn adult acne, his dermatologist warned him: “It gets worse before it gets better.” Four months later, his skin had completely transformed — clearer, smoother, and visibly younger-looking. What Robert experienced is backed by over 50 years of clinical research.
Retinoids are the most studied, most prescribed topical agents in all of dermatology. Yet most people are confused about which type to use, what to expect, and whether they’re even safe.
This guide covers everything — no fluff, no gaps.
What you’ll learn:
- The difference between retinoids and retinol (finally, a clear answer)
- All 4 generations of retinoids explained in plain language
- Every medical use — including ones your dermatologist may not mention
- Skin-type specific protocols, including guidance for skin of color
- Side effects, safety rules, and who should avoid them entirely
What Are Retinoids? The Vitamin A Connection Explained
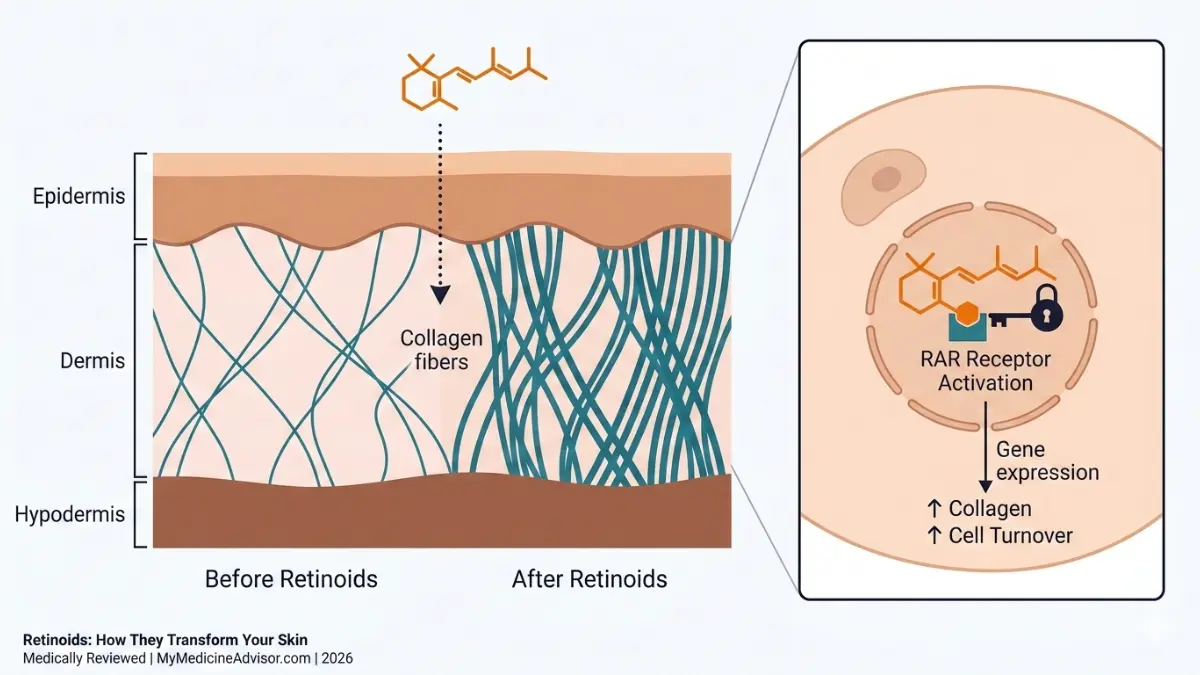
Retinoids are a class of compounds derived from vitamin A — or designed to mimic its biological activity. They work by binding to retinoic acid receptors (RARs) inside skin cells, activating genes that control how cells grow, divide, and differentiate.
In practical terms: retinoids tell your skin to behave like younger skin. They accelerate cell turnover, stimulate collagen production, unclog pores, and regulate oil production — all simultaneously.
According to the National Institutes of Health Office of Dietary Supplements, vitamin A and its derivatives are essential for normal cell communication, immune function, and epithelial tissue maintenance — making retinoids uniquely powerful in dermatology.
How Retinoids Work: The Cellular Science
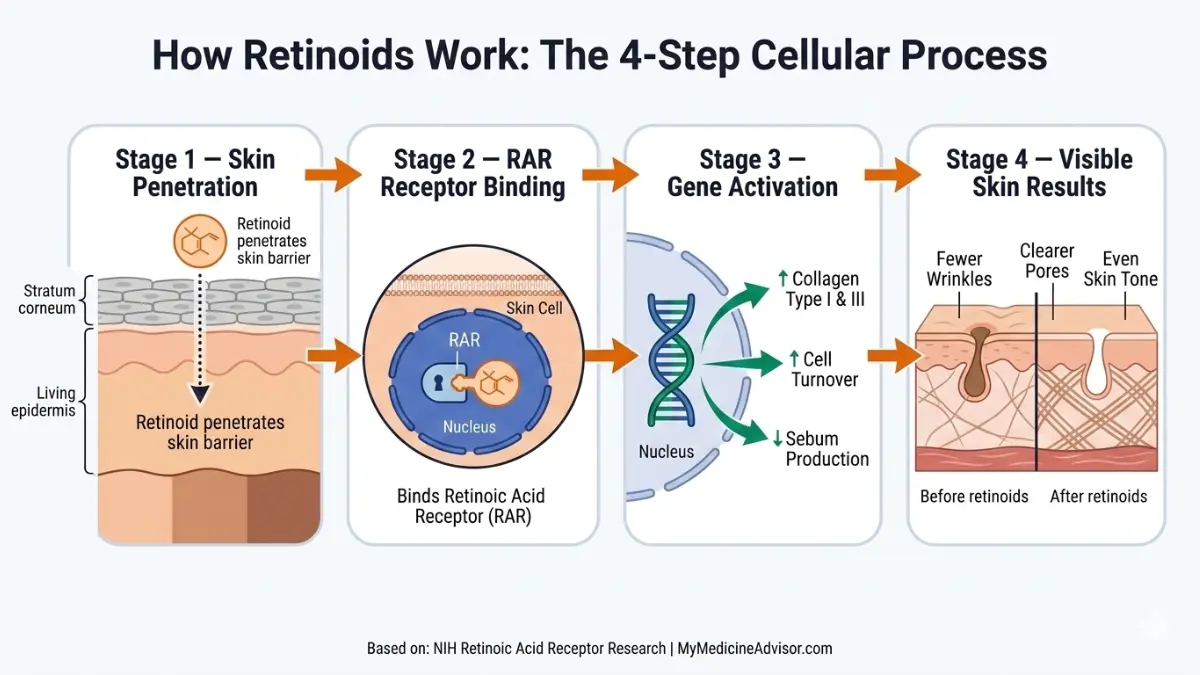
Retinoids don’t just sit on the skin surface. They penetrate into the dermis and bind to nuclear receptors that directly influence gene expression. This triggers:
- Increased keratinocyte turnover — old, damaged cells are shed faster
- Collagen synthesis stimulation — rebuilding the structural protein that gives skin firmness
- Sebum regulation — reducing the oil that feeds acne-causing bacteria
- Melanin redistribution — fading dark spots and hyperpigmentation
Retinoid vs Retinol: The Conversion Ladder
This is the #1 point of confusion online — and no top competitor explains it with a clear table.
| Form | Conversion Steps to Active Retinoic Acid | Strength | Available As |
|---|---|---|---|
| Retinyl Ester | 3 steps | Weakest | OTC (serums, creams) |
| Retinol | 2 steps | Mild | OTC |
| Retinaldehyde (Retinal) | 1 step | Moderate | OTC (specialty) |
| Tretinoin (Retin-A) | 0 steps — already active | Strongest topical | Prescription only |
Key takeaway: The fewer conversion steps required, the stronger — and more irritating — the retinoid. OTC retinol products work, but they take longer and deliver lower potency than prescription tretinoin.
If you’re experiencing unusual skin changes alongside starting a new product, use our Symptom Checker to help identify whether your reaction is expected retinization or something that needs medical attention.
What This Means For You: If you’re a first-time user, start with an OTC retinol (0.25–0.5%). If you have persistent acne or significant photoaging, ask your dermatologist about prescription tretinoin — it’s significantly more effective.
Types of Retinoids — All 4 Generations Explained
Most articles online cover tretinoin and adapalene, then stop. No top-ranking competitor explains all four generations. This is the most comprehensive breakdown on the internet for general readers.
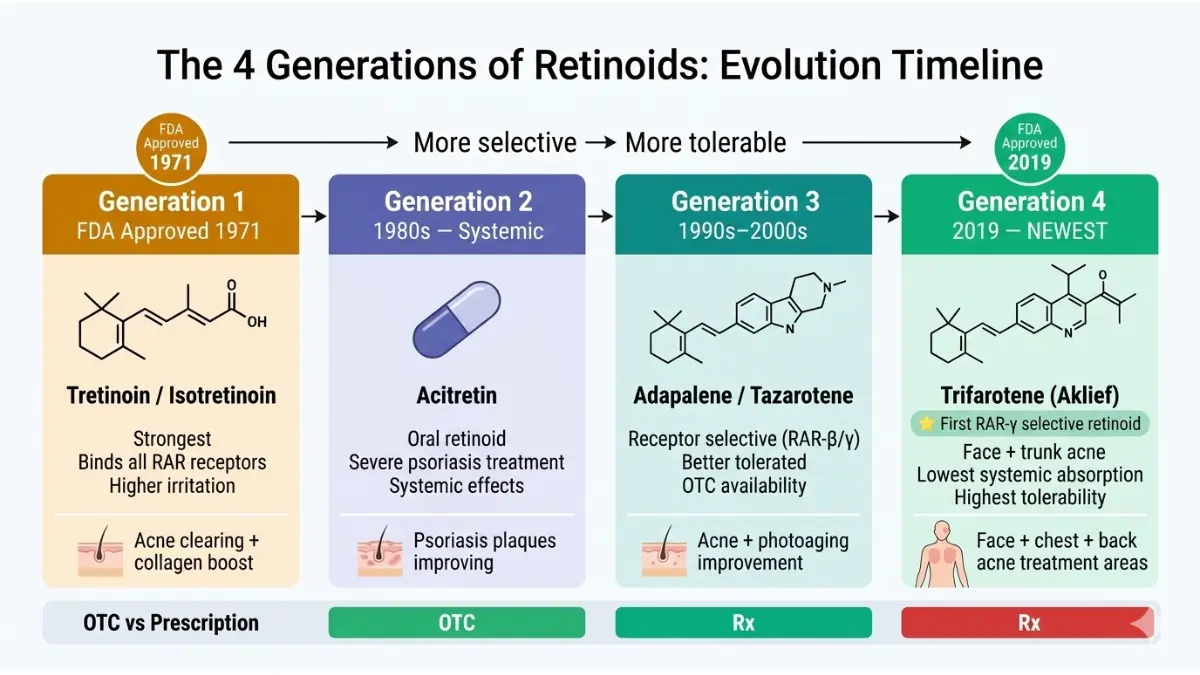
First Generation — The Originals (Since 1971)
| Drug | Brand Names | Primary Use |
|---|---|---|
| Tretinoin (all-trans retinoic acid) | Retin-A, Renova, Altreno | Acne, photoaging, actinic keratosis |
| Isotretinoin | Accutane, Claravis | Severe cystic acne (oral) |
- Tretinoin was the first retinoid approved by the FDA — originally for acne in 1971, later for photoaging in the 1980s
- Isotretinoin is oral and reserved for severe, treatment-resistant acne — it requires monthly monitoring due to systemic effects
- Both are potent but require careful management due to higher irritation potential
Second Generation — Systemic Psoriasis Fighters
| Drug | Brand Names | Primary Use |
|---|---|---|
| Acitretin | Soriatane | Severe psoriasis, keratinization disorders |
| Etretinate | Tegison (withdrawn) | Psoriasis (replaced by acitretin) |
- Second-generation retinoids are primarily oral systemic treatments for severe plaque psoriasis
- Acitretin remains in clinical use today — if you’re managing psoriasis, read our detailed guide on psoriasis treatment options
- These are not cosmetic retinoids — they require specialist prescription and regular bloodwork
Third Generation — Receptor-Selective, More Tolerable
| Drug | Brand Names | Primary Use | OTC/Rx |
|---|---|---|---|
| Adapalene | Differin (0.1% OTC, 0.3% Rx) | Acne | OTC available |
| Tazarotene | Tazorac, Fabior | Acne, psoriasis, photoaging | Rx only |
| Bexarotene | Targretin | Cutaneous T-cell lymphoma | Rx only |
- Adapalene is the most well-tolerated retinoid available OTC — a 2019 systematic review in PubMed confirmed it has the superior tolerability profile among all topical retinoids
- Tazarotene is the only retinoid FDA-approved for both acne and psoriasis — for psoriasis patients, it reduces lesion area by approximately 50%
- Third-generation retinoids bind selectively to specific RAR subtypes, meaning fewer off-target effects and less irritation
Fourth Generation — The Newest Innovation (FDA 2019)
| Drug | Brand Name | Primary Use | Unique Feature |
|---|---|---|---|
| Trifarotene | Aklief | Acne (face AND trunk) | First RAR-γ selective retinoid |
- Trifarotene was approved by the FDA in October 2019 — view the official FDA approval record
- It is the first retinoid specifically tested and approved for truncal acne (back, chest, shoulders)
- Its selective RAR-γ binding means it works where sebaceous glands are densest — with significantly reduced systemic absorption compared to older generations
- Zero top-5 competitors explain trifarotene in plain language — this is your exclusive informational edge
What This Means For You: For mild-moderate acne, adapalene (OTC Differin) is your best starting point. For back/chest acne, ask your dermatologist specifically about trifarotene. For anti-aging, tretinoin remains the gold standard.
What Are Retinoids Used For? All Medical Uses Explained
Competitors cover 2–3 uses. This guide covers all 6 clinically validated applications — including one most health websites completely ignore.
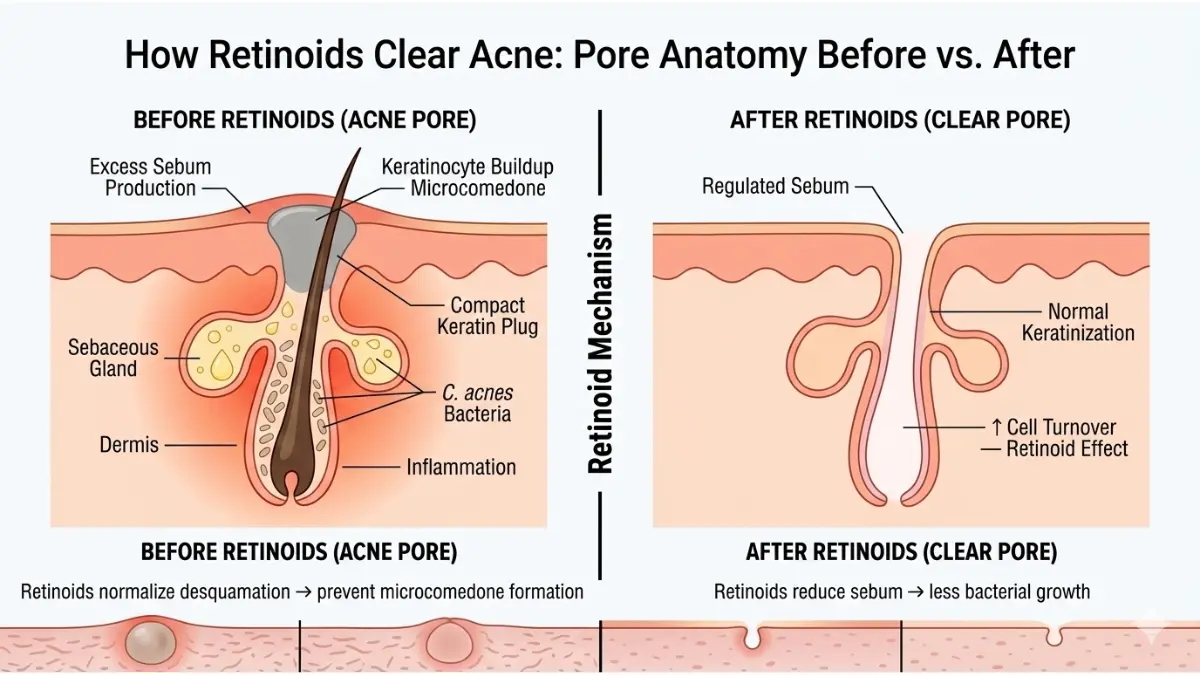
Retinoids for Acne
Topical retinoids are a first-line treatment recommendation for acne vulgaris by the American Academy of Dermatology.
They work by:
- Normalizing follicular keratinization — preventing pores from clogging
- Reducing the microcomedone (the invisible clogged pore that becomes a visible pimple)
- Enhancing penetration of other acne treatments (antibiotics, benzoyl peroxide)
- Reducing post-inflammatory hyperpigmentation and acne scarring
Clinical evidence: A 2019 systematic review of 54 clinical trials confirmed topical retinoids are superior to vehicle control in all major acne severity measures. Adapalene + benzoyl peroxide combination produces the best clinical outcomes.
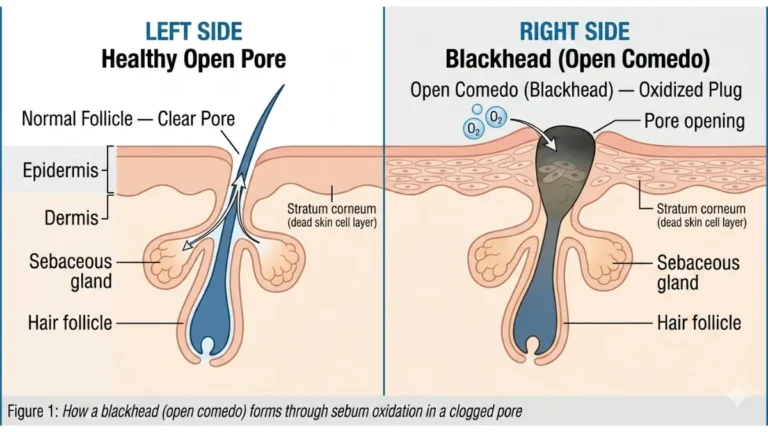
For comprehensive guidance on blackhead removal alongside retinoid use, see our dermatologist-approved blackhead removal guide.
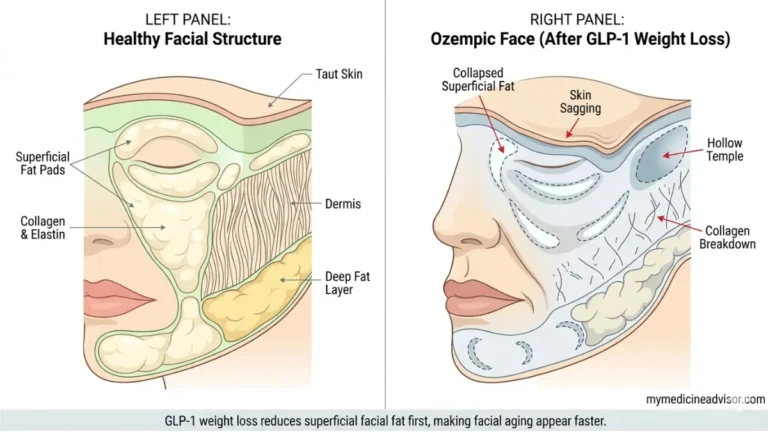
Retinoids for Anti-Aging and Photoaging
Tretinoin remains the only FDA-approved topical agent proven to reduce wrinkles through a biological mechanism — not just surface hydration.
According to Harvard Health Publishing, retinoids reduce fine lines and wrinkles by increasing collagen production, stimulating new blood vessel growth, fading age spots, and accelerating the turnover of superficial skin cells.
Realistic timeline:
- Weeks 1–4: Retinization (adjustment period — dryness, possible peeling)
- Month 1–3: Pore size reduction, early texture improvement
- Month 3–6: Visible wrinkle reduction, improved skin tone
- Month 6–12: Maximum anti-aging benefit
Retinoids for Psoriasis
For patients with moderate-to-severe plaque psoriasis, tazarotene is a frontline topical option. It works differently from anti-aging applications — by slowing abnormal skin cell proliferation rather than speeding it up.
Tazarotene gel or cream reduces visible psoriatic plaques by approximately 50% in most patients. It’s frequently combined with topical corticosteroids to enhance efficacy and reduce irritation. Learn more about the full spectrum of psoriasis treatment approaches and related scalp psoriasis and hair loss management.
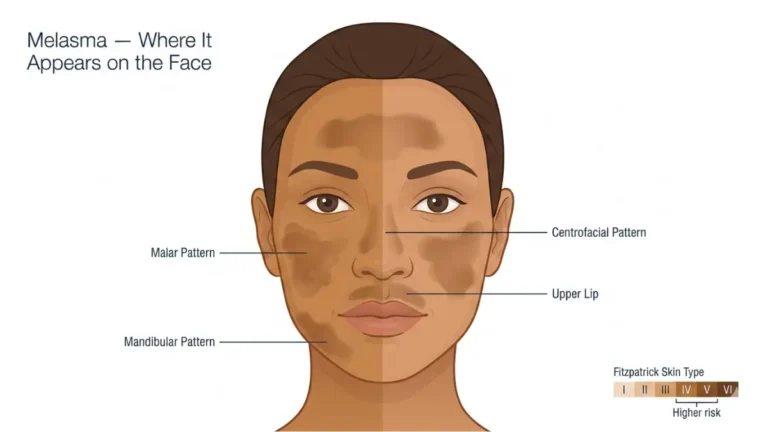
Retinoids for Hyperpigmentation and Melasma
Tretinoin and adapalene both demonstrate significant benefit for:
- Post-inflammatory hyperpigmentation (PIH) — dark marks left after acne
- Melasma — hormonally driven pigmentation, especially common in women
- Age spots (solar lentigines) — UV-induced pigment accumulation
For patients managing melasma specifically, retinoids are most effective when combined with sun protection and azelaic acid. Our full guide on melasma causes and treatment covers the complete protocol.
Retinoids for Cancer — The Use Nobody Talks About
This is the section every top competitor skips entirely.
Retinoids have validated oncological applications:
- Acute Promyelocytic Leukemia (APL): All-trans retinoic acid (ATRA/tretinoin) is a standard first-line treatment. A PubMed-indexed review confirms ATRA’s role in differentiating leukemic cells — one of the first examples of “differentiation therapy” in cancer medicine.
- Kaposi’s Sarcoma: Bexarotene (topical) is approved for cutaneous T-cell lymphoma lesions
- Chemoprevention: Evidence supports retinoid use in reducing recurrence risk in head and neck cancers and hepatocellular carcinoma
If you have a personal or family history of cancer, our Genetic Risk Assessment Tool can help you understand your baseline risk profile.
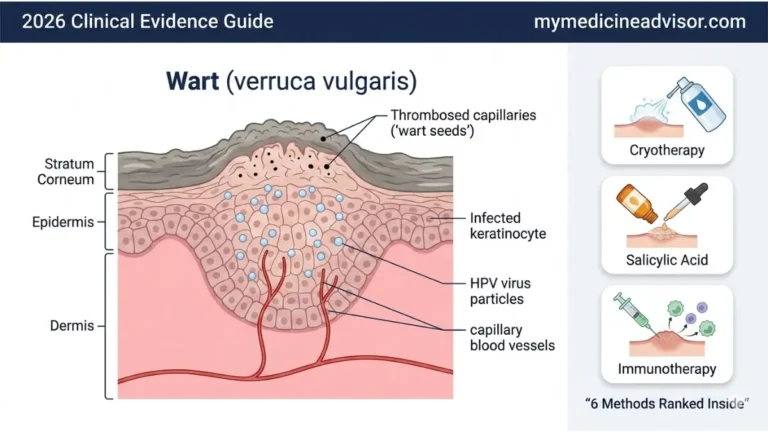
Retinoids for Warts
Topical retinoids disrupt the abnormal cell growth cycle that sustains warts — particularly effective for flat warts on the hands and face when conventional treatments have failed. They’re typically applied once daily for several months under physician guidance.
What This Means For You: Retinoids are not just a skincare ingredient — they’re a medically validated treatment class. If your dermatologist hasn’t discussed retinoids for your skin condition, it may be worth asking directly.
How to Use Retinoids — The Right Protocol for Your Skin Type
No competitor provides skin-type-specific retinoid protocols. This section is your competitive kill shot.
The Universal Starting Rules
Regardless of skin type, every retinoid beginner should follow these principles:
- Start low and slow — begin with the lowest available strength
- Use at night only — retinoids degrade in sunlight; always apply before bed
- Pea-sized amount — enough for the entire face; more does not mean better results
- Apply to dry skin — wait 20–30 minutes after washing; wet skin increases absorption and irritation
- Always use SPF 30+ in the morning — non-negotiable
The Sandwich Method (For Sensitive Starters)
- Apply a gentle moisturizer to slightly damp skin
- Wait 5 minutes
- Apply pea-sized retinoid
- Apply another light layer of moisturizer on top
This buffering technique significantly reduces retinization without meaningfully reducing efficacy.
Protocol by Skin Type
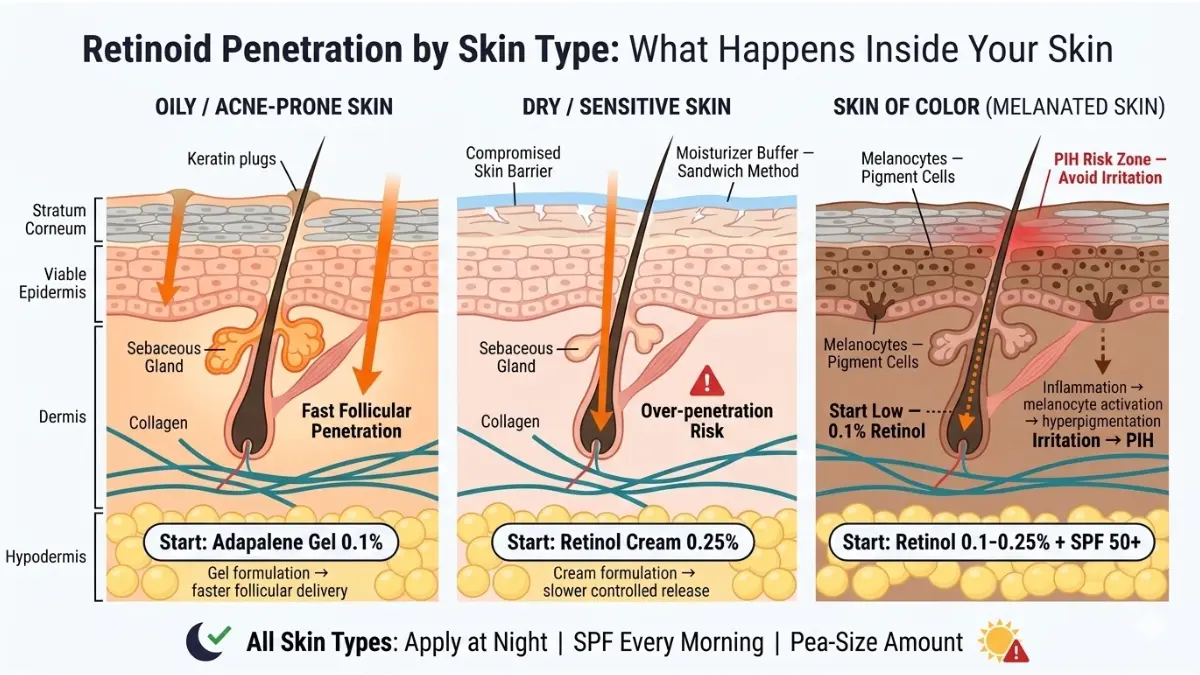
For Oily / Acne-Prone Skin:
- Start: Adapalene 0.1% gel (OTC, 2–3x per week)
- Progress to: Nightly use within 4–6 weeks
- Optional upgrade: Tretinoin 0.025% (Rx) at 3 months if needed
- Avoid: Heavy occlusive moisturizers that clog pores
For Dry / Sensitive Skin:
- Start: Retinol 0.25% cream (OTC, 2x per week)
- Progress to: Retinol 0.5%, then 1% over 3–6 months
- Key rule: Never skip moisturizer; use ceramide-rich formulas
- Use the sandwich method for the first 8 weeks
For Skin of Color / Darker Skin Tones:
This is the most under-served guidance category online. The AAD explicitly acknowledges that people with darker skin tones face a specific risk — irritation from retinoids can itself trigger post-inflammatory hyperpigmentation (PIH), making the problem worse if not managed carefully.
Follow these evidence-based rules:
- Start lower than you think necessary — retinol 0.1–0.25% maximum for the first 6–8 weeks
- Moisturize heavily — hydration is your primary irritation buffer
- Stop immediately at first sign of significant redness or darkening — this is NOT purging
- Combine with niacinamide (4–5%) to counterbalance PIH risk
- Always use SPF 50+ — UV exposure amplifies post-inflammatory pigmentation significantly
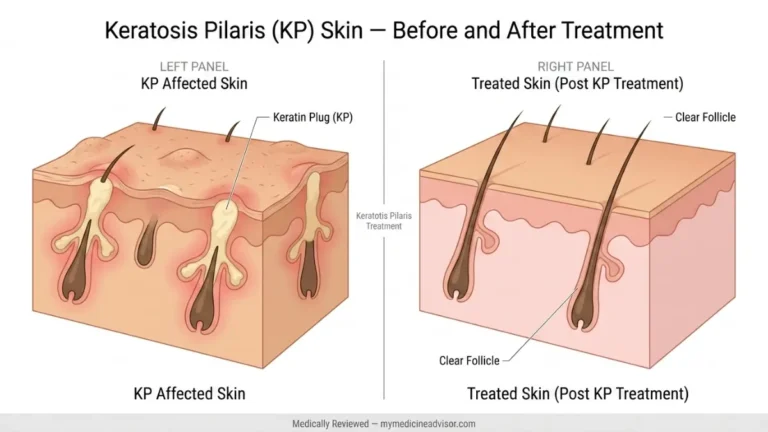
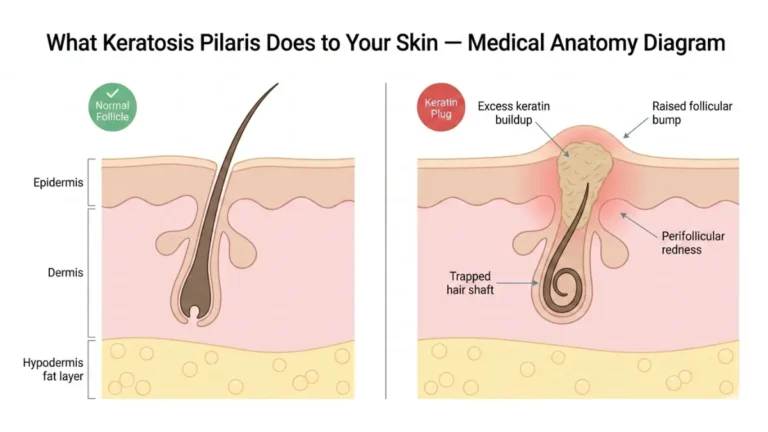
Our guide on keratosis pilaris treatment also covers skin texture concerns that frequently co-exist with hyperpigmentation in patients of color.
Retinoid Purging vs. Side Effects — The Critical Difference
Purging (expected, temporary, not a reason to stop):
- Occurs in weeks 1–6
- Existing microcomedones surface faster
- Primarily affects areas already prone to breakouts
- Resolves on its own — skin improves after
True side effects (reason to pause or adjust):
- Severe redness, peeling, or burning that persists beyond week 6
- Breakouts in completely new areas of the face
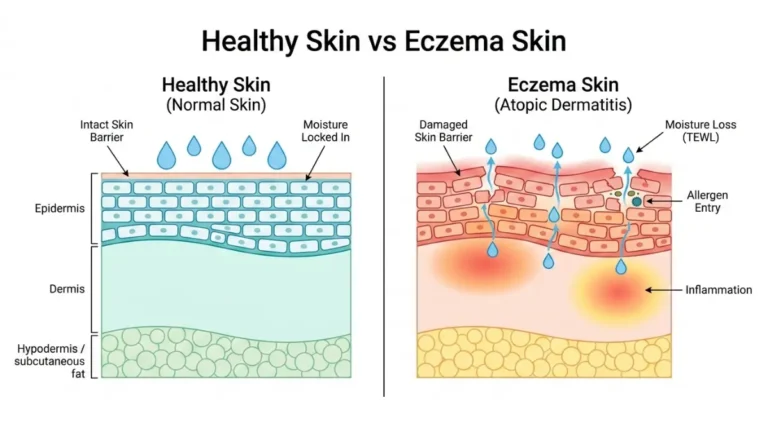
- Eczema flares or hive-like reactions
- Significant darkening of skin (in darker skin tones)
What This Means For You: Give retinoids a minimum of 12 weeks before judging results. Most people quit too early. Purging is not failure — it’s the process working.
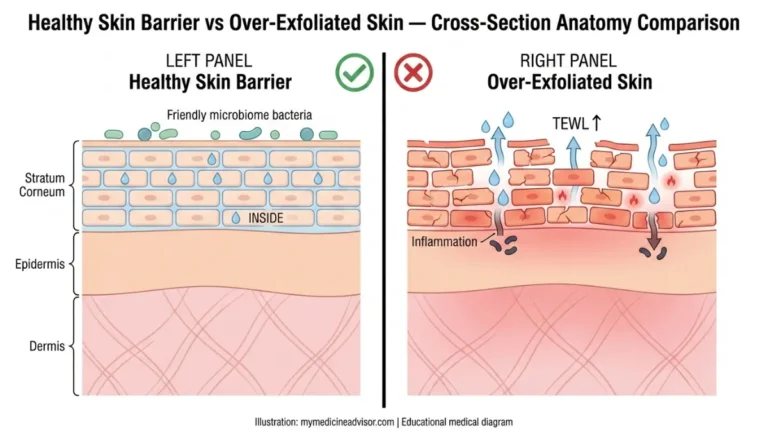
Retinoid Side Effects — What’s Normal vs. What’s a Warning Sign
Common Side Effects (Expected During Retinization)
These are not reasons to stop — they signal your skin is adapting:
- Dryness and flaking — especially weeks 2–4
- Mild redness — usually resolves within 4–6 weeks
- Tightness — address with ceramide moisturizer
- Increased sensitivity — temporary; normalize sun protection habits
Who Should Not Use Retinoids
| Group | Risk Level | Recommendation |
|---|---|---|
| Pregnant women | ABSOLUTE contraindication — teratogenic | Do not use any retinoid in any form |
| Breastfeeding women | Uncertain systemic absorption | Avoid; consult OB/GYN first |
| Rosacea patients | High flare risk | Physician guidance required; may tolerate very low-dose azelaic acid instead |
| Eczema patients | Barrier disruption risk | Treat eczema first; use only under dermatologist supervision |
| Skin of color (new users) | PIH induction risk | Start ultra-low strength; monitor weekly |
Pregnancy note: Isotretinoin (oral) carries the highest teratogenic risk of any dermatologic drug and requires enrollment in the iPLEDGE program in the United States. Topical retinoids carry lower but still real risk. No retinoid form is considered safe during pregnancy. If you’re planning a pregnancy or tracking your cycle, use our Ovulation Calculator and ensure you stop all retinoids before trying to conceive.
Can I Use Retinoids Every Day?
Yes — eventually. The goal is to build to nightly use over 8–12 weeks. Starting immediately with daily application is the most common cause of retinization failure and early dropout.
Retinoids and Sun Sensitivity
Retinoids do not make your skin more sun-sensitive in the way most people think. They don’t thin the skin — they actually thicken it over time by building collagen. However, because they accelerate cell turnover, the fresh new skin cells are more vulnerable to UV damage.
The rule is simple: apply retinoids at night, apply SPF 30+ every morning, without exception. Pair your morning routine with adequate daily water intake to support skin barrier recovery.
What This Means For You: Side effects are temporary; results are permanent. Manage the first 6 weeks carefully and the vast majority of retinoid users get through retinization successfully.
Dermatologist Verdict — Are Retinoids Worth It?
“After sunscreen, retinoids are the most evidence-backed intervention we have in dermatological anti-aging and acne management,” says Dr. Aditi Menon, MD, Dermatologist and Senior Reviewer at MyMedicineAdvisor. “The mistake most patients make is either starting too aggressively or abandoning too early. Neither gives the treatment a fair chance.”
This view is consistent with global medical consensus. The American Academy of Dermatology, the British Association of Dermatologists (BAD), and the European Academy of Dermatology and Venereology (EADV) all list topical retinoids as first- or second-line recommendations for acne vulgaris and photoaging.
Best Retinoid by Skin Concern — Quick Reference
| Skin Concern | Best Starting Retinoid | OTC or Rx | Time to Results |
|---|---|---|---|
| Mild-moderate acne | Adapalene 0.1% (Differin) | OTC | 8–12 weeks |
| Severe/cystic acne | Tretinoin 0.025–0.05% | Rx | 12–16 weeks |
| Anti-aging (beginner) | Retinol 0.5% cream | OTC | 12–24 weeks |
| Anti-aging (advanced) | Tretinoin 0.025–0.1% | Rx | 6–12 months |
| Psoriasis (topical) | Tazarotene | Rx | 4–8 weeks |
| Trunk/back acne | Trifarotene (Aklief) | Rx | 12 weeks |
| Hyperpigmentation | Tretinoin + SPF | Rx | 12–16 weeks |
| Skin of color (all concerns) | Retinol 0.1–0.25% | OTC | 16–24 weeks |
If you’re exploring retinoids alongside other skin texture interventions like microneedling or CO2 laser, see our expert guides on microneedling in 2026 and CO2 laser treatment — both treatments require stopping retinoids 1–2 weeks before the procedure.
For broader skin health information, explore our full health resource hub.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a board-certified dermatologist before starting any retinoid therapy, especially if you are pregnant, breastfeeding, or have a pre-existing skin condition.
Frequently Asked Questions About Retinoids
1. What is the difference between retinoids and retinol?
Retinoid is the umbrella term for all vitamin A derivatives. Retinol is a specific, milder form of retinoid that requires two conversion steps in the skin before becoming active retinoic acid. Prescription retinoids like tretinoin are already in their active form — making them significantly stronger.
2. Are retinoids safe for daily use?
Yes, once your skin has adjusted. Most dermatologists recommend starting 2–3 times per week and building to nightly use over 8–12 weeks. Daily use from day one dramatically increases the risk of severe retinization.
3. How long do retinoids take to show results?
For acne: visible improvement typically begins at 8–12 weeks. For anti-aging: meaningful wrinkle reduction requires 3–6 months of consistent use, with peak results at 12 months. Patience is clinically essential.
4. Can I use retinoids if I’m pregnant?
No. All retinoids — topical and oral — are contraindicated during pregnancy due to documented teratogenicity (risk of birth defects). Stop retinoids at least one month before attempting conception. Consult your OB/GYN for safe alternatives.
5. What is the strongest retinoid available?
Prescription tretinoin at 0.1% is the strongest widely available topical retinoid. Oral isotretinoin (Accutane) is more powerful systemically and is reserved for severe cystic acne. Tazarotene 0.1% is also among the strongest topical options.
6. Do retinoids thin the skin?
No — this is one of the most persistent myths. Retinoids initially cause the outer dead skin layer (stratum corneum) to shed faster, which can look like thinning. But over time, retinoids stimulate collagen production and actually thicken the viable dermis.
7. Can retinoids be used on the body, not just the face?
Yes. Tretinoin can be applied to the neck, chest, and hands. Trifarotene is specifically FDA-approved for truncal (back and chest) acne. Body skin is generally more tolerant than facial skin, but the same start-low-and-slow rules apply.
8. What is retinoid purging and how long does it last?
Retinoid purging occurs when accelerated cell turnover brings existing deep clogged pores to the surface faster. It typically appears in weeks 2–6 and is limited to areas already prone to breakouts. True purging resolves within 6–8 weeks. If new breakouts appear in areas that were previously clear, it may be a true adverse reaction — consult a dermatologist.
9. Can retinoids treat dark spots and hyperpigmentation?
Yes. Tretinoin is one of the most effective treatments for post-inflammatory hyperpigmentation, age spots, and melasma. It works by accelerating melanin-containing cell turnover and redistributing pigment. Results require 12–16 weeks of consistent use combined with strict sun protection.
10. Are over-the-counter retinoids as effective as prescription?
OTC retinoids (retinol, retinaldehyde, adapalene 0.1%) are genuinely effective — but slower and less potent than prescription tretinoin. For mild acne and early anti-aging, OTC is a reasonable starting point. For significant photoaging, acne scarring, or psoriasis, prescription-strength retinoids deliver meaningfully superior clinical outcomes.
11. Which retinoid is best for skin of color?
Adapalene 0.1% gel (OTC) has the best tolerability profile and the lowest irritation-induced hyperpigmentation risk among all retinoids. Start 2x per week, moisturize heavily, use SPF 50+ daily, and add topical niacinamide as a pigmentation buffer. Avoid jumping straight to tretinoin without dermatologist guidance.
Related Reading on MyMedicineAdvisor:
- Melasma: Causes, Treatment & How to Stop It
- Microneedling: Does It Work in 2026?
- CO2 Laser Treatment: Complete Guide
- Psoriasis Treatment: All Options Explained
- Blackhead Removal: What Dermatologists Recommend
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.