On This Page – Quick Medical Summary
Cellulite is a structural skin condition — not a fat problem — in which fibrous connective bands pull skin downward while subcutaneous fat pushes upward, creating the dimpled, orange-peel texture most women know all too well. It affects up to 98% of post-pubertal women worldwide, according to a 2026 peer-reviewed review published in the journal Cosmetics (MDPI). And yet, most online guides still treat it as a simple weight issue.
It isn’t. Here’s what science actually confirms.
What Is Cellulite? The Answer Most Sites Get Wrong
The Medical Definition — Plain Language
Mia, a 31-year-old marathon runner in Chicago, was frustrated. She was lean, active, and eating clean — but cellulite still appeared on her thighs after her second pregnancy. Her doctor had a simple explanation most websites never give: cellulite is anatomical, not cosmetic negligence.
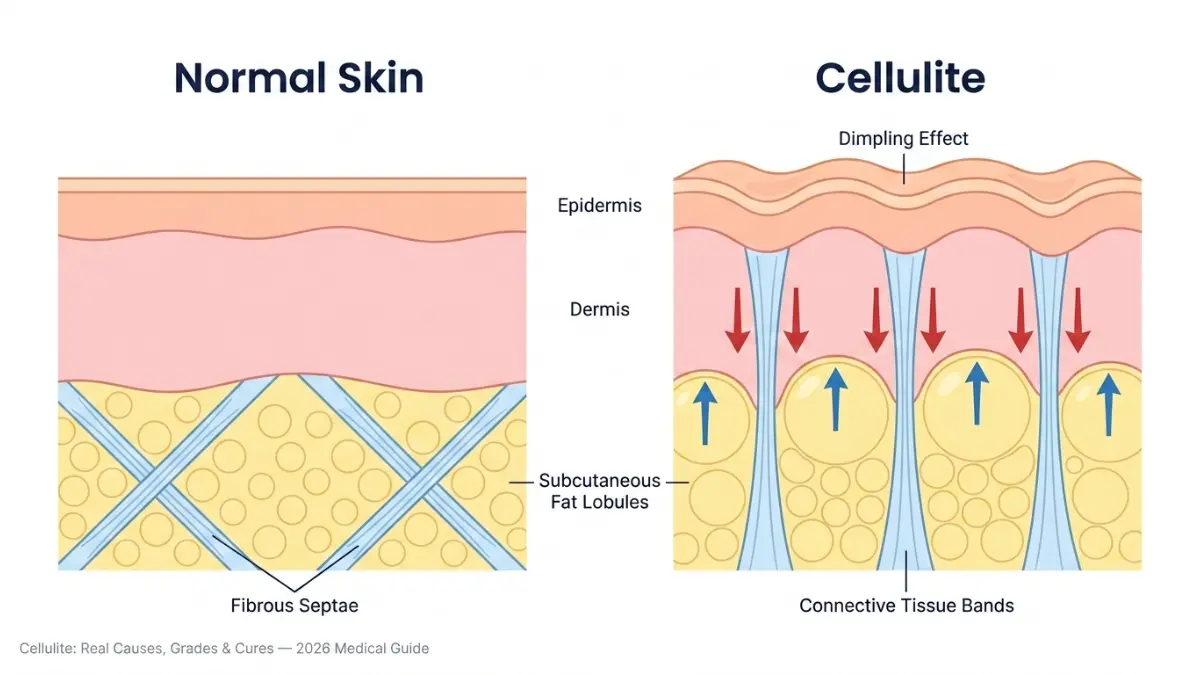
Medically known as gynoid lipodystrophy, cellulite occurs when subcutaneous fat lobules herniate through weakened connective tissue, creating the signature dimpled texture. It has nothing to do with how much you weigh or how hard you exercise.
Three things happening simultaneously under your skin:
- Fat cells enlarge and push upward against the dermis
- Fibrous bands called septae tighten, harden, and pull the skin downward
- Skin loses elasticity with age, making the underlying structure more visible
Why Healthy, Thin Women Get Cellulite Too
This is the question Healthline’s 2018 article answers poorly — and where your content wins.
| Myth | Medical Reality |
|---|---|
| “Cellulite means you’re overweight” | Even women with a healthy BMI and low body fat have cellulite — it’s structural |
| “Exercise can eliminate cellulite” | Exercise reduces its appearance but cannot remove the fibrous band architecture |
| “Cellulite means poor health” | It is a normal anatomical variation, not a disease |
To get a clearer picture of where you stand, using our Body Fat Calculator can help you understand your body composition in context — because cellulite appearance does relate to body fat percentage, even if it isn’t caused by it alone.
Key takeaway: Cellulite is anatomical — not a personal health failure.
Real Causes of Cellulite — What’s Actually Happening Under Your Skin
The Fibrous Septae Architecture: The Root Cause
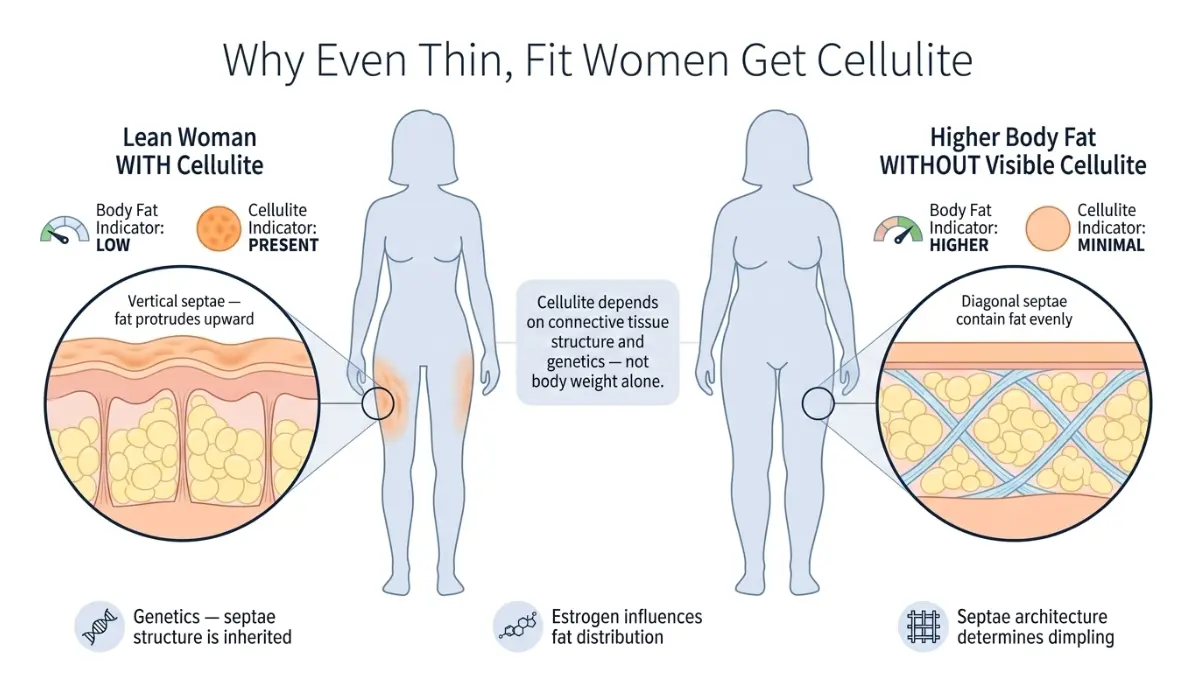
The most important piece of biology most articles skip is why women get cellulite far more than men. A landmark 2020 review by Bass and Kaminer — published in Dermatologic Surgery through PubMed Central (NIH) — established that the number and orientation of fibrous septae is the primary driver of cellulite pathophysiology.
Think of it like this: in women, the connective tissue strands run vertically, straight up like fence posts — so fat bulges through the gaps easily. In men, those same strands run at a 45-degree criss-cross angle, holding fat firmly in place. This structural gender difference explains why over 90% of cellulite cases occur in women, regardless of body type.
Estrogen’s Role — Why Cellulite Peaks During Pregnancy and Menopause
Estrogen directly influences fat distribution, collagen production, and skin elasticity. When estrogen levels shift — during puberty, pregnancy, or menopause — the connective tissue weakens faster, fat redistribution accelerates, and the dimpling worsens. This is why cellulite often appears or worsens after having a baby, as many American women in their 30s and 40s report.
Women using our Pregnancy Weight Gain Calculator during or after pregnancy may notice cellulite-related questions — understanding the hormonal driver helps frame realistic expectations.
The 3-Factor Risk Matrix: Genetics, Age, Lifestyle
| Risk Factor | How It Contributes |
|---|---|
| Genetics | Determines septae density, skin thickness, and fat cell distribution — the biggest single factor |
| Age | Collagen loss thins the dermis; the structural irregularity beneath becomes more visible |
| Body Fat % | Higher fat volume increases pressure against weakened septae |
| Sedentary Lifestyle | Reduces blood flow and lymphatic drainage, worsening fluid retention |
| High-Sodium Diet | Promotes tissue fluid retention, amplifying the dimpled appearance |
| Poor Circulation | Blood flow in cellulite-affected areas is up to 35% lower than non-affected areas |
What this means for you: Targeting only fat loss may not improve your cellulite — because the septae structure is still there. Effective treatment requires addressing the connective tissue directly.
Cellulite Grades 1–4 — Which Stage Are You, and What Should You Do?
Most women don’t know there is a clinical grading system for cellulite severity — and your grade directly determines which treatments will actually work. No top competitor explains this with actionable guidance. Here it is.
The Nürnberger-Müller Scale + Cellulite Severity Scale (CSS)
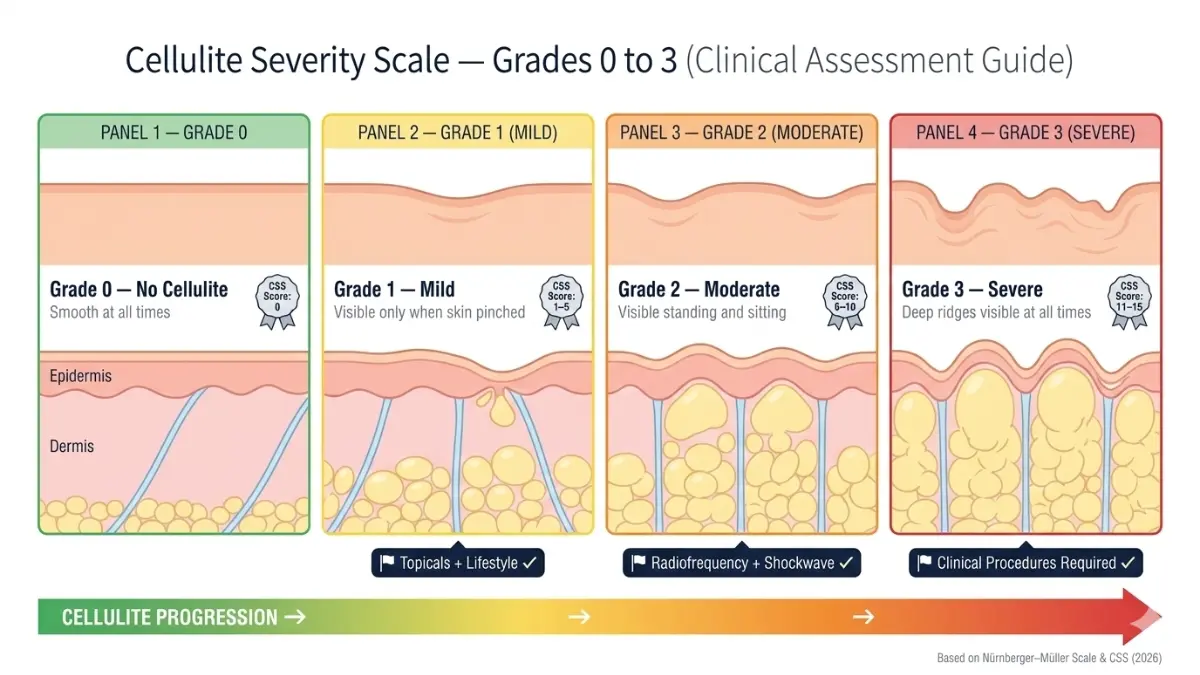
Dermatologists use two established scales to assess cellulite. The most widely used in 2026 clinical trials is the Cellulite Severity Scale (CSS), which evaluates the number and depth of dimples on a 0–15 point range.
| Grade | Clinical Description | When It Appears | What You Should Do |
|---|---|---|---|
| Grade 0 | Smooth skin; no dimpling even when pinched | Never | Prevention: exercise, hydration, collagen nutrition |
| Grade 1 (Mild) | Dimpling visible only when skin is pinched | Not visible standing | Topicals (retinol 0.3%), lifestyle changes, dry brushing as adjunct |
| Grade 2 (Moderate) | Orange-peel texture visible while standing AND sitting | Always present | Radiofrequency therapy + structured exercise + retinol |
| Grade 3 (Severe) | Deep dimples, raised ridges, skin draped over bumps | Prominent at all times | Clinical procedures: subcision, collagenase injections, SWT |
How Dermatologists Assess Your Grade
A board-certified dermatologist will assess your cellulite visually and by palpation (touch), using the CSS scale during a clinical consultation. Per the American Academy of Dermatology (AAD), the skill and experience of the treating physician is a critical factor in both assessment and outcome.
Key takeaway: Grade 1 responds well to lifestyle changes and topicals. Grade 3 requires clinical intervention to see meaningful improvement. Skipping this assessment means wasting money on the wrong treatment tier.
If you’re uncertain about your overall health metrics, our BMI Calculator and Weight Loss Calculator can help contextualize how body composition factors into your grade progression.
Cellulite Treatments Ranked by Evidence — What Doctors Actually Confirm in 2026
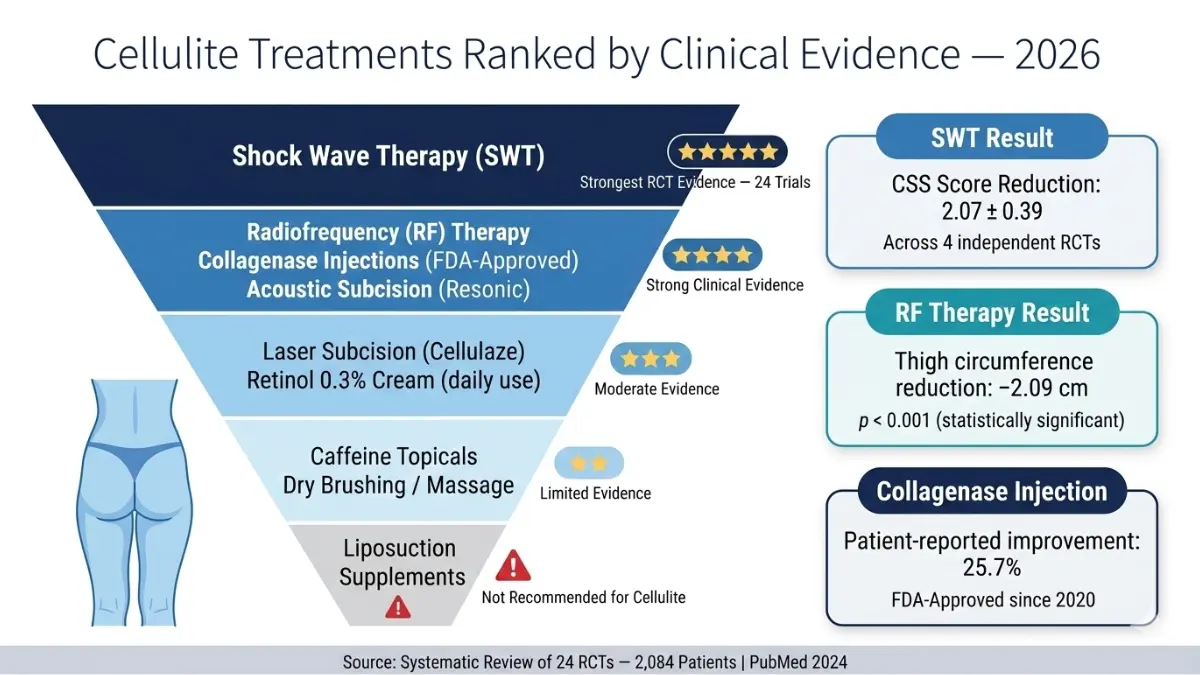
With over 50 cellulite treatments marketed globally, most women waste hundreds — sometimes thousands — on options with zero clinical backing. What follows is the most evidence-ranked treatment comparison available, based on a 2024 systematic review of 24 randomized controlled trials published in PubMed covering 2,084 patients.
Master Evidence Table: Cellulite Treatments Ranked
| Treatment | Evidence Strength | Best For Grade | Result Duration | 2026 Status |
|---|---|---|---|---|
| Shock Wave Therapy (SWT) | ⭐⭐⭐⭐⭐ Strongest RCT data | Grade 2–3 | 6–12 months | First-line clinical recommendation |
| Radiofrequency (RF) | ⭐⭐⭐⭐ Strong | Grade 2–3 | 6 months | Non-invasive clinical standard |
| Collagenase Injections (CCH-aaes) | ⭐⭐⭐⭐ Strong | Grade 2–3 | 12+ months | FDA-approved since 2020 |
| Acoustic Subcision (Resonic) | ⭐⭐⭐⭐ Strong, emerging | Grade 3 | 52+ weeks | Single-session FDA-cleared device |
| Laser Subcision (Cellulaze) | ⭐⭐⭐ Moderate | Grade 2–3 | 6–12 months | Minimally invasive option |
| Retinol Cream (0.3%) | ⭐⭐⭐ Moderate | Grade 1–2 | Temporary (daily use) | Daily maintenance adjunct |
| Caffeine Topicals | ⭐⭐ Limited | Grade 1 | Days only | Circulation aid, not a cure |
| Dry Brushing / Manual Massage | ⭐ Minimal | Grade 1 | Temporary | Lymphatic aid only |
| Liposuction | ⚠️ Not recommended | All | May worsen appearance | Avoid for cellulite-specific treatment |
Shock Wave Therapy (SWT) — The 2026 First-Line Treatment
Shock wave therapy uses acoustic pressure waves to break down hardened fibrous septae and stimulate collagen remodeling. In the 2024 systematic RCT review, SWT demonstrated a consistent cellulite reduction score of 2.07 ± 0.39 across four independent studies — the strongest reproducible result of any non-invasive treatment.
What you need to know:
- Typically 6–12 sessions, spaced weekly
- Performed in a dermatologist or cosmetic clinic setting
- Average cost in the US: $300–$600 per session
- No downtime; mild redness for a few hours post-treatment
- Best results on thighs and buttocks, Grade 2–3
Radiofrequency (RF) — The Non-Invasive Workhorse
RF therapy delivers controlled heat into the subcutaneous tissue, targeting both fat cells and fibrous septae while stimulating collagen production. The same 2024 RCT review found that RF produced a statistically significant reduction in thigh circumference of −2.09 cm (p < 0.001) and subcutaneous tissue thickness of −2.23 cm.
Key facts:
- 4–8 sessions typically required
- Results visible at 6 weeks; peak effect at 3–6 months
- Excellent safety profile; suitable for most skin types
- Often combined with SWT for synergistic results
- Cost: $200–$500 per session in the US
For readers who also want to understand how skin treatments like this interact with broader body-composition goals, our related guide on Morpheus8 — a radiofrequency microneedling device — gives doctors’ honest 2026 assessment.
Collagenase Injections (CCH-aaes / Qwo) — The Injectable That Targets Septae
The FDA approved collagenase clostridium histolyticum-aaes (CCH-aaes) in 2020 as the first injectable specifically for moderate-to-severe cellulite on the buttocks. The mechanism: two bacterial collagenase enzymes (AUX-I and AUX-II) directly hydrolyze the collagen-rich fibrous septae causing the dimpling.
In two Phase 3 randomized placebo-controlled trials, patients reported a 25.7% improvement on patient-reported photonumeric scales (p < 0.001). Results lasted 12 months or longer in most participants.
What to know before considering it:
- 3 treatment sessions, 21 days apart
- Significant bruising is common (especially in the buttocks)
- Suitable for Grade 2–3 cellulite
- Cost: $2,000–$3,500 for a full treatment course in the US
- Consult only with a board-certified dermatologist or plastic surgeon
Acoustic Subcision (Resonic) — The 2026 Single-Session Option
In a multicenter trial of 42 women with severe cellulite, 95.2% had their post-treatment photos correctly identified as improved, and 100% reported improved cellulite appearance at 52-week follow-up — after just a single treatment session. Published in PubMed Central (PMC), this is among the most promising single-session outcomes in recent cellulite research.
The device (Resonic by Allergan Aesthetics) uses rapid acoustic pulses to non-invasively shear the fibrous septae — no anesthesia required.
What About Home Remedies? The Honest Verdict
| Home Approach | Does It Work? | The Evidence |
|---|---|---|
| Retinol 0.3% cream (daily, 6 months) | Modestly — Grade 1 | Thickens dermis; reduces appearance temporarily |
| Caffeine topicals | Marginally | Diuretic effect; very temporary circulation boost |
| Dry brushing | Minimal | Improves surface circulation; does not affect septae |
| Supplements | No | No peer-reviewed evidence supports any supplement for cellulite |
What this means for you: Home remedies can complement clinical treatments for Grade 1. For Grade 2 or 3, they are not sufficient alone. Start with a dermatologist consultation.
The Evidence-Based Lifestyle Protocol to Reduce Cellulite at Home
While no lifestyle change eliminates cellulite permanently, a targeted, consistent protocol can significantly reduce Grade 1 and Grade 2 appearance within 8–12 weeks — and improve your foundation before or after clinical treatment.
Exercise — The Right Moves (Not Just Any Cardio)
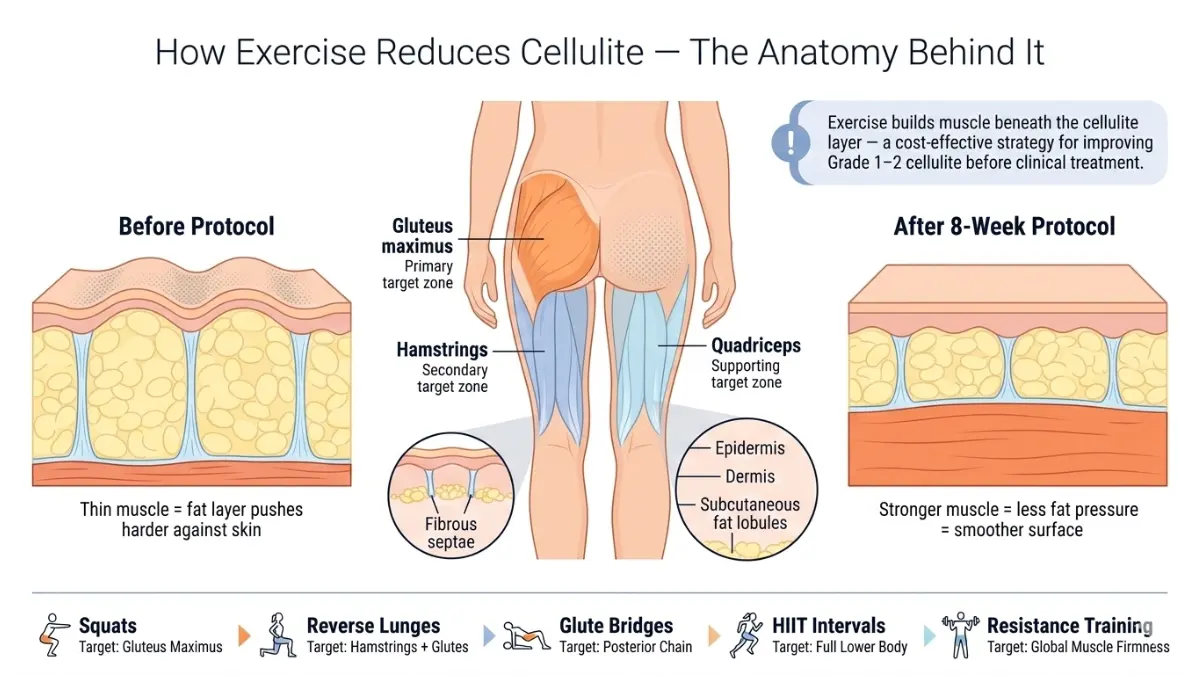
General cardio alone won’t address cellulite. The goal is to build muscle directly beneath the cellulite layer, which physically plumps the skin from within and improves circulation in the affected tissue.
5 evidence-supported exercises for cellulite reduction:
- Squats — Directly targets gluteal and thigh musculature beneath the primary cellulite zones
- Reverse Lunges — Engages deeper fascia layers; improves local circulation in the posterior thigh
- Glute Bridges — Tightens the connective tissue layer and strengthens the posterior chain
- HIIT Intervals (20 min, 3x/week) — Reduces subcutaneous fat volume, decreasing pressure on septae
- Resistance Training (3x/week) — Builds skin-firming muscle across the entire affected region
Train in the optimal fat-burning zone with our Heart Rate Zone Calculator, and track your cardio pace using our Running Pace Calculator to ensure you’re training effectively, not just frequently.
Anti-Cellulite Diet — What to Eat and What to Avoid
Diet directly influences fluid retention, inflammation, and collagen integrity — all factors that affect how visible cellulite appears.
| Eat More Of | Avoid or Reduce |
|---|---|
| Vitamin C-rich foods (citrus, peppers) — boost collagen synthesis | Ultra-processed foods — promote systemic inflammation |
| Omega-3 fatty acids (salmon, walnuts) — anti-inflammatory | High-sodium foods — accelerate fluid retention |
| High-fiber vegetables — support lymphatic drainage | Refined sugar — degrades collagen cross-linking |
| Lean protein (chicken, legumes) — tissue repair and firmness | Alcohol — dehydrates skin, weakens connective tissue |
Calculate your ideal daily protein for tissue repair using our Protein Intake Calculator, and understand your calorie targets with our Calorie Deficit Calculator.
Hydration — The Most Overlooked Factor
Blood flow in cellulite-affected areas is measurably lower than in healthy tissue. Proper hydration directly supports lymphatic function, reduces fluid retention, and maintains skin elasticity. Aim for at least 2–3 liters daily — more if you’re exercising regularly.
Use our Water Intake Calculator to get a personalized daily hydration target based on your body weight and activity level.
Your 8-week starter protocol:
- Weeks 1–2: Begin HIIT 2x/week + resistance training 2x/week. Eliminate ultra-processed food and alcohol.
- Weeks 3–6: Add squats, glute bridges, and lunges. Introduce retinol 0.3% cream nightly. Hit daily protein and water targets.
- Weeks 7–8: Assess results. If Grade 1, continue protocol. If Grade 2+, schedule dermatologist consultation alongside lifestyle maintenance.
For those interested in parallel skin-improvement approaches, our guide on microneedling in 2026 covers collagen-stimulating treatments that can complement a cellulite reduction plan.
Frequently Asked Questions About Cellulite
1. Does cellulite go away on its own?
No. Cellulite does not resolve without intervention. The fibrous septae causing the dimpling are structural — they do not self-correct. Grade 1 cellulite may become less visible with sustained lifestyle changes, but Grade 2–3 typically requires clinical treatment.
2. Can you permanently get rid of cellulite?
Not permanently, but significantly and durably. Subcision-based procedures (Avéli, Resonic) and collagenase injections provide the longest-lasting results — up to 12 months to 3 years in clinical studies. Most treatments require maintenance over time.
3. Why do I have cellulite if I’m thin?
Because cellulite is structural, not a fat mass problem. Even women with very low body fat percentages have vertically-oriented fibrous septae that allow fat to protrude through. Genetics and hormones — not weight — are the primary drivers.
4. Is cellulite dangerous or a health risk?
No. Cellulite poses no medical risk and is classified as a cosmetic condition. It does not indicate any underlying disease. However, its psychological impact — including reduced confidence and social anxiety — is well-documented in research and is a valid reason to seek treatment.
5. What does Grade 3 cellulite look like?
Grade 3 cellulite features deep raised ridges and pronounced depressions visible while standing, even without pinching the skin. It typically feels firm or rubbery to the touch, and the dimpling may be visible at rest in multiple positions.
6. Does losing weight remove cellulite?
Partially — and not always. Weight loss reduces the fat volume pushing against the septae, which can lessen the appearance. However, approximately 32% of people in one study found that weight loss actually made cellulite more visible, likely because skin lost elasticity as volume decreased.
7. At what age does cellulite appear?
Most women first notice cellulite in their late teens to mid-20s, coinciding with post-pubertal hormonal shifts. It becomes more prominent with age as collagen production decreases and skin thins. Pregnancy and menopause are the most common acceleration triggers.
8. Can men get cellulite?
Yes, but rarely. Fewer than 10% of men develop visible cellulite due to their criss-cross septae architecture. Men who take estrogen therapy or have androgen deficiency have significantly higher rates.
9. How long does radiofrequency treatment take to work?
Most patients see initial improvement within 4–6 weeks of starting a course of RF treatments. Peak results appear at 3–6 months, after collagen remodeling is complete. A typical course is 4–8 sessions. Results usually last around 6 months without maintenance.
10. Does dry brushing actually help cellulite?
Dry brushing improves surface circulation and lymphatic drainage temporarily, which can reduce puffiness and make skin appear smoother short-term. However, it does not address the underlying fibrous septae. It is best used as a daily adjunct to — not a replacement for — clinical treatment.
11. When should I see a doctor about my cellulite?
See a board-certified dermatologist if:
– Your cellulite is Grade 2 or higher (visible while standing)
– It is causing emotional distress or affecting daily life
– Home remedies and lifestyle changes haven’t improved it after 8–12 weeks
– You are considering any clinical procedure and want a personalized evidence-based treatment plan
The American Academy of Dermatology (AAD) recommends consulting a dermatologist who specializes in cosmetic procedures before pursuing any cellulite treatment. You can also use our Symptom Checker for a preliminary self-assessment, or explore our full library of dermatology guides at mymedicineadvisor.com/health/.
Medical Disclaimer: This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before starting any treatment for cellulite or any other medical condition.
📊 Quick Reference — Cellulite at a Glance
| Fact | Data |
|---|---|
| Prevalence in post-pubertal women | 80–98% |
| Primary cause | Fibrous septae architecture + hormonal influence |
| Most evidence-based treatment (2026) | Shock wave therapy (SWT) |
| Grades | 0 (none) to 3 (severe) |
| Can lifestyle alone cure Grade 3? | No — clinical treatment required |
| Does liposuction treat cellulite? | No — may worsen appearance |
| Best single-session option (2026) | Acoustic subcision (Resonic) |
Related Reading: Microneedling — Does It Work in 2026? | Morpheus8: Doctors’ Honest 2026 Review | Skin Cancer: 12 Warning Signs
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.