On This Page – Quick Medical Summary
⚡ Quick Answer: Most ringworm infections clear in 2–4 weeks with the correct antifungal cream. If yours isn’t healing, you’re likely using the wrong treatment for your specific body location — or you may be facing a drug-resistant strain now tracked by the CDC in the U.S. This guide covers both.
Marcus, a 38-year-old teacher from Ohio, tried three different over-the-counter antifungal creams over eight weeks. His ring-shaped rash kept spreading. His dermatologist finally ran a fungal culture and identified Trichophyton indotineae — a drug-resistant ringworm strain that standard creams simply cannot kill.
He’s not alone. Millions of Americans search “ringworm won’t go away” every month. The reason is almost always one of three things: wrong treatment for the body part, incorrect application, or an emerging resistant strain.
In this article, you’ll learn:
- Exactly which ringworm treatment works for each body part
- Why your antifungal cream may be failing — and what to use instead
- The 2026 drug-resistance warning no other health site covers for patients
- How to use antifungal medication correctly (most people skip a critical step)
- When to stop treating at home and see a doctor
What Actually Treats Ringworm? The Fast Medical Answer
Ringworm is not caused by a worm. It is a fungal skin infection — medically known as tinea or dermatophytosis — caused by dermatophyte fungi that feed on keratin in skin, hair, and nails. Because it is fungal, it requires antifungal medication, not antibiotics and not steroid creams.
🔑 Key Takeaway: Antifungal medication is the only proven ringworm treatment. Antibiotics do nothing. Steroid creams actively worsen the infection.
OTC vs. Prescription Ringworm Treatment at a Glance
| Treatment Type | Examples | Best For | Available Without Rx? |
|---|---|---|---|
| Terbinafine 1% | Lamisil AT | Body, feet, groin | ✅ Yes |
| Clotrimazole 1% | Lotrimin AF, Mycelex | Body, groin, mild cases | ✅ Yes |
| Miconazole 2% | Desenex, Micatin | Mild body ringworm | ✅ Yes |
| Tolnaftate 1% | Tinactin | Prevention + mild cases | ✅ Yes |
| Griseofulvin | Grifulvin V | Scalp, severe cases | ❌ Prescription only |
| Itraconazole | Sporanox, Onmel | Drug-resistant strains | ❌ Prescription only |
| Fluconazole | Diflucan | Widespread infections | ❌ Prescription only |
According to the CDC’s ringworm treatment guidelines, over-the-counter antifungal creams and ointments are appropriate for mild skin infections, but prescription oral medication is required for scalp infections and severe or resistant cases.
⚠️ Critical Danger Warning — Do NOT Use These on Ringworm
Many OTC rash creams contain corticosteroids (hydrocortisone, betamethasone, triamcinolone). Applying these to ringworm:
- Weakens your skin’s immune response, allowing the fungus to spread
- Can cause the rash to change appearance, making it harder to diagnose
- Creates “tinea incognita” — a masked, spreading infection that looks atypical
- Worsens burning, redness, and itching in the long term
Never use: Cortaid, Cortizone-10, or any cream labeled “anti-itch with hydrocortisone” on ringworm or any undiagnosed ring-shaped rash.
Ringworm Treatment by Body Part — The Complete 2026 Guide
This is the section that Healthline, WebMD, and Mayo Clinic all fail to provide. No body-part-specific treatment table exists anywhere in the current top 10 SERP results. This table is your answer.
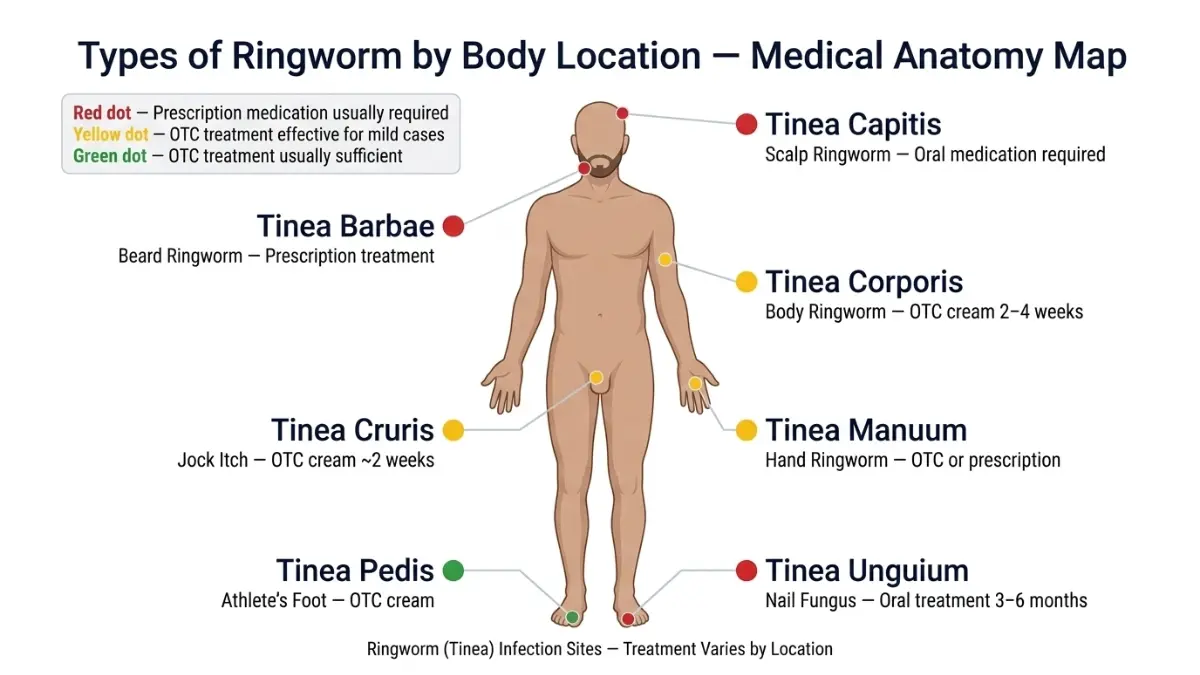
Master Ringworm Treatment Table by Body Location
| Body Part | Medical Name | First-Line Treatment | Duration | Prescription Required? |
|---|---|---|---|---|
| Body / Skin | Tinea corporis | Clotrimazole or terbinafine cream | 2–4 weeks | No (mild cases) |
| Scalp | Tinea capitis | Oral griseofulvin or terbinafine | 1–3 months | Yes — always |
| Groin / Jock Itch | Tinea cruris | Antifungal cream or powder | 2 weeks | No (mild cases) |
| Feet / Athlete’s Foot | Tinea pedis | Terbinafine cream | 2–4 weeks | No |
| Nails | Tinea unguium | Oral terbinafine or itraconazole | 3–6 months | Yes — always |
| Beard / Face | Tinea barbae | Oral antifungal | 4–8 weeks | Yes — usually |
| Drug-resistant strain | T. indotineae | Oral itraconazole | Varies (6+ weeks) | Yes — always |
⚠️ Scalp Ringworm: Why Cream Never Works
This is the #1 mistake people make. Antifungal cream cannot penetrate hair follicles. If you’re applying cream to a scaly, itchy scalp and seeing no results, the cream itself is the problem — not the brand.
- Only oral antifungal medication can treat scalp ringworm (tinea capitis)
- Griseofulvin is the standard first-line treatment for children — typically 6–8 weeks
- Medicated shampoo (ketoconazole 2%, selenium sulfide) can reduce spread but cannot cure the infection alone
- Always combine shampoo with oral medication for scalp infections
Not sure whether your rash is ringworm or something else — like eczema or psoriasis? Use our Symptom Checker to evaluate your skin symptoms before spending money on the wrong treatment.
⚠️ Nail Ringworm: The Longest and Hardest to Treat
Nail infections (tinea unguium) are stubborn for one reason: antifungal topical solutions cannot penetrate the full thickness of the nail plate in most cases.
- Oral terbinafine or itraconazole for 3–6 months is the standard protocol
- Toenail infections take longer than fingernail infections to clear
- Early diagnosis is critical — the longer you wait, the harder it becomes to treat
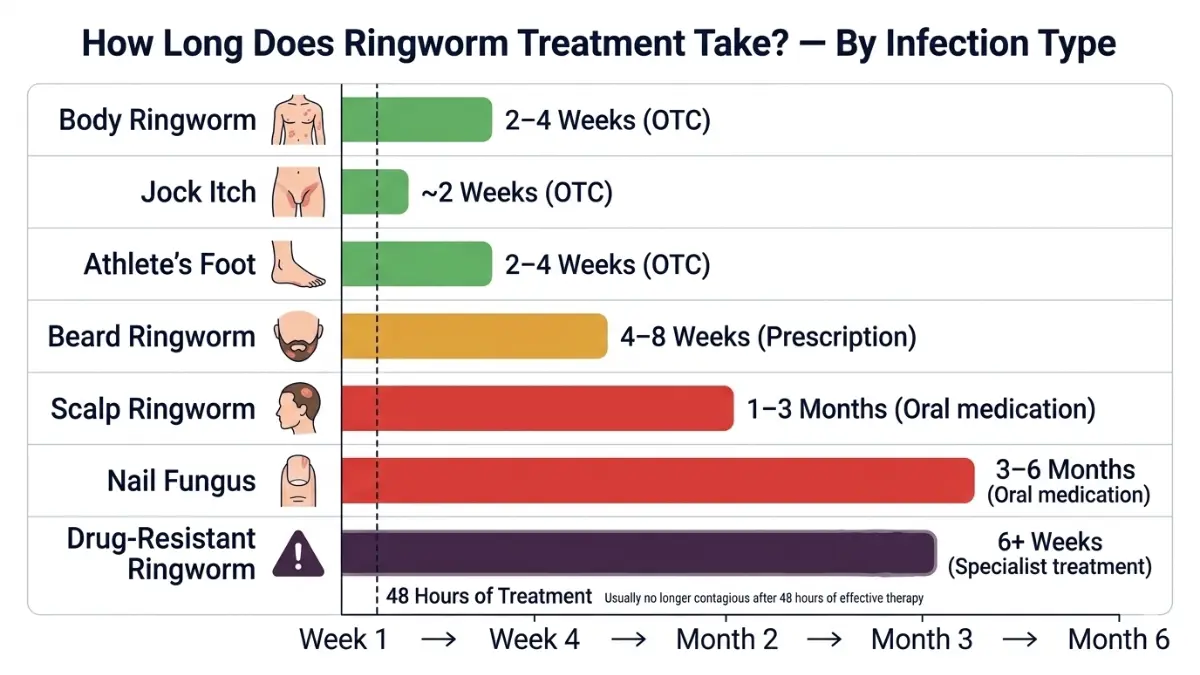
How Long Until Ringworm Is No Longer Contagious?
🔑 Key Fact: Ringworm becomes non-contagious within 48 hours of starting effective antifungal treatment. If you or your child are using the correct medication:
- Day 1–2: Still contagious — avoid skin contact and sharing items
- Day 3 onward: No longer contagious with active treatment
- Week 2–4: Rash visibly fading with consistent twice-daily application
How to Use Ringworm Treatment the Right Way
Most OTC antifungal cream failures are not caused by a bad product — they are caused by incorrect application. A survey of dermatology patients consistently shows two errors: applying too little cream and stopping treatment too early.
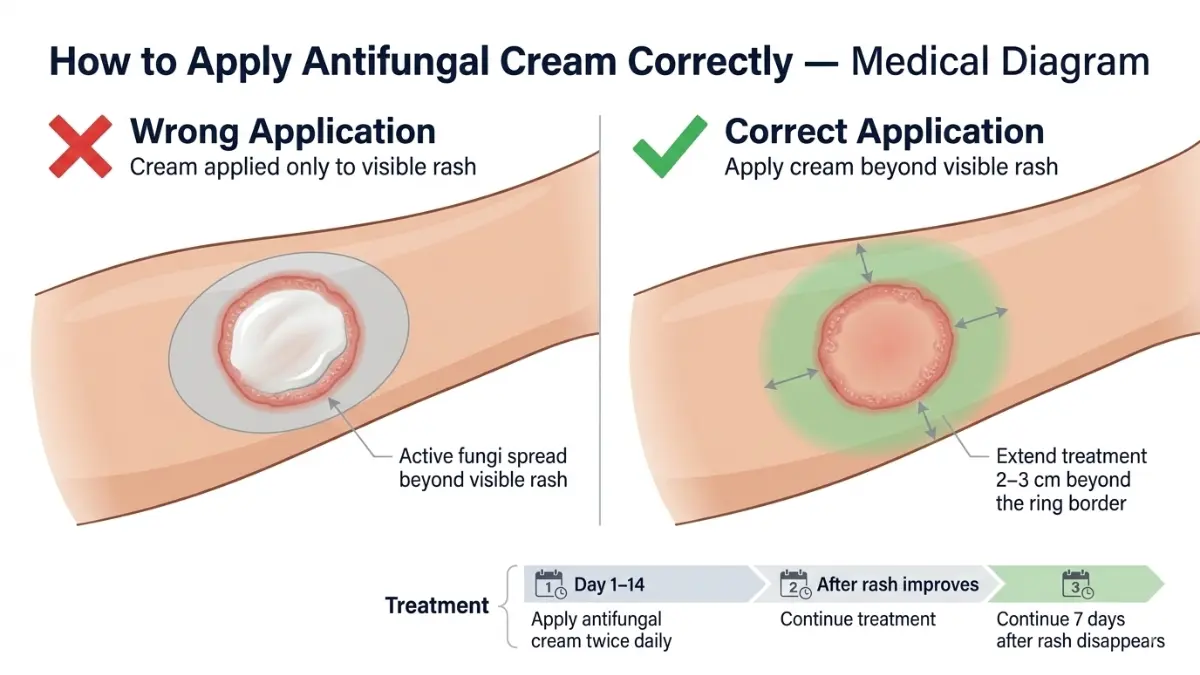
Step-by-Step Antifungal Application Protocol
- Wash the infected area with soap and water — then dry completely (moisture helps fungi survive)
- Apply cream beyond the rash border — extend at least 2–3 cm past the visible ring edge (this is where active fungi are spreading)
- Apply twice daily — morning and night — consistently
- Do not stop when the rash fades — continue for 7 full days after skin looks clear
- Wash hands immediately after every application
- Wash bedding, towels, and worn clothing in hot water (60°C/140°F) every 2–3 days during treatment
Why Isn’t My Ringworm Cream Working?
If you’ve been applying antifungal cream for 2+ weeks with no improvement, the likely reasons are:
- Wrong product: Using a cream with steroid ingredients that are worsening the infection
- Wrong application: Not extending past the ring border; applying once daily instead of twice
- Stopping too early: Rash clears visually but fungi remain — you stopped at day 10, fungi return by day 20
- Reinfection source: Infected pet, shared towel, gym equipment recontaminating the area
- Drug-resistant strain: Standard creams are biologically ineffective against T. indotineae — no amount of correct application will work
What This Means For You: If your ringworm won’t go away after 2 full weeks of twice-daily antifungal cream applied correctly, do not try a different OTC brand. See a dermatologist. You likely need oral medication or testing for resistance.
If you’ve been prescribed an oral antifungal and are unsure about your medication, use our Pill Identifier to verify your prescription before starting treatment.
Drug-Resistant Ringworm in 2026 — The Warning No One Is Telling Patients
This is the most important section in this article — and the one that Healthline, WebMD, Mayo Clinic, and the CDC’s patient-facing pages have not yet explained clearly to the general public.
Drug-resistant ringworm is real, it is in the United States, and it is spreading.
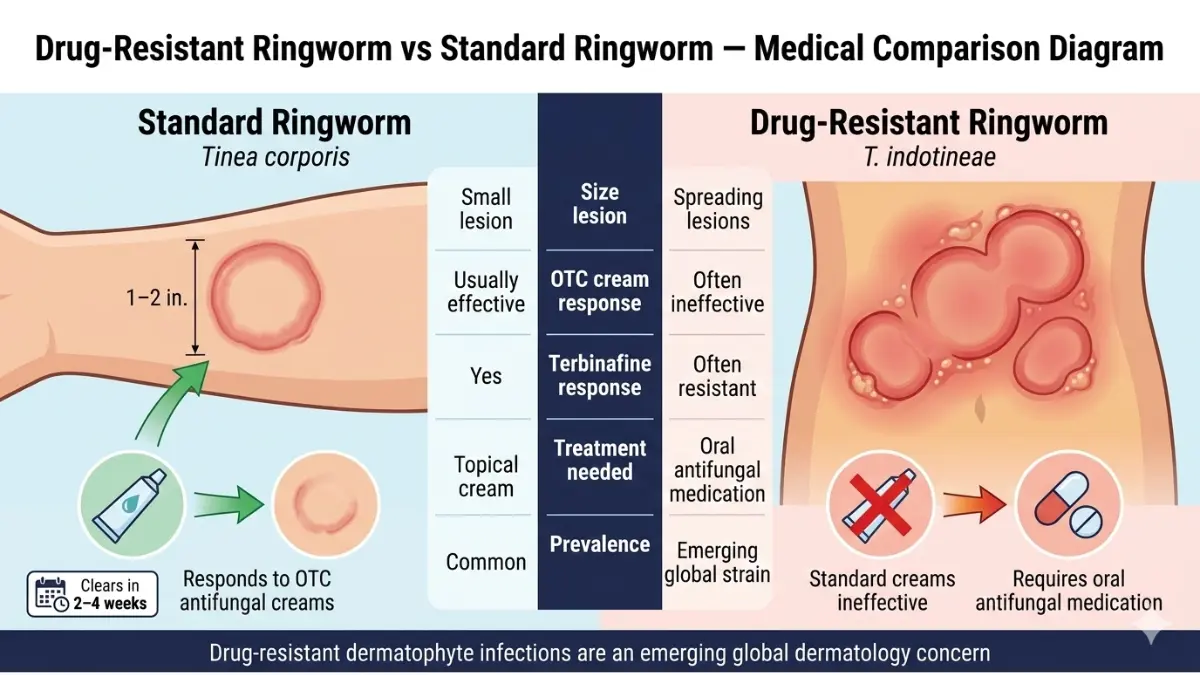
What Is Trichophyton indotineae?
Trichophyton indotineae (T. indotineae) is a drug-resistant fungal strain that originated in South Asia and has been spreading globally. According to the CDC’s emerging ringworm clinical overview:
- The first U.S. cases were confirmed in New York City in early 2023
- Cases have since been identified in multiple U.S. cities
- The strain is resistant to terbinafine — the most common OTC and prescription first-line treatment
- Standard clotrimazole and miconazole creams are also largely ineffective
Two antimicrobial-resistant strains of public health concern in the United States are T. indotineae and terbinafine-resistant T. rubrum, according to the CDC’s clinical briefing updated in 2024.
Unlike typical ringworm infections, those involving T. indotineae often do not resolve with over-the-counter topical antifungals or oral terbinafine, which is the standard first-line systemic therapy.
Signs Your Ringworm May Be Drug-Resistant
See a dermatologist urgently — do not wait — if your ringworm shows these signs:
- No improvement after 4 weeks of consistent, correct OTC antifungal use
- The rash is spreading rapidly despite treatment — covering thighs, trunk, or multiple body areas
- The rash is unusually severe — inflamed, pustular, or painful rather than mildly itchy
- You have recently traveled internationally, especially to South Asia, Southeast Asia, or Europe
- You have had close contact with someone who has a severe, spreading, or treatment-resistant ringworm infection
What to Tell Your Dermatologist
When you see your doctor for treatment-resistant ringworm, specifically ask for:
- A KOH (potassium hydroxide) skin scraping test to confirm it is truly ringworm
- A fungal culture to identify the specific species
- Antifungal susceptibility testing if available at their lab or a reference lab
- A discussion about oral itraconazole — currently the most effective treatment for T. indotineae and resistant strains
🔑 Key Takeaway: Itraconazole (Sporanox) for 6+ weeks is the current standard of care for drug-resistant ringworm in the U.S. Your GP may not be familiar with this — ask for a dermatology referral.
Some individuals with underlying immune conditions or autoimmune disorders may be at higher risk for persistent fungal infections. You can explore individual immune-related risk factors using our Genetic Risk Assessment Tool.
Home Remedies for Ringworm — What Science Actually Says
There is a lot of misinformation online about home remedies for ringworm. Here is an honest, evidence-ranked breakdown — because your health depends on getting this right.
First, the critical fact: Ringworm almost never heals on its own without antifungal treatment. Without medication, the infection slowly expands outward. Home remedies may reduce discomfort but cannot reliably eliminate the underlying fungal infection.
Home Remedy Evidence Table
| Remedy | Evidence Level | Can Replace Antifungal? | Safety Note |
|---|---|---|---|
| Tea tree oil (topical) | Limited — some antifungal activity in lab | No | Dilute before use; toxic if ingested |
| Coconut oil | Very limited evidence | No | Safe; may moisturize irritated skin |
| Garlic paste | Minimal lab evidence | No | Can cause skin burns — use with caution |
| Apple cider vinegar | Some antifungal properties | No | Risk of open sores and scarring |
| Turmeric paste | Anti-inflammatory only | No | Safe but not antifungal |
The American Academy of Dermatology confirms that antifungal treatments clear all ringworm infections, but it takes time and requires completing the full course. Natural remedies may be used alongside antifungal medication but should not delay starting proven treatment.
How to Stop Ringworm From Coming Back
Ringworm recurrence is extremely common — and almost always preventable. Follow this protocol during and after treatment:
- Wash all bedding and towels in hot water every 2–3 days during treatment and for one week after
- Never share combs, towels, clothing, hats, or pillowcases
- Wear flip-flops in gym showers, locker rooms, and public pools — bare feet are the most common infection vector
- Keep skin dry — fungi thrive in moisture and warmth; dry thoroughly after bathing
- Check your pets — dogs, cats, and rabbits commonly carry ringworm without visible symptoms; look for scaly, hairless patches and have your vet examine them
- Complete the full treatment course — stopping early when the rash fades is the #1 cause of recurrence
For more evidence-based guidance on skin health and immune support, visit our Health Tips hub.
When to See a Doctor + The Complete Summary
Most people can successfully treat mild body ringworm at home with OTC antifungals. But there are clear clinical signs that home treatment is no longer appropriate.
7 Signs You Need a Doctor for Ringworm — Do Not Wait
- No improvement after 2 weeks of correct, twice-daily OTC antifungal cream
- Scalp is affected — oral prescription medication is always required; no cream will work
- Nails are affected — thick, discolored, or crumbling nails need oral prescription treatment
- Rash is spreading rapidly, covering large body areas or multiple sites
- Rash is painful, oozing, crusting, or has pus-filled bumps — indicates severe infection or secondary bacterial infection
- You are immunocompromised, diabetic, on long-term steroids, or have an autoimmune condition
- You have recently traveled internationally and standard treatments are not working
Master Ringworm Treatment Reference Table
| Infection Type | OTC Sufficient? | Oral Meds Needed? | Treatment Duration |
|---|---|---|---|
| Body/skin (mild) | ✅ Yes | Only if widespread | 2–4 weeks |
| Scalp (tinea capitis) | ❌ No | ✅ Always | 1–3 months |
| Nails (onychomycosis) | ❌ No | ✅ Always | 3–6 months |
| Groin/jock itch (mild) | ✅ Yes | Rarely | 2 weeks |
| Beard area | ❌ Usually not | ✅ Usually | 4–8 weeks |
| Drug-resistant (T. indotineae) | ❌ No | ✅ Itraconazole | 6+ weeks |
If you are concerned about skin conditions that may be misidentified as ringworm — including eczema, psoriasis, or contact dermatitis — our articles on eczema treatment and psoriasis treatment can help you distinguish between these conditions.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider or board-certified dermatologist for the diagnosis and treatment of any skin condition.
Frequently Asked Questions About Ringworm Treatment
Q1. What is the fastest ringworm treatment that works?
Terbinafine 1% cream (Lamisil AT) is generally considered the fastest-acting OTC antifungal for body ringworm, with many patients seeing improvement within 7–10 days. For scalp or nail infections, prescription oral medication is required and is the fastest effective route.
Q2. How long does ringworm take to clear with treatment?
Body ringworm clears in 2–4 weeks with consistent OTC cream. Scalp ringworm requires 1–3 months of oral medication. Nail infections can take 3–6 months. Starting treatment immediately and completing the full course are the two most important factors.
Q3. Can ringworm go away without treatment?
Rarely, and very slowly. Without antifungal treatment, ringworm expands outward, becomes more contagious, and risks spreading to other body parts or household members. Treatment is always recommended.
Q4. Is ringworm still contagious after I start treatment?
Yes — for the first 48 hours. After 48 hours of effective antifungal treatment, the infection is generally no longer contagious. Always wash your hands after applying cream and avoid sharing personal items during active infection.
Q5. Why is my ringworm not going away with cream?
The most common reasons are: applying cream once instead of twice daily, stopping treatment when the rash visibly clears (too early), using a cream that contains steroids, reinfection from a contaminated surface or pet, or infection with a drug-resistant strain like T. indotineae that standard creams cannot treat.
Q6. What should I NOT put on ringworm?
Never apply steroid creams (hydrocortisone, betamethasone, or any “anti-itch” cream with cortisone) to ringworm. These worsen the infection by suppressing local immune response. Also avoid apple cider vinegar directly on broken or sensitive skin, as it can cause chemical burns.
Q7. Can I treat scalp ringworm with antifungal cream?
No. Antifungal cream cannot penetrate hair follicles and has zero efficacy against scalp ringworm (tinea capitis). Oral prescription medication — most commonly griseofulvin or terbinafine tablets — is always required for scalp infections.
Q8. Is ringworm treatment different for children?
Yes. Children with scalp ringworm are most commonly treated with oral griseofulvin (Grifulvin V) for 6–8 weeks, typically taken with a fatty meal to improve absorption. The AAD recommends children return to school after 48 hours of treatment; they do not need to miss school if the area can be covered.
Q9. What is drug-resistant ringworm and should I be worried?
Drug-resistant ringworm caused by Trichophyton indotineae and terbinafine-resistant T. rubrum has now been confirmed in multiple U.S. cities. If your ringworm treatment is not working after 4 weeks, you should ask your dermatologist about testing for these resistant strains and discuss itraconazole as an alternative.
Q10. Can pets give me ringworm again after I’m treated?
Yes. Cats, dogs, and rabbits are common carriers of ringworm and may show no visible symptoms. If ringworm keeps recurring in your household, have all pets examined and treated by a veterinarian while you complete your own treatment course.
Q11. Does ringworm leave a scar or dark mark after treatment?
Ringworm itself rarely causes permanent scarring on smooth skin. However, it can leave temporary post-inflammatory hyperpigmentation (dark marks) that fades over weeks to months. Scalp ringworm, if left untreated, can cause permanent hair loss and scarring — another reason early treatment is critical.
Related Reading on mymedicineadvisor.com:
- Skin Tag Removal: What Dermatologists Recommend
- Eczema Treatment: Dermatologist-Backed Guide
- Keratosis Pilaris Treatment That Actually Works
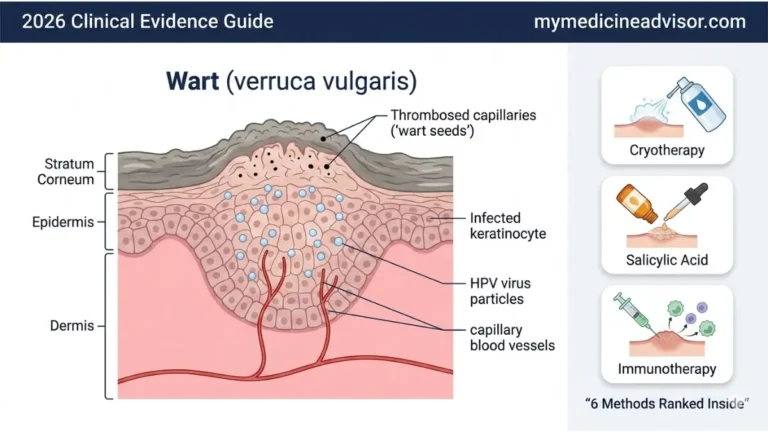
- Wart Removal Methods: What Dermatologists Use
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.