On This Page – Quick Medical Summary
What Is Keratosis Pilaris Treatment — And Does It Actually Work?
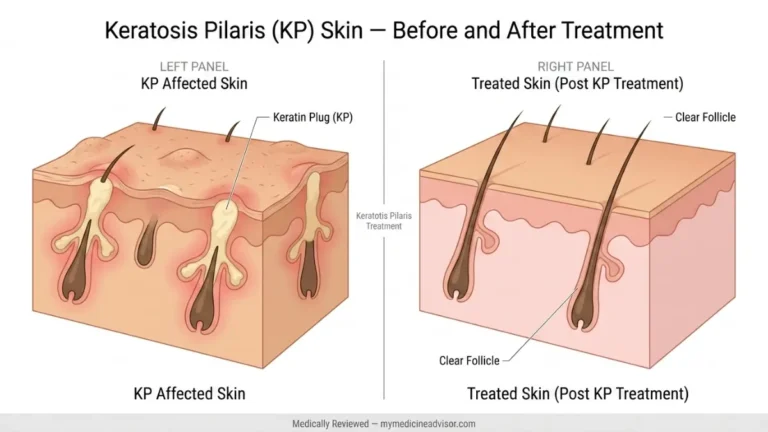
Keratosis pilaris (KP) treatment cannot permanently cure the condition, but clinically proven options — from lactic acid to Nd:YAG laser therapy — can dramatically reduce bumps, redness, and rough texture. Most patients see meaningful improvement within 6–12 weeks when using the right treatment matched to their severity level.
Marcus, a 31-year-old from Chicago, had lived with rough, sandpaper-textured bumps on his upper arms since age 14. He tried three different body lotions over two years with no results. The problem wasn’t effort — it was strategy. He was moisturizing without exfoliating. Once his dermatologist added a 12% lactic acid lotion, he saw visible smoothing within eight weeks.
That’s the core truth about keratosis pilaris treatment: the right mechanism matters more than the number of products you use.
Fast Facts — KP by the Numbers
| Statistic | Data |
|---|---|
| Adults affected | ~40% of the global adult population |
| Adolescents affected | 50–80% of teenagers |
| Most common body sites | Upper arms (92%), thighs (59%), buttocks (30%) |
| #1 dermatologist first-line choice | Topical lactic acid (43.6% of dermatologists surveyed) |
| KP treatment market size (2024) | $7.3 billion, growing at 6.1% CAGR |
Source: StatPearls/NCBI — Keratosis Pilaris, 2025
If you’re unsure whether your bumps are KP or another skin condition like eczema or folliculitis, use our free Symptom Checker before starting any treatment protocol.
The 4-Step Keratosis Pilaris Treatment Protocol (By Severity)
This is what no top competitor gives you — a clear, severity-matched treatment ladder. Mayo Clinic, Healthline, and AAD all list ingredients. None tell you which to use first, next, or when to escalate.
Here is the exact framework board-certified dermatologists use.
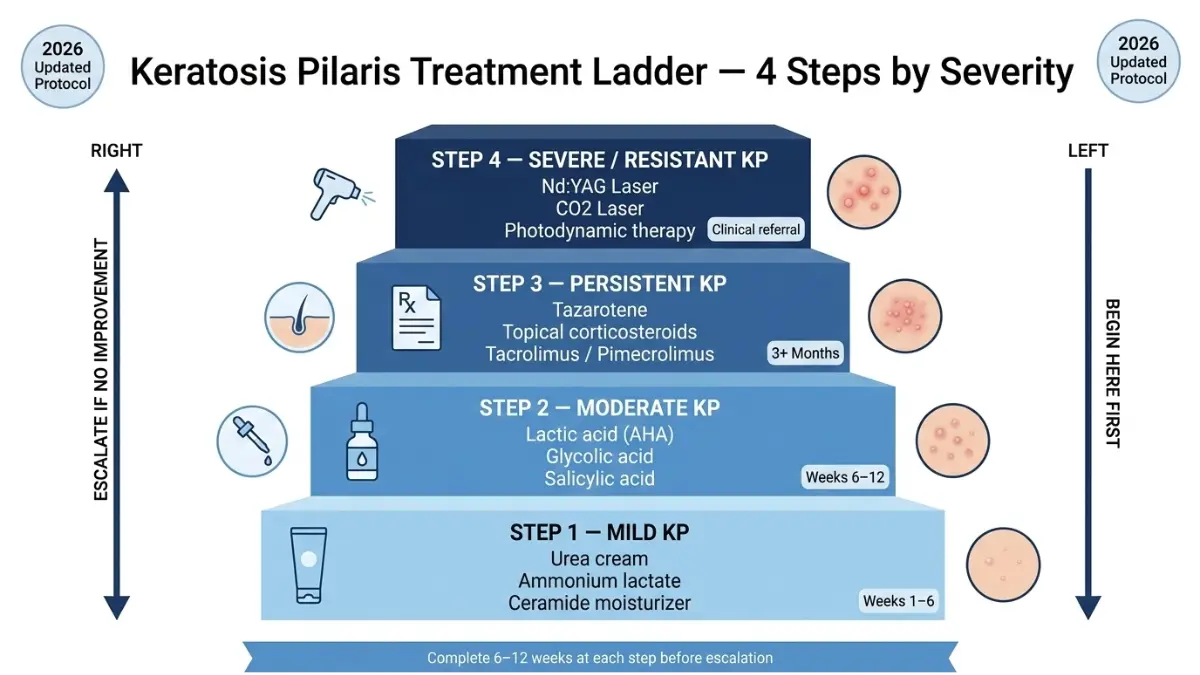
Step 1 — Mild KP (Weeks 1–6): Moisturizer + Urea Basics
This is your entry point. If your bumps are subtle, skin-colored, and mostly a texture issue, start here.
What to use:
- Urea 10–20% creams — breaks down the keratin plug directly
- Ammonium lactate lotion (12%) — hydrates and exfoliates simultaneously
- Ceramide-rich moisturizers — repairs the skin barrier disrupted by KP
Application protocol:
- Apply within 3 minutes of bathing, while skin is still damp
- This maximizes ingredient absorption through open pores
- Use twice daily — morning and evening
Expected result: Softer texture, reduced roughness within 4–6 weeks of consistent use.
⚡ Key Takeaway: Moisturizer alone won’t clear KP. You need an ingredient that actively dissolves keratin — urea is your first weapon.
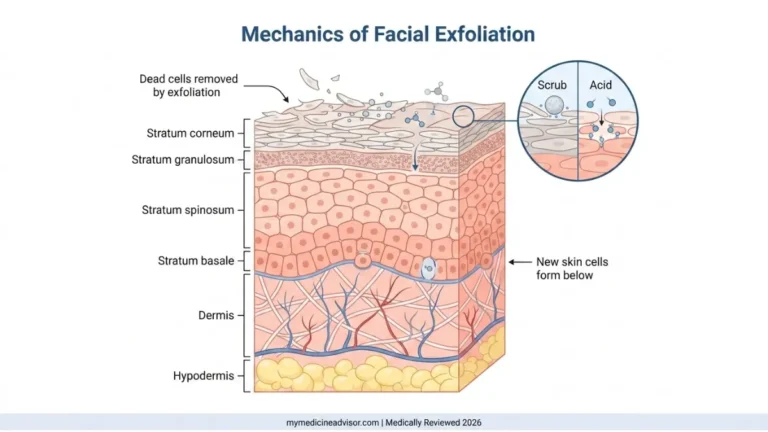
Step 2 — Moderate KP (Weeks 6–12): Chemical Exfoliants (AHA/BHA)
If Step 1 hasn’t produced visible clearing after six weeks, your KP requires active keratolytic exfoliation.
Clinical evidence matters here. A 2023 dermatologist survey published at the ODAC Conference confirmed that topical lactic acid is the most used first-line therapy for KP, chosen by 43.6% of board-certified dermatologists, followed by salicylic acid (20.7%).
AHA vs. BHA — Quick Reference:
| Ingredient | Type | Best For | Frequency | Caution |
|---|---|---|---|---|
| Lactic acid | AHA | All skin types, hydrating | 2–3×/week | Mild stinging on broken skin |
| Glycolic acid | AHA | Oily/normal skin | 2–3×/week | Higher irritation potential |
| Salicylic acid | BHA | Oily, inflamed KP | 2–3×/week | Can over-dry if overused |
| Urea (20%+) | Keratolytic | Thick, rough KP | Daily | Avoid eye area |
How to use correctly:
- Apply chemical exfoliant to affected area 2–3 nights per week
- Do not combine with retinoids on the same night
- Always follow with a moisturizer to prevent dryness
⚡ What This Means For You: If urea cream hasn’t worked in six weeks, switch the mechanism — move to lactic acid or glycolic acid. More product isn’t the answer. A different ingredient is.
For related skin texture concerns, our guide on CO2 laser treatment covers professional resurfacing options in depth.
Step 3 — Persistent KP (3+ Months): Prescription Topicals
When OTC options plateau, prescription-strength treatments become the next clinical step.
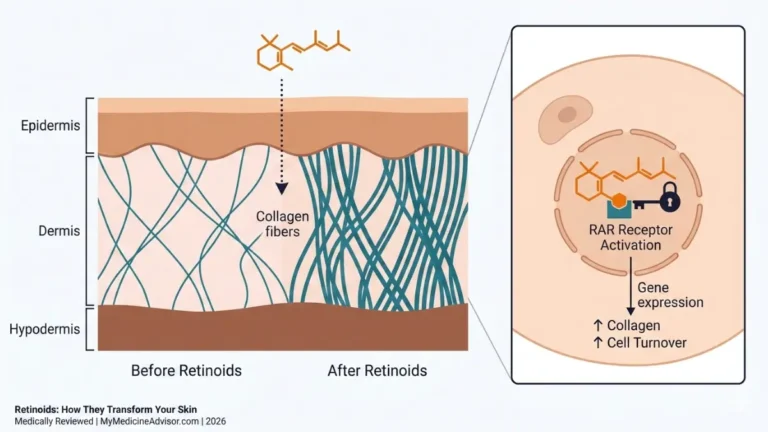
Topical Retinoids (Tazarotene 0.05%/0.1%)
A randomized, placebo-controlled, double-blind trial published in the Journal of the American Academy of Dermatology confirmed that tazarotene 0.05% cream significantly improved pruritus, erythema, and skin roughness in KP patients compared to placebo. Results appeared within 4–8 weeks of nightly use.
- Available only by prescription
- Apply at night — retinoids degrade in sunlight
- Not safe during pregnancy — if you are pregnant or planning pregnancy, discuss alternatives with your OB/GYN. You can use our Pregnancy Weight Gain Calculator to track your overall pregnancy health while exploring safe skincare options with your provider.
Topical Corticosteroids (Short-Term)
- Reduce inflammation and redness in KP rubra subtype
- For short-term use only — not a long-term keratosis pilaris treatment
- Prescription required for mid-potency options
Off-Label Options (For Resistant Cases)
- Tacrolimus/pimecrolimus — topical immunomodulators used for inflammatory KP variants
- Topical sirolimus — emerging case report evidence for KP rubra faciei (2025, JAAD Case Reports)
Step 4 — Severe/Resistant KP: Clinical & Laser Treatments
When months of topical treatment haven’t delivered results, clinical procedures are the next frontier.
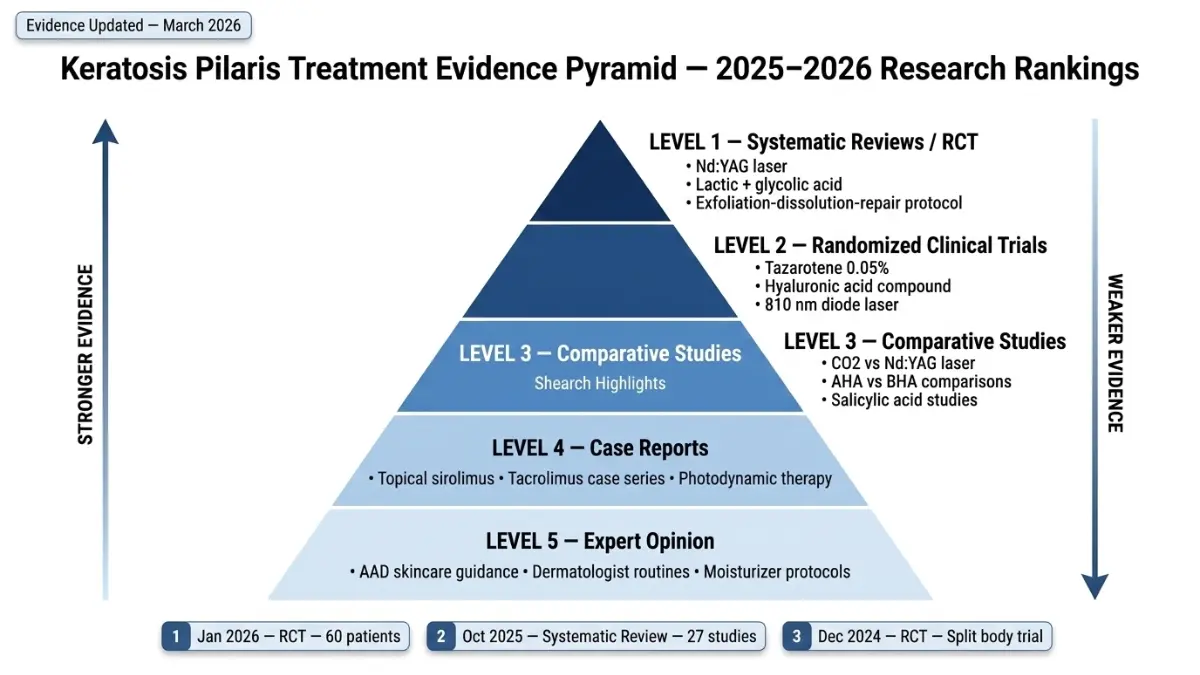
A landmark systematic review published in October 2025 in the European Journal of Dermatology — analyzing 27 studies published between 2011 and 2024 — confirmed the Nd:YAG 1064nm laser as the most consistently effective clinical treatment for keratosis pilaris.
| Laser/Procedure | What It Does | Sessions Needed | Evidence Level |
|---|---|---|---|
| Nd:YAG 1064nm | Reduces texture, redness, papules | 3–6 sessions | Highest (multiple RCTs) |
| CO2 Laser | Ablative resurfacing, texture | 1–3 sessions | Moderate |
| Erbium:YAG | Resurfacing, fewer side effects | 2–4 sessions | Emerging |
| Pulsed Dye Laser (PDL) | Targets redness in KP rubra | 3–5 sessions | Case report level |
| Photodynamic Therapy (PDT) | Off-label, emerging | Variable | Limited RCT data |
For a complete overview of professional laser skin treatments, read our detailed guide on microdermabrasion and whether it’s worth it for comparison.
⚡ 2026 Research Breakthrough: A January 2026 randomized controlled trial published in PMC (Journal of Cosmetic Dermatology, Wiley) evaluated a novel three-component Exfoliation-Dissolution-Repair formula in 60 KP volunteers over 28 days. The combined scrub-plus-moisturizing-lotion approach showed statistically significant reduction in follicular papules and roughness scores versus the control group — the first RCT to validate a multi-mechanism KP protocol in a single study design.
Keratosis Pilaris Treatment by Skin Tone — What Changes and Why
This is the most critical gap in every top-ranking KP article. Healthline, Mayo Clinic, and AAD treat keratosis pilaris as a single condition with a single treatment path. It isn’t. Your skin tone directly affects which treatments are safe and effective.
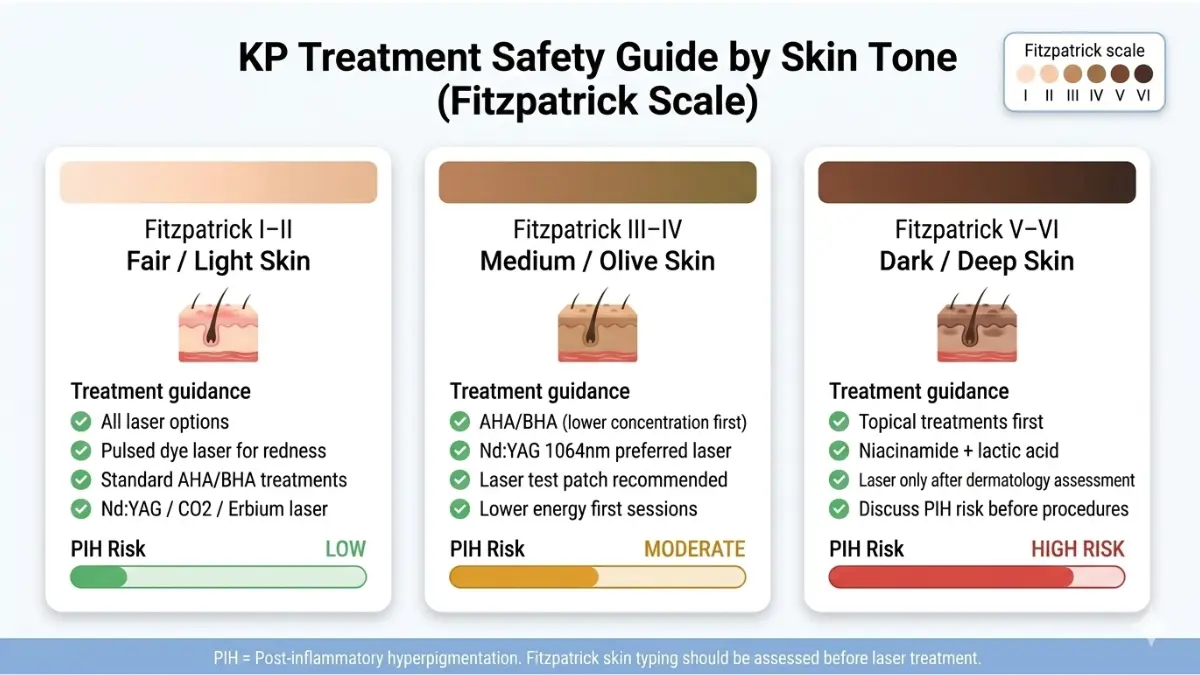
Fair/Light Skin Tones (Fitzpatrick I–II)
- Full range of laser options available with minimal risk
- Pulsed dye laser is particularly effective for visible redness (KP rubra)
- Standard AHA/BHA protocols apply without modification
- Post-inflammatory hyperpigmentation (PIH) risk: low
Medium/Olive Skin Tones (Fitzpatrick III–IV)
- Chemical exfoliant protocols are safe — begin with lower concentrations
- Laser treatment requires a test patch first — 2–3 sessions at lower fluence
- Nd:YAG 1064nm is the preferred laser (deeper wavelength = less epidermal thermal damage)
- PIH risk: moderate — monitor closely after any laser session
Dark/Deep Skin Tones (Fitzpatrick V–VI)
This is where the stakes are highest, and where the information gap is most dangerous.
- PIH risk from laser treatment is significant and must be explicitly discussed with your dermatologist before any procedure
- Topical-first approach is strongly recommended as the primary strategy
- Niacinamide + lactic acid combination addresses both KP bump reduction and hyperpigmentation simultaneously — a highly effective dual-mechanism approach for deeper skin tones
- Never agree to laser treatment without a formal Fitzpatrick skin typing assessment
According to the American Academy of Dermatology’s KP treatment guidelines, a personalized dermatologist-created treatment plan is essential — and this is especially true for patients with darker skin tones where procedure selection has direct safety implications.
⚡ What This Means For You: Your skin tone should be the first factor your dermatologist considers when building your KP treatment plan. If they haven’t mentioned PIH risk, ask about it directly.
How to Build a Daily Keratosis Pilaris Treatment Routine That Works
Consistency defeats intensity every time with KP. The right daily routine — applied correctly — outperforms aggressive treatment used haphazardly.
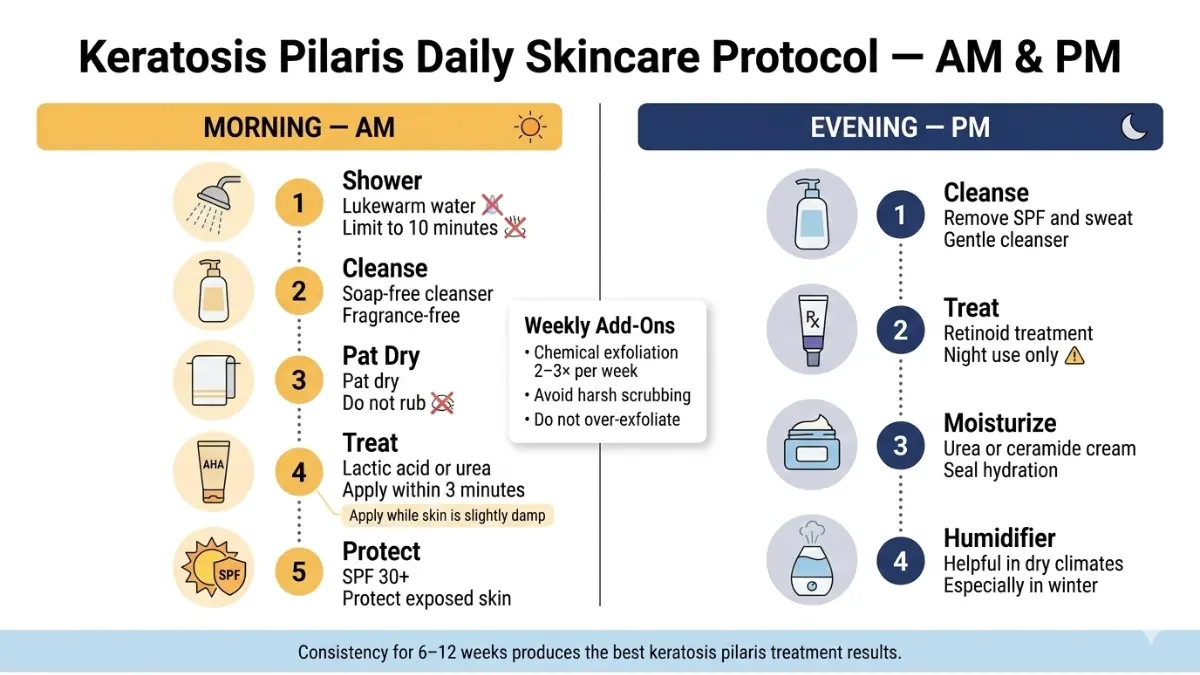
Morning Routine
- Shower in lukewarm water, max 10 minutes — hot water strips the skin’s natural lipid barrier, directly worsening KP
- Use a gentle, soap-free cleanser on affected areas (avoid fragrance, sulfates)
- Pat skin dry — do not rub
- Apply your lactic acid or urea treatment while skin is still slightly damp — absorption is 40% higher in the first 3 minutes post-bath
- Apply SPF 30+ sunscreen to exposed KP areas if going outside — UV exposure can worsen PIH in affected skin
Evening Routine
- Gentle cleanse to remove sunscreen, sweat, and environmental debris
- If using a prescription retinoid — apply at this step only (never morning)
- Wait 20 minutes, then apply urea-based or ceramide moisturizer as final step
- In dry winter months (especially relevant in northern US states, Canada, and UK): run a humidifier in your bedroom — low ambient humidity is a documented KP trigger
Weekly Protocol
- Chemical exfoliation 2–3× per week — not more; over-exfoliation inflames hair follicles and worsens KP
- Avoid physical scrubbing tools (loofahs, pumice stones) on active bumps — these cause microtrauma
- Dry-brush only on areas without active inflammation
Lifestyle Factors That Directly Affect KP
| Factor | Impact | Recommended Action |
|---|---|---|
| Hot showers | Worsens — strips skin oils | Keep ≤10 min, lukewarm temperature |
| Tight synthetic clothing | Worsens — friction inflames follicles | Choose breathable cotton or bamboo |
| Winter/low humidity | Worsens — moisture loss | Use bedroom humidifier |
| High psychological stress | May worsen inflammatory KP | Prioritize sleep and stress management |
| Diet (omega-3 fatty acids) | Limited but emerging evidence | Fatty fish, walnuts, flaxseed |
Skin health is inseparable from overall body health. Maintaining adequate hydration is foundational — use our Water Intake Calculator to determine your personalized daily fluid target based on your body weight and activity level.
For broader evidence-based skin and health strategies, explore our Health Tips hub which is updated regularly with physician-reviewed guidance.
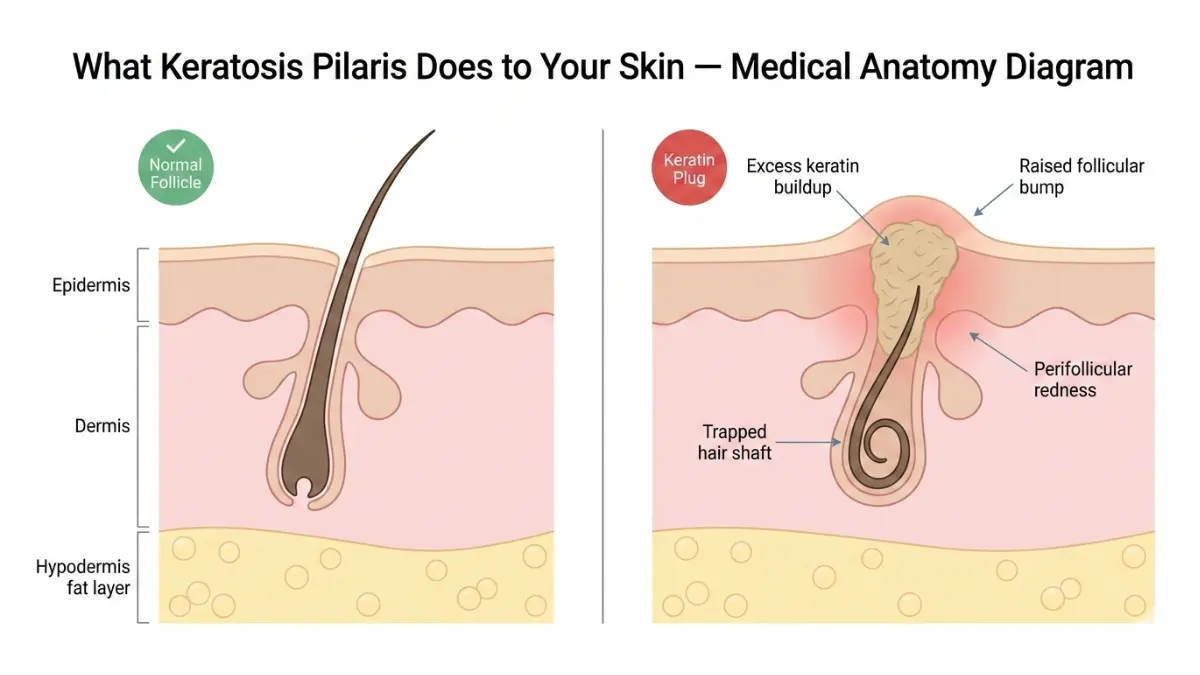
As MedlinePlus (NIH) confirms, keratosis pilaris is caused by keratin forming hard plugs within hair follicles — and managing the skin environment daily is the most sustainable long-term strategy for keeping those plugs clear.
KP and Mental Health — When to Stop Self-Treating and See a Doctor
Keratosis pilaris is classified as benign. But “benign” does not mean “without impact.”
A comprehensive 2024 review from the University of New South Wales and St George Hospital, Sydney — published in Clinical and Experimental Dermatology — confirmed that KP causes measurable psychosocial distress in a clinically significant proportion of patients. Cosmetic disfigurement on visible, exposed areas — particularly the arms, cheeks, and thighs — directly affects self-esteem, social confidence, and body image.
Priya, a 19-year-old university student from New Jersey, avoided short sleeves for three years. She hadn’t seen a dermatologist because she assumed KP was “just cosmetic and not serious enough.” By the time she was evaluated, she was eligible for a laser referral — a conversation that could have happened 18 months earlier.
Seeking clinical help for KP is always valid. The condition’s psychological impact is real and recognized in medical literature.
Red Flags — See a Dermatologist If:
- No visible improvement after 12 continuous weeks of correct OTC treatment
- KP bumps are red, inflamed, painful, or warm to the touch — this may indicate folliculitis overlap or KP rubra requiring different treatment
- KP appears on your face (cheeks) and is affecting your daily confidence or social interactions
- You are pregnant and considering any treatment beyond basic moisturization
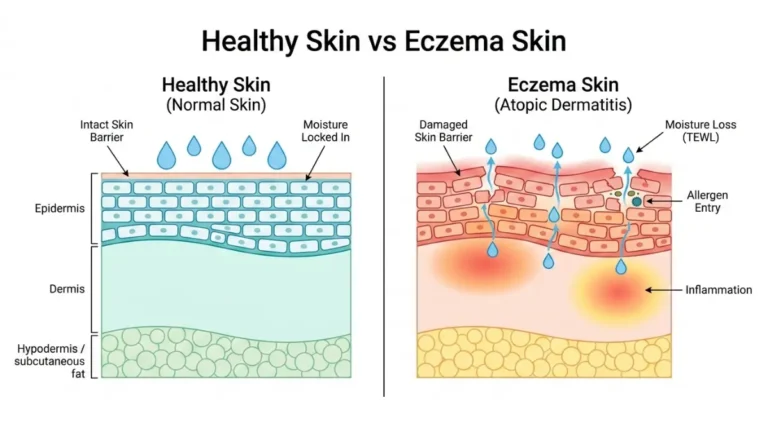
- KP appears alongside eczema flares — these conditions frequently co-occur and may require simultaneous management (see our related guide on eczema treatment for combined management strategies)
What to Expect at Your First Dermatology Appointment
- Diagnosis is visual — no biopsy or blood test needed in the vast majority of cases
- Your dermatologist will assess KP subtype (classic, rubra, atrophicans), location, severity, and skin tone
- Expect a written treatment protocol with clear timelines
- For resistant cases, a referral for laser evaluation may follow
Since KP follows an autosomal dominant inheritance pattern, it often runs in families. Understanding your genetic predisposition can be informative — our Genetic Risk Assessment Tool provides a starting framework for assessing hereditary skin and health conditions.
New Keratosis Pilaris Treatments in 2026 — What the Research Shows
This is where mymedicineadvisor.com goes further than every competitor. Mayo Clinic’s KP page cites no research from 2024 or 2025. Healthline’s treatment information references no clinical trials. What follows is the frontline of KP science — updated to March 2026.
Breakthrough #1: The Exfoliation-Dissolution-Repair Protocol (January 2026 RCT)
A randomized controlled trial published in January 2026 in PMC (Journal of Cosmetic Dermatology, Wiley Periodicals, approved by the Ethics Committee of Beijing Technology and Business University) evaluated a novel three-component formula in 60 KP volunteers over 28 days.
The protocol tested:
- A physical scrub containing olive shell powder, hydrated silica, and papain enzyme
- A moisturizing lotion with peony seed oil, oat kernel oil, and rice bran oil
Results at Day 28:
- Statistically significant reduction in follicular papule count vs. control group (p<0.05)
- Significant improvement in roughness and overall skin appearance scores (both physician-assessed and patient self-assessed)
- First RCT to validate a combined multi-mechanism approach — exfoliation + dissolution + skin repair — in a single prospective study
Why this matters: Every competitor’s article recommends a single product or single ingredient. This 2026 trial confirms that KP responds best to a layered, simultaneous attack on three mechanisms — exfoliation, keratin dissolution, and barrier restoration.
Breakthrough #2: Nd:YAG Laser Confirmed as Gold Standard (October 2025 Systematic Review)
The October 2025 systematic review published in the European Journal of Dermatology analyzed 27 peer-reviewed studies published between 2011 and 2024, making it the most comprehensive up-to-date synthesis of KP treatment evidence available.
Key findings:
- Lactic acid and glycolic acid confirmed as the most effective and well-tolerated topical agents
- Nd:YAG 1064nm laser yields consistently favorable outcomes across multiple study designs — the strongest evidence of any clinical procedure
- CO2 laser demonstrates efficacy for texture improvement
- Erbium:YAG laser is emerging as promising with a more favorable adverse effect profile than CO2
- The review proposes a stepwise, stratified therapeutic approach — aligned with the 4-step protocol outlined in Section 2 of this article
Breakthrough #3: Hyaluronic Acid as an Emerging Mechanism (December 2024 RCT)
A split-body, investigator-blinded randomized clinical trial published in December 2024 (Journal of Cosmetic Dermatology) evaluated a non-cross-linked hyaluronic acid compound for KP treatment. Results showed statistically significant improvements in roughness and redness scores versus the control side (p<0.05).
This represents a new moisturizing mechanism beyond traditional urea and lactic acid — particularly relevant for patients who experience irritation from AHA/BHA products.
Where KP Research Is Heading in 2026 and Beyond
- Microbiome-targeted treatments — emerging research explores the role of skin microbiome dysregulation in KP severity
- At-home LED and photobiomodulation devices — consumer-grade light therapy devices being studied for KP maintenance between clinical laser sessions
- Personalized topical formulations — compounding pharmacies increasingly offering customized AHA + urea + retinoid blends matched to patient skin type and KP severity
⚡ What This Means For You: If your current keratosis pilaris treatment hasn’t worked, 2026 research confirms that a combination approach — exfoliation + dissolution + repair — consistently outperforms any single-product strategy. Present this evidence to your dermatologist and ask about multimodal treatment planning.
For patients dealing with related skin conditions that may co-occur with KP, our guides on psoriasis treatment and microneedling for skin texture provide additional clinically reviewed options.
Frequently Asked Questions About Keratosis Pilaris Treatment
1: Does keratosis pilaris go away on its own?
KP often improves naturally after puberty and tends to fade with age in many patients. However, StatPearls/NCBI data confirms that 43% of patients have persistent symptoms into adulthood without treatment. Consistent keratosis pilaris treatment significantly accelerates clearing.
2: What is the #1 dermatologist-recommended treatment for KP?
Topical lactic acid is the most widely used first-line keratosis pilaris treatment, selected by 43.6% of board-certified dermatologists in a 2023 ODAC Conference survey. Salicylic acid (20.7%) and urea-based creams follow closely.
3: How long does keratosis pilaris treatment take to work?
OTC treatments like lactic acid typically require 6–12 weeks of consistent daily use. Prescription retinoids show results in 4–8 weeks. Laser therapy requires 3–6 sessions spaced 4–6 weeks apart. No treatment produces overnight results.
4: Can keratosis pilaris be permanently cured?
There is no permanent cure for KP at this time. Treatment keeps bumps minimal and skin smooth, but discontinuing treatment usually allows KP to return. Think of it as ongoing management, not a one-time fix.
5: Is keratosis pilaris treatment safe during pregnancy?
Gentle moisturizers and low-concentration urea creams are generally considered safe. Topical retinoids (tazarotene, tretinoin) must be strictly avoided during pregnancy due to teratogenic risk. Always discuss all skincare treatments with your OB/GYN before use.
6: What ingredients should I look for in KP creams?
The most evidence-backed active ingredients are lactic acid, glycolic acid, urea, and salicylic acid — all keratolytics that dissolve the excess keratin blocking hair follicles. Ceramides and niacinamide support barrier repair alongside exfoliation.
7: Does diet affect keratosis pilaris?
Clinical evidence for dietary effects on KP is limited. Some research suggests omega-3 fatty acids (found in fatty fish, walnuts, flaxseed) may support skin barrier integrity. No specific diet has been proven to cure KP, but overall nutritional health supports skin health broadly.
8: Can children use keratosis pilaris treatments?
Gentle, low-concentration moisturizers and urea-based creams are generally safe for children with pediatrician guidance. Prescription retinoids and laser therapy require dermatologist supervision for patients under 12. Always confirm ingredient safety for pediatric use before application.
9: Is keratosis pilaris the same as acne?
No. KP is caused by excess keratin plugging hair follicles — not by bacteria, sebum, or hormonal acne pathways. KP bumps are not infected pimples. Standard acne treatments (benzoyl peroxide, antibiotics) are not effective for KP and may worsen skin irritation.
10: What is KP rubra and does it need different treatment?
KP rubra is a subtype characterized by significant redness and inflammation around the bumps, often appearing on the cheeks and upper arms. It typically requires anti-inflammatory treatment alongside standard keratolytics — including pulsed dye laser or off-label topical sirolimus (supported by 2025 JAAD case reports).
11: When should I see a doctor about keratosis pilaris?
See a board-certified dermatologist if bumps haven’t improved after 12 weeks of consistent OTC treatment, if they are painful or inflamed, if they appear on your face, or if they are significantly affecting your confidence or daily life. Early escalation to clinical treatment produces better long-term outcomes.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.