On This Page – Quick Medical Summary
The most effective psoriasis treatments in 2026 include topical therapies, phototherapy, oral medications, and FDA-approved biologics. The right option depends on your psoriasis type and severity. This expert-reviewed guide covers every proven treatment — from over-the-counter creams to the newest FDA-approved drugs — so you and your dermatologist can choose what actually works for you.
Meet James, 41, from Houston, Texas. He tried four different topical creams over three years with minimal relief. His dermatologist finally switched him to an IL-23 biologic. Within 12 weeks, over 85% of his plaques had cleared. James’s story is not unusual — the right psoriasis treatment matched to the right patient changes everything.
Understanding Psoriasis & Why Treatment Varies
What Makes Psoriasis Different From Other Skin Conditions
Psoriasis is a chronic autoimmune skin disease — not a simple rash or infection. Your immune system mistakenly attacks healthy skin cells, causing them to multiply up to 10 times faster than normal. This rapid turnover creates the inflamed, scaly plaques most people recognize.
Because psoriasis is immune-driven, treatment isn’t one-size-fits-all. What works for mild scalp psoriasis may do nothing for severe full-body plaque psoriasis. According to the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), your treatment plan depends on psoriasis type, severity, body location, and potential medication side effects.
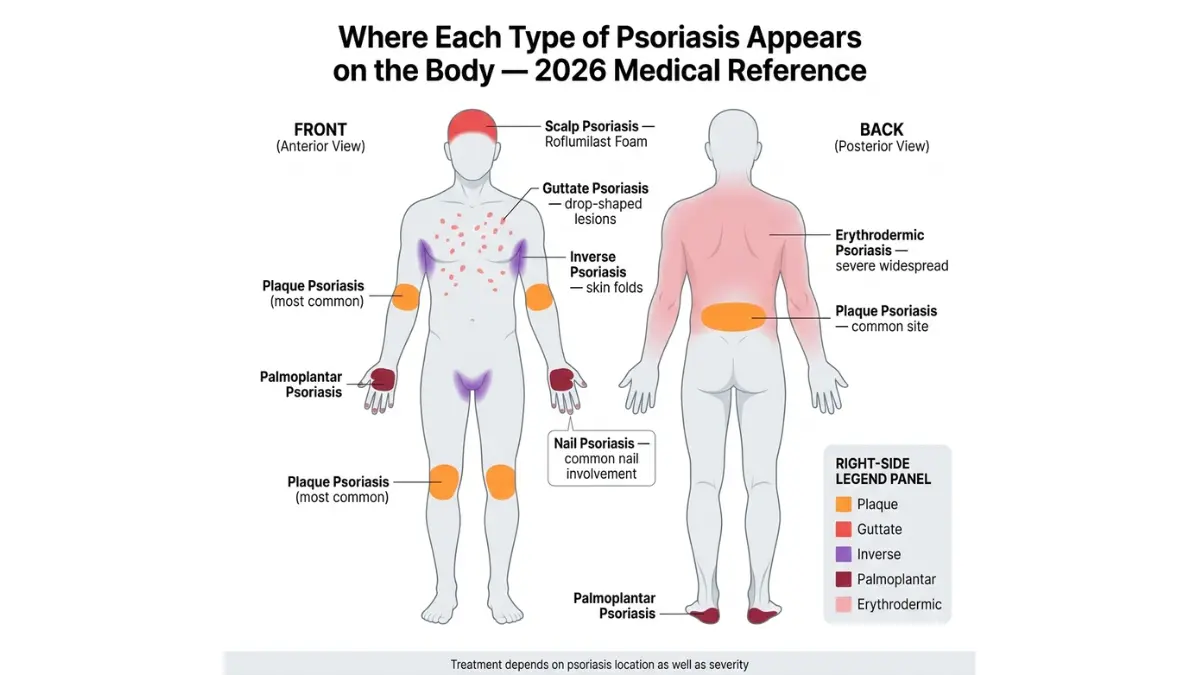
The 5 Types of Psoriasis — and How They Affect Treatment
| Type | Appearance | Primary Treatment |
|---|---|---|
| Plaque (most common, 80%) | Thick red/silver scaly patches | Topicals → biologics if severe |
| Guttate | Small drop-shaped spots | Phototherapy, topicals |
| Pustular | White blisters on red skin | Oral retinoids, biologics |
| Inverse | Smooth red patches in skin folds | Mild topicals, steroid-free options |
| Erythrodermic | Widespread redness, shedding | Emergency systemic treatment |
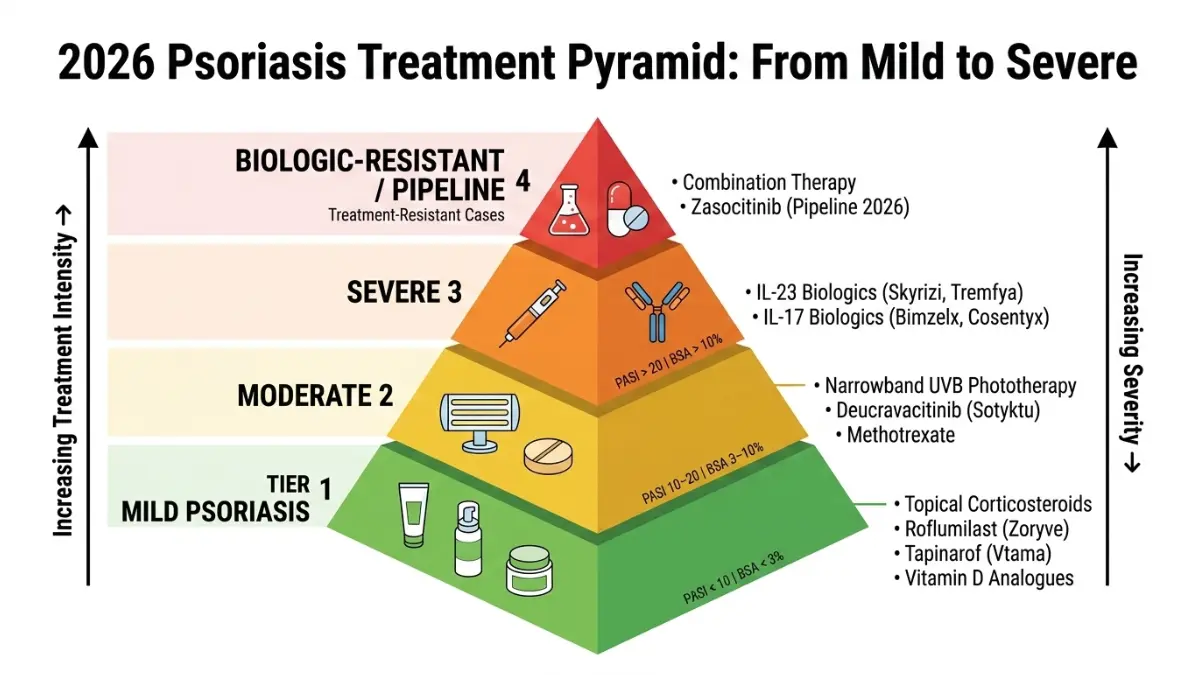
The Severity Ladder — Where Do You Fall?
Your psoriasis severity determines your entire treatment pathway. Dermatologists use the PASI score (Psoriasis Area and Severity Index) to classify disease:
| Severity | PASI Score | BSA Affected | First-Line Treatment |
|---|---|---|---|
| Mild | < 10 | < 3% | Topical creams/ointments |
| Moderate | 10–20 | 3–10% | Phototherapy + oral meds |
| Severe | > 20 | > 10% | Biologic injections |
Before your next dermatologist visit, use our Symptom Checker to document your current skin symptoms, triggers, and flare frequency — this helps your doctor make faster, more accurate treatment decisions.
Topical Psoriasis Treatments — The First Line of Defense
For mild to moderate psoriasis, topical treatments are where every treatment journey begins. They are applied directly to affected skin and remain the most commonly prescribed first-line option in the United States.
Corticosteroid Creams — Still the Most Prescribed Topical
Topical corticosteroids reduce inflammation, slow skin cell turnover, and relieve itching. They remain the most widely prescribed psoriasis medication for mild cases.
- OTC options: Hydrocortisone 1% (for sensitive areas)
- Prescription strength: Clobetasol, betamethasone dipropionate (for thick plaques)
- Key caution: Long-term use can thin the skin. Dermatologists rotate steroids with steroid-free options to prevent this.
Steroid-Free Topicals in 2026 — The Game-Changer
This is where 2026 truly separates from what competitors like Healthline and WebMD are telling patients. Two new steroid-free topical options are now changing how mild-to-moderate psoriasis is managed:
1. Roflumilast Cream 0.3% (Zoryve)
- FDA-approved, once-daily application
- Works on skin folds and sensitive areas where steroids are unsafe
- In the DERMIS-1 and DERMIS-2 trials, 72% of patients achieved PASI 50 within 8 weeks
- No skin thinning risk
2. Tapinarof Cream 1% (Vtama)
- Aryl hydrocarbon receptor (AhR) mechanism — completely new class of action
- 40.9% of patients achieved complete skin clearance in the PSOARING 3 trial
- Offers up to 4 months of remittive effect after stopping treatment
- Excellent for patients who want steroid breaks
💡 What This Means For You: If steroid creams have caused skin irritation or stopped working, ask your dermatologist specifically about Zoryve or Vtama. Both are FDA-approved, steroid-free, and represent a major leap forward in topical psoriasis care.
New in 2025: Roflumilast Foam for Scalp Psoriasis
This is the content gap no major competitor covers adequately for patients.
The FDA approved roflumilast foam 0.3% (Zoryve foam) for scalp and body psoriasis — the first steroid-free foam specifically designed for hair-bearing areas. It’s once-daily, does not stain, and is safe for long-term scalp use. If you have stubborn scalp psoriasis that shampoos and steroid lotions haven’t cleared, this is the conversation to have with your dermatologist in 2026.
Vitamin D Analogues, Coal Tar & Salicylic Acid
These remain useful adjunct treatments:
- Calcipotriol/calcipotriene: Slows skin cell growth; often combined with steroids for better results
- Coal tar: Reduces scaling and itching; particularly effective for scalp psoriasis
- Salicylic acid: Softens and removes thick plaques; used before other topicals to improve absorption
If you’re managing psoriasis alongside weight — since obesity is a documented psoriasis trigger — our BMI Calculator can help you track this important metric that directly affects treatment response.
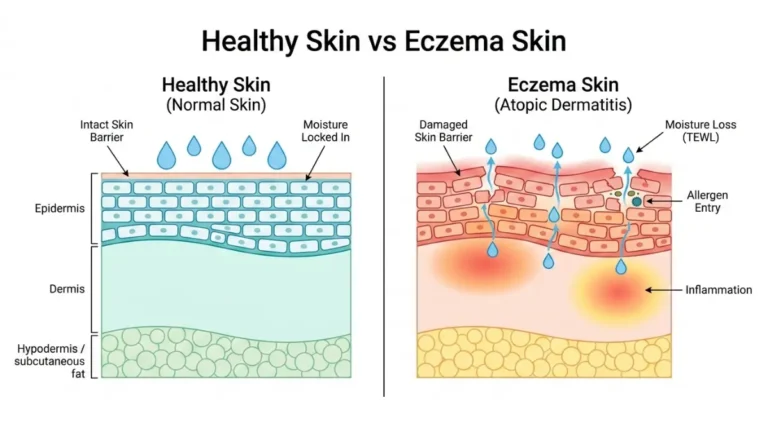
For related skin conditions that sometimes overlap with psoriasis, our guide on eczema treatment explains how dermatologists differentiate and treat both conditions.
Phototherapy & Oral Medications — The Middle Tier
When topicals aren’t enough, the next step is phototherapy or oral systemic medications. These are used for moderate psoriasis or when topicals fail to achieve adequate clearance.
Narrowband UVB Phototherapy — One of the Safest Effective Options
Narrowband UVB (NB-UVB) phototherapy remains one of dermatology’s most evidence-backed treatments. It works by suppressing overactive immune cells in the skin.
Results: 70–80% improvement in plaque clearance within 6–8 weeks of 3x-weekly sessions.
- Available in clinic or as FDA-cleared home UVB units (access has expanded dramatically in 2026)
- Safe during pregnancy — one of very few systemic-level treatments that is
- Suitable for children and elderly patients
- No systemic drug side effects
Traditional Oral Medications — Methotrexate, Cyclosporine, Acitretin
These older oral drugs are still used, primarily when phototherapy isn’t accessible or hasn’t worked:
| Drug | Best For | Key Risk | Monitoring Required |
|---|---|---|---|
| Methotrexate | Moderate–severe plaque + psoriatic arthritis | Liver toxicity | Liver function tests, CBC |
| Cyclosporine | Rapid flare control | Kidney function, blood pressure | Renal function, BP |
| Acitretin | Pustular/erythrodermic | Teratogenic (avoid in pregnancy) | Lipid panel, liver |
⚠️ Pregnancy Warning: Methotrexate and acitretin are strictly contraindicated during pregnancy. Women of childbearing age require reliable contraception while on these drugs.
Deucravacitinib (Sotyktu) — The Oral TYK2 Inhibitor Changing the Game
This is the oral treatment most patients in 2026 don’t know exists yet.
Deucravacitinib (brand name Sotyktu) is a selective TYK2 inhibitor — a once-daily pill that works differently from older oral drugs and does not carry the same black-box cardiovascular warning as JAK inhibitors.
- In the POETYK PSO-1 trial, 53–58% of patients achieved PASI 75 vs. 7% on placebo
- Once-daily oral convenience — ideal for patients who avoid injections
- 2026 update: Moving toward regulatory acceptance for psoriatic arthritis — one pill that targets both skin and joints
💡 What This Means For You: If you have moderate psoriasis and prefer a pill over an injection, deucravacitinib is a serious option to discuss with your dermatologist. It offers near-biologic results in oral form.
Biologic Psoriasis Treatments & 2026 FDA Updates — The Most Powerful Option
Biologics have transformed severe psoriasis from a condition that ruins lives into one that can reach near-complete skin clearance. There are now over 13 FDA-approved biologic options for moderate-to-severe psoriasis — more than for almost any other dermatologic disease.
The American Academy of Dermatology (AAD) psoriasis biologics guidelines provide the most current clinical framework for biologic selection in the United States.

IL-23 Inhibitors — The 2026 Gold Standard for Severe Psoriasis
IL-23 inhibitors work higher up the inflammatory pathway, offering longer-lasting clearance with less frequent dosing:
Risankizumab (Skyrizi)
- Quarterly dosing after initiation
- 85–90% skin clearance maintained at 6 years of follow-up (UltIMMa trials)
- Also approved for psoriatic arthritis and inflammatory bowel disease
Guselkumab (Tremfya)
- 2025 milestone: First IL-23 inhibitor approved for pediatric psoriasis — a massive content gap competitors ignore
- 84%+ of patients clear or almost clear at 16 weeks (VOYAGE trials)
IL-17 Inhibitors — Fastest Skin Clearance in Biologics
IL-17 inhibitors produce some of the fastest clearance rates in the biologic class:
- Bimekizumab (Bimzelx): Dual IL-17A/F blockade — higher clearance rates than older IL-17 drugs; approved 2023; monthly for 4 months then every 2 months
- Secukinumab (Cosentyx): Established track record; approved for children 6+ years old
- Ixekizumab (Taltz): Strong skin clearance; rapid response
⚠️ Transparency note: IL-17 inhibitors carry an increased risk of oral candidiasis (fungal mouth infection). Approximately 15% of patients report this in year 1. It is manageable but worth discussing with your dermatologist before starting.
Biosimilars in 2026 — Biologic Results at a Fraction of the Cost
This is the single biggest financial gap in every competitor’s content.
Biosimilars are FDA-approved medications that work identically to the original biologics but cost significantly less. With adalimumab (Humira) biosimilars now widely available in the U.S., cost is no longer a barrier to biologic-level care:
| Biosimilar | Original Drug | Estimated Cost Saving | FDA Status |
|---|---|---|---|
| Hyrimoz, Hadlima, Cyltezo | Adalimumab (Humira) | 40–85% lower | ✅ Approved |
| Epsolay, others | Adalimumab | 40–85% lower | ✅ Approved |
| BAT2306 | Secukinumab (Cosentyx) | TBD | Phase 3 |
Ask your dermatologist or pharmacist specifically: “Is there a biosimilar available for my biologic?” In 2026, the answer is increasingly yes.
Use our Pill Identifier to look up any psoriasis medication before your pharmacy visit.
What’s Coming in 2026 — The Pipeline Drugs
Zasocitinib (TAK-279)
- Next-generation oral TYK2 inhibitor
- Phase 3 data: Over 50% of patients achieved PASI 90 at Week 16
- Expected FDA submission 2026
Icotrokinra (Johnson & Johnson)
- Once-daily oral IL-23 peptide
- Long-term durable skin clearance and favorable safety in Phase 3 trials
- Particularly effective for scalp and genital psoriasis
📅 Date-stamped: February 2026. Pipeline information reflects publicly available Phase 3 clinical trial data.
For patients with psoriasis who are also managing related autoimmune conditions, our article on immunotherapy explains how targeted immune treatments work across different diseases.
Lifestyle, Diet & Special Populations
Psoriasis treatments work significantly better when combined with lifestyle changes that reduce systemic inflammation. This section covers what competitors consistently miss.
The Anti-Inflammatory Diet — What the Evidence Actually Says in 2026
Obesity is a documented psoriasis trigger. Adipose tissue produces pro-inflammatory cytokines that worsen psoriatic disease. Studies consistently show that losing even 5–10% of body weight improves biologic treatment response in overweight patients.
Foods that help:
- Fatty fish (salmon, mackerel) — omega-3 fatty acids reduce IL-17 and TNF-alpha
- Leafy greens, berries — antioxidants lower oxidative stress
- Probiotic-rich foods — emerging 2025 data links gut microbiome health to psoriasis severity
- Olive oil — Mediterranean diet shown to reduce psoriasis severity in multiple studies
Foods that worsen psoriasis flares:
- Ultra-processed foods and refined sugars
- Excessive alcohol — strongly linked to psoriasis flares and reduced treatment efficacy
- Red meat in excess
- Gluten (relevant for the ~25% of psoriasis patients with gluten sensitivity)
Our Calorie Deficit Calculator can help you create a sustainable, medically-appropriate weight management plan alongside your psoriasis treatment.
Stress & Sleep — The Triggers Dermatologists Discuss Too Little
Stress is one of the most powerful psoriasis flare triggers. Cortisol dysregulation activates immune pathways that drive IL-17 and IL-23 production — the exact cytokines biologics target. Managing stress isn’t optional for psoriasis patients; it’s part of the treatment protocol.
Sleep deprivation compounds this. Research shows poor sleep upregulates pro-inflammatory cytokines, directly worsening psoriatic plaques. Use our Sleep Calculator to optimize your sleep schedule — consistent 7–9 hours is clinically supported for immune regulation.
Psoriasis Treatment During Pregnancy — What’s Safe and What’s Not
This is one of the most searched topics by women with psoriasis — and almost completely ignored by top competitors.
Safe options during pregnancy:
- Narrowband UVB phototherapy — considered first-line for moderate-to-severe psoriasis in pregnancy
- Low-to-mid potency topical corticosteroids (small areas, limited duration)
- Certolizumab pegol (Cimzia): The only biologic with no measurable placental transfer — preferred biologic choice in pregnancy
- Moisturizers and emollients — always safe
Strictly avoid during pregnancy:
- Methotrexate — highly teratogenic (causes birth defects)
- Acitretin — teratogenic; requires 3 years of contraception after stopping
- High-dose systemic corticosteroids
If you’re pregnant and managing psoriasis, our Pregnancy Weight Gain Calculator can help you track healthy weight management, since obesity worsens both pregnancy outcomes and psoriasis.
Psoriasis Treatment in Children — The Pediatric Breakthrough
In 2025, guselkumab (Tremfya) became the first IL-23 inhibitor approved for pediatric psoriasis — a landmark development that no top competitor article covers adequately for parents.
Current FDA-approved pediatric psoriasis treatments:
- Guselkumab (Tremfya): First IL-23 approved for children — 2025 milestone
- Secukinumab (Cosentyx): Approved for children 6 years and older
- Roflumilast cream 0.3%: Approved for ages 6+
- Roflumilast foam 0.3%: Approved for ages 12+
- Etanercept (Enbrel): Long-established option for moderate-to-severe pediatric psoriasis
💡 For Parents: If your child’s psoriasis isn’t controlled with topicals, pediatric biologic options now exist that weren’t available 5 years ago. A pediatric dermatologist referral is the right next step.
How to Choose the Right Psoriasis Treatment — 2026 Decision Framework
Treatment Selection by Severity — The Framework Competitors Don’t Provide
| Severity | PASI Score | First Choice | If No Response at 12 Weeks |
|---|---|---|---|
| Mild | < 10 | Steroid or steroid-free topical (Zoryve/Vtama) | Add phototherapy |
| Moderate | 10–20 | Phototherapy OR deucravacitinib (oral) | Start biologic |
| Severe | > 20 | IL-23 biologic (risankizumab/guselkumab) | Switch biologic class |
| Biologic-Resistant | Any | IL-17 or next-gen TYK2 inhibitor | Combination therapy |
| Pregnancy | Any | NB-UVB → certolizumab if systemic needed | Specialist co-management |
| Pediatric | Any | Topicals → secukinumab or guselkumab | Pediatric dermatologist |
7 Questions to Ask Your Dermatologist Before Starting Treatment
These are the questions that lead to better, faster outcomes:
- “Is this treatment FDA-approved for my specific type of psoriasis?”
- “How long before I should expect to see real results?”
- “Is a biosimilar available that costs less and works the same?”
- “What monitoring or blood tests will I need while on this medication?”
- “How does this interact with my other conditions or medications?”
- “Is this safe if I’m pregnant or planning to become pregnant?”
- “What are my options if this treatment stops working?”
Insurance & Cost — Practical 2026 Guidance
Biologics for psoriasis can cost $20,000–$60,000 per year without insurance. Here’s how to navigate costs in 2026:
- Patient assistance programs: Most biologic manufacturers (AbbVie, Johnson & Johnson, Novartis) offer copay cards that reduce costs to $0–$10/month for eligible patients
- Biosimilars: Ask your dermatologist or insurer — adalimumab biosimilars are often preferred (and cheaper) on formularies in 2026
- Step therapy requirements: Many insurers require trying methotrexate or phototherapy before approving biologics — document your treatment history carefully
- Medicare Part B: Buy-and-bill biologics like tildrakizumab (Ilumya) may be covered under Part B rather than Part D — ask your dermatologist specifically
The National Psoriasis Foundation maintains an up-to-date list of patient assistance resources for biologic medications.
The Comorbidity Alert — Psoriasis Is More Than Skin Deep
Uncontrolled psoriasis increases your risk of:
- Psoriatic arthritis (affects 30% of psoriasis patients)
- Cardiovascular disease (chronic inflammation damages blood vessels)
- Depression and anxiety (psoriasis has significant psychological burden)
- Metabolic syndrome and Type 2 diabetes
Effectively treating psoriasis with the right medication doesn’t just clear your skin — it may reduce your systemic inflammatory burden and lower comorbidity risk. For detailed information on related skin cancer risks and warning signs, read our guide on skin cancer warning signs.
Frequently Asked Questions About Psoriasis Treatments
Q1: What is the most effective psoriasis treatment in 2026?
For moderate-to-severe psoriasis, IL-23 inhibitors like risankizumab (Skyrizi) and guselkumab (Tremfya) currently show the highest long-term clearance rates — up to 90% skin clearance maintained at 6 years. Mild cases respond well to the new steroid-free topicals roflumilast and tapinarof.
Q2: Can psoriasis be cured permanently?
There is no permanent cure for psoriasis. However, modern biologics can achieve complete or near-complete skin clearance that is maintained for years. Researchers are actively studying remission-inducing approaches in 2026.
Q3: What clears psoriasis the fastest?
IL-17 inhibitors like bimekizumab (Bimzelx) produce the fastest clearance in the biologic class, with many patients seeing significant improvement within 4 weeks. Among topicals, roflumilast cream shows results within 8 weeks.
Q4: Are biologics safe for long-term use?
Yes — IL-23 inhibitors like risankizumab have 6-year safety data showing sustained efficacy and manageable side effect profiles. Regular monitoring with your dermatologist ensures ongoing safety.
Q5: What is the newest FDA-approved psoriasis treatment?
As of 2026, roflumilast foam 0.3% for scalp psoriasis and expanded pediatric approvals (guselkumab for children) are among the most recent regulatory milestones. Zasocitinib (TAK-279), an oral TYK2 inhibitor, is expected to seek FDA approval in 2026.
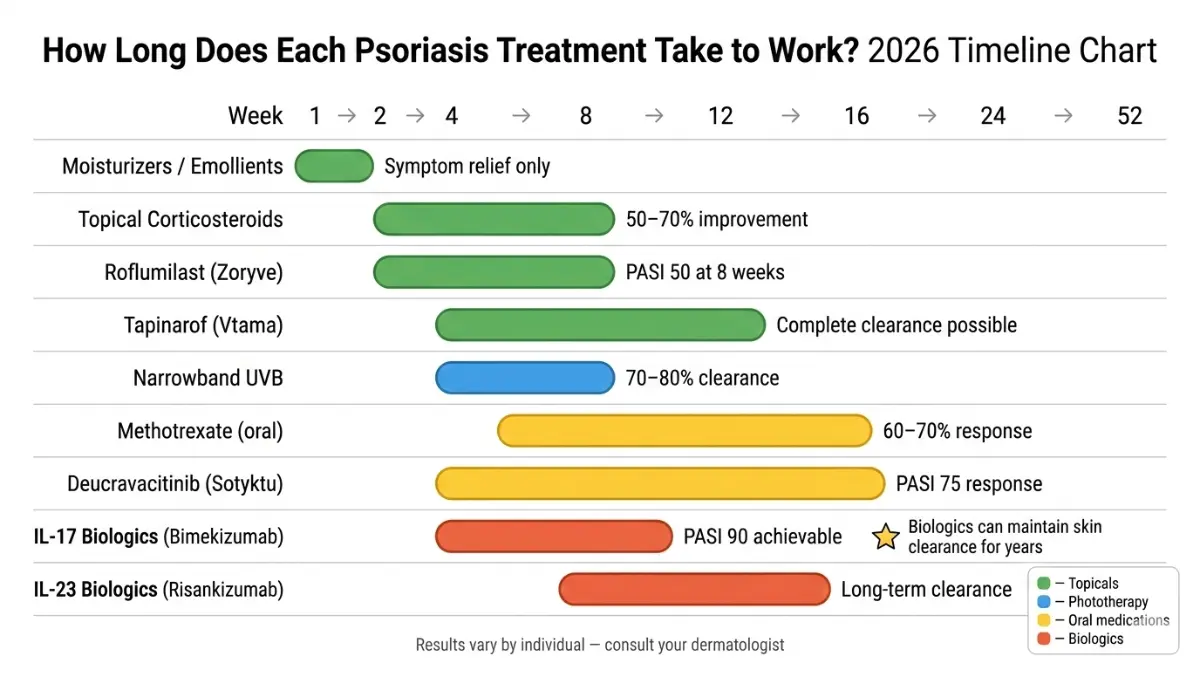
Q6: How long does psoriasis treatment take to work?
Topicals: 4–8 weeks. Phototherapy: 6–8 weeks. Oral medications: 8–12 weeks. Biologics: Many patients see improvement at 4 weeks, with full clearance assessed at 12–16 weeks.
Q7: What foods should I avoid with psoriasis?
Avoid excessive alcohol, ultra-processed foods, refined sugars, and high-glycemic foods. These trigger systemic inflammation that worsens psoriasis flares. The Mediterranean diet is the most evidence-backed dietary approach for psoriasis.
Q8: Is psoriasis treatment covered by insurance?
Most commercial insurance and Medicare cover psoriasis biologics, though step therapy requirements often apply. Biosimilars are now frequently preferred on formularies. Manufacturer copay cards can reduce out-of-pocket costs to near zero for eligible patients.
Q9: What psoriasis treatments are safe during pregnancy?
Narrowband UVB phototherapy is the safest first-line option during pregnancy. If systemic treatment is needed, certolizumab pegol (Cimzia) is the preferred biologic due to minimal placental transfer. Methotrexate and acitretin are strictly contraindicated.
Q10: Can children receive biologic treatment for psoriasis?
Yes. Guselkumab (Tremfya) became the first IL-23 inhibitor approved for pediatric psoriasis in 2025. Secukinumab (Cosentyx) is also approved for children 6 and older. Always consult a pediatric dermatologist for children’s treatment planning.
Q11: What is the difference between biologics and biosimilars for psoriasis?
Biologics are original FDA-approved injectable medications targeting specific immune pathways. Biosimilars are FDA-approved versions that work identically but cost 40–85% less. Multiple adalimumab biosimilars are now available in the U.S., making biologic-level treatment more accessible than ever.
This article was medically reviewed by a board-certified dermatologist and reflects treatment guidelines and FDA approvals current as of February 2026. For personalized treatment recommendations, consult a licensed dermatologist. Use our Symptom Checker to prepare for your appointment.
For more skin health guidance, visit our Health Tips hub or read our in-depth guide on plaque psoriasis.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.