On This Page – Quick Medical Summary
Yes — complete skin clearance from plaque psoriasis is now a documented, achievable outcome in 2026, not just a distant hope. New FDA-approved biologics achieve full skin clearance (PASI 100) in 40–60% of patients. Here is exactly what causes it, what the latest treatments can do, and what you should ask your doctor today.
⚕️ Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified, licensed healthcare professional for diagnosis and treatment.
What Is Plaque Psoriasis?
The Most Common Skin Condition You May Be Misreading
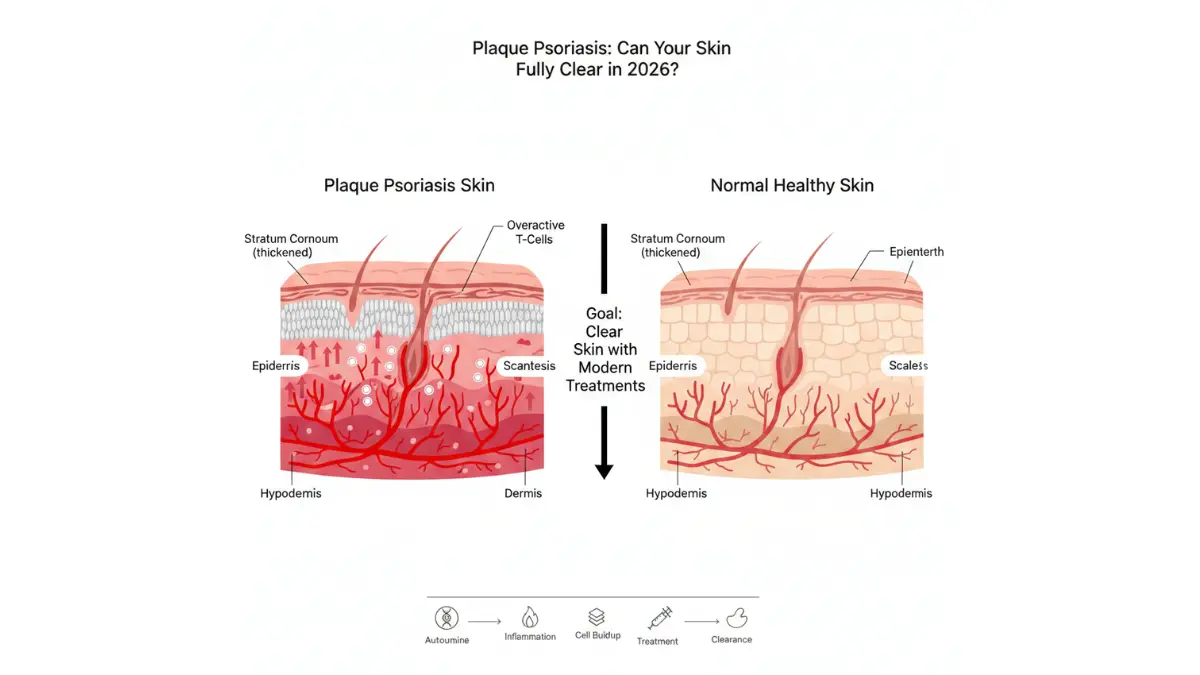
Plaque psoriasis — also called psoriasis vulgaris — is a chronic, immune-mediated inflammatory skin disorder that causes well-defined, raised patches covered with silvery-white scales. It accounts for 80–90% of all psoriasis cases and affects approximately 8 million Americans and 125 million people worldwide, according to JAMA’s landmark 2020 review.
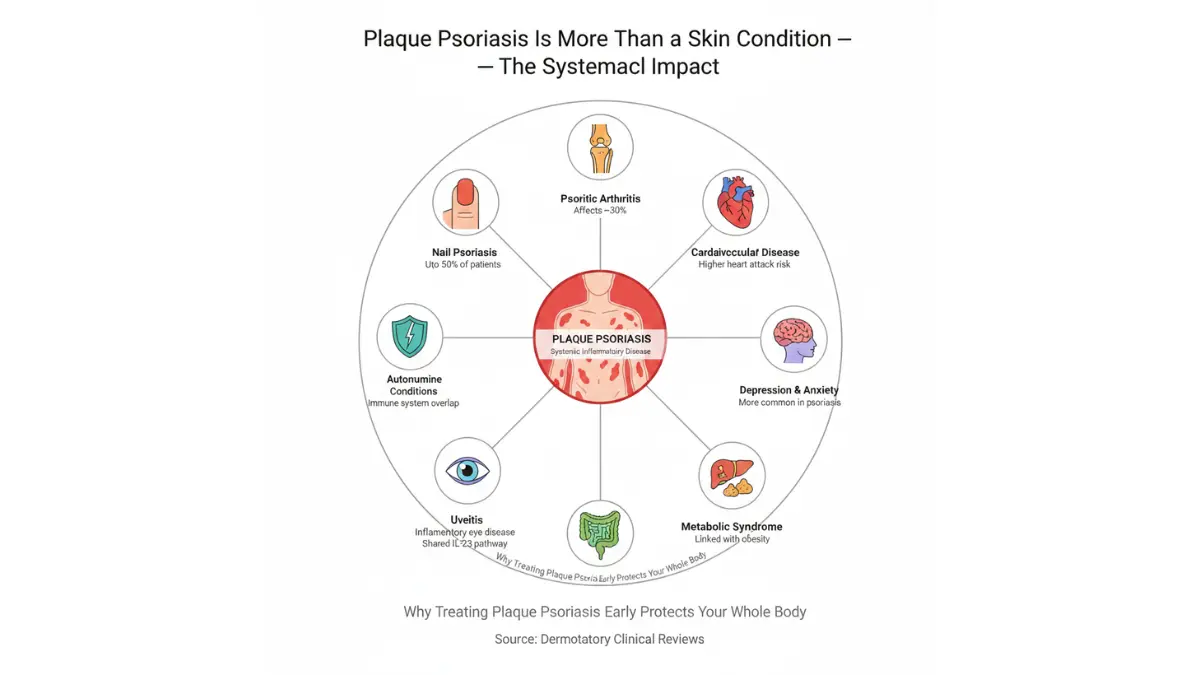
It is not a surface-level skin problem. At its root, plaque psoriasis is an autoimmune disease — your immune system mistakenly accelerates skin cell production, causing new cells to pile up 10x faster than normal.
How It Looks — On Every Skin Tone
Most articles describe psoriasis only on light skin. That’s a gap we’re closing:
| Skin Tone | Plaque Color | Scale Color |
|---|---|---|
| Light / Fair | Pink to red | Silvery-white |
| Medium / Olive | Salmon or coral | Silver-white |
| Dark / Deep | Dark brown or violet | Gray |
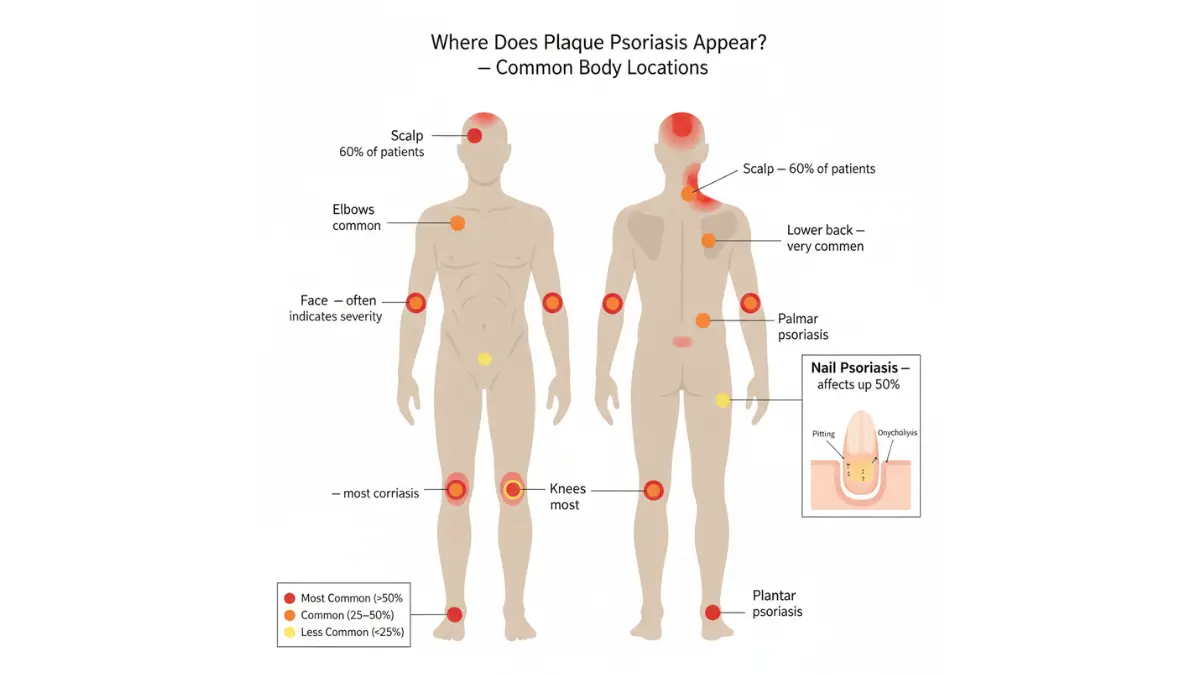
Plaques are usually symmetrical — if you have them on your left knee, they often appear on your right knee too. Common locations include the elbows, knees, scalp, lower back, and skin folds.
If you’re unsure whether your patches are plaque psoriasis, eczema, or another skin condition, our Symptom Checker can help you assess your symptoms before your next appointment.
Mild, Moderate, or Severe — Know Your Level
| Severity | Body Surface Area (BSA) | PASI Score | Typical First Step |
|---|---|---|---|
| Mild | Less than 5% | Below 7 | Topical creams |
| Moderate | 5–10% | 7–12 | Phototherapy + topicals |
| Severe | More than 10% | Above 12 | Biologics or systemic agents |
About 80% of cases are mild to moderate. The remaining 20% — severe disease — are the patients who benefit most dramatically from 2026’s biologic revolution.
What Causes Plaque Psoriasis? Root Causes + 2026 Trigger Intelligence
The Immune System Malfunction Behind Every Flare
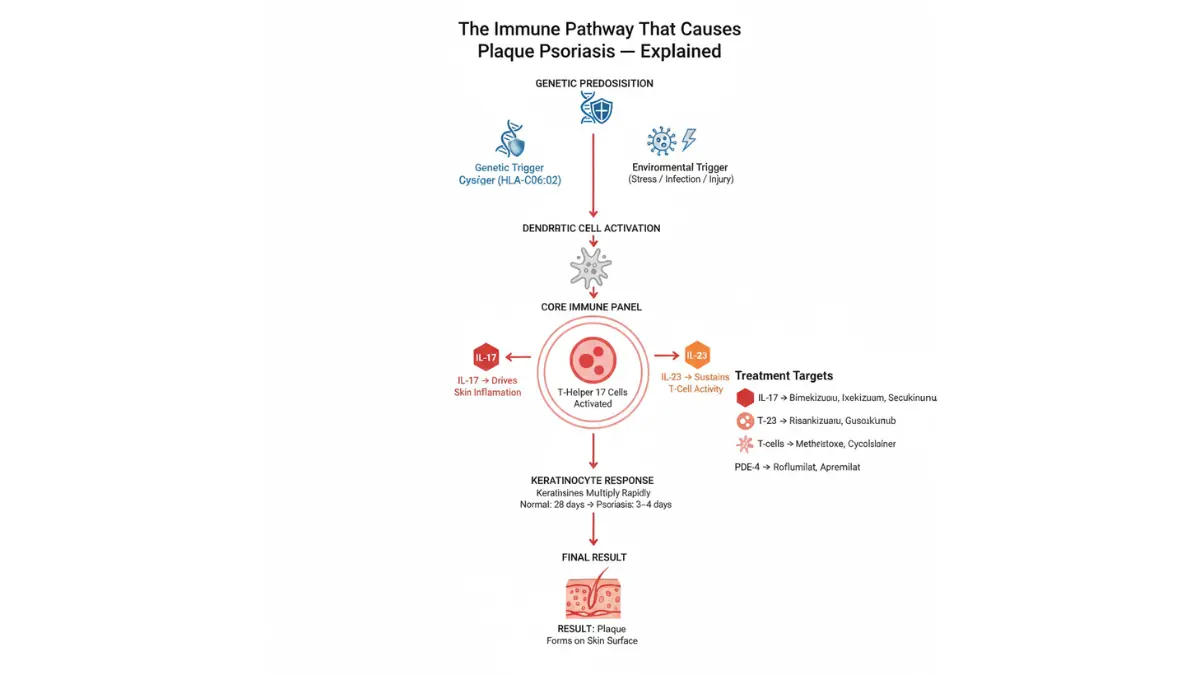
Plaque psoriasis begins deep in your immune system. Normally, T-cells (white blood cells) fight infection. In psoriasis, they mistakenly attack healthy skin cells, triggering an inflammatory cascade driven by two key proteins: interleukin-17 (IL-17) and interleukin-23 (IL-23).
This immune misfire tells your skin to produce new cells every 3–4 days instead of the normal 28–30 days. Dead cells pile up into the thick, scaly plaques that define the condition.
Genetics plays a critical role — if a first-degree relative has psoriasis, your risk rises significantly. According to StatPearls (NCBI), the HLA-C*06:02 genetic variant shows the strongest known association with early-onset plaque psoriasis.
2026 Trigger Intelligence: What’s Making It Worse
New in 2025: A landmark study found that people with a genetic predisposition to psoriasis who live in high air-pollution areas face a compounded — not just added — risk of developing the condition. This gene-environment interaction is something Healthline, WebMD, and Mayo Clinic have not yet addressed.
Other evidence-backed triggers:
- Stress — the #1 self-reported flare trigger in US patients
- Strep throat infections — directly linked to guttate flare-ups that can evolve into plaque disease
- Medications — beta-blockers, lithium, and NSAIDs are documented triggers
- Alcohol and smoking — both worsen severity and reduce biologic effectiveness
- Skin injury — the Koebner phenomenon (new plaques form at injury sites)
- Obesity — excess adipose tissue increases systemic inflammation
What This Means For You: Body weight has a direct, measurable impact on psoriasis severity. Research shows that losing even 5–10% of body weight can reduce flare frequency. Use our BMI Calculator to understand whether your weight may be amplifying your skin inflammation.
Plaque Psoriasis Symptoms — The Full Picture Most Articles Skip
Beyond the Rash: What Plaque Psoriasis Actually Feels Like
Most articles list visual symptoms and stop there. Patients live with far more:
Skin Symptoms:
- Raised, inflamed patches with thick silvery or gray scale
- Intense itching — described by patients as “burning from inside”
- Cracking and bleeding, especially on hands and feet
- Patches that merge into large plaques covering wide areas
Nail Symptoms (affects up to 50% of patients):
- Pitting (small dents in the nail surface)
- Yellow-brown discoloration (“oil drop” sign)
- Nail separation from the nail bed (onycholysis)
Scalp Symptoms:
- Thick crusting often mistaken for severe dandruff
- Hair loss in severe cases due to inflammation
- Often the first site of psoriasis before body involvement
The Joint Warning Sign No One Should Miss
Between 30–33% of people with plaque psoriasis develop psoriatic arthritis — a serious inflammatory joint condition that can cause permanent joint damage if untreated, according to the American Academy of Dermatology guidelines.
Red flags for psoriatic arthritis:
- Swollen, sausage-like fingers or toes (dactylitis)
- Morning joint stiffness lasting more than 30 minutes
- Lower back pain that improves with movement
- Heel pain or Achilles tenderness
If any of these sound familiar, mention them to your doctor urgently. Untreated psoriatic arthritis causes irreversible joint erosion.
The Mental Health Crisis Hidden Inside Plaque Psoriasis
This is the section competitors consistently skip — and it may be the most important.
People with plaque psoriasis have significantly elevated rates of anxiety and depression compared to the general population. Social stigmatization, workplace discrimination, and disrupted intimacy are commonly reported. For many patients, visible plaques on the face, hands, or scalp are more psychologically devastating than the physical pain.
What This Means For You: If psoriasis is affecting your mental wellbeing, this is a medically significant symptom — not a side effect to manage alone. Tell your dermatologist. Effective plaque psoriasis treatment frequently produces dramatic improvements in anxiety and depression scores within weeks of achieving skin clearance. Our guide on managing depression explores evidence-based strategies that can work alongside medical treatment.
Plaque Psoriasis Treatments in 2026 — The Complete Ranked Guide
Step 1 — Topical Treatments: Your First Line of Defense
For mild to moderate plaque psoriasis, topical agents remain the starting point. The landscape expanded significantly in 2025:
Evidence-Strong Topicals:
- Topical corticosteroids — Gold standard. Reduce inflammation rapidly. Risk of skin thinning with prolonged use.
- Vitamin D analogues (calcipotriol/calcitriol) — Slow abnormal cell growth. Often combined with steroids for additive benefit.
- Tapinarof cream (Vtama) — Nonsteroidal, once-daily. FDA-approved. Works on face and skin folds.
NEW 2025 FDA Approval — Competitors Haven’t Updated:
- Roflumilast foam 0.3% (Zoryve Foam) — A steroid-free, PDE-4 inhibiting foam specifically designed for hair-bearing areas like the scalp. Phase 3 ARRECTOR trial demonstrated strong efficacy with an excellent safety profile. This is a major breakthrough for the estimated 60% of US psoriasis patients who have scalp involvement.
If you’ve been prescribed a new topical or oral medication and want to verify it before taking, use our Pill Identifier to confirm you have the correct medication.
Step 2 — Phototherapy: The Underused Middle Option
Narrowband UVB (NB-UVB) phototherapy is recommended for moderate disease and is highly effective when used 2–3 times per week. It works by slowing skin cell growth and reducing inflammation.
Home NB-UVB devices now feature guided dosage systems that algorithmically adjust exposure based on skin type — dramatically reducing the risk of under- or over-treatment.
Step 3 — Oral Systemic Agents
For patients who need more than topicals but aren’t yet candidates for biologics:
- Methotrexate — Decades of data, effective, but requires liver monitoring
- Cyclosporine — Fast-acting for severe flares; not for long-term use
- Deucravacitinib (Sotyktu) — A TYK2 inhibitor (oral) showing superiority over older oral agents in head-to-head trials
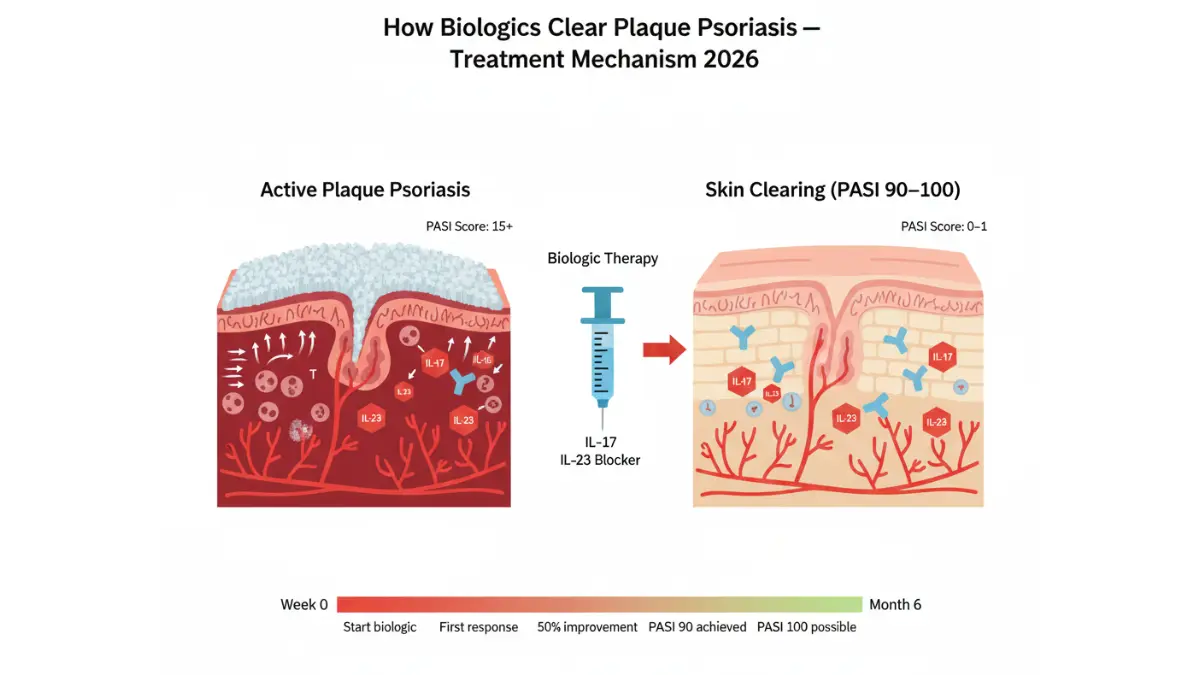
Step 4 — Biologics: The Skin-Clearing Revolution
This is where 2026 changes everything. Biologics target the exact cytokines (IL-17, IL-23) driving plaque psoriasis — with precision that older drugs couldn’t match.
2026 Biologic Comparison — The Table No Competitor Has Built:
| Biologic | Target | PASI 90 Rate | Dosing | Best For |
|---|---|---|---|---|
| Bimekizumab (Bimzelx) | IL-17A/F | ~85–90% | Every 4→8 weeks | Fastest onset, highest clearance rates |
| Risankizumab (Skyrizi) | IL-23 (p19) | ~80–85% | Every 12 weeks (maintenance) | Convenient dosing, long-term durability |
| Ixekizumab (Taltz) | IL-17A | ~78–82% | Every 4→8 weeks | Scalp and nail involvement |
| Guselkumab (Tremfya) | IL-23 (p19) | ~75–80% | Every 8 weeks | Joint + skin combination |
| Secukinumab (Cosentyx) | IL-17A | ~70–75% | Monthly | Well-established long-term safety data |
A 2025 Cochrane network meta-analysis confirmed bimekizumab, ixekizumab, and risankizumab as top performers for PASI 90 achievement with high-certainty evidence.
Breaking — February 2026: At the Maui Derm 2026 Hawaii conference, data on icotrokinra — an investigational once-daily oral IL-23 receptor blocker — showed clearance rates matching injectable IL-23 inhibitors and outperforming all other approved oral agents. This could represent the first oral biologic-level option for psoriasis patients who prefer pills over injections.
Can Your Skin Fully Clear? What PASI 100 Really Means
PASI 100 = zero visible plaques. Complete clearance. Not “managed” — gone.
Modern biologics achieve PASI 100 in 40–60% of patients in clinical trials. In real-world practice, the figure is somewhat lower — but for the first time in dermatology history, complete remission is a routinely documented outcome.
What This Means For You: If your current treatment hasn’t achieved at least 75% improvement (PASI 75) within 12–16 weeks, it’s time to have an escalation conversation with your dermatologist. IL-23 inhibitors and dual IL-17A/F blockers represent the current evidence ceiling. Don’t accept “managed” when “clear” may be possible for you.
Since biologic therapy can have implications for immune function, understanding your metabolic and inflammatory baseline matters. If obesity is a contributing factor to your psoriasis severity, our Weight Loss Calculator can help you set realistic weight reduction goals that complement medical treatment.
Living With Plaque Psoriasis — Flare Prevention, Diet & Daily Management
Diet and Psoriasis: What the Evidence Actually Says in 2026
No diet cures plaque psoriasis. But specific dietary patterns have measurable effects on inflammation and flare frequency:
Evidence-supported approaches:
- Mediterranean diet — Emerging evidence shows reduced systemic inflammation and lower PASI scores in adherent patients. Emphasizes olive oil, fish, legumes, and vegetables.
- Anti-inflammatory eating — Reducing ultra-processed foods, red meat, and refined sugars lowers circulating IL-17 and CRP levels.
- Gluten-free diet — Only beneficial if you have confirmed celiac disease or gluten sensitivity. For others, evidence is weak.
- Dairy and nightshades — Anecdotally reported as triggers by patients, but clinical trial evidence remains insufficient.
What doesn’t work: Extreme elimination diets, detox protocols, or supplement regimens marketed for psoriasis. These are not supported by peer-reviewed evidence.
Nutrition quality directly impacts inflammatory burden. Use our Macro Calculator to design a balanced anti-inflammatory eating plan that supports — not replaces — your medical treatment.
8 Evidence-Based Flare Prevention Strategies
- Moisturize daily — Thick emollients (ointments over creams) restore the skin barrier and reduce flare frequency by up to 50% in consistent users
- Manage stress actively — Stress is the #1 self-reported trigger; mindfulness-based stress reduction has clinical trial support in psoriasis
- Optimize sleep — Poor sleep amplifies systemic IL-17 and TNF-α levels; our Sleep Calculator can help you determine your optimal nightly sleep target based on age and activity
- Quit smoking — Smoking doubles psoriasis risk and directly reduces biologic effectiveness
- Limit alcohol — Alcohol interferes with methotrexate metabolism and worsens inflammation
- Protect skin from injury — Even minor cuts can trigger new plaques (Koebner phenomenon); moisturize before physical activities
- Treat infections promptly — Strep throat is a documented psoriasis trigger; antibiotics reduce flare risk when infection is confirmed
- Stay hydrated — Skin barrier function depends on adequate internal hydration; use our Water Intake Calculator to find your daily target
A Real Patient Outcome — What 2026 Treatment Can Achieve
Marcus, 44, from Houston, Texas, had lived with severe plaque psoriasis covering his torso and arms for 9 years. Three different topical regimens had failed. After switching to a biologic (IL-23 inhibitor) in late 2024, he achieved PASI 90 by week 16 and PASI 100 by month 6. His Dermatology Life Quality Index score dropped from 24 (maximum impairment) to 2. He reported: “I wore short sleeves in public for the first time in a decade.”
Outcomes like Marcus’s are now well-documented in real-world registry data — not just controlled trials. The National Psoriasis Foundation’s patient support resources can connect you with peer communities and advocacy tools if you’re navigating a similar journey.
Since psoriasis is linked to cardiovascular comorbidity risk — including metabolic syndrome and hypertension — it’s worth understanding your full inflammatory picture. Our guide on recognizing metabolic syndrome signs covers the overlap between systemic inflammation and cardiovascular risk that your dermatologist may want to address alongside your skin treatment.
When to See a Dermatologist — And What to Ask in 2026
5 Signs You Need to Escalate Your Care Now
Don’t wait if any of these apply:
- Plaques cover more than 10% of your body — this is classified as severe and qualifies for biologic therapy under most US insurance guidelines
- Joint pain, stiffness, or swollen fingers are developing — psoriatic arthritis risk is time-sensitive; early treatment prevents permanent joint damage
- Your current treatment hasn’t improved symptoms by at least 50% in 12–16 weeks — this is a clinical non-response; your regimen needs to change
- Plaque psoriasis is significantly affecting your mental health — anxiety, depression, or social withdrawal are valid clinical escalation reasons, not “soft” complaints
- Scalp or nail involvement is severe and unresponsive to OTC options — these sites require specialist-grade topicals or systemic treatment
If psoriasis runs in your family and you want to understand your genetic risk before symptoms worsen, our Genetic Risk Assessment Tool can help you frame a more informed conversation with your doctor.
5 Questions to Ask Your Dermatologist at Your Next Visit
These questions separate patients who get the best care from those who stay stuck on ineffective treatments:
- “Am I a candidate for a biologic, and which target — IL-17 or IL-23 — is most appropriate for my disease pattern?”
- “What PASI score should we realistically target, and in what timeframe?”
- “Is roflumilast foam (Zoryve) appropriate for my scalp involvement, given it’s steroid-free?”
- “Should I be screened for psoriatic arthritis, and how often?”
- “Are there ongoing clinical trials — including icotrokinra — that I might qualify for?”
For a deeper understanding of how the immune system behaves in inflammatory skin conditions like psoriasis, our guide on how immunotherapy works provides valuable scientific context on targeted immune modulation.
External clinical resource: The NCBI StatPearls clinical review on Plaque Psoriasis is one of the most comprehensive and up-to-date physician-level references available, updated through late 2025.
Frequently Asked Questions — Plaque Psoriasis
Q1. What is plaque psoriasis?
Plaque psoriasis is a chronic autoimmune skin condition where the immune system overproduces skin cells, creating raised, scaly patches called plaques. It is the most common form of psoriasis, affecting 80–90% of patients.
Q2. Is plaque psoriasis contagious?
No. Plaque psoriasis is not contagious in any way. It cannot be transmitted through touch, shared items, or proximity. It is an internal immune system disorder, not an infection.
Q3. Can plaque psoriasis be cured?
There is currently no permanent cure. However, “complete clearance” (PASI 100) is achievable for 40–60% of patients on modern biologics. Many patients maintain clear skin for years on maintenance therapy.
Q4. What does plaque psoriasis look like?
It appears as raised, clearly defined skin patches. On light skin, they look red with silvery scales. On medium skin, salmon-colored with silver scales. On dark skin, dark brown or violet with gray scales.
Q5. What is the difference between plaque psoriasis and eczema?
Plaque psoriasis typically has thicker, drier, more silvery scales and appears on extensor surfaces (elbows, knees). Eczema tends to appear in flexural areas (inside elbows, behind knees), is wetter, and lacks the defined silvery scale.
Q6. What triggers plaque psoriasis flares?
The most common triggers are stress, strep infections, certain medications (beta-blockers, lithium), alcohol, smoking, skin injury, and obesity. Air pollution combined with genetic susceptibility is an emerging trigger confirmed in 2025 research.
Q7. What is the best biologic for plaque psoriasis in 2026?
Based on current evidence, bimekizumab (Bimzelx) achieves the highest PASI 90 rates (~85–90%). Risankizumab (Skyrizi) offers the most convenient dosing (quarterly maintenance). The “best” biologic depends on individual disease pattern, comorbidities, and insurance coverage.
Q8. Can plaque psoriasis affect the scalp?
Yes — scalp psoriasis affects up to 60% of plaque psoriasis patients. It causes thick crusting, itching, and sometimes temporary hair loss. Roflumilast foam (FDA 2025) is now a proven steroid-free option for scalp involvement.
Q9. Does diet affect plaque psoriasis?
Yes, with caveats. A Mediterranean or anti-inflammatory diet can reduce flare frequency and systemic inflammation. Gluten-free diets help only those with confirmed celiac disease. No diet alone replaces medical treatment.
Q10. Can stress cause plaque psoriasis to get worse?
Yes. Stress is the most commonly reported flare trigger. It elevates cortisol and inflammatory cytokines, directly worsening psoriatic plaques. Stress management is now considered a clinical component of comprehensive psoriasis care.
Q11. How long does it take for plaque psoriasis treatment to work?
Topical treatments show results in 2–4 weeks. Phototherapy typically requires 6–8 weeks of regular sessions. Biologics demonstrate significant improvement by week 12–16, with maximum clearance often achieved by month 6.
Reviewed by the mymedicineadvisor.com International Medical Expert Panel. Last updated: February 2026. For educational purposes only — not a substitute for professional medical advice.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.