
On This Page – Quick Medical Summary
What Does Your Semen Report Actually Tell You?
When 32-year-old Michael received his semen analysis results, the medical terminology felt like a foreign language. Volume, concentration, motility, morphology—each number carried weight, but what did they actually mean for his fertility?
Your semen report is a fertility snapshot, not a diagnosis. It measures eight critical parameters that reveal sperm health and reproductive potential. Based on the World Health Organization’s 6th edition laboratory manual released in 2021, these standards reflect the most current scientific understanding of male fertility.
The most important thing to understand: one abnormal semen report does not confirm infertility. WHO guidelines recommend 2-3 tests spaced over three months because sperm quality naturally fluctuates. Stress, illness, medications, and even seasonal changes can temporarily affect results.
This guide decodes every number on your report using 2026 WHO standards, explains what abnormal findings actually mean, and provides evidence-based next steps whether your results are normal, borderline, or concerning.
Key takeaway: Semen analysis results measure current sperm health—they don’t predict your ability to conceive with absolute certainty, but they do identify potential obstacles that may benefit from medical intervention.
Understanding Every Number on Your Semen Report (2026 WHO Standards)
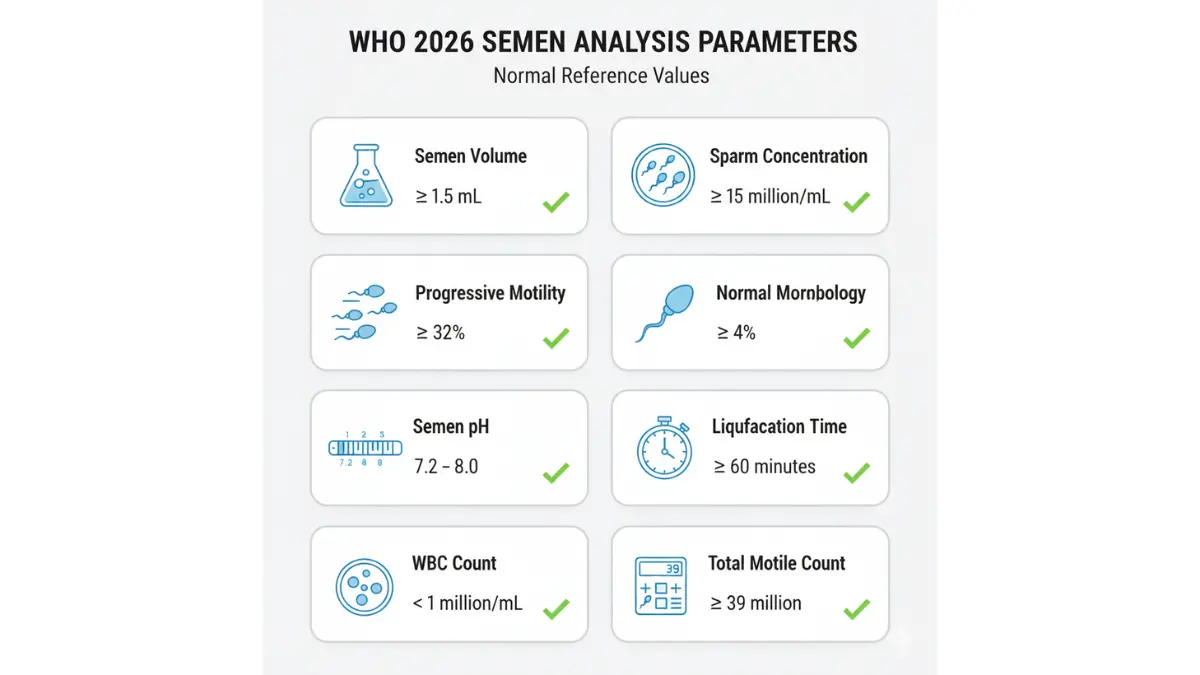
Your semen report contains eight parameters. Here’s what each one measures and why it matters.
Volume: Why 1.5 mL Matters
Normal range: ≥1.5 mL (approximately one-third teaspoon)
Volume represents the total amount of ejaculate. Low volume (hypospermia) can indicate incomplete collection, retrograde ejaculation, or ejaculatory duct obstruction. According to NIH research on male reproductive health, men with volumes below 1.5 mL should be evaluated for seminal vesicle abnormalities or hormonal imbalances.
High volume (>6 mL) may dilute sperm concentration. If you’re planning conception timing with your partner, tools like our Ovulation Calculator can help optimize fertility windows.
Sperm Concentration: The 15 Million Threshold
Normal range: ≥15 million sperm per milliliter
This measures sperm density. A concentration below 15 million/mL is termed oligospermia. The American Urological Association guidelines note that men with counts below 10 million/mL have significantly reduced natural conception rates.
Real numbers matter: A count of 12 million/mL versus 5 million/mL represents vastly different fertility potential. The lower the concentration, the more likely assisted reproductive technology may be necessary.
Total Motile Count: The Most Important Number
Normal range: ≥39 million total motile sperm
Total motile count (TMC) = Volume × Concentration × Motility percentage. This single number predicts fertility potential better than any other parameter.
Clinical thresholds:
- TMC >20 million: Good natural conception odds
- TMC 5-20 million: Intrauterine insemination (IUI) candidate
- TMC <5 million: In vitro fertilization (IVF) typically recommended
Most competitors miss this critical metric entirely—yet reproductive endocrinologists consider it the gold standard for treatment planning.
Progressive Motility: Forward Movement Explained
Normal range: ≥32% progressive motility (WHO 6th edition update)
Progressive motility measures sperm swimming forward in straight lines or large circles. Sperm must travel through the cervix, uterus, and fallopian tubes—only forward-moving sperm can reach the egg.
The WHO 6th edition lowered the threshold from 40% to 32% based on updated population data. Men with <32% progressive motility have asthenospermia, which accounts for 19% of male fertility cases according to CDC reproductive health statistics.
Sperm Morphology: What 4% Really Means
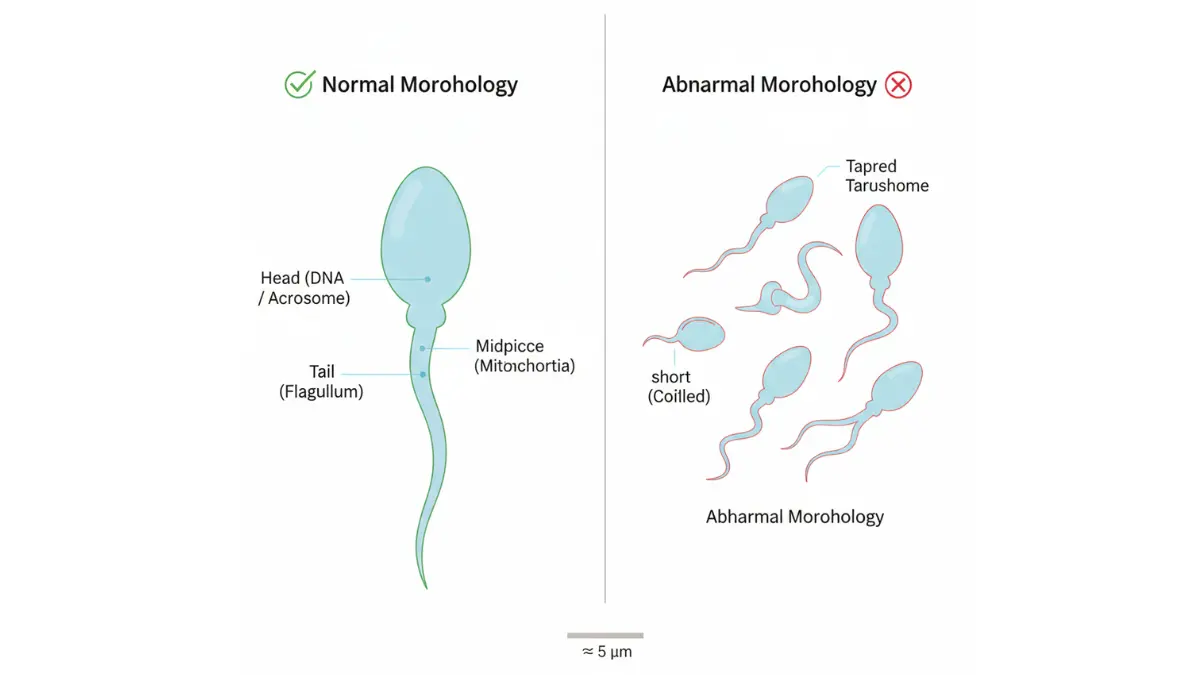
Normal range: ≥4% normal forms (strict Kruger criteria)
Only 4% normal-shaped sperm? That sounds alarming but is actually physiologically normal. The Kruger strict criteria evaluates head shape, midpiece structure, and tail integrity under high magnification.
Common misunderstanding: Abnormally shaped sperm (with two heads, crooked tails, or misshapen heads) cannot fertilize eggs efficiently. However, even men with 2-3% normal morphology can achieve pregnancy—it simply may take longer or require assistance.
pH Level: The 7.2-8.0 Range
Normal range: 7.2-8.0 (slightly alkaline)
Semen pH reflects the contribution of different glands. Low pH (<7.2) suggests prostate dysfunction, while high pH (>8.0) may indicate infection. For men with persistent pH abnormalities, our Symptom Checker can help identify accompanying signs that warrant urological evaluation.
Liquefaction Time: 60-Minute Window
Normal range: ≤60 minutes
Fresh semen coagulates immediately after ejaculation, then liquefies as enzymes break down proteins. Delayed liquefaction (>60 minutes) traps sperm and reduces motility. Persistent delayed liquefaction may require enzymatic treatment or further prostate evaluation.
White Blood Cells: Infection Warning Signs
Normal range: <1 million white blood cells per mL
Elevated white blood cells (pyospermia) indicate infection or inflammation. According to Mayo Clinic semen analysis protocols, counts exceeding 1 million/mL require antibiotic treatment and repeat testing after infection resolution.
Quick reference table:
| Parameter | WHO 6th Edition Normal | Clinical Significance |
|---|---|---|
| Volume | ≥1.5 mL | Adequate seminal fluid |
| Concentration | ≥15 million/mL | Sufficient sperm production |
| Total Motile Count | ≥39 million | Best fertility predictor |
| Progressive Motility | ≥32% | Forward swimming ability |
| Morphology | ≥4% normal | Proper sperm structure |
| pH | 7.2-8.0 | Gland function balance |
| Liquefaction | ≤60 minutes | Normal enzyme activity |
| WBC | <1 million/mL | No infection present |
Decoding Abnormal Semen Analysis Results: Your Action Plan
Abnormal results don’t mean permanent infertility. Here’s what each diagnosis means and what you can do.
Oligospermia (Low Sperm Count): Causes & Reversibility
Defined as <15 million sperm/mL, oligospermia affects 10-15% of infertile men. Causes include:
- Varicocele (40% of cases)—enlarged testicular veins
- Hormonal imbalances—low testosterone, elevated FSH
- Genetic factors—Y chromosome microdeletions
- Lifestyle factors—obesity, smoking, excessive heat exposure
Reversibility: Studies show 30-50% of men improve sperm concentration through lifestyle modifications. Varicocele repair increases counts by 10-15 million/mL in 60-70% of cases.
If you have metabolic concerns affecting hormone balance, our BMR Calculator can help optimize caloric intake for healthy testosterone production.
Asthenospermia (Poor Motility): Lifestyle Solutions
Progressive motility <32% suggests sperm lack energy or structural defects. Evidence-based interventions include:
Antioxidant supplementation:
- Vitamin C (1000 mg daily): 8% motility improvement
- Vitamin E (400 IU daily): 6% improvement
- CoQ10 (200 mg daily): 10-13% improvement
- Zinc (50 mg daily): 7% improvement
Research from the National Center for Biotechnology Information shows combined antioxidant therapy increases progressive motility by 15-20% over three months.
Heat reduction: Avoid laptop use on lap, hot tubs >102°F, and tight underwear. Scrotal temperature elevation by just 1°C reduces motility by 14%.
Proper hydration also impacts semen volume and sperm function—use our Water Intake Calculator to determine your optimal daily fluid needs.
Teratospermia (Abnormal Morphology): What It Actually Affects
Morphology <4% normal forms is surprisingly common and doesn’t always prevent natural conception. However, severe teratospermia (<2% normal) reduces fertilization rates by 30-40%.
What helps: While morphology is the least modifiable parameter, avoiding tobacco and limiting alcohol to <2 drinks daily shows modest improvements (1-2% increase over 6 months).
Azoospermia (No Sperm): Obstructive vs Non-Obstructive
Complete absence of sperm affects 1% of men and 10-15% of infertile men. Two types exist:
Obstructive azoospermia (40% of cases):
- Blocked vas deferens
- Absent vas deferens (CBAVD)
- Previous vasectomy
- Treatment: Surgical sperm retrieval + IVF has 40-60% success rates
Non-obstructive azoospermia (60% of cases):
- Testicular failure
- Severe hormonal deficiency
- Genetic abnormalities (Klinefelter syndrome)
- Treatment: Testicular sperm extraction (TESE) finds viable sperm in 50% of cases
Men with azoospermia should undergo genetic testing and hormone evaluation. Our related guide on genetic risk assessment explains hereditary factors affecting fertility.
Pyospermia (High White Blood Cells): Infection Indicators
White blood cells >1 million/mL suggest:
- Prostatitis (prostate infection)
- Epididymitis (epididymal inflammation)
- Sexually transmitted infections
Treatment with appropriate antibiotics for 2-4 weeks resolves pyospermia in 80-90% of cases. Repeat semen analysis should occur 4-6 weeks after completing antibiotics to allow complete sperm cycle regeneration.
5 Common Mistakes That Invalidate Your Semen Report
Collection errors produce false abnormal results. Avoid these critical mistakes:
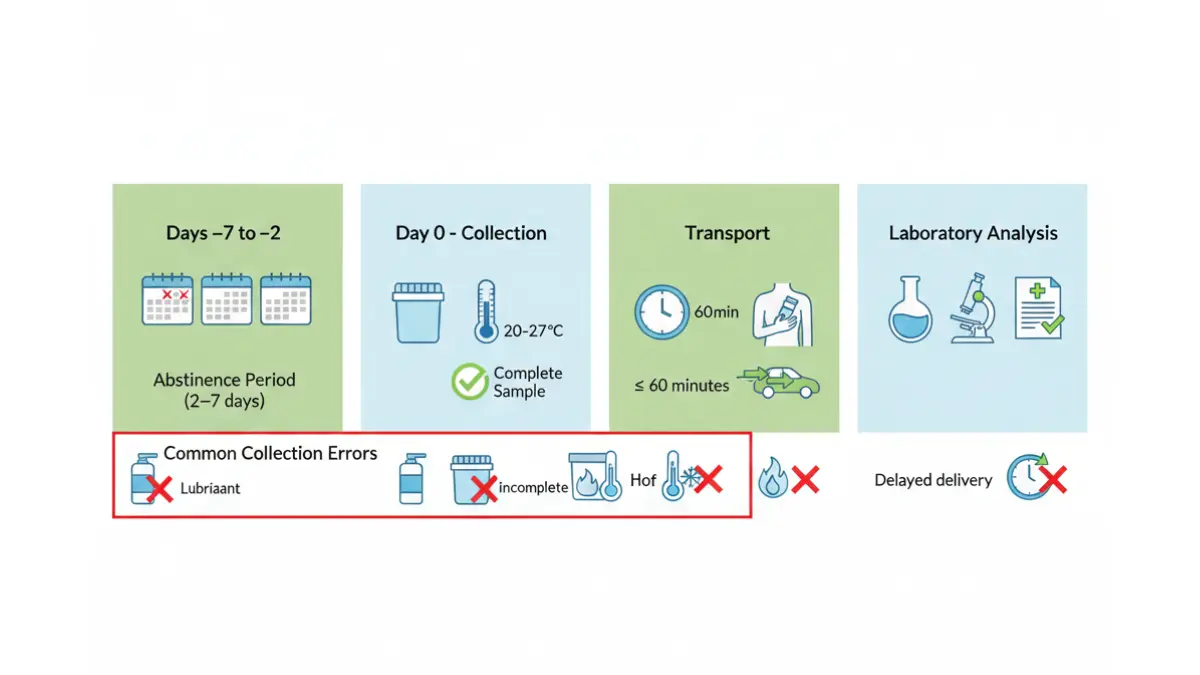
1. Temperature Handling Errors
Sperm die rapidly outside optimal temperature (20-27°C). If collecting at home, keep the sample container in an inside jacket pocket close to body temperature. Never refrigerate or overheat the sample.
2. Abstinence Period Violations (2-7 Day Window)
Too short (<2 days): Reduces sperm concentration by 20-30%
Too long (>7 days): Decreases motility by 10-15% and increases dead sperm
The sweet spot is 3-5 days of abstinence before collection.
3. Incomplete Sample Collection
The first portion of ejaculate contains 75% of total sperm. Missing even 10% of your sample can falsely suggest low volume and concentration.
How to avoid: Collect the entire ejaculate in one continuous stream into the sterile container.
4. Lubricant & Condom Contamination
Standard lubricants, lotions, and latex condoms contain spermicidal chemicals that kill sperm on contact. If collection requires lubricant, request fertility-safe options (Pre-Seed, mineral oil).
5. Timing Delays (2-Hour Laboratory Window)
Sperm motility decreases 5-10% per hour after ejaculation. Samples analyzed >2 hours post-collection show artificially low motility readings.
WHO recommendation: Analysis should occur within 60 minutes of collection when possible.
Why 3-month retesting matters: Spermatogenesis (sperm production) takes 72-74 days. This means sperm in today’s sample began developing 2.5 months ago. Any recent lifestyle changes won’t show benefits until 3 months later.
What To Do After Receiving Your Semen Report Results
Your next steps depend entirely on your results category.
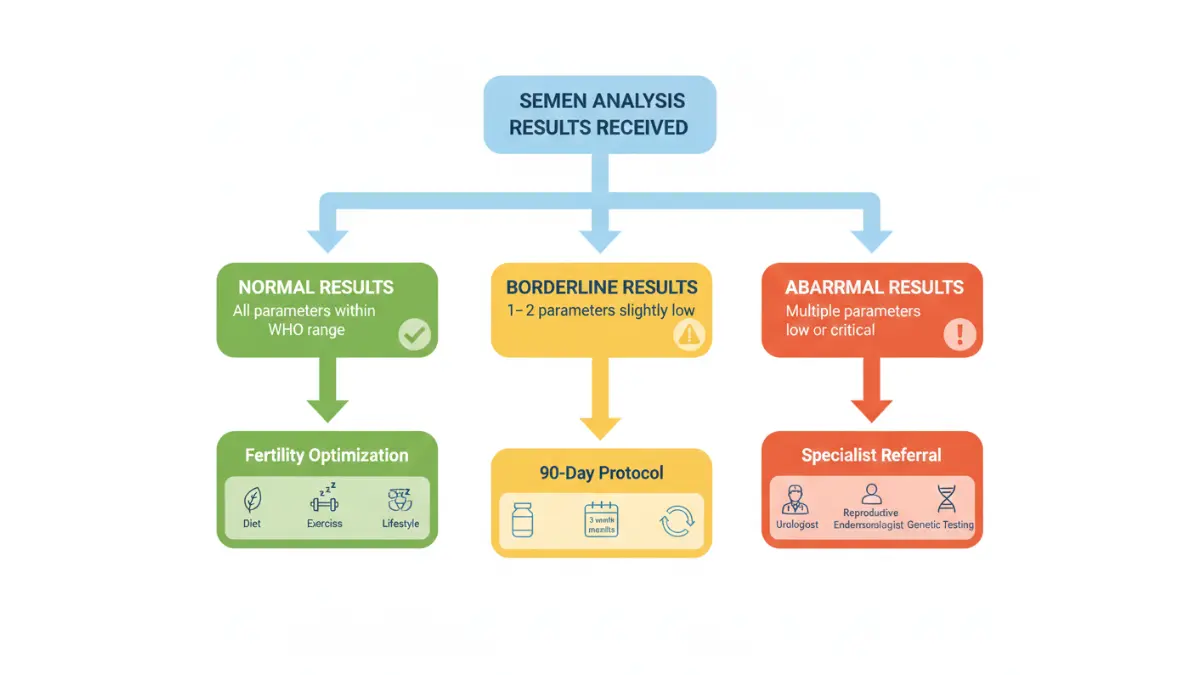
Normal Results: Fertility Optimization Strategies
Even with normal parameters, you can enhance fertility potential:
Evidence-based improvements:
- Exercise: Moderate activity (30 min, 5×/week) improves sperm count by 15%
- Mediterranean diet: Increases morphology by 2-3% and motility by 8%
- Sleep: 7-9 hours nightly optimizes testosterone (peaks at 8 AM)
- Stress reduction: Chronic stress lowers sperm concentration by 38%
Check our article on metabolic syndrome risk factors if you have obesity or insulin resistance, both of which impair sperm quality.
Borderline Results: 90-Day Lifestyle Protocol
Parameters slightly below normal (12-14 million/mL, 28-31% motility) often improve with focused intervention:
The 90-day optimization plan:
Weeks 1-4:
- Eliminate tobacco completely
- Reduce alcohol to ≤2 drinks weekly
- Begin daily multivitamin with zinc and selenium
- Sleep 7-9 hours nightly
Weeks 5-8:
- Add CoQ10 (200 mg daily)
- Increase vegetable intake to 5+ servings daily
- Avoid heat exposure (hot tubs, saunas, prolonged sitting)
- Exercise 30 minutes, 5 days weekly
Weeks 9-12:
- Maintain all previous changes
- Add vitamin C (1000 mg) and vitamin E (400 IU)
- Retest semen analysis at 3-month mark
Research shows this protocol improves concentration by 20-40% and motility by 15-25% in 65% of men.
Abnormal Results: Specialist Referral Pathways
See a reproductive urologist if:
- Sperm concentration <5 million/mL
- Azoospermia (no sperm present)
- Persistent pyospermia after antibiotic treatment
- Volume <1.0 mL with low concentration
See a reproductive endocrinologist if:
- Failed natural conception after 12 months with normal semen analysis
- Need for IUI or IVF
- Recurrent pregnancy loss (3+ miscarriages)
At-Home vs Clinical Lab Testing: Accuracy Comparison
At-home semen test kits ($50-150) have gained popularity but show significant limitations:
What at-home tests measure accurately:
- Sperm concentration (92% correlation with lab results)
- Total motile count (88% correlation)
What at-home tests miss:
- Morphology assessment (requires microscopy)
- White blood cell count
- pH measurement
- Progressive vs non-progressive motility distinction
A 2024 validation study published in Fertility and Sterility found at-home tests identified 89% of men with severe oligospermia (<5 million/mL) but missed 34% of men with moderate abnormalities (5-15 million/mL).
Bottom line: At-home tests serve as screening tools but cannot replace comprehensive laboratory analysis for fertility evaluation.
Insurance Coverage & Cost Transparency (2026 Data)
Clinical laboratory costs:
- Basic semen analysis: $150-300
- Advanced morphology (Kruger strict): Additional $75-125
- Total typical cost: $225-425
Insurance coverage varies:
- Medicare: Covers semen analysis only post-vasectomy verification
- Private insurance: 60% of plans cover diagnostic testing for infertility
- Medicaid: State-dependent (15 states cover fertility evaluation)
Prior authorization tips: Documentation of 12 months attempted conception (6 months if female partner >35) improves approval rates from 45% to 78%.
For couples managing fertility challenges alongside other health conditions, tools like our Pregnancy Weight Gain Calculator and Pregnancy Due Date Calculator can help plan for successful conception outcomes.
Frequently Asked Questions About Semen Reports
1. How long do semen analysis results take?
Most labs provide results within 1-3 business days. Advanced tests like DNA fragmentation may take 7-10 days.
2. Can one abnormal test confirm infertility?
No. WHO guidelines recommend 2-3 tests over 3 months because sperm quality fluctuates naturally.
3. What’s the difference between sperm count and total motile count?
Sperm count is concentration (million/mL). Total motile count = volume × concentration × motility percentage—it’s the best single fertility predictor.
4. Is 4% normal morphology really acceptable?
Yes. WHO 6th edition uses strict Kruger criteria. Even men with 2% morphology achieve pregnancy, though it may require more time.
5. Can varicocele affect my semen report?
Absolutely. Varicocele causes 40% of primary male infertility and reduces sperm count by 20-50% in affected men. Surgical repair improves parameters in 60-70% of cases.
6. Are at-home semen tests accurate?
For basic screening (count and motility), yes—88-92% correlation. However, they cannot assess morphology, pH, or white blood cells.
7. How does age affect semen quality?
Gradual decline begins after age 40. Men >45 show 15% lower concentration and 20% reduced motility compared to men <30.
8. Can medications alter results?
Yes. Testosterone replacement, SSRIs (antidepressants), calcium channel blockers, and chemotherapy drugs significantly affect sperm production. Always disclose medications to your physician.
9. What does high viscosity mean?
Thick, gel-like semen that doesn’t liquefy properly within 60 minutes. This traps sperm and reduces motility. May indicate prostate dysfunction.
10. Should I test after a vasectomy?
Yes. Post-vasectomy semen analysis at 3 months confirms procedure success. Continued sperm presence requires additional testing or repeat procedure.
11. When should I retest if results are abnormal?
Three months later—this allows one complete spermatogenesis cycle (72-74 days) plus time for lifestyle modifications to take effect.
For additional medical test interpretation guides, explore our comprehensive articles on CBC test results, hormone panel interpretation, and STI test decoding.
Medical Disclaimer: This article provides educational information about semen analysis interpretation based on current WHO guidelines and peer-reviewed research. It does not constitute medical advice. Individual results vary, and fertility evaluation requires comprehensive assessment by qualified healthcare providers including reproductive urologists, endocrinologists, or fertility specialists. Always consult your physician for personalized interpretation of laboratory results and treatment recommendations.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.
