On This Page – Quick Medical Summary
Your CMP flagged one of these three lines
It’s 9pm, the portal has pushed your CMP results to your phone, one line carries an H or an L — total protein, albumin, or calcium — and nobody has called you.
- Just outside range, no symptoms? Most common by far. Usually settled by a repeat draw. Sections 2–3.
- High calcium? One hormone test comes next. Section 6.
- Low albumin? Points at liver, kidneys, or inflammation — rarely diet. Section 4.
- High total protein, already searched “myeloma”? Section 5 has the real numbers.
- Confusion, relentless thirst, repeated vomiting, or spasms in your hands or face? Seek care now. Section 7.
These three results are not independent. Albumin physically carries a large share of your calcium, so when one moves it drags the other — which is why reading one line alone, as almost everyone does, can frighten you over a number that means nothing by itself. The same logic governs the rest of the panel.
ℹ️ Medical Disclaimer: This explains how clinicians read lab results. It does not diagnose you, recommend treatment, adjust medication, or advise on coverage. Thresholds are applied to an individual by a clinician who knows your history. Bring abnormal results to the clinician who ordered them, and ask a board-certified endocrinologist about persistent calcium abnormalities.
How albumin, total protein, and calcium fit together
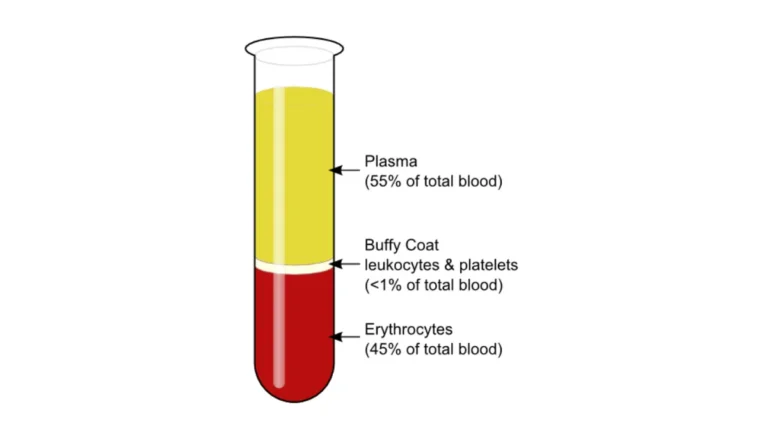
Albumin, total protein, and calcium are three readouts of one system. Albumin is the main protein your liver releases into your blood; total protein is albumin plus everything else; and roughly 40% to 45% of your blood calcium is bound to protein — mostly to albumin itself.
| Test | Typical adult range | Key clinical detail |
|---|---|---|
| Albumin | 3.4–5.4 g/dL | Falls with inflammation, liver disease, protein loss |
| Total protein | 6.5–8.1 g/dL | Albumin + globulins combined |
| Calcium, total | 8.8–10.3 mg/dL | Counts bound and free calcium |
| Calcium, ionized | 4.8–5.6 mg/dL | The free, active fraction — a separate test |
Verified: MedlinePlus Medical Encyclopedia (NLM), July 2026. Labs differ — the range beside your result governs. Many sites still print an outdated total protein range of 6.0–8.3 g/dL. Compare every range on the panel.
Albumin carries almost everything
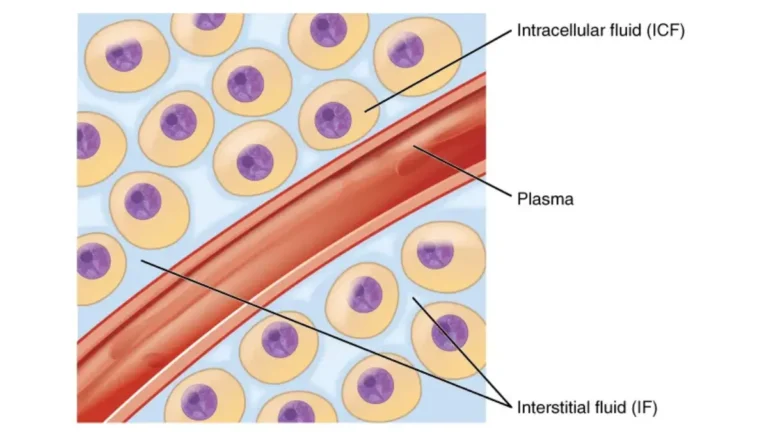
Albumin holds fluid inside your vessels and ferries hormones, vitamins, and drugs around your body, per the NLM’s total protein and A/G ratio overview. It also carries calcium.
🔬 How It Works: Picture albumin as buses, calcium as passengers. Total calcium counts everyone — riders plus people standing free on the pavement. Take buses off the road and the headcount drops. Nobody on the pavement moved, and it’s only those free passengers, the ionized calcium, that your nerves, muscles, and heart use.
The number your lab didn’t print
Globulin isn’t measured on a CMP. It’s calculated — total protein minus albumin — and that arithmetic, or the A/G ratio it produces (normally just above 1), is what your clinician is actually reading.
When all three rise together
Dehydration concentrates blood, lifting albumin, total protein, and calcium at once. A tourniquet left on too long, or a fist clenched during the draw, nudges the same three upward. It’s why these proteins and the electrolyte panel drift together with no disease behind it — and why one borderline value gets re-drawn rather than acted on. Set a daily fluid target if hydration is a recurring issue.
Why “corrected calcium” may mislead you
Often, no — don’t correct your own calcium. The standard formula adjusts total calcium upward when albumin is low, but a 2025 analysis found it agreed with the reference standard less often than the raw number already on your report, and performed worst in exactly the low-albumin patients it was built for.
The formula every calculator uses
Corrected calcium is simple, which is why it’s everywhere: measured calcium + 0.8 × (4.0 − albumin). It has been in use for five decades.
📊 Clinical Data Point: Among 22,658 adults with total and ionized calcium measured simultaneously, the uncorrected total calcium classified calcium status correctly 74.5% of the time. The widely used simplified correction managed 58.7% — and misclassified worse in patients with low albumin. — Source: JAMA Network Open, 2025 (PMID 39836424).
One alternative formula in that study did slightly beat the raw number, so not all correction is useless. The specific correction consumer calculators use is simply weaker than advertised.
The test that answers the question
Ionized calcium measures the free fraction directly, and MedlinePlus notes it may be needed precisely when albumin or immunoglobulins are abnormal — the very situation the formula was invented to paper over.
✅ Patient Action: Ask the clinician who ordered the test: “My albumin is [x] and my total calcium is [y] — do you want an ionized calcium before we interpret this?”
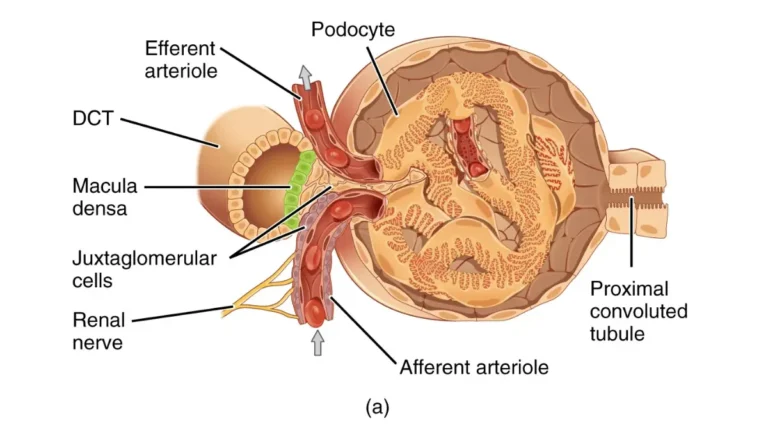
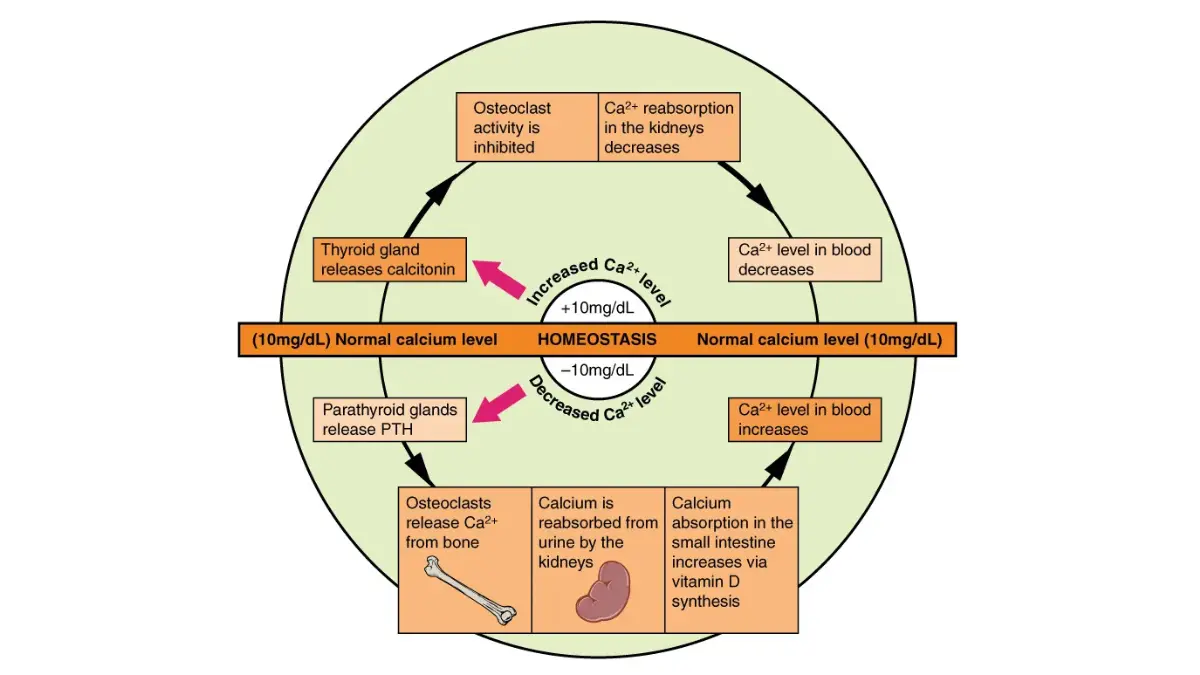
Adapted from OpenStax Anatomy and Physiology 2e Figure 17.16, licensed under CC BY 4.0.
None of this is permission to ignore an abnormal calcium. It’s a reason to let a better test answer the question instead of a worse formula.
What a low albumin actually means
Hypoalbuminemia is a signal, and it usually points somewhere other than your dinner plate.
The common explanations
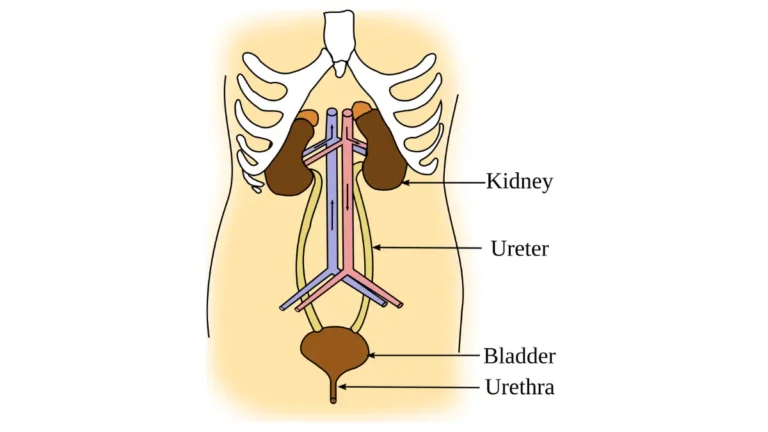
MedlinePlus attributes low albumin to liver disease (cirrhosis, hepatitis, fatty liver), kidney disease, inflammation and infection, malnutrition, and digestive conditions that impair protein use, such as Crohn’s disease. It also falls after a day or two without eating, in pregnancy, after large volumes of IV fluid, and with some medicines including birth control pills.
Why more protein powder won’t fix it
If inflammation is suppressing production, or a damaged kidney is leaking protein into your urine, dietary protein corrects nothing — it only delays the appointment that would. Protein still matters for general health, and you can estimate your daily target — just don’t expect it to move an albumin that’s low for the reasons above.
What your clinician checks next
Albumin is made in the liver, so it’s read beside the liver markers on the same panel. If those are clean, attention turns to your kidney numbers and whether protein is leaking into your urine.
✅ Patient Action: Ask your primary care clinician: “Is my low albumin coming from my liver, my kidneys, or inflammation — and which single test separates them?”
High total protein: the number your lab didn’t print
A high total protein has a short list of explanations, and the order they’re considered in matters more than the list.
- Dehydration — most common, least alarming.
- Chronic inflammation or infection — your body makes more globulins.
- Liver disease.
- A plasma-cell disorder such as multiple myeloma — real, uncommon, and last for a reason.
The protein gap
Your clinician subtracts albumin from total protein. That difference — the protein gap, or gamma gap — decides whether further testing follows. A threshold near 4.0 g/dL commonly triggers it, though published analyses note the cut-off is convention more than hard evidence.
Adapted from Wikimedia Commons CRUK 414, licensed under CC BY-SA 4.0.
What the numbers say about myeloma
📊 Clinical Data Point: Multiple myeloma affects roughly 7.4 people per 100,000 per year in the US. — Source: National Cancer Institute, SEER Cancer Stat Facts: Myeloma, accessed July 2026.
One wrinkle is worth knowing: in light-chain plasma-cell disorders, total protein and globulin are often normal, and standard serum protein electrophoresis misses roughly half of them. A reassuring protein gap is genuinely reassuring — but it’s your clinician’s judgment, not a home calculation, that closes the question.
✅ Patient Action: Ask: “Is my globulin or protein gap raised — and do you want a serum protein electrophoresis?”
High calcium: what your doctor checks next
Hypercalcemia has a short differential, and the first test is nearly always the same.
The first test is PTH
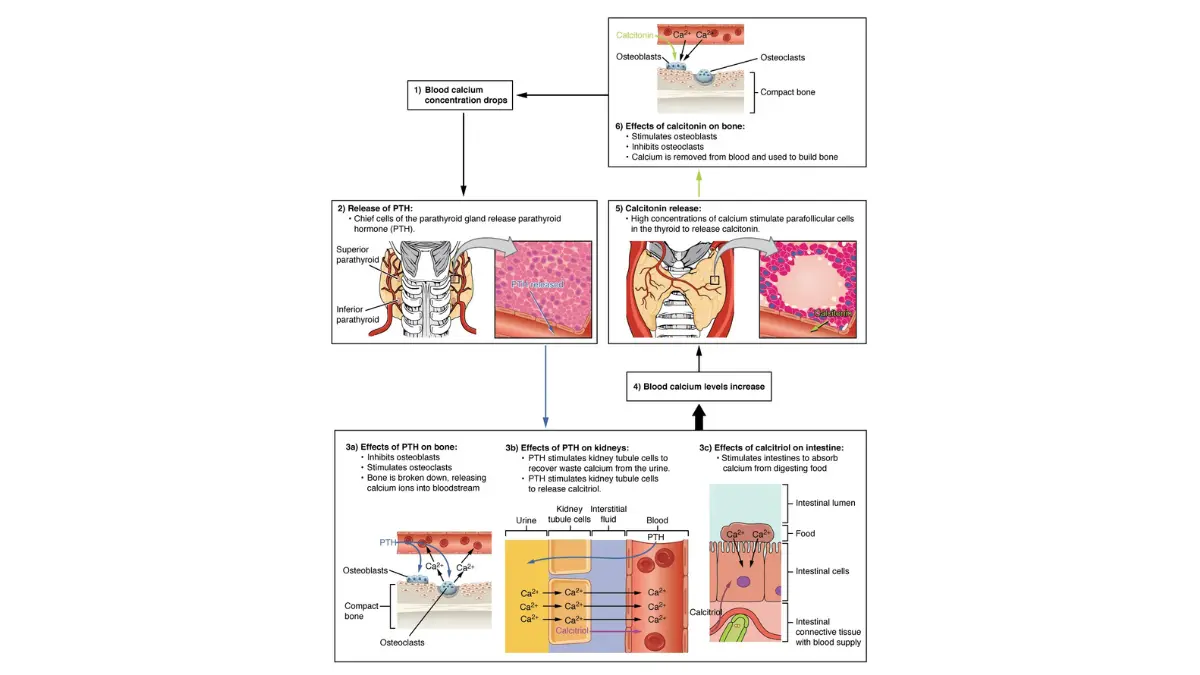
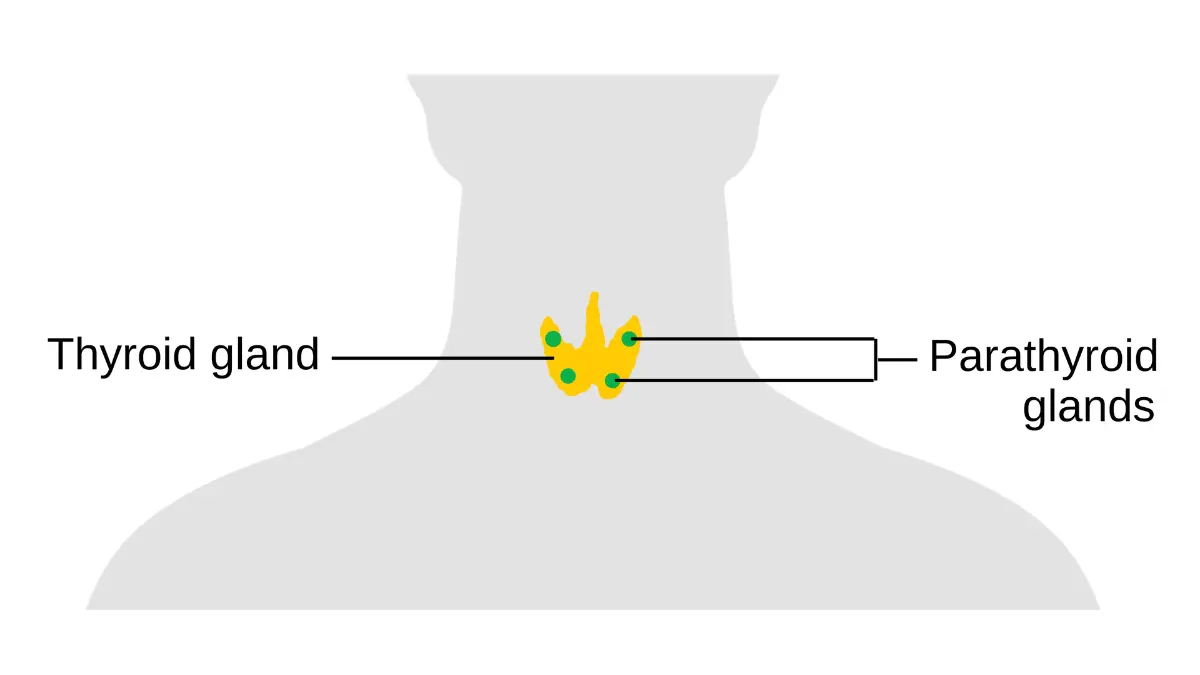
Around 90% of high calcium traces to two causes: primary hyperparathyroidism and cancer-related hypercalcemia. Parathyroid hormone (PTH) separates them, which is why it’s drawn first. A “normal” PTH isn’t automatically reassuring — NIDDK notes it is sometimes only in the upper part of the normal range when a high calcium should have driven it below normal.
📊 Clinical Data Point: About 100,000 Americans develop primary hyperparathyroidism yearly. It peaks between ages 50 and 60, affects women 3–4× more often than men, and in roughly 8 of 10 cases stems from a single benign tumor on one parathyroid gland. Most people have no symptoms. — Source: NIDDK, Primary Hyperparathyroidism (last reviewed March 2019).
Whether surgery is recommended rests on criteria revised in 2022 and applied by an endocrinologist. Older patient pages, NIDDK’s included, predate that update — a reason to ask rather than self-assess.
Medicines and supplements that push calcium up
Thiazide diuretics, lithium, calcium salts, excess vitamin D, and long bed rest can all raise calcium. Diet alone rarely does: the NIH Office of Dietary Supplements notes hypercalcemia is rare in healthy people, usually reflecting hyperparathyroidism or cancer.
⚠️ Clinical Warning: Do not stop a prescribed thiazide, lithium, or any medication on your own. Raise it with the prescriber, and ask: “Has my PTH been drawn alongside my calcium — and could anything I take be contributing?” Bring the bottles, vitamin D included.
When an abnormal calcium is an emergency
Most abnormal calcium results are worked up over weeks. A small number are not.
| Calcium level | Called | Key clinical detail |
|---|---|---|
| Above 14 mg/dL | Severe / hypercalcemic crisis | Treated as an emergency |
| 12–14 mg/dL | Moderate | Symptoms likely; urgent review |
| ~10.5–12 mg/dL | Mild | Investigated, not rushed |
Verified: StatPearls (NCBI Bookshelf, NIH), July 2026. Sources place the lower edge of “mild” at 10 or 10.5, so these are approximate — symptoms matter as much as the number.
Symptoms that mean call now
Severe hypercalcemia symptoms include confusion, persistent vomiting, extreme thirst with heavy urination, and marked weakness. Severe hypocalcemia can cause spasms of the hands or face, seizures, and difficulty breathing.
⚠️ Clinical Warning: Any symptom above warrants emergency care now, not a portal message. An abnormal number with no symptoms is a different situation — contact the office that ordered the test and expect a repeat draw.
When calcium is too low
The two most common causes are vitamin D deficiency and an underactive parathyroid gland, often following thyroid or neck surgery. Chronic kidney disease and low magnesium also contribute.
✅ Patient Action: If your calcium is low and you’ve had neck or thyroid surgery, say so explicitly — it changes the workup. Ask: “Should my vitamin D, magnesium, and PTH be checked together?”
Frequently asked questions
1. What is a normal total protein and calcium level?
MedlinePlus lists total protein at 6.5 to 8.1 g/dL, total calcium at 8.8 to 10.3 mg/dL, and albumin at 3.4 to 5.4 g/dL for adults. Laboratories differ, so the range printed beside your own result is the one that applies. Many websites still quote an outdated total protein range of 6.0 to 8.3.
2. Can dehydration cause high protein and calcium?
Yes. Dehydration concentrates your blood, raising albumin, total protein, and calcium together with no disease present. A tourniquet left on too long during the draw does the same thing. This is one reason a single borderline result is usually repeated rather than acted on, and why hydration before a blood test genuinely matters.
3. Should I use a corrected calcium calculator?
Not to reach your own conclusion. A 2025 analysis of 22,658 patients found the widely used simplified correction classified calcium status correctly 58.7% of the time, against 74.5% for the uncorrected number already on your report — and it fared worst in low-albumin patients. Ask your clinician whether an ionized calcium test is warranted instead.
4. Does eating more protein raise my blood albumin?
Rarely, and not when something else is driving it down. Low albumin usually reflects liver disease, kidney protein loss, or inflammation, and dietary protein corrects none of those. Adequate protein still matters for general health. If your albumin is low, ask your clinician to identify the cause before changing your diet in response.
5. What does a low albumin mean?
Low albumin points toward liver disease, kidney disease, inflammation or infection, malnutrition, or a digestive condition affecting protein use, per MedlinePlus. It can also fall after a day or two without eating, in pregnancy, or after large volumes of intravenous fluid. Ask your primary care clinician which of these fits you before assuming the worst.
6. Does high total protein mean cancer?
Usually not. Dehydration, chronic inflammation, and infection are far more common explanations, and multiple myeloma affects roughly 7.4 people per 100,000 per year in the US. A high total protein is a reason for a follow-up test, not a diagnosis. Ask your clinician whether a serum protein electrophoresis is warranted for you.
7. What is the albumin/globulin (A/G) ratio?
Globulin is not measured directly on a CMP — it is calculated by subtracting albumin from total protein. The A/G ratio compares the two and normally sits slightly above 1. A shifted ratio tells your clinician which side of your total protein has changed, and that determines what gets investigated next.
8. What test comes after a high calcium?
Parathyroid hormone, almost always. PTH separates primary hyperparathyroidism from cancer-related hypercalcemia, and those two causes account for roughly 90% of high calcium results. A PTH sitting in the upper-normal range is not necessarily reassuring when calcium is high. Ask the clinician who ordered your test whether PTH has been drawn alongside it.
9. Can calcium supplements cause high blood calcium?
They can contribute, especially alongside excess vitamin D. But the NIH Office of Dietary Supplements notes hypercalcemia is rare in healthy people and usually reflects hyperparathyroidism, cancer, or another underlying condition. Bring every supplement bottle to your appointment and ask your clinician whether any could be contributing to your result.
10. What are the symptoms of high calcium?
Most people with mildly raised calcium have no symptoms at all. When they appear, they include increased thirst and urination, nausea, constipation, loss of appetite, muscle weakness, fatigue, and aching bones and joints. More severe or long-standing hypercalcemia can cause confusion. Report any of these to the clinician who ordered your test.
11. When is an abnormal calcium an emergency?
Calcium above 14 mg/dL is treated as a hypercalcemic crisis. Seek emergency care now for confusion, persistent vomiting, extreme thirst with heavy urination, or marked weakness — or, with low calcium, spasms of the hands or face, seizures, or trouble breathing. An abnormal number with no symptoms is not an emergency; contact the ordering office.
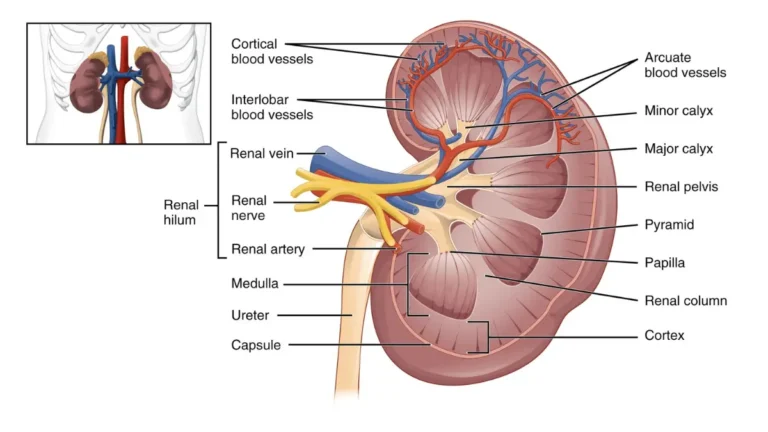
Adapted from OpenStax Anatomy and Physiology 2e Figure 6.24, licensed under CC BY 4.0.
What to do with these three numbers
One system, three readouts, and a repeat draw that settles most of it.
Take three questions into your appointment: whether an ionized calcium is warranted before anyone interprets your result; whether your PTH was drawn alongside a high calcium; and whether a low albumin is coming from your liver, kidneys, or inflammation.
If more than one line is flagged, read the panel as a whole rather than one result at a time.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.