On This Page – Quick Medical Summary
What Knee Replacement Costs in 2026 (And How to Pay $15K or Less)
Sarah Martinez, a 62-year-old teacher from Phoenix, paid $14,200 for her robotic knee replacement in January 2026 and walked out of the surgery center that same afternoon. Five years ago, her neighbor underwent the identical procedure—spent three nights in a hospital and paid $32,800. The difference? Strategic planning, facility choice, and understanding the 2026 cost landscape.
Direct Answer: What You’ll Actually Pay
Knee replacement surgery in 2026 ranges from $15,000 to $50,000+ depending on procedure type, robotic technology, facility selection, and insurance coverage. Outpatient knee replacement procedures performed at ambulatory surgery centers cost 30-40% less than traditional hospital stays, averaging $16,000-$25,000 versus $30,000-$42,000 for inpatient care. Total knee replacement remains the most common orthopedic surgery in the United States, with over 790,000 procedures performed annually.
2026 Knee Replacement Cost Breakdown
| Procedure Type | Outpatient Cost | Hospital Inpatient Cost |
|---|---|---|
| Partial Knee Replacement | $15,000 – $22,000 | $28,000 – $35,000 |
| Total Knee Replacement | $18,000 – $28,000 | $30,000 – $42,000 |
| Robotic-Assisted (Mako/CORI) | $22,000 – $32,000 | $35,000 – $48,000 |
| Bilateral (Both Knees) | $28,000 – $45,000 | $45,000 – $70,000 |
| Revision Surgery | $30,000 – $50,000+ | $50,000 – $85,000+ |
*Data compiled from CMS 2026 payment schedules and national surgery center pricing *
What’s Actually Included in Your Bill
Understanding knee replacement cost itemization prevents surprise charges. The Centers for Medicare & Medicaid Services tracks these standardized components in their 2026 hospital payment systems:
- Surgeon’s professional fee: $3,500 – $8,000
- Anesthesiologist charges: $800 – $2,500
- Operating room facility fee: $5,000 – $15,000
- Knee implant device: $6,000 – $12,000 (varies by brand and material)
- Hospital stay or recovery: $2,000 – $10,000 (1-3 days inpatient vs. 4-6 hours outpatient)
- Pre-operative testing: $500 – $1,200
- Post-operative physical therapy: $150 – $300 per session (typically 12-20 sessions)
Outpatient knee replacement eliminates overnight hospital charges, reducing costs by $5,000-$10,000 immediately. Candidates with healthy BMI levels under 35 typically qualify for same-day discharge protocols.
Why 2026 Prices Differ From Previous Years
Three technological advances impact 2026 knee replacement pricing. Cementless implants using advanced bone-integration materials add $2,000-$3,500 to traditional cemented designs but demonstrate superior 15-year survival rates. 3D-printed custom implants tailored to individual anatomy cost $3,000-$5,000 more than standard sizes but reduce surgical time and improve alignment precision. Robotic surgical systems (Mako by Stryker, CORI by Smith & Nephew) increase upfront costs by $3,000-$8,000 while delivering measurably better outcomes—studies show 23% improved implant positioning and 18% faster recovery compared to conventional techniques.
Medicare Coverage Reality Check for 2026
Medicare Part A and Part B cover medically necessary knee replacement with specific out-of-pocket expenses. For 2026, beneficiaries pay:
- Part A deductible: $1,676 per benefit period (covers inpatient hospital stay up to 60 days)
- Part B deductible: $257 annually
- Part B coinsurance: 20% of Medicare-approved amounts after deductible
- Outpatient surgery center: Approximately $2,000-$2,800 total out-of-pocket
- Inpatient hospital procedure: Capped at $1,676 Part A deductible for surgery and rehab combined
Medicare Advantage plans average $14 monthly premiums in 2026 (down from $17 in 2025) with out-of-pocket maximums typically ranging $3,000-$6,000 annually. The Medicare durable medical equipment policy covers 80% of walker, cane, and continuous passive motion machine costs for knee replacement recovery.
Five Proven Strategies to Hit the $15,000 Target
1. Choose Outpatient Surgery Centers Over Hospitals
Ambulatory facilities charge $17,800 for partial knee replacement versus $28,000+ at hospitals. Same-day discharge candidates save $7,000-$12,000 immediately.
2. Negotiate Cash-Pay Discounts
Self-pay patients securing pre-surgery cash agreements receive 30-50% discounts. One Oklahoma surgery center quotes $17,000 all-inclusive cash pricing for total knee replacement versus $35,000 billed to insurance.
3. Strategic Timing Around Insurance Deductibles
Scheduling surgery in January after meeting annual deductibles maximizes coverage. Compare this to December procedures requiring new deductibles in January for follow-up care.
4. Medical Financing Options
- CareCredit: 0% APR for 24 months on amounts over $1,000
- Prosper Healthcare Lending: Fixed rates 6.99-35.99% APR
- Hospital payment plans: Often interest-free 12-36 month arrangements
Compare financing carefully—a similar strategic approach helped patients reduce costs for other major procedures.
5. HSA/FSA Pre-Tax Contributions
Health Savings Accounts and Flexible Spending Accounts provide 22-35% effective savings through pre-tax dollars. A $15,000 knee replacement costs $9,750-$11,700 in after-tax equivalent dollars for middle-income earners.
Research from the National Institutes of Health demonstrates knee replacement delivers cost-effectiveness ratios of $18,300-$28,100 per quality-adjusted life year—well within accepted healthcare value thresholds. High-volume surgical centers (performing 50+ procedures annually) consistently outperform low-volume facilities in both outcomes and cost-efficiency.
Same-Day Knee Replacement – The 2026 Revolution
James Peterson scheduled his total knee replacement expecting three hospital nights and a $38,000 bill. Instead, the 64-year-old accountant walked into an ambulatory surgery center at 6:00 AM, underwent robotic-assisted surgery, and drove home with his wife at 2:30 PM that same afternoon—paying $19,400 total. By 2026, approximately 70% of knee replacement patients qualify for same-day discharge protocols, fundamentally changing recovery expectations and costs.
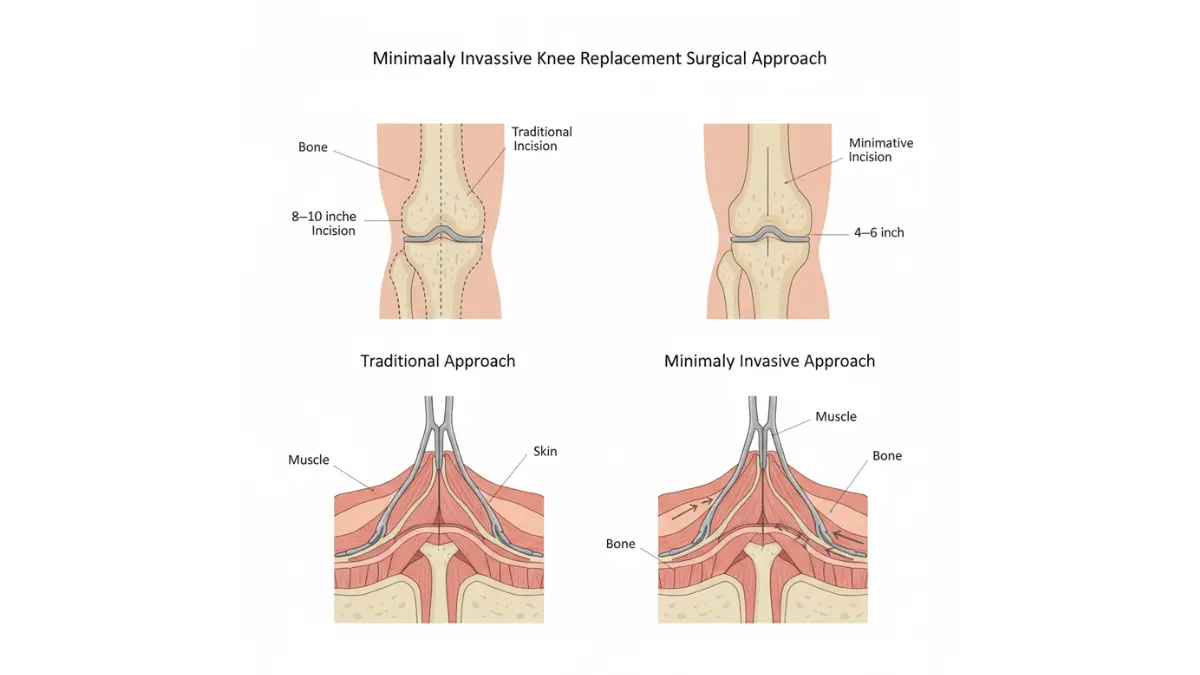
What Same-Day Knee Replacement Actually Means
Same-day (outpatient) knee replacement allows qualified patients to return home 2-6 hours after surgery using minimally invasive techniques, regional anesthesia blocks, and accelerated recovery protocols. This approach reduces costs by $5,000-$10,000 compared to traditional inpatient hospital stays while delivering equivalent safety outcomes. Research published in the National Institutes of Health database demonstrates that properly selected outpatient knee replacement patients experience 3.3% readmission rates versus 4.9% for inpatient procedures—actually lower complications when protocols are followed.
Medicare officially approved outpatient knee replacement reimbursement in 2018, accelerating adoption nationwide. Academic medical centers now discharge 98% of eligible patients directly from post-anesthesia recovery units without overnight observation.
Your Hour-by-Hour Same-Day Timeline
5:30-6:30 AM – Arrival & Pre-Op
- Registration and pre-surgical screening
- IV placement and regional nerve block (adductor canal block for knee)
- Final surgeon consultation
7:00-9:00 AM – Surgery Window
- 60-90 minute procedure using general anesthesia
- Enhanced recovery anesthesia protocols minimize drowsiness
- Real-time pain management optimizes early mobility
9:30-11:30 AM – Post-Anesthesia Recovery
- Vital sign monitoring (2-3 hours typical)
- Oral pain medication transition
- Initial ice and elevation protocols
12:00-2:00 PM – Physical Therapy Clearance
- Walking 70+ meters with assistive device
- Stair navigation demonstration
- Transfer safety assessment (bed, chair, toilet)
- Durable medical equipment fitting
2:00-3:30 PM – Discharge Preparation
- Final surgeon/anesthesia approval
- Prescription review and pain management plan
- 24-hour caregiver confirmation
- Home safety checklist verification
3:30-4:00 PM – Home Departure
- Discharge directly to vehicle
- No wheelchair transport delays
- Same-day recovery begins in familiar environment
Who Qualifies for Same-Day Discharge
The University of Arkansas Medical Sciences published criteria showing 98% successful same-day discharge when patients meet specific standards:
Medical Eligibility Checklist:
- Age under 75 years (case-by-case exceptions possible)
- BMI under 35 kg/m² (check your body mass index for qualification)
- No sleep apnea, recent heart attack, or pacemaker
- No chronic obstructive pulmonary disease
- Controlled diabetes without kidney complications
- American Society of Anesthesiologists (ASA) score 1-2 (occasionally 3)
Social Support Requirements:
- Responsible adult at home for minimum 24 hours
- Ground-floor sleeping arrangements or manageable stairs
- Transportation within 30 minutes of surgery center
- Reliable phone access for follow-up calls
- Motivated patient with realistic expectations
Patients with balanced caloric needs and healthy baseline fitness levels tolerate accelerated protocols better—preoperative conditioning matters significantly.
Setting Up Home Recovery (Before Surgery Day)
Essential Equipment Delivered Pre-Op:
- Walker or crutches (fitted during PT clearance)
- Elevated toilet seat (adds 4-6 inches)
- Shower chair with non-slip feet
- Reacher/grabber tool (27-32 inch length)
- Ice therapy system or gel packs
Home Modifications Checklist:
- Remove throw rugs and electrical cords from walkways
- Install temporary grab bars in bathroom
- Prepare ground-floor sleeping area
- Stock 2-week supply of easy-prep meals
- Arrange medication organization system
Same-Day vs. Hospital Stay: Real Cost Comparison
| Cost Component | Same-Day Outpatient | Hospital Inpatient (2-3 nights) |
|---|---|---|
| Facility Fee | $8,000 – $12,000 | $15,000 – $25,000 |
| Surgeon Professional | $4,500 – $7,000 | $4,500 – $7,000 |
| Anesthesia | $1,200 – $2,000 | $1,500 – $2,800 |
| Implant Device | $7,000 – $11,000 | $7,000 – $11,000 |
| Overnight Care | $0 | $4,000 – $8,000 |
| Pharmacy | $300 – $600 | $800 – $1,500 |
| Physical Therapy | $0 (home-based) | $600 – $1,200 |
| TOTAL AVERAGE | $18,000 | $33,000 |
Cost savings: $15,000 (45% reduction) for qualified same-day patients
Patient satisfaction surveys show 80% report being “very satisfied” with same-day discharge, citing comfort of home recovery and reduced infection exposure. The accelerated timeline particularly appeals to working-age patients returning to employment—similar strategic planning applies to other surgical procedures requiring quick recovery.
Robotic Knee Replacement Technology in 2026 (Mako vs. CORI vs. Traditional)
Linda Chen researched knee replacement options for eight months before committing. Her surgeon offered traditional surgery at $23,000 or robotic-assisted at $28,500. She chose the Mako robotic system—and six months later walks pain-free with implant alignment measuring within 0.5 degrees of optimal positioning. Robotic knee replacement technology demonstrates 23% better component alignment and 19-30% improved six-year implant survivorship compared to manual surgery, but costs $3,000-$8,000 more.
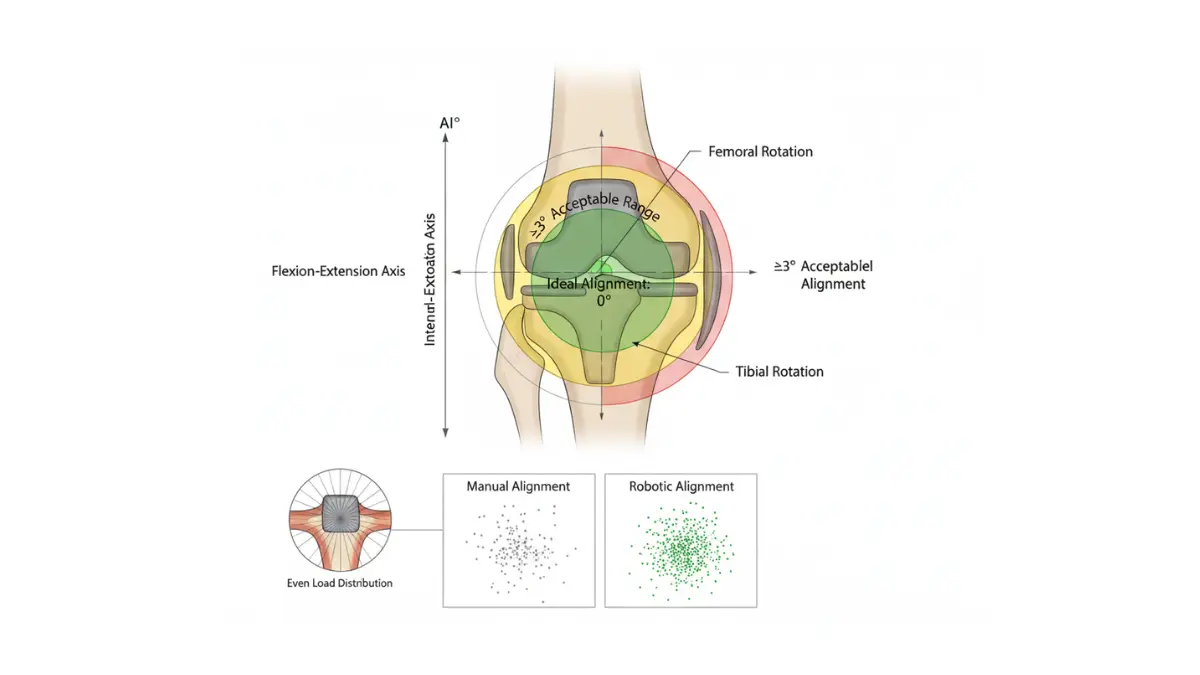
How Robotic Surgery Actually Works
Robotic-assisted knee replacement uses computer-guided precision systems to create personalized surgical plans and improve implant positioning accuracy. Two dominant platforms emerged by 2026: Mako (Stryker Corporation) and CORI (Smith & Nephew), each with distinct technological approaches. Neither system operates autonomously—surgeons maintain complete control while robotic arms enforce safety boundaries preventing deviation from the pre-planned surgical parameters.
The 2024 Australian National Joint Replacement Registry reported six-year survivorship for Mako-implanted knees showed 19% relative improvement over manual surgery, increasing to 30% when combined with patella resurfacing. Medium-term functional outcome scores measured through validated patient-reported instruments favored robotic assistance (mean difference 5.50 points on standardized scales, 95% confidence interval 2.19 to 8.81) across seven studies involving 1,101 participants.
Mako System: CT-Based Pre-Planning
Mako requires pre-operative CT scanning 1-2 weeks before surgery to create 3D digital models of patient anatomy. Software analyzes bone density, cartilage wear patterns, and ligament positions to generate optimized implant size and placement plans. During surgery, infrared sensors track bone position in real-time, adjusting the robotic cutting boundaries 1,000+ times per second.
Mako Advantages:
- Pre-surgical visualization identifies challenges before incision
- Detailed bone quality assessment guides fixation choices
- Higher initial accuracy from comprehensive 3D planning
- Patient education tool (viewing personalized 3D models)
Mako Limitations:
- Requires separate CT appointment ($500-$1,200 additional cost)
- 7-14 day wait between CT and surgery scheduling
- Radiation exposure (typical knee CT: 0.1 mSv—equivalent to 10 chest X-rays)
CORI System: Image-Free Intraoperative Mapping
CORI eliminates pre-operative imaging by creating 3D digital models during surgery using infrared cameras and handheld sensors. The system collects anatomical data points, sending precise knee position information to the robotic handpiece over 300 times per second to guide bone preparation and implant placement.
CORI Advantages:
- No pre-operative CT required (saves time and radiation)
- Surgery scheduled immediately after consultation
- Adapts to intraoperative findings in real-time
- Lower facility equipment costs (typically passed to patients)
CORI Limitations:
- Less pre-surgical planning visualization
- Surgeon learning curve steeper without advance planning
- Cannot pre-identify unusual anatomy before incision
Technology Head-to-Head Comparison
| Feature | Mako Robotic | CORI Robotic | Traditional Manual |
|---|---|---|---|
| Pre-Op Imaging | CT scan required | None needed | X-rays only |
| 3D Planning | 1-2 weeks before | During surgery | Mental visualization |
| Alignment Accuracy | ±0.5 degrees | ±1.0 degrees | ±3-5 degrees |
| Positioning Updates | 1,000+/second | 300+/second | Manual adjustment |
| Surgery Duration | 90-110 minutes | 80-100 minutes | 70-90 minutes |
| Cost Premium | $5,000-$8,000 | $3,000-$6,000 | Baseline |
| 6-Year Survivorship | 19-30% better | Emerging data | Reference standard |
| Patient Satisfaction | 93-96% | 90-94% | 85-87% |
*Data compiled from Australian Registry 2024, NIH systematic reviews, and multi-center trials *
3D-Printed and Cementless Implants in 2026
The FDA cleared 3D-printed AFFIXIUM knee implants with advanced porous surface technology for cementless fixation in 2020, with expanded indications granted through 2024. These implants use additive manufacturing to create highly porous titanium surfaces mimicking natural bone structure, promoting biological integration without cement.
Cementless Implant Benefits:
- Faster bone ingrowth (4-6 weeks vs. 8-12 weeks)
- Easier revision surgery if needed (no cement removal)
- Reduced allergic reaction risk (no methylmethacrylate exposure)
- Ideal for younger patients (<60 years) with dense bone
Cost Impact: 3D-printed cementless implants add $2,000-$3,500 to standard cemented designs. Combined with robotic surgery, total premiums reach $7,000-$11,000 above baseline manual surgery with standard implants.
Is Robotic Technology Worth the Extra Cost?
Calculate return on investment beyond surgical fees. Robotic knee replacement patients demonstrate measurably improved outcomes translating to financial value:
- Faster recovery: 14-18 days to independence vs. 21-28 days traditional (reduced caregiver costs)
- Less physical therapy: 12-15 sessions vs. 18-24 sessions ($1,800-$2,700 savings)
- Fewer complications: 3.3% readmission vs. 4.9% traditional ($8,000+ per readmission avoided)
- Longer implant survival: 19-30% improvement potentially delays revision 5-8 years ($30,000-$50,000 revision cost)
Patients maintaining optimal post-surgical fitness levels using evidence-based rehabilitation protocols maximize robotic surgery benefits. The technology advantage amplifies with younger patients (<65) expecting 25-30 years of implant function.
Recovery Timeline + Physical Therapy Blueprint (2026 Protocols)
Michael Thompson walked unassisted to his mailbox on day 12 after knee replacement—a milestone his surgeon predicted for week 3. The difference? New 2026 accelerated recovery protocols emphasizing immediate mobility, aggressive pain control, and structured physical therapy benchmarks. Knee replacement recovery typically spans 3-6 months for full return to daily activities, with major milestones at 2 weeks (walking independently), 6 weeks (driving clearance), 3 months (low-impact sports), and 12 months (maximum improvement).
First 48 Hours: Critical Action Steps
The immediate post-operative period determines long-term outcomes. Research from the National Institutes of Health shows patients starting rehabilitation within 24 hours experience 3.3-day average hospital stays versus 6.6 days for delayed mobilization.
Hour 2-4 Post-Surgery:
- Begin continuous passive motion (CPM) machine for 1-hour sessions
- Ice therapy with cryotherapy unit (20 minutes every 2 hours)
- Ankle pumps and quad sets (10 repetitions hourly while awake)
- Elevate leg above heart level continuously
Day 1 (Surgery Day or Next Morning):
- Stand at bedside with physical therapist assistance
- Walk 10-20 feet using walker
- Practice toilet transfers and bed mobility
- Begin oral pain medication transition from IV narcotics
Day 2:
- Walk 50-100 feet in hallway (2-3 times daily)
- Bend knee to 70-80 degrees actively
- Practice stair climbing (minimum 3-4 steps for discharge clearance)
- Wound inspection and dressing change
Quality sleep patterns significantly impact healing—aim for 7-9 hours nightly with pain medication timed for uninterrupted rest.
Month-by-Month Recovery Roadmap
| Timeline | Key Milestones | Range of Motion Goal | Activity Level |
|---|---|---|---|
| Week 1-2 | Walking 100+ feet, basic self-care | 70-90° flexion | House mobility with walker |
| Week 3-6 | Independent walking, stairs mastered | 100-110° flexion | Transition to cane, light housework |
| Month 2-3 | Return to desk work, driving resumed | 110-120° flexion | Normal daily activities, shopping |
| Month 4-6 | Low-impact exercise, strengthening | 120-125° flexion | Swimming, cycling, golf |
| Month 7-12 | Maximum improvement plateau | 125-130° flexion | All activities except high-impact |
*Data compiled from NIH systematic reviews tracking 2,703 knee replacement patients *
Weeks 1-2: Foundation Phase
Walking independently around your home represents the primary goal. NIH research demonstrates 85% of patients achieve 90-degree knee flexion by week 2 with consistent therapy.
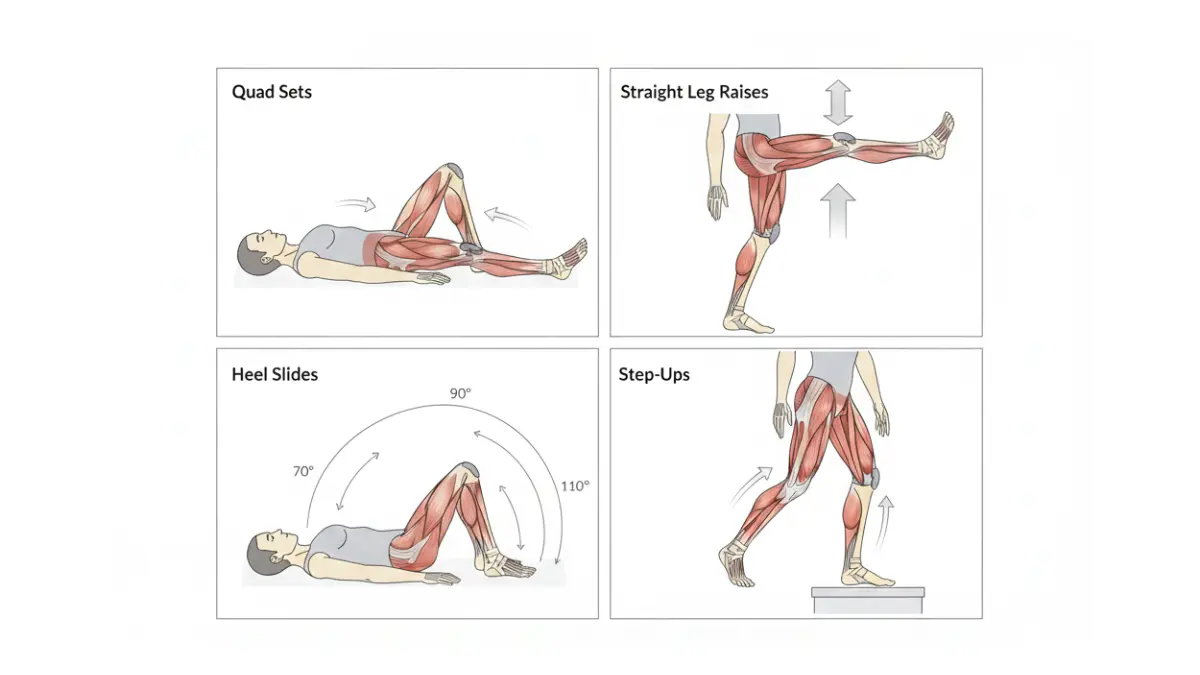
Daily Exercise Protocol:
- Heel slides: 10 repetitions, 3 sets
- Straight leg raises: 10 repetitions, 3 sets
- Quad sets: 10 repetitions, 3 sets
- Ankle pumps: 20 repetitions every waking hour
Weeks 3-6: Strengthening Transition
Graduating from walker to cane marks functional independence. Studies show patients completing 17 physical therapy sessions over 6 weeks achieve 95% success reaching 90-degree flexion and 85% achieving 100-degree flexion.
Progression Exercises:
- Seated knee extension with resistance
- Standing hip abduction (side leg lifts)
- Step-ups (4-6 inch platform)
- Balance training on one leg
Months 2-6: Return to Life
Most patients resume driving at 6 weeks when reaction time normalizes and they discontinue narcotic pain medication. Return to work varies—desk jobs typically 6-8 weeks, standing occupations 10-12 weeks, physical labor 12-16 weeks.
Physical Therapy Costs and Insurance Coverage
Medicare Part B covers 80% of medically necessary physical therapy after meeting the $257 annual deductible, leaving patients responsible for 20% coinsurance. Typical costs:
- Per session: $150-$300 (varies by region)
- Standard protocol: 17 sessions over 6 weeks
- Total out-of-pocket (Medicare): $510-$1,020
- Private insurance: Variable copays $25-$75 per visit
Achieving adequate protein intake supports tissue healing—target 1.2-1.5 grams per kilogram body weight daily during recovery months.
Red Flags Requiring Immediate Medical Attention
The CDC monitors post-surgical infections that can present subtly in early stages. Recognize warning signs demanding same-day evaluation:
Infection Indicators:
- Fever >101°F (38.3°C) after first 48 hours
- Increasing redness spreading beyond incision edges
- Wound drainage (pus, foul odor, or greenish discharge)
- Warmth radiating from surgical site
Blood Clot Symptoms (Deep Vein Thrombosis/Pulmonary Embolism):
- Calf pain, swelling, or warmth in one leg only
- Sudden shortness of breath or chest pain
- Rapid heartbeat with unexplained anxiety
- Coughing blood
Implant Complications:
- Sudden severe pain after initial improvement
- Popping sensation with immediate loss of function
- Knee feels unstable or gives way unexpectedly
- New numbness or tingling below knee
Nontuberculous mycobacterial infections represent rare but serious risks requiring extended antimicrobial therapy and potential hardware removal if diagnosed.
Insurance, Medicare & Financing Your Knee Replacement in 2026
Dorothy Williams opened her Medicare Explanation of Benefits expecting catastrophic costs. Instead, her $31,500 total knee replacement generated $2,847 in actual out-of-pocket expenses—$1,676 Part A deductible plus $1,171 in Part B coinsurance for surgeon and anesthesia fees. Medicare covers medically necessary knee replacement through Part A (inpatient hospital) and Part B (outpatient surgery and professional services), with 2026 beneficiary costs ranging $2,800-$6,200 depending on facility choice and supplemental insurance.
What Medicare Actually Covers in 2026
Medicare Part A and Part B provide comprehensive knee arthroplasty coverage when deemed medically necessary by an orthopedic surgeon. The program paid for over 467,000 knee replacement procedures in 2023, making it Medicare’s most common inpatient surgical service.
Medicare Part A (Hospital Insurance) – 2026 Costs:
- Deductible: $1,676 per benefit period (covers days 1-60 inpatient hospital stay)
- Days 61-90: $434 daily coinsurance
- Lifetime Reserve Days: $868 daily coinsurance (60 days total lifetime)
- Skilled Nursing Facility: $0 days 1-20, then $217.50 daily days 21-100
Medicare Part B (Medical Insurance) – 2026 Costs:
- Annual Deductible: $257 (once per calendar year)
- Coinsurance: 20% of Medicare-approved amounts
- Surgeon Professional Fee: 20% after deductible (typically $700-$1,600)
- Anesthesiologist Fee: 20% after deductible (typically $160-$500)
- Outpatient Facility: 20% after deductible (typically $3,200-$5,000 for surgery center)
For outpatient knee replacement (increasingly common in 2026), total out-of-pocket averages $2,800-$3,400 with Original Medicare. Traditional hospital inpatient procedures cost beneficiaries the $1,676 Part A deductible plus 20% Part B charges—typically $4,200-$6,200 total.
Medicare Advantage Plan Considerations
Medicare Advantage (Part C) plans averaged $14 monthly premiums in 2026 (down from $17 in 2025) while offering out-of-pocket maximum protections typically $3,000-$6,700 annually. These plans often include:
- $0-$400 surgery copays (fixed amounts vs. percentage coinsurance)
- Pre-authorization requirements for elective surgery
- Network restrictions requiring in-network orthopedic surgeons
- Bundled episode-based payments covering 90-day recovery period
Original Medicare with Medigap Supplement Plan G eliminates most cost-sharing, covering the 20% Part B coinsurance that can reach $5,000+ on complex cases.
Private Insurance Navigation Roadmap
Commercial insurance typically covers 70-90% of knee replacement costs after deductibles, with patients paying $3,000-$8,000 out-of-pocket depending on plan design. Key coverage variables:
Pre-Authorization Requirements (Critical):
- Submit 30-60 days before scheduled surgery
- Include conservative treatment documentation (6+ months physical therapy, injections, medications)
- Medical necessity criteria: Pain scale 7+/10, limited daily function, X-ray evidence
- Denial rate: 8-12% initially, 60% successful on appeal
In-Network vs. Out-of-Network Cost Differences:
- In-network: 80-90% coverage after deductible
- Out-of-network: 50-70% coverage with higher deductibles
- Balance billing exposure: Out-of-network surgeons may bill above insurance-allowed amounts
Insurance Appeal Success Strategy
If initial authorization is denied, systematic appeals succeed 60% of the time. Winning elements include:
- Detailed pain diary documenting daily functional limitations
- Failed conservative treatment timeline (minimum 6 months)
- Peer-reviewed studies supporting necessity at your age/condition
- Letter from orthopedic surgeon citing specific clinical guidelines
- Second opinion confirmation from different board-certified surgeon
Similar strategic approaches proved effective for patients navigating complex surgical insurance coverage in other orthopedic procedures.
Medical Financing and Payment Plan Options
CareCredit Healthcare Financing:
- 0% APR promotional financing: 6, 12, 18, or 24 months on amounts $200+
- Extended payment plans: 24-60 months with 17.90-26.99% APR
- Minimum monthly payment: 3% of balance or $29 (whichever greater)
- Application approval: 580+ credit score typically required
Prosper Healthcare Lending:
- Fixed APR: 6.99-35.99% based on creditworthiness
- Loan amounts: $1,000-$40,000
- Terms: 24-84 months
- No prepayment penalties
Hospital Direct Payment Plans:
- Interest-free: 12-36 months (most common: 24 months)
- Qualification: Typically no credit check required
- Down payment: Usually 10-20% upfront
- Automatic withdrawal from checking account
Health Savings Account (HSA) Tax Advantages:
- Pre-tax contributions reduce taxable income
- Triple tax benefit: Tax-free deposits, growth, and withdrawals for medical expenses
- 2026 contribution limits: $4,300 individual, $8,550 family
- Effective savings: 22-37% depending on tax bracket
Uninsured Patient Options
Surgery centers offer self-pay discounts 30-50% below insurance-billed rates. Strategies for uninsured patients:
Cash-Pay Negotiation Framework:
- Request written self-pay quote including all components
- Negotiate 30-40% discount for prepayment
- Oklahoma Surgery Center example: $17,000 all-inclusive vs. $35,000 insurance billing
- Exclude unnecessary add-ons (private hospital rooms, extended monitoring)
Medical Tourism Considerations:
- India knee replacement: $4,000-$7,000 (JCI-accredited hospitals)
- Mexico: $8,000-$12,000 (U.S.-trained surgeons)
- Risks: Travel complications, limited follow-up access, infection treatment delays
- Insurance typically excludes international complications
Choosing the Right Procedure, Surgeon & When to Have Surgery
Barbara Reynolds waited 38 months from her first orthopedic consultation to finally scheduling knee replacement—two years longer than medically optimal according to her surgeon. The most common patient regret? Waiting too long. Studies show 43% of knee replacement patients wish they’d undergone surgery 18-24 months earlier when pain first exceeded 7/10 on daily basis and conservative treatments stopped providing relief.
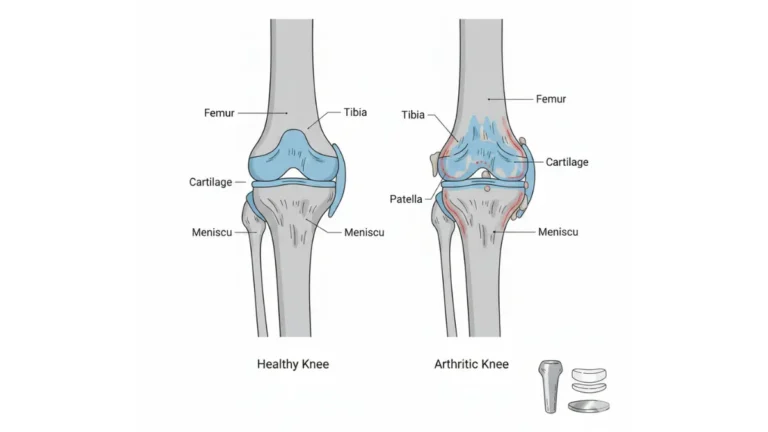
Total vs. Partial vs. Revision Knee Replacement
Selecting the appropriate procedure type determines long-term satisfaction and functional outcomes. Your damaged knee anatomy guides this critical decision.
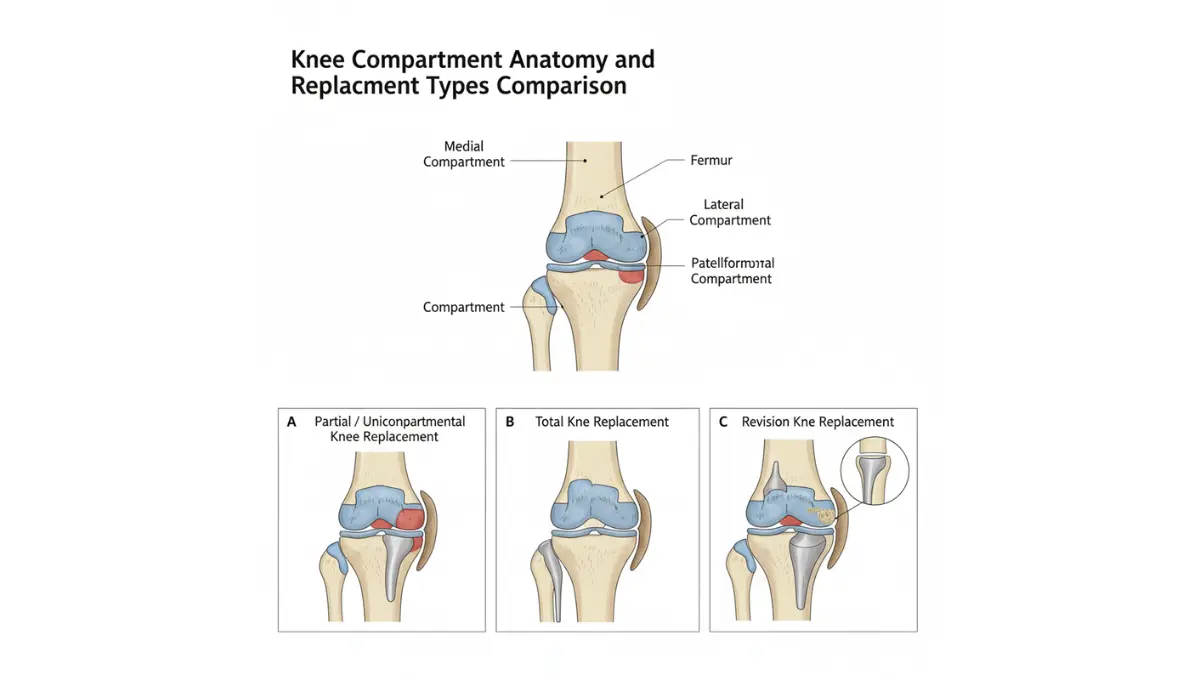
Total Knee Replacement (TKR):
- Replaces all three knee compartments (medial, lateral, patellofemoral)
- Best for: Multi-compartment arthritis, rheumatoid arthritis, post-traumatic damage
- Success rate: 95-97% function at 15 years, 82% at 25 years
- Recovery timeline: 3-6 months to full daily activities
- Implant lifespan: 15-25 years average
Partial (Unicompartmental) Knee Replacement:
- Replaces only damaged compartment (typically medial side)
- Best for: Single-compartment osteoarthritis with healthy ligaments
- Faster recovery: 4-6 weeks vs. 12+ weeks for total replacement
- More natural feel: Preserves 60-70% of original knee structure
- Higher revision rate: 15-20% require conversion to total within 10 years
Revision Knee Replacement:
- Removes failed implant and replaces with new components
- Required for: Implant loosening, infection, instability, wear
- More complex: 2-3 hour surgery vs. 90 minutes for primary
- Lower success rate: 85-90% vs. 95%+ for primary procedures
- Cost: $35,000-$65,000 (nearly double primary replacement)
Qualifying Criteria: Which Procedure Fits You?
| Factor | Partial Replacement | Total Replacement |
|---|---|---|
| Arthritis Location | Single compartment only | Multiple compartments |
| Ligament Integrity | ACL/PCL intact | Can accommodate damaged ligaments |
| Knee Deformity | <10 degrees varus/valgus | Any degree of deformity |
| Age Consideration | Often preferred ages 50-65 | Standard for 65+ |
| Activity Goals | High (running, sports) | Moderate (walking, golf) |
| Revision Risk | 15-20% at 10 years | 5-8% at 10 years |
Patients considering partial replacement should have damage limited to one compartment on X-ray imaging, intact cruciate ligaments, and realistic expectations about potential future conversion to total replacement.
Finding the Best Knee Replacement Surgeon in 2026
Surgeon selection impacts outcomes more than hospital choice for knee replacement procedures. Research analyzing 94,150 joint procedures found fellowship-trained orthopedic surgeons demonstrated 7% lower reoperation rates and 5% fewer emergency department visits compared to non-fellowship trained colleagues.
Essential Surgeon Qualifications Checklist:
- Board certification in orthopedic surgery (verify at ABOS.org)
- Fellowship training in adult reconstruction or sports medicine
- Minimum 50-100 knee replacements performed annually
- Hospital affiliation with joint replacement program certification
- Willingness to discuss personal complication and revision rates
- Experience with your specific procedure type (partial, robotic, revision)
Critical Questions to Ask During Consultation:
- How many knee replacements do you perform yearly? (Target: 75-150+)
- What percentage of your patients qualify for same-day discharge? (Target: 60-80%)
- What are your personal infection and revision rates? (Target: <2% infection, <5% revision at 10 years)
- Do you use robotic assistance? What are your outcomes with it?
- What implant brand do you prefer and why?
- Can you provide references from recent patients?
High-volume surgeons (100+ procedures annually) consistently deliver superior alignment precision but paradoxically show slightly higher revision rates due to treating more complex cases. Mid-volume surgeons (50-100 annually) often provide the optimal balance of experience and selective case acceptance.
Age Considerations: Timing Surgery for Best Outcomes
The “sweet spot” for knee replacement surgery occurs between ages 65-75, delivering optimal cost-effectiveness and implant longevity. Age-specific considerations:
Under Age 55:
- Higher revision risk (younger = more active = faster implant wear)
- Consider partial replacement to delay total procedure
- Modern implants lasting 20-25 years may eliminate need for revision
- Assess if 5-10 more years of conservative management is realistic
Ages 55-70 (Optimal Window):
- Lowest complication rates
- Fastest recovery times
- Peak cost-effectiveness
- 90%+ implant survival at 20 years
Ages 70-80:
- Excellent outcomes with careful patient selection
- Slower recovery (3-4 weeks vs. 2-3 weeks for younger patients)
- Lower activity demands preserve implant longer
- Highest satisfaction rates (94-97%)
Over Age 80:
- Case-by-case evaluation required
- Medical optimization critical (cardiac, pulmonary clearance)
- Consider partial replacement for faster recovery
- Success rate remains 90%+ with proper screening
Strategic Surgery Timing for Maximum Benefit
Insurance Deductible Optimization:
Schedule surgery in January-March after meeting annual deductibles, maximizing coverage for follow-up care, physical therapy, and potential complications through year-end. Avoid November-December scheduling requiring new deductibles for January rehabilitation.
Seasonal Recovery Advantages:
- Spring (March-May): Ideal for outdoor walking rehabilitation, vitamin D from sunshine accelerates healing
- Fall (September-November): Comfortable temperatures, avoids summer heat and winter ice hazards
- Avoid summer: Hot weather increases swelling and limits outdoor exercise tolerance
Professional Timing:
- Plan 8-12 weeks off for physically demanding jobs
- Desk workers often return part-time at 4-6 weeks
- Self-employed individuals schedule during anticipated slow business periods
- Coordinate with employer short-term disability benefits (typically 6-12 weeks)
Success Rates and Realistic Expectations
Modern knee replacement surgery achieves 95-97% success rates with proper patient selection and surgical technique. Understanding limitations prevents disappointment:
Activities You CAN Do Post-Replacement:
- Walking unlimited distances
- Swimming and water aerobics
- Cycling (stationary or road)
- Golf (with cart initially)
- Doubles tennis (6+ months post-op)
- Elliptical and rowing machines
- Low-impact hiking on moderate terrain
Activities to AVOID:
- Running and jogging (excessive implant stress)
- Contact sports (football, hockey, soccer)
- High-impact aerobics and jumping
- Squatting with heavy weights
- Kneeling on hard surfaces (uncomfortable but safe)
- Singles tennis and racquetball (high pivot stress)
Patient satisfaction rates reach 93-94% at 5 years, with dissatisfaction strongly correlated to unrealistic pre-operative expectations, untreated depression, and persistent opioid use beyond 3 months post-surgery. The 6% dissatisfaction rate primarily involves patients expecting complete pain elimination—while 90% achieve 80-90% pain reduction, most retain mild discomfort with extreme weather changes or prolonged standing.
What Success Actually Looks Like:
- 80-95% pain reduction (not 100% elimination)
- Walking 1-2 miles without significant discomfort
- Climbing stairs reciprocally (alternating legs)
- Getting in/out of cars without assistance
- Sleeping through night without knee pain waking you
- Returning to recreational activities (golf, cycling, swimming)
Long-term implant survival depends heavily on maintaining healthy body weight and avoiding high-impact activities. Patients gaining 30+ pounds post-surgery experience 3.2x higher revision rates at 10 years compared to weight-stable patients.
Frequently Asked Questions About Knee Replacement
1. How long does knee replacement surgery take?
Total knee replacement surgery typically takes 60-90 minutes, while robotic-assisted procedures take 90-110 minutes. Partial knee replacement is faster at 45-60 minutes. Total time in the surgical facility ranges 4-8 hours including pre-op preparation and post-anesthesia recovery.
2. Can you walk immediately after knee replacement?
Yes, most patients stand and take steps within 2-4 hours after surgery with physical therapist assistance. Same-day discharge protocols require walking 70+ meters (230 feet) and climbing 3-4 steps before leaving the facility. Full independent walking without assistive devices typically occurs at 2-4 weeks.
3. What is the most painful day after knee replacement?
Days 2-3 post-surgery are typically most painful as nerve blocks wear off and inflammation peaks. Pain levels decrease significantly by day 5-7 with proper medication management. Most patients rate pain at 6-7/10 during peak days, dropping to 3-4/10 by week 2.
4. How long do knee replacements last?
Modern knee implants last 15-25 years on average, with 95% surviving 15 years and 82% lasting 25 years. Younger patients (<55 years) may require revision surgery due to higher activity levels and longer lifespan. Factors affecting longevity include body weight, activity level, and surgical technique.
5. Is 70 too old for knee replacement surgery?
No, age 70 is within the optimal range for knee replacement (65-75 years shows best outcomes). Patients over 80 successfully undergo surgery with proper medical screening and achieve 90%+ success rates. Age alone doesn’t disqualify you—overall health, activity level, and medical conditions matter more.
6. What is the fastest way to recover from knee replacement?
Start physical therapy within 24 hours, perform exercises 3-4 times daily, maintain 1.2-1.5 grams protein per kilogram body weight, and get 7-9 hours sleep nightly. Ice therapy 20 minutes every 2 hours for the first week and stay ahead of pain with prescribed medication schedule. Patients following accelerated protocols achieve independence 5-7 days faster than those delaying rehabilitation.
7. Can you kneel after knee replacement?
Yes, kneeling is physically safe after knee replacement but often uncomfortable due to implant pressure against skin and tissue. About 60-70% of patients can kneel comfortably by 6-12 months post-surgery. Use kneeling pads or avoid prolonged kneeling on hard surfaces for comfort.
8. Will I set off metal detectors after knee replacement?
Knee implants may occasionally trigger airport metal detectors, though modern sensitivity settings reduce false alarms. Carry your surgical identification card (provided by hospital) when traveling. TSA agents are trained to handle orthopedic implants—simply inform them before screening if the alarm sounds.
9. When can I drive after knee replacement?
Most patients resume driving at 4-6 weeks for right knee replacement once off narcotic pain medication and able to perform emergency brake stop safely. Left knee replacement patients (with automatic transmission) often drive at 2-3 weeks. Your surgeon will assess reaction time and strength before clearance.
10. What happens if I don’t get knee replacement?
Delaying medically necessary knee replacement leads to progressive cartilage loss, increased bone damage, muscle atrophy, and compensatory injuries to hips and opposite knee. Chronic pain often causes depression, weight gain, and reduced quality of life. Waiting too long can result in more complex surgery with worse outcomes.
11. Does insurance cover knee replacement for arthritis?
Yes, Medicare and private insurance cover knee replacement for severe osteoarthritis when conservative treatments (physical therapy, injections, medications) fail for 6+ months and X-rays show significant joint damage. Pre-authorization requires documentation of pain level 7+/10, functional limitations, and failed non-surgical interventions. Approval rate exceeds 90% with proper documentation.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.