On This Page – Quick Medical Summary
When Michael, a 58-year-old from Ohio, received a diagnosis of hepatocellular carcinoma, his first question to his surgeon was: “What are my real chances?” His surgeon explained that at a high-volume center, his 5-year survival after liver resection could exceed 60%. He had the surgery — and two years later, his scans remain clear.
If you or a loved one is facing liver surgery, you deserve honest, current numbers — not vague reassurances. Here is what the data actually says in 2026.
Quick Answer: Liver resection success rates depend on cancer type and where surgery is performed. At specialist centers, 5-year survival reaches 45–65% for liver cancer (HCC), 25–58% for colorectal liver metastases, and 90-day mortality is below 3% at high-volume hospitals.
Liver Resection Results at a Glance
| Cancer Type | 5-Year Survival | 90-Day Mortality |
|---|---|---|
| Hepatocellular Carcinoma (HCC) | 45–65% | <3% (specialist) |
| Colorectal Liver Metastases (CRLM) | 25–58% | <5% |
| Intrahepatic Cholangiocarcinoma | 32% | 4–8% |
| Benign conditions (hemangioma, cysts) | Near 100% cure | <1% |
What Is Liver Resection? And Why Results Vary So Much
The Surgery That Can Beat Liver Cancer
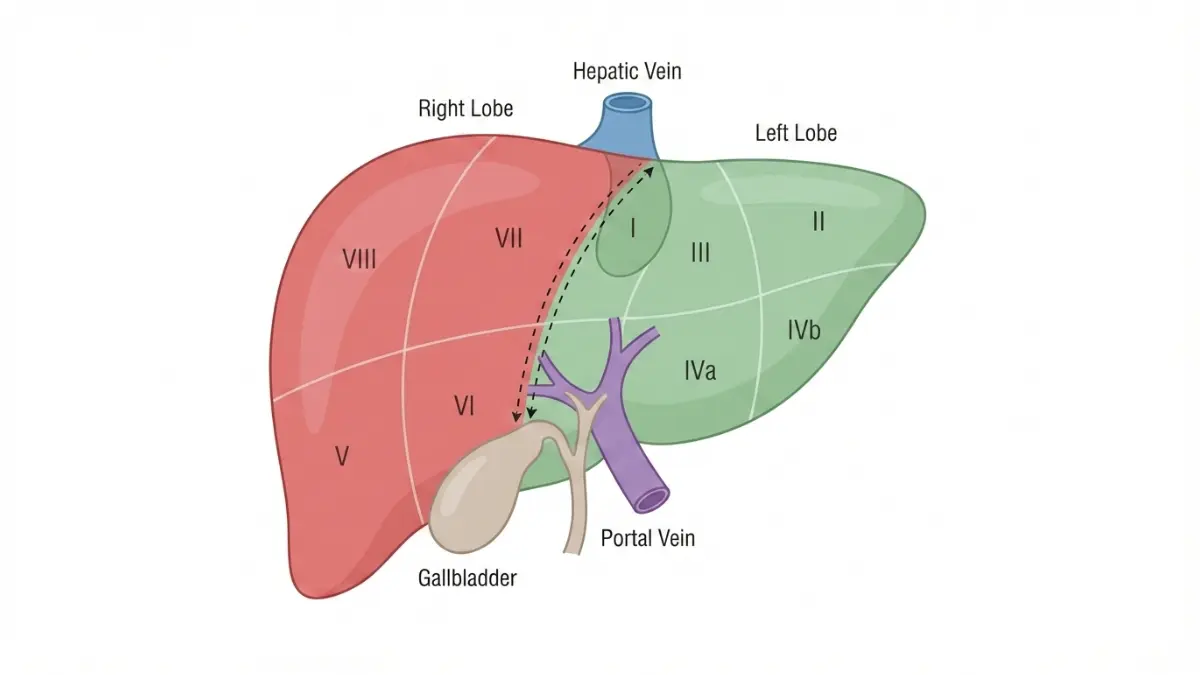
A liver resection — also called a hepatectomy or partial hepatectomy — is a surgical procedure to remove a diseased portion of the liver. It is the most effective curative treatment for eligible patients with primary or secondary liver cancer, according to the National Cancer Institute.
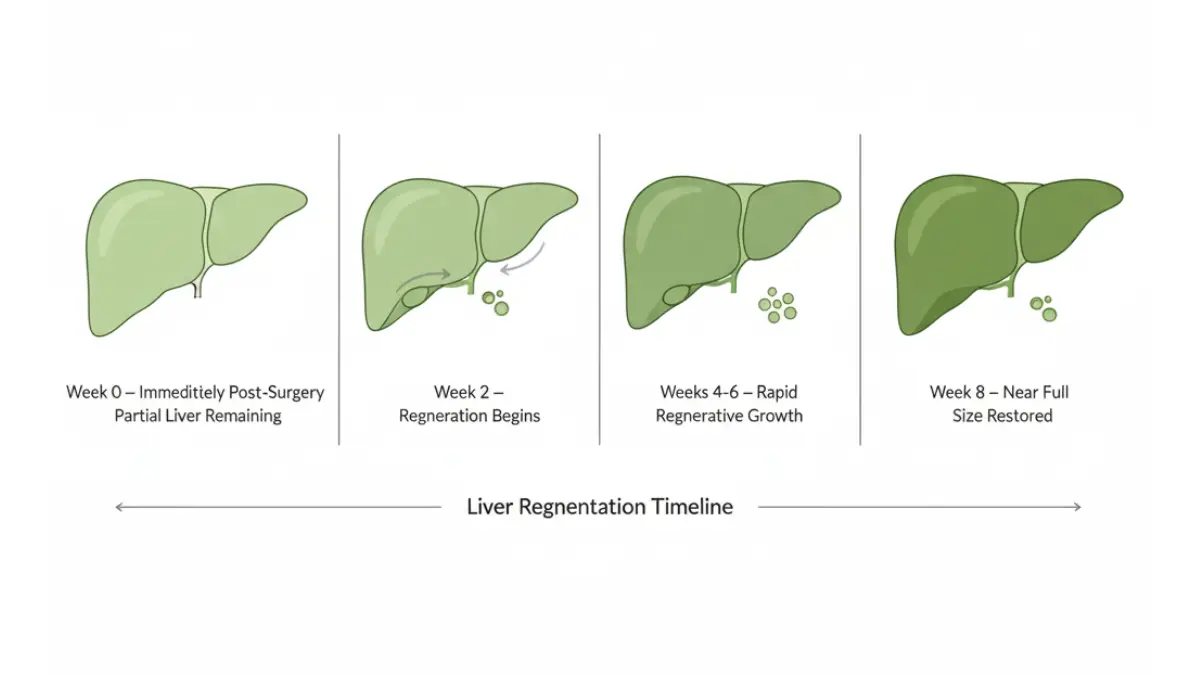
The liver is unique: it is the only major organ that regenerates. Up to 75% of the liver can be safely removed, and the remaining tissue grows back to near full size within 6–8 weeks in healthy patients.
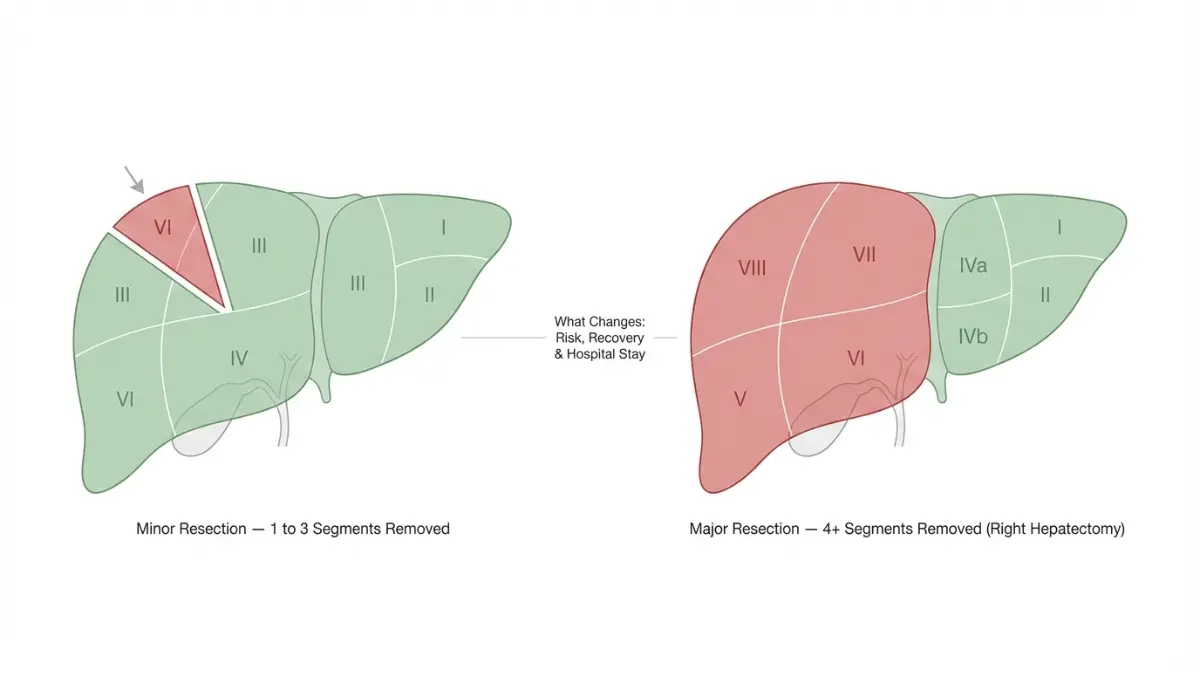
Not all liver resections are equal. Results vary significantly based on the extent of surgery:
Minor vs. Major Resection — Why It Changes Everything
| Feature | Minor Resection | Major Resection |
|---|---|---|
| Segments removed | 1–3 segments | 4+ segments |
| Hospital stay | 2–4 days | 5–10 days |
| 90-day mortality | <2% | 4–10% |
| Recovery time | 4–6 weeks | 8–12 weeks |
| Best approach | Laparoscopic | Often open or robotic |
Key takeaway: Minor resections at specialist centers are remarkably safe. Major resections require more careful patient selection and carry higher — though still manageable — risk.
Who Is a Candidate for Liver Resection Surgery?
Surgeons consider liver resection when:
- The tumor is confined to the liver (no distant spread)
- Enough healthy liver tissue will remain after surgery (≥25% in healthy patients, ≥40% if cirrhosis is present)
- The patient’s overall health can tolerate surgery
- Liver function tests (blood tests) show adequate reserve
If you are experiencing unexplained symptoms, use our Symptom Checker to identify patterns before your next clinical appointment — early identification of liver symptoms can affect candidacy and outcomes.
Real Liver Resection Survival Rates by Cancer Type (2026 Data)
This is the information no competitor gives you clearly. Here are condition-specific, peer-reviewed survival rates — the most important numbers a patient can have.
Hepatocellular Carcinoma (HCC) — What the Numbers Say
HCC is the most common primary liver cancer. When caught early and resected at a specialist center, outcomes are genuinely encouraging.
HCC Liver Resection Survival Rates (2026):
| Timeframe | Survival Rate |
|---|---|
| 1-year | 85–89% |
| 3-year | 64% |
| 5-year | 45–65% (up to 70% at top centers) |
| 10-year | 15–21% |
Source: ASCO multi-center data; high-volume hepatobiliary center series.
What This Means For You: If you have a single small HCC tumor, preserved liver function, and surgery at a high-volume center, your odds of 5-year survival are comparable to many early-stage cancers. Hospital choice matters enormously.
Colorectal Liver Metastases (CRLM) — When Cancer Spreads From the Colon
CRLM is the most common reason for liver resection in the United States. These are secondary liver tumors that spread from colorectal cancer. Resection is the only potentially curative treatment.
CRLM Survival Rates After Liver Resection:
| Timeframe | Survival Rate |
|---|---|
| 1-year | 91% |
| 3-year | 56% |
| 5-year | 25–58% |
| 10-year | 24% (with ~20% observed cure rate) |
Based on a 1,211-patient study from Johns Hopkins with 11-year median follow-up.
What This Means For You: Approximately 1 in 5 patients with colorectal liver metastases who undergo resection achieves genuine long-term cure — a fact rarely communicated to patients in plain language.
For patients monitoring blood sugar as part of colorectal cancer surveillance, our Blood Sugar Converter can help track glucose levels, which directly affect surgical risk and liver regeneration capacity.
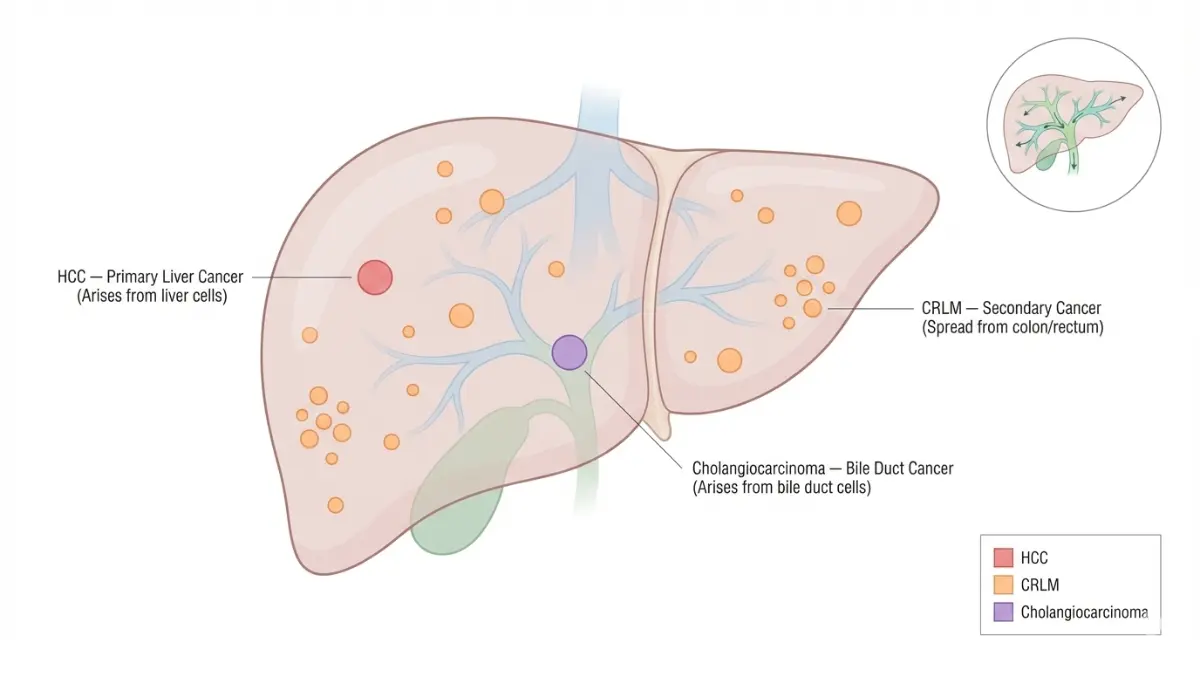
Intrahepatic Cholangiocarcinoma — Rarer but Resectable
Cholangiocarcinoma (bile duct cancer) is less common but equally important. The NCI liver cancer treatment guidelines confirm that complete surgical resection is the only curative option for intrahepatic cholangiocarcinoma.
- 5-year survival after R0 resection: ~32%
- 10-year survival: ~8.4%
- Complete removal (R0 margin) is the single most important predictor of long-term survival
Benign Conditions (Hemangioma, Cysts, Adenoma)
When liver resection is performed for benign disease, outcomes are excellent:
- 90-day mortality: <1% at specialist centers
- Symptom resolution rate: >90%
- Recurrence rate: very low with complete resection
7 Factors That Directly Affect Your Liver Resection Outcomes
Your results are not just determined by your diagnosis. Seven modifiable and non-modifiable factors predict whether liver resection surgery leads to long-term survival or early recurrence.
1. Hospital Volume — The Single Biggest Variable
Studies across 248,707 patients confirm that high-volume centers have up to 50% lower mortality than low-volume hospitals. Choose a hospital performing more than 50 liver resections per year.
2. Surgeon Specialization
A hepatobiliary-trained surgeon versus a general surgeon produces meaningfully different outcomes. Ask specifically whether your surgeon is HPB (hepato-pancreato-biliary) fellowship-trained.
3. Cancer Type and Stage
HCC, CRLM, and cholangiocarcinoma each have different baseline outcomes. Staging also matters: a solitary tumor under 3 cm has dramatically better outcomes than multiple large tumors.
4. Future Liver Remnant (FLR) Volume
- Healthy liver: FLR must be ≥25% of total liver volume
- Cirrhotic liver: FLR must be ≥40%
- Below these thresholds, surgery is withheld — post-hepatectomy liver failure is the leading cause of death after liver resection
5. Presence of Cirrhosis
Patients with cirrhosis face higher risk from liver resection. Child-Pugh Class A patients are the best surgical candidates. Class C cirrhosis is an absolute contraindication.
6. Surgical Approach
Laparoscopic and robotic approaches produce 89% fewer complications and 39% shorter hospital stays compared to open surgery in eligible patients. However, open surgery remains essential for complex major resections.
7. Pre-Surgery Health Optimization
Patients enrolled in Enhanced Recovery After Surgery (ERAS) protocols experience 30–40% fewer complications. Optimizing nutrition, stopping smoking 4–6 weeks before surgery, and managing blood pressure all independently improve outcomes.
If you have underlying risk factors such as hereditary liver disease, consider using our Genetic Risk Assessment Tool to understand your baseline risk profile before discussing surgical candidacy with your physician.
✅ 5 Questions to Ask Your Surgeon Before Liver Resection:
- How many liver resections does your center perform per year?
- Are you HPB fellowship-trained?
- What is your center’s 90-day mortality rate for this type of resection?
- Will I be on an ERAS protocol?
- What is my estimated Future Liver Remnant (FLR) volume?
Liver Resection Recovery: What Really Happens Week by Week
Recovery from liver resection varies significantly between patients, cancer types, and surgical approaches. Here is the honest week-by-week breakdown competitors do not provide.
Recovery Timeline After Liver Resection
| Phase | Timeline | What Happens |
|---|---|---|
| Hospital stay | Days 1–7 | Pain management, drain monitoring, liver function tests every 24–48 hours |
| Early recovery | Weeks 1–4 | Light walking, soft diet, wound healing; avoid lifting >10 lbs |
| Intermediate | Weeks 4–8 | Driving may resume (open: week 6–8; laparoscopic: week 3–4) |
| Return to work | Weeks 4–12 | Desk work: 4–6 weeks; physical labor: 10–12 weeks |
| Liver regeneration | Weeks 6–8 | Liver regrows to near-original functional size |
| Long-term surveillance | Every 3–6 months | CT/MRI scans, AFP (for HCC) or CEA levels (for CRLM) |
When James, a 64-year-old teacher from Texas, underwent laparoscopic liver resection for a 4 cm HCC tumor, he was walking the hospital corridor within 48 hours and back in his classroom at week 6 — without chemotherapy.
What This Means For You: Laparoscopic patients typically return to normal activity 3–4 weeks faster than open surgery patients. If you are eligible for minimally invasive liver resection, this is a quality-of-life advantage worth discussing with your care team.
⚠️ Warning Signs to Call Your Doctor Immediately Post-Surgery:
- Fever above 101°F (38.3°C)
- Sudden severe abdominal pain
- Yellowing of skin or eyes (jaundice)
- Dark urine or clay-colored stools
- Swelling in the abdomen
- Confusion or sudden fatigue
Good quality sleep accelerates liver regeneration significantly. Our Sleep Calculator helps you plan an optimal rest schedule during your recovery period — poor sleep has been shown to impair post-surgical immune function.
Laparoscopic vs. Open vs. Robotic Liver Resection — What the 2026 Data Shows
The method of liver resection surgery directly impacts your recovery speed, complication rate, and quality of life — though long-term cancer survival is equivalent across all three approaches.
3-Way Head-to-Head: Laparoscopic vs. Open vs. Robotic
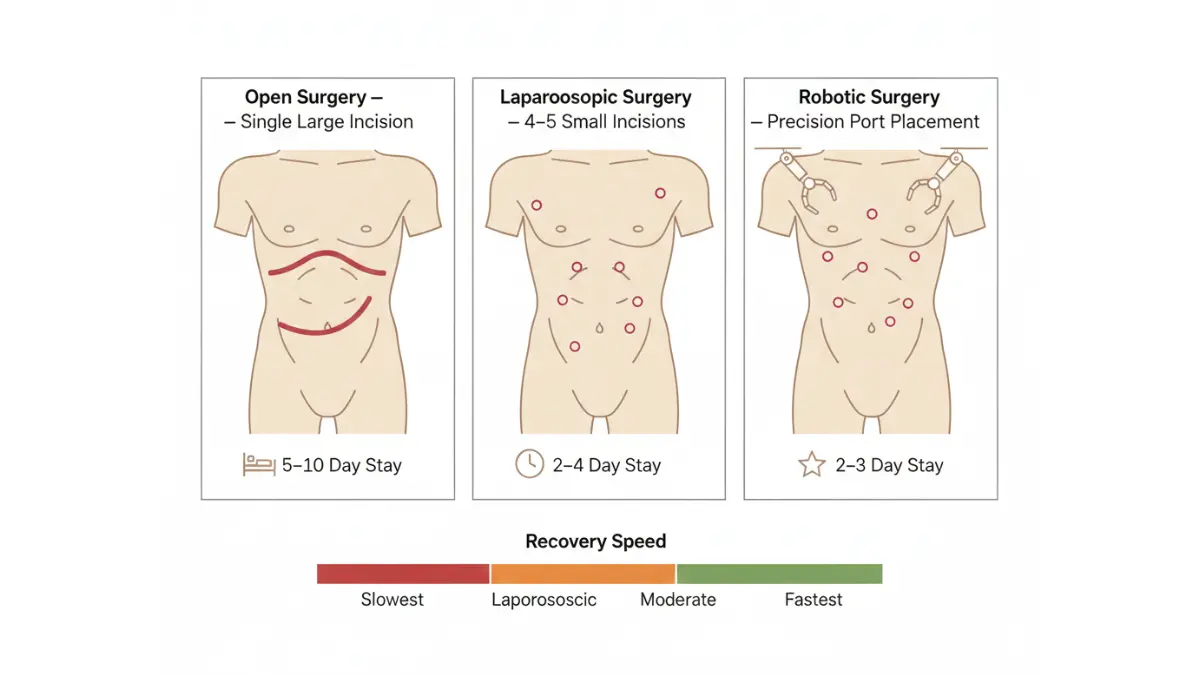
| Metric | Laparoscopic | Open Surgery | Robotic (2026) |
|---|---|---|---|
| Hospital stay | 2–4 days | 5–10 days | 2–3 days |
| Complication rate | Up to 89% lower than open | Baseline (reference) | Superior to laparoscopic |
| Blood loss | Significantly lower | Higher | Lowest of all 3 |
| Conversion to open | 10–15% of cases | N/A | 87% lower than laparoscopic |
| 5-year cancer survival | Equivalent | Equivalent | Equivalent |
| Best for complex cases | Moderate complexity | High complexity | Increasing range |
The 2026 Robotic Revolution: At specialized centers, robotic liver resection usage rose from 36% to 68% between 2017–2023, while laparoscopic use dropped from 39% to 9%. Robotic surgery now achieves better outcomes in complex hepatectomies that were previously open-only cases.
What This Means For You: Ask your center specifically about robotic options — especially for technically difficult segments (Segments 7 and 8). This is not available everywhere, but it represents the fastest-growing advancement in liver surgery outcomes.
For patients also navigating related gastrointestinal concerns, our guide on laparoscopic surgery success rates covers minimally invasive outcomes across a range of abdominal procedures.
How to Maximize Your Liver Resection Results in 2026
Your surgical outcome is not entirely in your surgeon’s hands. These evidence-based steps — before and after surgery — directly improve liver resection results.
Before Surgery: Preparation That Changes Your Outcome
- Choose a high-volume HPB center (>50 resections/year) — the single highest-impact decision you can make
- Optimize your BMI before surgery — obesity increases complication risk significantly. Use our BMI Calculator to assess your current status
- Stop smoking at least 4–6 weeks before surgery — smoking impairs liver regeneration and wound healing
- Manage diabetes aggressively — uncontrolled blood sugar is an independent predictor of post-hepatectomy complications
- Ask about prehabilitation — structured exercise and nutritional optimization in the weeks before surgery has been shown to reduce complication rates by up to 30%
- Ensure adequate protein intake — protein is the building block of liver regeneration; our Protein Intake Calculator helps you calculate your daily target
After Surgery: What Accelerates Healing
- Walk as early as possible — mobilization within 24–48 hours post-surgery reduces pneumonia and blood clot risk
- Follow a high-protein, low-fat diet — supports liver cell regeneration
- No alcohol — even small amounts impair liver regeneration after hepatectomy; avoid completely for at least 6 months
- Never miss a surveillance scan — early recurrence detection saves lives. Most liver cancer recurrences after resection occur in the first 2 years
Long-Term: Surveillance That Saves Lives
For patients who have undergone liver resection for cancer, the post-surgery monitoring schedule is not optional — it is lifesaving.
- HCC patients: AFP blood test + MRI or CT every 3–6 months for 2 years, then every 6 months
- CRLM patients: CEA blood test + CT chest/abdomen every 3–6 months for 3 years
- Cholangiocarcinoma patients: CA19-9 blood test + imaging every 3–4 months
For additional context on understanding your liver function test numbers after surgery, our detailed guide on LFT results explains what each value means and when to act. You may also find our guide on liver cancer early signs and symptoms useful for monitoring purposes during your long-term follow-up period.
The American Liver Foundation’s patient resources provide additional support tools, clinical trial access, and community programs for patients recovering from liver surgery and managing ongoing liver health.
11 Frequently Asked Questions About Liver Resection Results
1. What is the success rate of liver resection?
At high-volume specialist centers, success rates exceed 97% for procedure completion with fewer than 3% 90-day mortality. Long-term success depends on cancer type — HCC 5-year survival reaches 65%, CRLM reaches 58% in best-case scenarios.
2. What is the 5-year survival rate after liver resection for liver cancer (HCC)?
Expected 5-year survival after HCC resection is 45–65% at specialist centers, with 1-year survival of 85–89%. Patients with a single small tumor and preserved liver function achieve the best outcomes.
3. Is liver resection a major surgery?
Minor liver resection (1–3 segments, laparoscopic) is considered moderate complexity with a short hospital stay. Major liver resection (4+ segments, often open) is a high-complexity procedure requiring a specialist center and carries higher short-term risk.
4. How long does recovery from liver resection take?
Laparoscopic patients typically return to light activity in 3–4 weeks. Open surgery patients require 8–12 weeks for full recovery. Liver regeneration to near-original size takes 6–8 weeks regardless of surgical approach.
5. Can the liver grow back after resection?
Yes. The liver is the only major organ that regenerates. Up to 75% can be removed in healthy patients, with the remaining liver growing back to near-original functional size within 6–8 weeks.
6. What is the mortality rate for liver resection?
At high-volume specialist centers, 90-day mortality is below 3% for most resections. At low-volume hospitals, mortality risk can be up to double. Major resections (4+ segments) carry a 4–10% mortality rate even at expert centers.
7. What are the most common complications after liver resection?
The most common serious complications include post-hepatectomy liver failure (1–8%), bile leak (3%), pleural effusion (9%), wound infection (5%), and blood clots. Most complications are manageable when identified early.
8. Is laparoscopic liver resection safer than open surgery?
For eligible patients, laparoscopic resection produces up to 89% fewer complications, shorter hospital stays, and faster recovery with equivalent long-term cancer survival. Not all patients or tumor locations are suitable for laparoscopic approach.
9. What factors predict good liver resection outcomes?
Hospital volume, surgeon specialization, cancer type and stage, Future Liver Remnant (FLR) ≥25–40%, absence of cirrhosis or well-compensated (Child-Pugh A) cirrhosis, and early-stage disease at diagnosis.
10. How much liver can be safely removed?
Healthy liver patients can safely have up to 75% removed. Patients with cirrhosis, fatty liver, or chemotherapy damage require a larger remnant — typically 40–60% of the total liver must remain functional.
11. Does liver resection cure liver cancer?
For carefully selected patients, liver resection is genuinely curative. Approximately 20% of CRLM patients who undergo resection achieve observed 10-year cure. HCC patients with small solitary tumors and preserved liver function have 5-year survival rates comparable to many Stage II cancers. Early detection and specialist surgery maximize the chance of cure.
Sources: National Cancer Institute (cancer.gov), LiverMetSurvey International Registry (43 centers, 12,154 patients), American Society of Clinical Oncology, Johns Hopkins Hepatobiliary Surgery Database, Nature Scientific Reports 2025.
This article is for educational and informational purposes only. It does not replace professional medical advice, diagnosis, or treatment. Always seek the guidance of a qualified healthcare provider with any questions about your medical condition.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











