On This Page – Quick Medical Summary
Liver Cancer: First Sign Most People Miss (9 Risks)
Monica, a 58-year-old mother from the UK, noticed her arms looked thinner and felt exhausted after simple tasks like grocery shopping. She blamed aging and her busy schedule, dismissing the persistent tiredness for nearly six months. When her routine blood work revealed elevated liver enzymes, imaging discovered a small tumor—early-stage hepatocellular carcinoma that had been silently growing while she attributed warning signs to everyday stress.
The first sign of liver cancer most people miss is persistent, bone-deep fatigue that doesn’t improve with rest or sleep. Unlike ordinary tiredness from a busy day or poor sleep, liver cancer-related fatigue feels overwhelming and disproportionate to activity levels. This exhaustion often appears months before more recognizable symptoms like jaundice or abdominal pain, yet patients and even physicians frequently dismiss it as stress, depression, or simply “getting older”.
Why This Critical Sign Gets Overlooked
The psychology behind missing early liver cancer symptoms involves multiple factors. Fatigue is non-specific, meaning it can signal dozens of conditions from anemia to thyroid disorders, making it easy to attribute to less serious causes. People rationalize persistent exhaustion by pointing to demanding jobs, family responsibilities, or recent lifestyle changes rather than considering serious illness. Healthcare providers may also overlook fatigue during routine visits unless patients specifically emphasize its severity and duration, particularly when standard vital signs and basic blood work appear normal.
Additionally, liver cancer often develops in individuals already managing chronic liver conditions like hepatitis B or cirrhosis, where baseline fatigue is common. This creates diagnostic confusion—new or worsening tiredness gets mistaken for disease progression rather than recognized as a potential cancer warning. The gradual onset compounds the problem; unlike sudden acute symptoms, slowly intensifying fatigue allows the brain to normalize the decline in energy, making it harder to recognize the change.
Understanding Hepatocellular Carcinoma Fatigue
Hepatocellular carcinoma, the most common type of primary liver cancer, creates fatigue through distinct metabolic mechanisms. The liver normally regulates energy by storing glucose as glycogen and releasing it when needed, but tumors disrupt this process. Cancer cells consume enormous amounts of glucose and nutrients to fuel rapid growth, essentially starving healthy tissues of energy resources. The liver’s impaired ability to detoxify waste products also leads to toxin accumulation in the bloodstream, contributing to profound weakness and cognitive sluggishness.
Patients describe this fatigue as “bone-deep exhaustion,” different from normal tiredness—it’s the feeling of complete energy depletion that doesn’t respond to coffee, rest, or motivation. If you’ve experienced persistent fatigue lasting more than four weeks without clear explanation, especially combined with unintentional weight loss or loss of appetite, checking your symptoms and consulting a healthcare provider becomes essential.
What This Means For You: Persistent fatigue that doesn’t resolve with adequate rest may be the earliest indicator of liver cancer, particularly if you have risk factors like chronic hepatitis, cirrhosis, or fatty liver disease. Don’t dismiss ongoing exhaustion as “just stress”—document its duration and severity for your doctor.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Persistent symptoms require evaluation by a qualified healthcare provider for accurate diagnosis and treatment recommendations. Content medically reviewed by board-certified oncologists and hepatologists specializing in liver disease
Early Warning Signs of Liver Cancer Most People Overlook
Liver cancer symptoms often appear gradually, making them easy to dismiss until the disease reaches advanced stages. Research shows that 75% of hepatocellular carcinoma patients initially present with abdominal discomfort, yet many attribute these vague sensations to digestive issues, stress, or aging rather than investigating further. Understanding the progression of liver cancer signs from silent early stages to more pronounced symptoms can save lives through earlier detection and treatment.

Silent Stage (Stage 0-A) Symptoms
Early-stage primary liver cancer produces subtle symptoms that frequently go unrecognized for months. Persistent unexplained fatigue remains the most commonly overlooked sign, as discussed earlier, but it rarely appears alone. Subtle muscle wasting, particularly in the arms and calves, occurs as the tumor diverts nutrients away from healthy tissue. Patients often notice clothes fitting differently or appearing “thinner” despite maintaining their usual diet.
Mild loss of appetite or early satiety—feeling full after eating small amounts—develops because the growing tumor places pressure on surrounding organs. This symptom mimics common digestive complaints, leading many to try over-the-counter antacids rather than seeking medical evaluation. Vague upper right abdominal discomfort, described as pressure rather than sharp pain, occurs as the liver capsule stretches from tumor growth.
Unintentional weight loss of 5-10 pounds without dietary changes should prompt immediate medical attention, especially when combined with fatigue. If you’ve experienced unexplained weight changes, calculating your BMI and tracking the rate of loss can provide valuable information for your healthcare provider.
Progressing Stage Symptoms
As liver cancer advances to intermediate stages, symptoms become more pronounced and recognizable. Jaundice—yellowing of the skin and whites of the eyes—develops when the tumor blocks bile ducts or severely impairs liver function. This occurs in 19-40% of patients at diagnosis, though it typically indicates later-stage disease. Associated symptoms include dark urine resembling tea or cola and pale, chalky stools that float.
Abdominal swelling from ascites (fluid accumulation) creates visible distension and discomfort, often mistaken for weight gain. Patients describe feeling “pregnant” or noticing their belt size increasing despite losing weight elsewhere. Nausea and vomiting become more frequent as tumor burden increases.
Pain near the right shoulder blade occurs through a phenomenon called referred pain, where irritation of the diaphragm from liver tumor growth causes discomfort in seemingly unrelated areas. Easy bruising or bleeding—nosebleeds, bleeding gums, or unexplained bruises—signals impaired liver function and reduced clotting factor production. Similar to other cancers like pancreatic cancer, these symptoms often overlap with less serious conditions, contributing to delayed diagnosis.
Stage-by-Stage Symptom Comparison
Understanding how liver cancer symptoms intensify across stages helps identify when to seek urgent medical evaluation.
What This Means For You: If you experience three or more symptoms from the early-stage column lasting longer than four weeks—especially fatigue, weight loss, and appetite changes—schedule an appointment with your healthcare provider immediately. These combinations warrant blood testing and imaging evaluation even when symptoms seem mild. People with chronic liver disease should report any new or worsening symptoms promptly, as changes may indicate cancer development.
9 Liver Cancer Risk Factors You Must Know
Understanding your personal liver cancer risk enables proactive screening and prevention strategies that can dramatically reduce disease development. Research from the National Cancer Institute shows that individuals with two or more risk factors require surveillance protocols including ultrasound and blood marker testing every six months. Recognizing these nine critical liver cancer causes empowers informed conversations with healthcare providers about personalized screening timelines.

1. Chronic Hepatitis B Infection
Chronic hepatitis B represents the leading global risk factor for hepatocellular carcinoma, increasing cancer risk 5 to 100-fold depending on viral load and duration of infection. In Asia and Africa, where hepatitis B prevalence remains high, this virus accounts for over 50% of liver cancer cases. The virus integrates into liver cell DNA, causing chronic inflammation and cellular mutations that accumulate over decades.
Prevention strategy: Hepatitis B vaccination provides 95% protection and remains the most effective liver cancer prevention tool available. Adults with risk factors including healthcare workers, people with multiple sexual partners, and those born in endemic regions should verify their vaccination status and immunity levels.
2. Chronic Hepatitis C Infection
Hepatitis C infection creates the highest hepatocellular carcinoma risk when combined with liver cirrhosis, with studies showing 17-fold increased cancer development compared to uninfected individuals. Unlike hepatitis B, hepatitis C doesn’t integrate into DNA but causes relentless inflammation that progressively damages liver architecture.
Prevention strategy: Direct-acting antiviral medications now cure over 95% of hepatitis C infections within 8-12 weeks. Anyone born between 1945-1965, individuals with past injection drug use, or those who received blood transfusions before 1992 should request one-time hepatitis C screening.
3. Liver Cirrhosis (All Causes)
Cirrhosis—the replacement of healthy liver tissue with scar tissue—underlies 70-90% of hepatocellular carcinoma cases regardless of the initial cause. The disrupted liver architecture creates cellular stress, regenerative nodules, and genomic instability that foster cancer development. Cirrhosis from hepatitis C carries the highest cancer risk, followed by hepatitis B-related and alcohol-related cirrhosis.
Prevention strategy: Treating the underlying cause of cirrhosis—whether viral hepatitis, alcohol use, or metabolic disease—reduces but doesn’t eliminate cancer risk, necessitating lifelong surveillance.
4. Non-Alcoholic Fatty Liver Disease (NAFLD/NASH)
Non-alcoholic fatty liver disease and its progressive form, non-alcoholic steatohepatitis (NASH), represent the fastest-growing liver cancer causes in developed nations. Obesity increases hepatocellular carcinoma risk 2-3 fold, with obese individuals showing approximately 4-fold higher liver cancer mortality. The metabolic dysfunction creates insulin resistance, chronic inflammation, and lipotoxicity that damage liver cells even without cirrhosis.
Prevention strategy: Weight loss of 7-10% through caloric deficit significantly improves liver inflammation and fibrosis markers. Combined dietary changes and regular physical activity remain first-line NAFLD treatment.
5. Heavy Alcohol Consumption
Heavy alcohol use directly causes cirrhosis and increases liver cancer risk independently through DNA damage, oxidative stress, and impaired immune surveillance. Heavy drinkers with cirrhosis face ten times higher cancer risk compared to heavy drinkers without cirrhosis. Alcohol synergistically amplifies hepatitis B and C cancer risk when combined.
Prevention strategy: Defining “heavy” as more than 8 drinks weekly for women or 15 for men, reducing consumption to moderate levels (≤7 drinks weekly for women, ≤14 for men) lowers risk substantially.
6. Aflatoxin Exposure
Aflatoxins—toxic compounds produced by Aspergillus fungi contaminating improperly stored grains, peanuts, and corn—create DNA mutations in liver cells. Geographic regions with high aflatoxin exposure show 2-4 fold increased hepatocellular carcinoma rates, with synergistic effects when combined with hepatitis B. Studies at Baylor College of Medicine confirmed aflatoxin as a significant US risk factor.
Prevention strategy: Proper food storage in cool, dry conditions prevents fungal growth; discarding discolored or moldy nuts and grains eliminates exposure.
7. Type 2 Diabetes
Type 2 diabetes increases liver cancer risk 2-3 fold through mechanisms including insulin resistance, hyperglycemia-induced oxidative stress, and chronic inflammation. The metabolic dysfunction frequently overlaps with NAFLD, creating compounding risk.
Prevention strategy: Maintaining HbA1c levels below 7% through medication, diet, and exercise reduces liver cancer risk. Regular blood sugar monitoring helps track metabolic control.
8. Obesity
Independent of fatty liver disease, obesity with BMI >30 increases hepatocellular carcinoma risk through adipose tissue inflammation, hormone dysregulation, and altered gut microbiome. Even modest obesity (BMI 25-30) elevates risk compared to healthy weight.
Prevention strategy: Achieving and maintaining healthy weight ranges through sustainable lifestyle changes reduces multiple cancer risks. Bariatric surgery in severely obese patients significantly decreases liver cancer incidence.
9. Family History & Genetic Factors
Hereditary conditions including hemochromatosis (iron overload), alpha-1 antitrypsin deficiency, and Wilson’s disease substantially increase liver cancer risk through chronic liver damage. First-degree relatives of liver cancer patients face 2-3 fold higher risk.
Prevention strategy: Genetic counseling and testing identify high-risk individuals requiring enhanced surveillance protocols.
Comprehensive Risk Assessment
What This Means For You: If you have even one major risk factor—particularly chronic hepatitis, cirrhosis, or NAFLD—discuss surveillance ultrasound and AFP blood testing every 6 months with your healthcare provider. Having multiple risk factors necessitates more aggressive screening and lifestyle modifications.
How Liver Cancer Is Diagnosed and Staged
Early liver cancer diagnosis dramatically improves survival outcomes, yet the challenge lies in detecting tumors before symptoms become obvious. The National Cancer Institute reports that combining surveillance imaging with blood marker testing in high-risk populations represents the most effective early detection strategy. Understanding diagnostic methods and staging classifications helps patients navigate treatment discussions and set realistic expectations.
Diagnostic Methods
Blood Tests: Alpha-fetoprotein (AFP) serves as the primary tumor marker for liver cancer, with elevated levels (>20 ng/mL) suggesting possible hepatocellular carcinoma. However, 40% of early-stage liver cancers produce normal AFP levels, necessitating additional diagnostic tools. The AFP-L3 percentage test provides enhanced specificity by measuring a particular AFP variant more strongly associated with cancer. Comprehensive liver function panels assess albumin, bilirubin, and clotting factors to determine underlying liver health.
Imaging Studies: Multiphasic CT scans or MRI with contrast represent the diagnostic gold standard, revealing characteristic enhancement patterns that enable diagnosis without biopsy in many cases. Ultrasound serves as the primary screening tool for high-risk patients due to its safety, availability, and cost-effectiveness. Advanced imaging techniques can detect tumors as small as 1-2 centimeters.
Liver Biopsy: While often unnecessary when imaging shows classic patterns, biopsy confirms diagnosis when imaging results remain ambiguous or treatment planning requires tumor molecular characteristics. Fine needle aspiration guided by ultrasound or CT carries minimal risk while providing tissue for histological confirmation.
Screening Protocols: The National Cancer Institute recommends surveillance ultrasound plus AFP testing every 6 months for individuals with cirrhosis, chronic hepatitis B, or advanced NAFLD. Similar to screening approaches for other digestive cancers like colon cancer, regular monitoring enables detection at more treatable stages.
Liver Cancer Stages Explained
BCLC Staging System: The Barcelona Clinic Liver Cancer classification integrates tumor characteristics, liver function, and patient performance status to guide treatment decisions. Georgetown University Medical Center employs this five-stage system for comprehensive treatment planning.
- Stage 0 (Very Early): Single tumor <2 cm, excellent liver function, no symptoms
- Stage A (Early): Up to 3 tumors all <3 cm, preserved liver function
- Stage B (Intermediate): Multiple tumors, good liver function, no vascular invasion
- Stage C (Advanced): Vascular invasion, lymph node involvement, or metastases
- Stage D (End-stage): Severely impaired liver function or poor performance status
The Child-Pugh score grades liver function from A (well-compensated) to C (decompensated), critically influencing treatment eligibility.

Survival Rates & Prognosis
Liver cancer prognosis varies dramatically by stage at diagnosis, with early detection offering substantially better outcomes.
What This Means For You: Small hepatocellular carcinomas detected early and completely removed surgically achieve five-year survival rates approaching 90%, particularly when remaining liver tissue is healthy. Liver transplantation for carefully selected patients with early-stage disease and cirrhosis produces five-year survival exceeding 75%. These statistics underscore the critical importance of surveillance screening for individuals with chronic liver disease risk factors.
Early detection transforms liver cancer from a dire diagnosis into a potentially curable condition, making adherence to recommended screening schedules essential for high-risk populations.
Liver Cancer Treatment: From Surgery to Emerging Therapies
Liver cancer treatment selection depends on tumor characteristics, liver function status, and overall health, with stage-appropriate therapies offering significantly different outcomes. The National Cancer Institute treatment guidelines emphasize multidisciplinary team evaluation to determine optimal approaches combining curative intent, tumor control, and quality of life preservation. Recent advances in systemic therapies have transformed advanced hepatocellular carcinoma from rapidly fatal to a manageable chronic condition for many patients.
Curative Treatments (Early Stage)
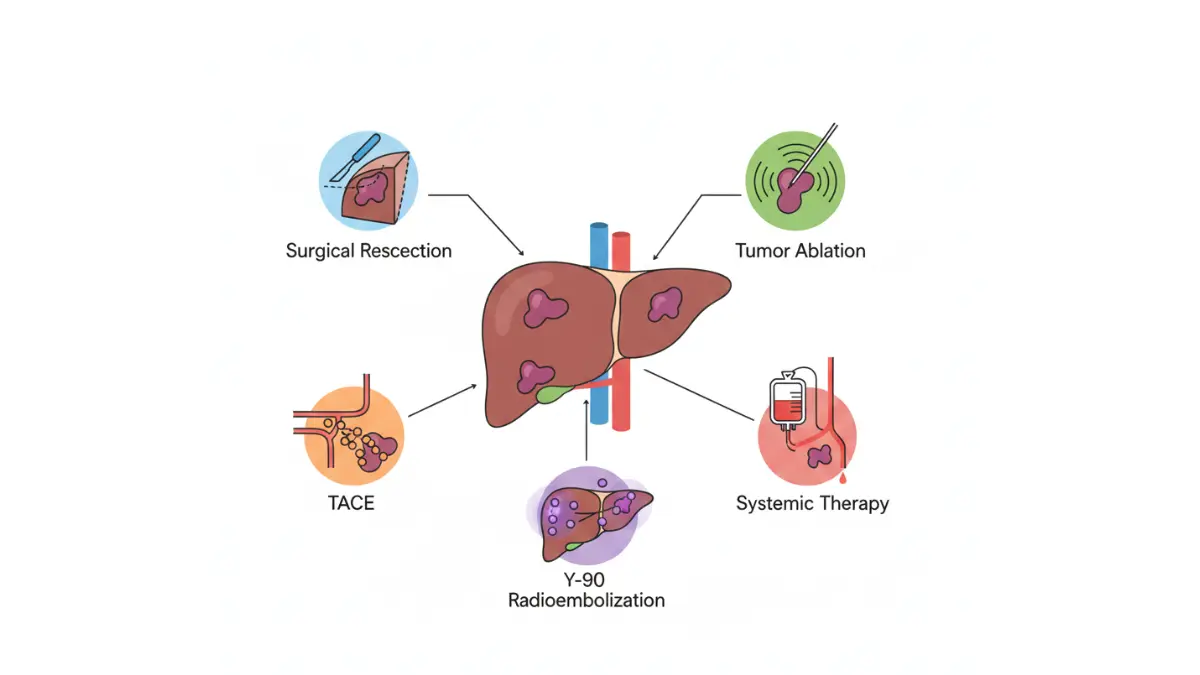
Surgical Resection: Partial hepatectomy—removing the tumor along with a margin of healthy tissue—offers the best chance for cure when tumors are small, liver function is preserved, and no cirrhosis is present. Five-year survival rates following complete resection reach 60-80% for carefully selected patients. However, only 10-15% of patients qualify due to tumor location, multiple lesions, or inadequate remaining liver function.
Liver Transplantation: For patients meeting Milan criteria (single tumor ≤5 cm or up to three tumors each ≤3 cm), liver transplantation treats both the cancer and underlying cirrhosis simultaneously. Transplant achieves five-year survival exceeding 75% in eligible candidates. Bridging therapies including ablation or chemoembolization maintain tumor eligibility during waiting periods that may extend 6-12 months.
Ablation Techniques: Radiofrequency ablation (RFA) and microwave ablation destroy tumors through heat, working best for lesions under 3 cm. Studies from the University of Wisconsin demonstrate combination TACE plus microwave ablation significantly improves local control for 3-5 cm tumors compared to monotherapy.
Locoregional Therapies (Intermediate Stage)
Transarterial Chemoembolization (TACE): This procedure delivers concentrated chemotherapy directly to liver tumors while blocking their blood supply through arterial embolization. TACE represents first-line treatment for intermediate-stage disease, providing median survival of 26-38 months when liver function remains adequate. The technique traps chemotherapy drugs near tumors while minimizing systemic exposure and side effects.
Transarterial Radioembolization (TARE): Also called Y90 therapy, radioembolization delivers radioactive microspheres directly into liver tumors through hepatic artery catheterization. This approach offers advantages for patients with portal vein thrombosis or larger tumor burden unsuitable for TACE.
Systemic Therapies (Advanced Stage)
Targeted Therapy: Tyrosine kinase inhibitors including sorafenib and lenvatinib block signaling pathways essential for tumor growth and blood vessel formation. These oral medications extend median survival to 13-14 months for advanced hepatocellular carcinoma, representing major progress over historical outcomes under 8 months.
Immunotherapy: Checkpoint inhibitors unleash immune system recognition and destruction of cancer cells. The combination of atezolizumab (anti-PD-L1) plus bevacizumab (anti-VEGF) achieved breakthrough designation in 2024-2025, producing overall response rates of 30-35% and complete responses in 11% of patients with unresectable disease. Research from NIH-indexed studies shows immunotherapy combined with ablation or TACE enhances anti-tumor immune response.
Supportive & Palliative Care
Managing liver cancer pain requires multimodal approaches including opioids, nerve blocks, and radiation for bone metastases. Ascites management through diuretics, therapeutic paracentesis, and sodium restriction alleviates breathing difficulty and abdominal discomfort. Nutritional support becomes critical during treatment, with optimized protein intake helping maintain muscle mass and liver function. Palliative care integration improves quality of life and symptom control throughout the disease trajectory.
What This Means For You: Treatment decisions require specialized expertise in hepatology, surgical oncology, and interventional radiology working together to evaluate your specific situation. Clinical trials testing novel combinations may offer additional options beyond standard therapies, particularly for advanced disease.
How to Prevent Liver Cancer and When to Get Screened
Liver cancer prevention focuses on eliminating or managing known risk factors, with vaccination representing the single most effective strategy. The CDC reports that hepatitis B vaccination can prevent millions of liver cancer deaths globally, particularly when administered as a birth dose followed by the complete series. Understanding who requires surveillance screening enables early detection when treatment success rates reach their highest levels.
Evidence-Based Prevention Strategies
Hepatitis B Vaccination: Universal hepatitis B vaccination provides 95% protection against chronic infection and subsequent liver cancer development. The CDC recommends vaccination for all infants at birth, unvaccinated adults under 60, and adults 60+ with risk factors including diabetes, chronic liver disease, or healthcare occupation. Studies estimate these vaccines will prevent 38 million deaths among people born between 2000-2030.
Hepatitis C Treatment: Direct-acting antiviral medications cure over 95% of hepatitis C infections, dramatically reducing cirrhosis and liver cancer risk. One-time screening for adults born 1945-1965 identifies undiagnosed chronic infections.
Weight Management: Maintaining healthy body weight through structured weight loss plans and adequate hydration reduces NAFLD progression and associated cancer risk. Research from NIH-funded studies shows Mediterranean diet adherence with high vegetable content (100g/day increase) decreases hepatocellular carcinoma risk by 8%.
Alcohol Moderation: Limiting consumption to ≤7 drinks weekly for women or ≤14 for men prevents alcohol-related cirrhosis and liver cancer.
Diabetes Control: Maintaining HbA1c <7% through medication and lifestyle modifications reduces metabolic liver cancer risk.
Coffee Consumption: Regular coffee intake (2-3 cups daily) demonstrates protective effects against liver cancer in multiple studies, reducing risk by 40-50%.
Screening Recommendations for High-Risk Groups
The National Cancer Institute recommends surveillance for specific populations:
Who Should Get Screened:
- Cirrhosis patients (any cause) – ultrasound + AFP every 6 months
- Chronic hepatitis B: Asian males >40, Asian females >50, Africans >20, family history of liver cancer
- Chronic hepatitis C with advanced fibrosis (stage F3-F4)
- NAFLD with cirrhosis or advanced fibrosis
Screening Protocol: Abdominal ultrasound with or without AFP testing performed every 6 months optimizes early detection. MRI provides superior sensitivity for patients with poor ultrasound visualization due to obesity or cirrhosis.
When to Seek Immediate Medical Evaluation
Contact your healthcare provider urgently if you experience:
- Persistent fatigue lasting >4 weeks without explanation
- Unintentional weight loss exceeding 5% of body weight
- New jaundice, severe abdominal pain, or abdominal swelling
- Any new symptoms if you have chronic liver disease
What This Means For You: If you have cirrhosis, chronic hepatitis B or C, or advanced fatty liver disease, scheduling ultrasound screening every 6 months can detect liver cancer when it’s most treatable, with cure rates approaching 90% for small tumors. Combining vaccination, lifestyle modification, and appropriate surveillance offers the strongest defense against this preventable cancer.
Frequently Asked Questions about Liver Cancer
1. What is the first sign of liver cancer most people miss?
Persistent, bone-deep fatigue that doesn’t improve with rest is the most commonly overlooked early sign, often dismissed as stress or aging rather than investigated medically.
2. Can liver cancer be cured if caught early?
Yes. Early-stage liver cancer detected when tumors are small (<3 cm) achieves 70-90% five-year survival rates with surgical resection, transplantation, or ablation.
3. How long can you have liver cancer without knowing?
Many patients have liver cancer for 6-12 months without recognizing symptoms, as early stages produce vague signs like fatigue and mild abdominal discomfort easily attributed to other causes.
4. What are the 3 main causes of liver cancer?
The three leading causes are chronic hepatitis B infection, chronic hepatitis C infection, and cirrhosis from any cause (including alcohol, NAFLD, or viral hepatitis).
5. Is liver cancer painful in early stages?
No. Early-stage liver cancer rarely causes pain. Patients typically experience vague upper right abdominal pressure or discomfort rather than sharp pain, which develops only in advanced stages.
6. Who should get screened for liver cancer?
People with cirrhosis (any cause), chronic hepatitis B or C, advanced fatty liver disease, or family history should get ultrasound screening every 6 months.
7. What blood test detects liver cancer?
Alpha-fetoprotein (AFP) is the primary tumor marker, though 40% of early liver cancers show normal AFP levels, requiring imaging for diagnosis.
8. Can you prevent liver cancer?
Yes. Hepatitis B vaccination (95% effective), hepatitis C treatment, maintaining healthy weight, limiting alcohol, and controlling diabetes significantly reduce liver cancer risk.
9. What is the life expectancy with liver cancer?
Life expectancy varies by stage: early-stage (5+ years with treatment), intermediate-stage (2-3 years), and advanced-stage (1-2 years). Early detection dramatically improves survival.
10. Does liver cancer spread quickly?
Liver cancer progression varies. Early hepatocellular carcinoma may grow slowly over months, while advanced disease with vascular invasion spreads rapidly to lymph nodes, lungs, and bones.
11. What foods help prevent liver cancer?
Mediterranean diet rich in vegetables, fruits, whole grains, coffee (2-3 cups daily), and omega-3 fatty acids reduces liver cancer risk by 40-50% while avoiding processed foods and excess alcohol.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











