On This Page – Quick Medical Summary
If a doctor has told you that you have a pancreatic neuroendocrine tumor, the most useful first fact is this: it is usually not the same disease as the pancreatic cancer behind the frightening headlines and survival statistics. A pancreatic neuroendocrine tumor — often shortened to pNET, and sometimes called an islet cell tumor — begins in different cells and tends to behave very differently from the far more common pancreatic adenocarcinoma.
This guide is built around where you are right now. If you were just diagnosed and want to understand what it means, start with how a pNET differs from ordinary pancreatic cancer. If you are a caregiver, the outlook and treatment sections will matter most. If you have unexplained symptoms such as repeated low blood sugar or stubborn ulcers, the symptoms section explains hormone-producing tumors. And if you are facing high-grade or advanced disease, later sections cover treatment and when this cancer turns more serious.
For the wider context, the overview of pancreatic cancer and its stages covers the whole picture; here, the focus is the neuroendocrine type specifically.
ℹ️ Medical Disclaimer: This article is general education about pancreatic neuroendocrine tumors and does not diagnose disease, recommend treatment, prescribe medication, or substitute for evaluation of your specific case. Decisions about diagnosis, staging, surgery, medication, radiopharmaceutical therapy, and insurance coverage should be made with a board-certified oncologist or neuroendocrine tumor specialist who has examined you and reviewed your records.
How a pancreatic neuroendocrine tumor differs from pancreatic cancer
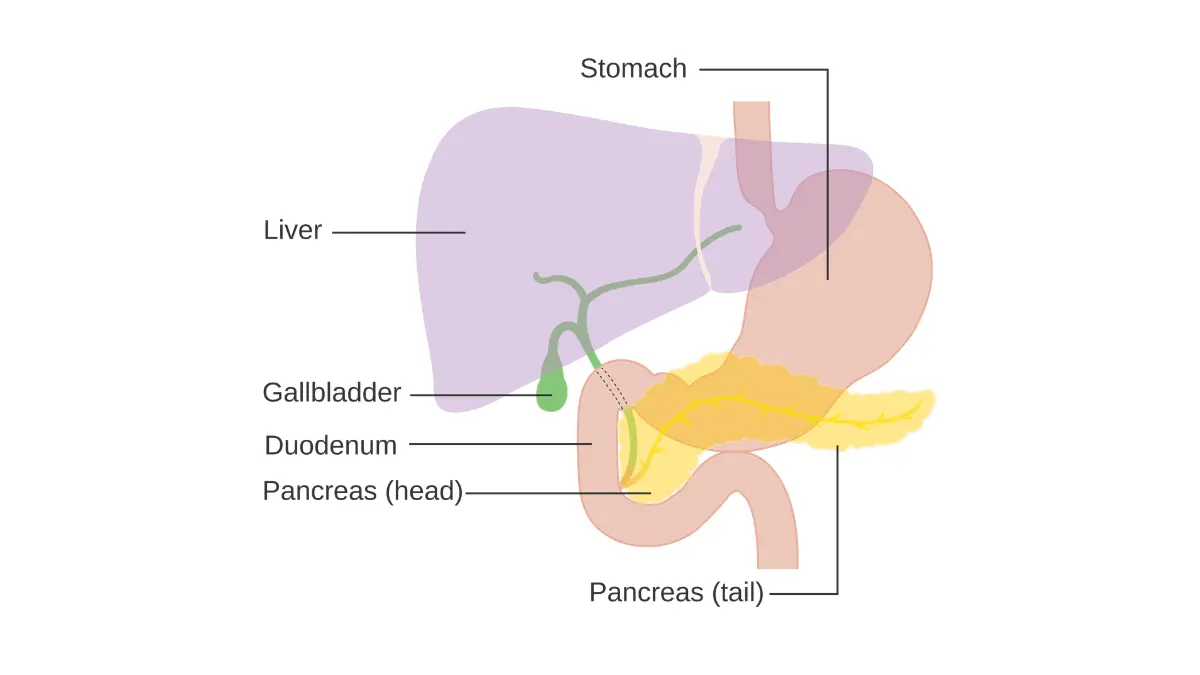
A pancreatic neuroendocrine tumor is not the same as the common form of pancreatic cancer. It starts in the pancreas’s hormone-producing neuroendocrine cells — the islet cells — while the disease most people mean by “pancreatic cancer,” pancreatic adenocarcinoma, starts in the exocrine cells that make digestive enzymes. Because the cell of origin differs, the two usually grow at different speeds and carry very different outlooks.
Most pNETs are well-differentiated, meaning the cells still resemble normal tissue and tend to grow slowly. Many are also found by accident on a scan done for an unrelated reason. That combination — slower-growing biology, often caught earlier — is much of why survival figures for pNETs differ so sharply from those for adenocarcinoma. You can see how the American Cancer Society defines pNETs for more on the subtypes.
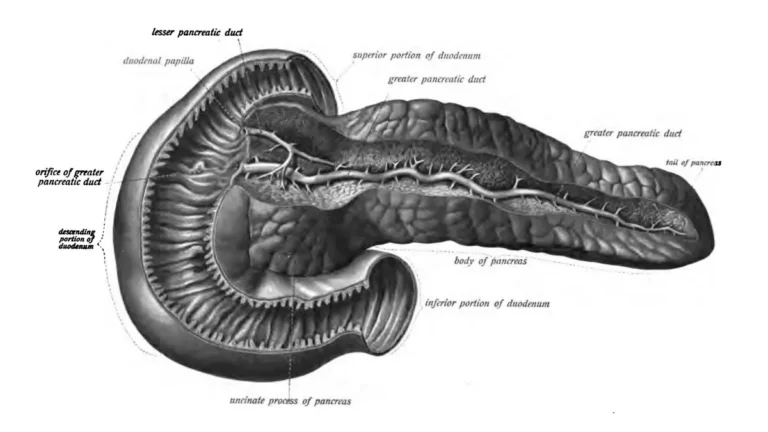
What neuroendocrine cells do in the pancreas
🔬 How It Works: The pancreas has two jobs. Its exocrine cells release enzymes into the gut to digest food, while its endocrine (islet) cells release hormones such as insulin and glucagon into the blood to control blood sugar. A pNET is an overgrowth of those hormone-making islet cells, which is why some pNETs disrupt hormone levels while adenocarcinomas usually do not.
pNET vs adenocarcinoma at a glance
| Feature | Pancreatic neuroendocrine tumor (pNET) | Pancreatic adenocarcinoma | Key clinical detail |
|---|---|---|---|
| Cell of origin | Hormone-making islet (neuroendocrine) cells | Enzyme-making exocrine cells | A different cell means a different disease |
| Typical behavior | Often slow-growing, well-differentiated | Often aggressive | Grade matters more here than for adenocarcinoma |
| Share of pancreatic cancers | Under 2% | The large majority | pNETs are genuinely rare |
| Overall 5-year relative survival | 48% (91% if localized) | About 8% | The gap between the two is large |
| Main treatment intent | Often surgery; sometimes monitoring | Usually multimodal, frequently palliative | Some pNETs are curable |
Survival figures from the American Cancer Society (SEER): pNET rates from the ACS pancreatic NET survival page; the roughly 8% adenocarcinoma figure from the ACS Cancer Statistics 2025 report. See the ACS survival statistics for pancreatic cancer.
Symptoms of a pancreatic neuroendocrine tumor
Many pancreatic neuroendocrine tumors cause no symptoms at all. Most are nonfunctional, meaning they do not release active hormones, so they often grow quietly and are discovered incidentally on imaging done for another reason. When nonfunctional tumors do cause symptoms, it is usually from their size or spread — vague abdominal discomfort, a mass, or jaundice if a tumor presses on the bile duct.
Functional tumors: hormone-driven symptoms
A minority of pNETs are functional, releasing hormones that create recognizable patterns:
- Insulinoma — excess insulin, causing repeated low blood sugar with shakiness, confusion, or fainting.
- Gastrinoma — excess gastrin (Zollinger-Ellison syndrome), causing severe or recurrent stomach ulcers and reflux.
- Glucagonoma, VIPoma, and somatostatinoma — rarer types causing a distinctive rash, profuse watery diarrhea, or blood-sugar and digestive changes.
These syndromes are uncommon, but they are the reason some people reach a pNET diagnosis through symptoms rather than a scan.
When to seek evaluation
✅ Patient Action: If you have unexplained low blood sugar or ulcers that keep returning, ask an endocrinologist or gastroenterologist: “Could a hormone-producing tumor explain this, and should my hormone levels be tested?”
You can compare these against the general early signs of pancreatic cancer, and a symptom checker can help organize what to raise at your visit.
What tumor grade means for a pancreatic neuroendocrine tumor
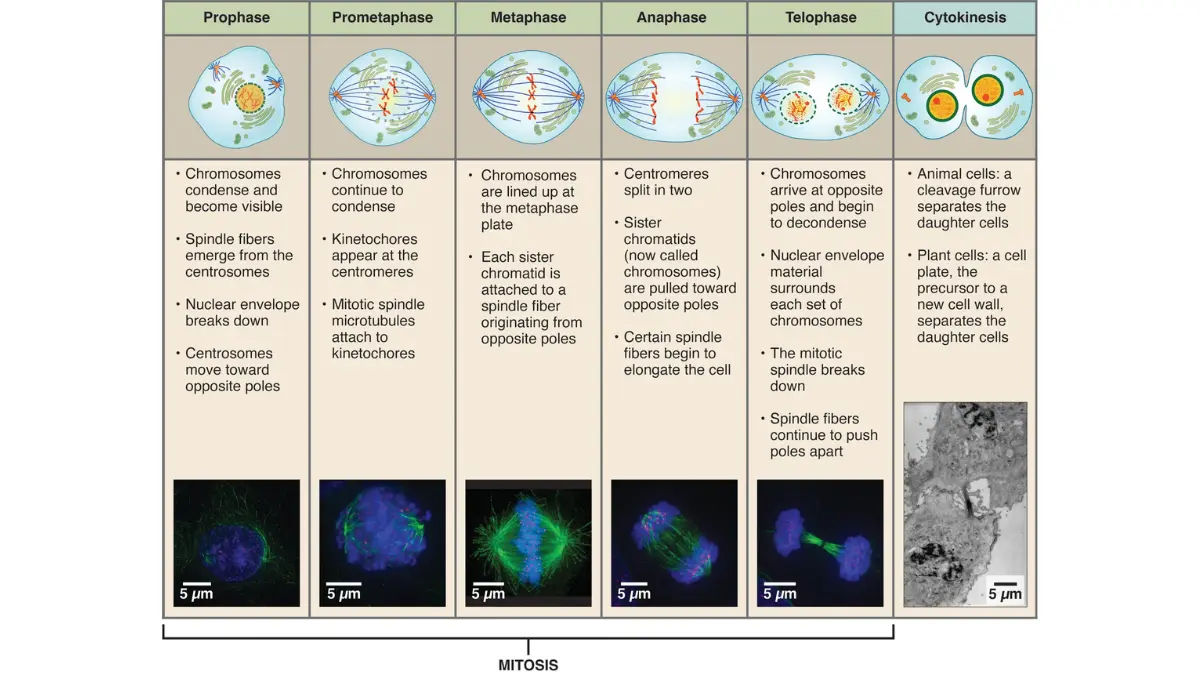
For a pancreatic neuroendocrine tumor, grade often matters as much as stage. Grade describes how quickly the tumor’s cells are dividing, and pathologists measure it two ways: the Ki-67 index (the percentage of cells actively multiplying) and the mitotic rate (how many cells are dividing under the microscope). Under the World Health Organization’s 2022 system, well-differentiated pNETs are graded:
- Grade 1 — Ki-67 under 3% and fewer than 2 dividing cells per 2 mm² (slowest-growing).
- Grade 2 — Ki-67 of 3–20%, or 2–20 dividing cells.
- Grade 3 — Ki-67 above 20%, or more than 20 dividing cells, while the cells still look well-differentiated.
When the two measurements disagree, the higher one sets the grade.
NET versus NEC: why this distinction matters
🩺 Physician Note: The 2022 WHO classification separates well-differentiated grade 3 neuroendocrine tumors from poorly-differentiated neuroendocrine carcinomas (NEC). Both are high-grade, but an NEC is a distinct, more aggressive cancer treated differently — a difference many general articles blur.
✅ Patient Action: Ask your oncologist: “What is my tumor’s grade and Ki-67, and is it a well-differentiated NET or a neuroendocrine carcinoma?” The answer shapes nearly every decision that follows. For the wider workup, see how pancreatic cancer is diagnosed.
Survival rates for pancreatic neuroendocrine tumors
Survival figures for pancreatic neuroendocrine tumors are far more encouraging than the numbers attached to common pancreatic cancer — but they vary widely by how far the tumor has spread. The survival rate below comes from the American Cancer Society, drawn from SEER data on people diagnosed between 2015 and 2021.
📊 Clinical Data Point: 5-year relative survival for pNET — Localized 91% · Regional 64% · Distant 19% · All stages combined 48%. Source: American Cancer Society (SEER), last revised July 2025.
| SEER stage | 5-year relative survival | What it means | Key clinical detail |
|---|---|---|---|
| Localized | 91% | No spread beyond the pancreas | Most favorable; often surgically treatable |
| Regional | 64% | Spread to nearby tissue or lymph nodes | Still far better than adenocarcinoma |
| Distant | 19% | Spread to liver, lungs, or bone | Where outlook varies most by grade |
| All combined | 48% | Average across all stages | Compare with about 8% for adenocarcinoma |
Source: American Cancer Society pancreatic NET survival statistics (SEER, people diagnosed 2015–2021).
What these numbers do and don’t tell you
These are population averages from people diagnosed years ago, grouped only by spread — not by grade. They cannot predict any single person’s outcome, and people diagnosed today may do better as treatments improve. A low-grade tumor and a high-grade NEC at the same stage can follow very different courses, which is why your own grade matters so much here.
✅ Patient Action: Ask your oncologist: “Given my stage, grade, and overall health, how do these population statistics apply to me?” For how staging itself works, see how pancreatic cancer is staged.
How pancreatic neuroendocrine tumors are treated
Treatment for a pancreatic neuroendocrine tumor depends on its grade, stage, and whether it produces hormones — and the options are broader than for most pancreatic cancers. The main approaches are surgery, active surveillance, hormone-control medication, targeted radiation, and targeted drugs.
Surgery and active surveillance
Surgery is the main potentially curative treatment for a localized pNET. For some small, low-grade, symptom-free tumors, doctors may instead recommend active surveillance — careful monitoring rather than immediate treatment. Removing a localized tumor offers the best chance of long-term control.
Systemic options: hormone control, PRRT, and targeted therapy
For tumors that have spread or cannot be removed, several systemic options exist. Somatostatin analogs (octreotide and lanreotide) can slow growth and control hormone symptoms. The targeted drugs everolimus and sunitinib are FDA-approved for advanced pNETs. And peptide receptor radionuclide therapy (PRRT) uses a radioactive drug, lutetium Lu 177 dotatate (Lutathera), to deliver radiation directly to tumor cells.
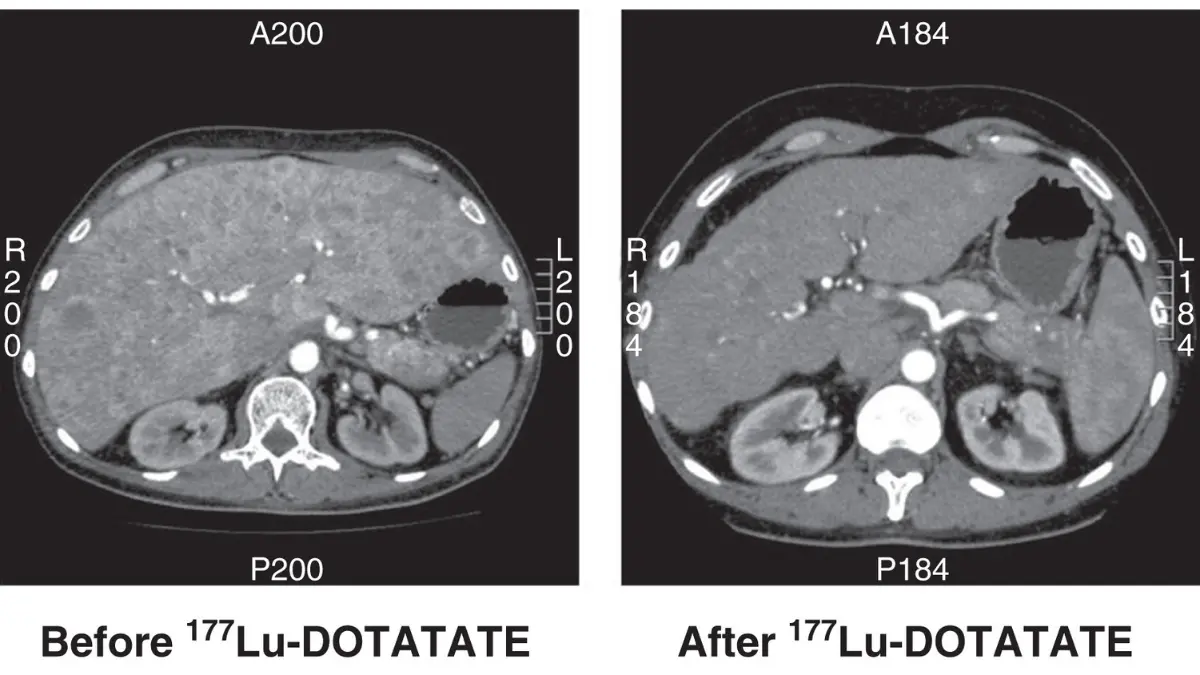
🔬 How It Works: PRRT pairs a radioactive particle with a molecule that seeks out somatostatin receptors on neuroendocrine tumor cells. The drug binds to those receptors, enters the cell, and releases radiation that damages it from the inside — sparing most healthy tissue.
The FDA approval for this radiopharmaceutical covers these tumors, and in 2024 the NCI summarized the trial results supporting its use earlier in treatment. A related radioligand therapy is used in prostate cancer, which uses the same targeting principle.
✅ Patient Action: Ask a neuroendocrine tumor specialist: “Is my tumor a surgical candidate, and am I somatostatin-receptor-positive — a candidate for PRRT?” High-grade tumors may instead need chemotherapy, and pancreatic cancer treatment options differ for the exocrine form.
When a pancreatic neuroendocrine tumor is more serious
Not every pancreatic neuroendocrine tumor follows the hopeful path. The encouraging survival figures above do not apply evenly, and some forms of this disease are aggressive and need urgent, specialized care.
Neuroendocrine carcinoma and high-grade disease
A poorly-differentiated neuroendocrine carcinoma is high-grade by definition and behaves far more aggressively than a typical well-differentiated pNET. Distant-stage disease also carries a markedly lower outlook — the 19% figure above reflects how much spread changes the picture.
⚠️ Clinical Warning: A neuroendocrine carcinoma (NEC) is not a slow-growing tumor and should not be managed as one. It often requires prompt evaluation at a center experienced with neuroendocrine cancers, where chemotherapy and other systemic treatments can begin without delay.
Hereditary risk and finding the right team
Some pNETs are linked to inherited syndromes such as MEN1 and von Hippel-Lindau disease, which can affect screening for relatives. A family-history risk check and a conversation about whether pancreatic cancer can be hereditary may be worthwhile.
✅ Patient Action: Ask for referral to a neuroendocrine tumor center of excellence, and confirm in writing whether your tumor is a well-differentiated NET or an NEC.
Pancreatic neuroendocrine tumor: frequently asked questions
1. Is a pancreatic neuroendocrine tumor cancer?
A pancreatic neuroendocrine tumor can be cancerous, but most are well-differentiated and slower-growing than the common form of pancreatic cancer. Behavior ranges from very indolent low-grade tumors to aggressive high-grade ones, so the term covers a wide spectrum. Your tumor’s grade and stage define where it falls.
2. Is a pancreatic neuroendocrine tumor the same as pancreatic cancer?
No. A pancreatic neuroendocrine tumor starts in the pancreas’s hormone-making islet cells, while the disease most people call pancreatic cancer — adenocarcinoma — starts in enzyme-making exocrine cells. They differ in behavior and outlook: pNETs have an overall 48% five-year relative survival, versus about 8% for adenocarcinoma.
3. What is the survival rate for a pancreatic neuroendocrine tumor?
By American Cancer Society SEER data, the five-year relative survival for a pancreatic neuroendocrine tumor is 91% when localized, 64% when regional, 19% when distant, and 48% across all stages combined. These are population averages and cannot predict an individual outcome. Ask your oncologist how they apply to your case.
4. What is the difference between functional and nonfunctional pancreatic neuroendocrine tumors?
A functional pancreatic neuroendocrine tumor releases active hormones that cause symptoms, such as low blood sugar from an insulinoma or ulcers from a gastrinoma. A nonfunctional tumor does not release active hormones and often causes no symptoms until it grows or spreads. Most pNETs are nonfunctional.
5. What does Ki-67 or grade mean for a pancreatic neuroendocrine tumor?
Grade measures how fast a pancreatic neuroendocrine tumor’s cells divide, using the Ki-67 index and mitotic rate. Under the 2022 WHO system, well-differentiated tumors are Grade 1 (Ki-67 under 3%), Grade 2 (3–20%), or Grade 3 (above 20%). Grade strongly shapes treatment, so ask your team for yours.
6. What is the difference between a pancreatic neuroendocrine tumor and a neuroendocrine carcinoma?
A well-differentiated neuroendocrine tumor still resembles normal tissue and is often slower-growing. A poorly-differentiated neuroendocrine carcinoma (NEC) is high-grade by definition and behaves more aggressively, requiring different, often more urgent treatment. The 2022 WHO classification treats them as distinct entities. Confirm which one you have with your oncologist.
7. How is a pancreatic neuroendocrine tumor treated?
Treatment for a pancreatic neuroendocrine tumor depends on grade and stage. Options include surgery (often curative for localized tumors), active surveillance for small low-grade tumors, somatostatin analogs, the FDA-approved targeted drugs everolimus and sunitinib, PRRT, and chemotherapy for high-grade disease. Discuss the right sequence with a neuroendocrine tumor specialist.
8. What is PRRT or Lutathera?
PRRT (peptide receptor radionuclide therapy) treats a pancreatic neuroendocrine tumor with lutetium Lu 177 dotatate, sold as Lutathera. It pairs radiation with a molecule that targets somatostatin receptors on tumor cells, delivering radiation from inside the cell. The FDA approved it for these tumors. Ask whether you are somatostatin-receptor-positive and eligible.
9. Are pancreatic neuroendocrine tumors hereditary?
Most pancreatic neuroendocrine tumors are not inherited, but some are linked to genetic syndromes such as MEN1 and von Hippel-Lindau disease. These can also affect cancer screening for blood relatives. If you have a family history of these syndromes, ask your team whether genetic counseling is appropriate for you and your family.
10. What symptoms does a pancreatic neuroendocrine tumor cause?
Many pancreatic neuroendocrine tumors cause no symptoms and are found incidentally. Functional tumors can cause hormone-driven symptoms such as repeated low blood sugar, recurrent ulcers, watery diarrhea, or a distinctive rash. Larger tumors may cause abdominal discomfort or jaundice. Unexplained, persistent versions of these warrant medical evaluation.
11. Can a pancreatic neuroendocrine tumor be cured?
A localized, low-grade pancreatic neuroendocrine tumor can often be removed surgically with a strong chance of long-term control, which is why localized disease carries a 91% five-year relative survival. High-grade or widely spread tumors are harder to cure but can still be treated to control growth. Outcomes depend heavily on grade and stage.
Where this leaves you
A pancreatic neuroendocrine tumor is its own disease, with a path that usually looks very different from the pancreatic cancer most people fear. Two facts shape almost everything ahead: your tumor’s stage and its grade. Knowing both turns a frightening, vague diagnosis into a set of specific questions you can bring to the right specialist.
The single most useful next step is a conversation with a neuroendocrine tumor team that can confirm whether your tumor is a well-differentiated NET or a neuroendocrine carcinoma, and whether surgery, monitoring, or systemic treatment fits your situation. You now know what those terms mean and what to ask.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.