On This Page – Quick Medical Summary
If someone in your family was recently diagnosed with pancreatic cancer, or a genetic test flagged a mutation, or a doctor mentioned “family history,” you are likely asking one question: can I catch this early? This guide is built for three readers. If a close relative was just diagnosed and you are frightened for yourself, start with who actually counts as high-risk. If you already carry a known mutation such as BRCA2, the sections on when to begin and what the tests involve are for you. And if you have no family history but a general worry, the most useful thing you will read is why routine screening is not recommended for most people — and why that is reassuring rather than neglectful.
There is no screening test offered to the general public for this cancer. But people at genuinely high risk are a recognized exception, with real surveillance options. Knowing which group you fall into is the first step, and everything below is organized to help you find it.
ℹ️ Medical Disclaimer: This article is general health education, not a medical diagnosis, screening recommendation, or treatment plan. Decisions about pancreatic cancer screening — whether you qualify, which test fits your situation, when to begin, and when to stop — must be made with a board-certified gastroenterologist or a genetics professional, ideally a certified genetic counselor. Risk figures vary between individuals and studies, and genetic results require expert interpretation. Do not start, delay, or stop any screening or testing based on this article alone.
Why pancreatic cancer screening isn’t recommended for everyone
For most adults, no leading medical group recommends routine pancreatic cancer screening. The U.S. Preventive Services Task Force gives screening of average-risk, symptom-free adults a “D” grade — its judgment is that the likely harms outweigh the benefits. That conclusion explicitly does not apply to people at high risk.
What the recommendation actually means
The reason is statistical, not neglect. Most cases — roughly 85% to 90% — occur in people with no family history or inherited syndrome, and because the early symptoms of pancreatic cancer tend to appear late, watching for symptoms rarely catches it early.
📊 Clinical Data Point: About 1.7% of Americans are diagnosed with pancreatic cancer in their lifetime — an incidence near 13.9 cases per 100,000 people a year. Source: NCI national pancreatic cancer statistics (2019–2023 incidence; lifetime risk from 2021–2023 data).
Why screening healthy people can do harm
🔬 How It Works: When a disease is this uncommon, even an accurate test flags far more healthy people than real cancers. Those false alarms lead to repeat scans, biopsies, and sometimes surgery on a pancreas that would never have become cancerous — and pancreatic surgery carries genuine risk.
There is also no blood test accurate enough to screen everyone, which we cover below. For people with a strong family history or a known mutation, the odds shift enough to change the math — and that is who the rest of this guide is for.
Who counts as high-risk for pancreatic cancer?
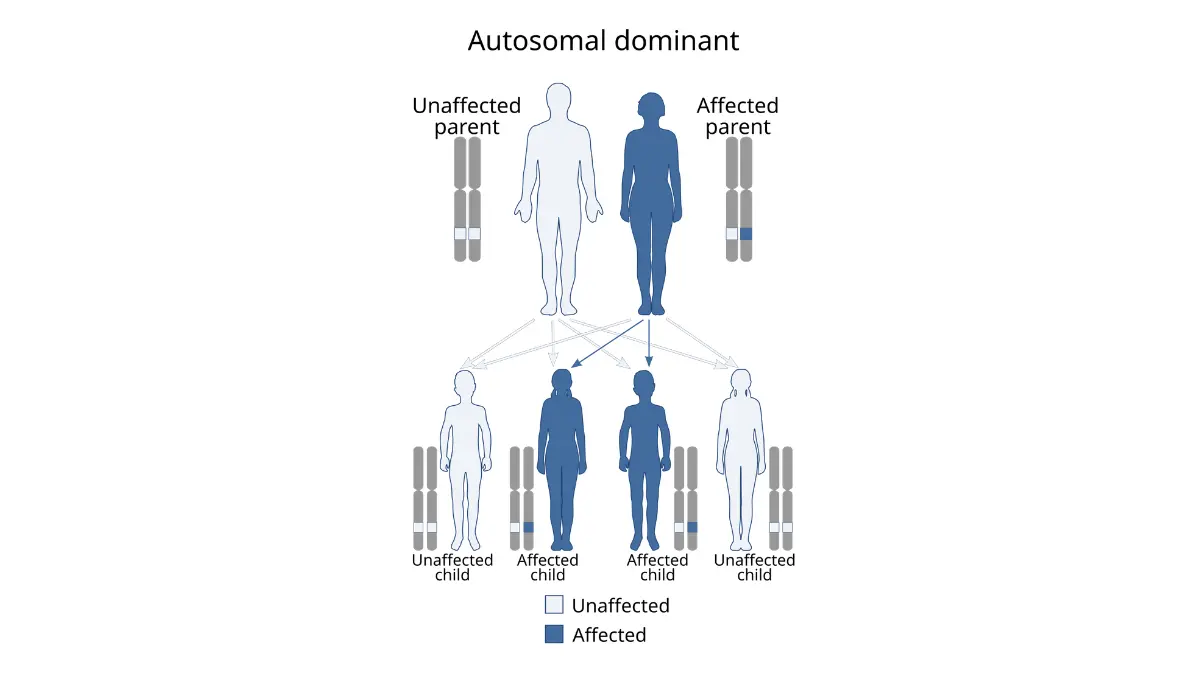
“High-risk” is not a vague label — it names specific, recognized situations. You may be high-risk for pancreatic cancer if you have two or more close blood relatives with it, a first-degree relative diagnosed before about age 50, or a known inherited gene change linked to the disease.
Family history that raises your risk
Doctors use the term familial pancreatic cancer for families with at least two affected first-degree relatives — a parent, sibling, or child — and risk climbs with the number affected and how young they were. One distant relative usually does not place you in the high-risk group. Our guide to whether pancreatic cancer is hereditary explains where that line falls.
Inherited genetic syndromes and gene changes
A few inherited conditions raise risk steeply. The highest are Peutz-Jeghers syndrome (the STK11 gene) and hereditary pancreatitis (the PRSS1 gene), where published cohorts put lifetime risk near 40% or higher; CDKN2A-linked familial melanoma is often cited around 17% to 25%. Changes in BRCA2, BRCA1, PALB2, ATM, and the Lynch syndrome genes raise risk more modestly. These figures vary widely between studies, so treat them as ranges.
🔬 How It Works: Many of these genes normally repair damaged DNA or restrain cell growth. An inherited change that disables one lets pancreatic cells accumulate mutations more easily over a lifetime — which is why some syndromes justify surveillance even with no family history at all.
Do I need genetic testing first?
For most people weighing screening, the starting point is genetic counseling, not a scan. A certified counselor can review your family tree, decide whether genetic testing for pancreatic cancer is warranted, and interpret the result — including the “uncertain” findings that are easy to misread alone. Mapping your history first with our genetic risk assessment tool gives you something concrete to bring.
✅ Patient Action: Before any imaging, ask to see a certified genetic counselor and ask directly: “Given my family history or gene result, do I meet criteria for a pancreatic surveillance program, and should I have germline genetic testing?”
When should high-risk adults start screening, and how often?
For people who qualify, expert guidelines tie the starting age to the specific gene or family pattern — not to a single universal age. Most programs begin between ages 30 and 50, and one rule often moves it earlier: start about 10 years before the youngest relative was diagnosed.
Start ages by syndrome and family history
| Genetic or family-history group | Typical age to begin | Key clinical detail |
|---|---|---|
| Peutz-Jeghers syndrome (STK11) | ~30–35 (some guidance, 40) | Surveillance advised even with no family history |
| CDKN2A (familial melanoma) | ~40 | Advised regardless of family history |
| Hereditary pancreatitis (PRSS1) | ~40, or 20 years after the first pancreatitis attack | Whichever comes first |
| BRCA2, PALB2, or ATM change | ~50, or 10 years before the youngest case | Generally requires a relative with pancreatic cancer |
| BRCA1, Lynch genes, or TP53 | ~50, or 10 years before the youngest case | Paired with a family history of the disease |
| Familial kindred (no identified gene) | ~50 (experts differ on 50 vs 55) | Based on two or more affected first-degree relatives |
Source: compiled from the International Cancer of the Pancreas Screening (CAPS) Consortium (2020) and NCCN guidance. These are general guideline figures, not a personal plan — your program sets your exact schedule.
How often screening repeats
When the first scan is reassuring, surveillance is usually repeated once a year. Programs adjust this for individual findings — some CDKN2A carriers, for example, are watched more closely because cancers can appear between annual exams. These international expert surveillance recommendations describe the approach in detail.
🩺 Physician Note: Current guidelines stress that surveillance should happen at a high-volume pancreatic center, ideally within a research program — not as a one-off scan ordered in isolation. Centralizing care is how subtle, early changes get caught and interpreted correctly.
When screening may stop
There is no firm stopping age. The decision weighs your other health conditions, life expectancy, and personal preference, and it belongs to you and your care team rather than a fixed cutoff.
✅ Patient Action: Ask a gastroenterologist at a high-volume pancreatic center: “Based on my gene or family history, what start age and interval apply to me, and can I enroll in a formal surveillance program?”
What pancreatic cancer screening actually involves
Pancreatic surveillance relies on two imaging tests, used alone or alternated: endoscopic ultrasound (EUS) and MRI with MRCP. Routine surveillance does not use CT scans, which add radiation and detect these small early changes less reliably.
How EUS and MRI work
🔬 How It Works: In an EUS, a thin scope with an ultrasound probe on its tip is passed into the stomach under sedation, placing the camera millimeters from the pancreas for a close look. MRI with MRCP is a non-invasive scan, with no radiation, that maps the pancreas and its ducts in detail. Studies find the two perform comparably for spotting the earliest worrisome changes.
What the tests are looking for
The goal is not to find advanced cancer — it is to catch a precursor lesion or a stage I tumor while it is still curable, including high-grade changes in the pancreatic ducts known as PanIN or IPMN. This differs from the work-up done once someone already has symptoms, which our guide on how pancreatic cancer is diagnosed explains.
A reassuring note: small pancreatic cysts are common in high-risk people — found in roughly half at the first scan — and most are harmless. Finding one is rarely cause for alarm.
Where surveillance happens
Guidelines favor specialized centers, and many of the best programs run as research studies you can join. You can search for an active pancreatic surveillance study near you.
Can a blood test screen for pancreatic cancer?
The honest answer most people don’t expect: no single blood test is approved to screen for pancreatic cancer, and the marker patients most often request — CA 19-9 — was never built for it.
Why CA 19-9 isn’t a screening test
🔬 How It Works: CA 19-9 is a sugar-protein that some pancreatic tumors shed into the blood. But pancreatitis, gallstones, and a blocked bile duct also raise it, and roughly 10% to 15% of people don’t produce it at all — so a “normal” result can be falsely reassuring. It is used to monitor a known cancer, not to find one.
Our deeper guide covers what a CA 19-9 test can and can’t tell you.
⚠️ Clinical Warning: A normal CA 19-9 does not rule pancreatic cancer out, and a high one does not confirm it. It should never be used on its own to decide whether you are in the clear.
New-onset diabetes as a warning signal
Diabetes that appears suddenly after age 50 is one signal researchers watch, since it can occasionally be the first clue to a hidden tumor — though the great majority of new diabetes is not cancer. Our article on new-onset diabetes and pancreatic cancer explains the link without overstating it.
Blood tests in development
This is an active research front. Recent NIH-funded early-detection blood-marker research reported a multi-marker panel identifying most cancers in stored blood samples — promising, but not yet approved to screen the general public.
What screening can’t do, and why genetic counseling comes first
Surveillance is worth taking seriously, but honesty matters more than false hope. Catching changes earlier is the goal — yet a clear survival benefit has not been definitively proven, which is exactly why guidelines urge that it happen within research programs.
The limits of surveillance today
The harms are real too: false alarms, anxiety, and occasionally surgery for a lesion that turns out benign. Weighing this is personal, and it is part of why enrolling in a study — see current pancreatic cancer clinical trials and research programs — both protects you and helps answer the open questions.
Your first step
None of this requires you to decide alone. The single most useful move is genetic counseling, which tells you whether you qualify at all and connects you to a program if you do.
✅ Patient Action: Book a certified genetic counselor first; if you qualify, ask for a referral to a high-volume pancreatic surveillance program. Bring your full family cancer history to the appointment.
Frequently asked questions about pancreatic cancer screening
1. Is there a screening test for pancreatic cancer?
There is no pancreatic cancer screening test offered to the general public, because the disease is uncommon and current tests cause too many false alarms. People at high risk are the exception and may be offered imaging surveillance. Discuss your own situation with a gastroenterologist or genetic counselor.
2. Who should be screened for pancreatic cancer?
Screening is considered for high-risk people: those with two or more close relatives who had pancreatic cancer, a first-degree relative diagnosed before about 50, or certain inherited gene changes. Most people do not qualify. A genetic counselor can confirm whether you do.
3. At what age should high-risk people start pancreatic cancer screening?
It depends on the specific gene or family pattern. Peutz-Jeghers carriers may start around 30–35, CDKN2A and hereditary pancreatitis around 40, and most others around 50 — or 10 years before the youngest relative’s diagnosis. Your surveillance program sets your exact start age.
4. How often should you be screened for pancreatic cancer?
When the first scan is reassuring, pancreatic cancer surveillance is usually repeated once a year. Some carriers are watched more closely when findings warrant it. Programs individualize the interval, so confirm your schedule with the gastroenterologist managing your surveillance.
5. Does a CA 19-9 blood test screen for pancreatic cancer?
No. CA 19-9 is a tumor marker used to monitor known pancreatic cancer, not to screen for it. It rises in benign conditions, and 10–15% of people don’t produce it, so results mislead easily. Never rely on it alone; ask your doctor what your result means.
6. Is EUS or MRI better for pancreatic cancer screening?
Studies show endoscopic ultrasound and MRI/MRCP perform comparably for detecting the earliest concerning changes in pancreatic cancer surveillance. EUS uses sedation; MRI is non-invasive with no radiation. Many programs alternate them, and your center will recommend the right approach for you.
7. Can pancreatic cancer be detected early?
In high-risk people under surveillance, the aim is to catch a precursor lesion or a stage I tumor while it is still treatable. For most others, pancreatic cancer is hard to find early because symptoms appear late — which is why risk-based screening exists at all.
8. If pancreatic cancer runs in my family, will I get it?
No — a family history raises your risk but does not mean you will develop pancreatic cancer. Most people with an affected relative never get it. Your degree of risk depends on how many relatives were affected and which gene, if any, is involved. A genetic counselor can clarify yours.
9. Should I get genetic testing for pancreatic cancer risk?
Possibly. Genetic testing is worthwhile when your family history suggests an inherited syndrome, but it should be guided by a certified genetic counselor who can interpret the result. Uncertain findings are common and easy to misread, so start with counseling before testing for pancreatic cancer risk.
10. Does new-onset diabetes mean I have pancreatic cancer?
Almost always no. New diabetes after 50 is very common and rarely caused by pancreatic cancer, though researchers study it because it can occasionally be an early clue. If you have new diabetes alongside weight loss or other symptoms, mention it to your doctor.
11. Is pancreatic cancer screening covered by insurance?
Coverage varies by plan and by whether you meet high-risk criteria, since surveillance is not a routine screening benefit. Many research programs reduce or cover costs. Confirm specifics with your insurer and the program before scheduling, and ask about financial-assistance options.
The bottom line on screening when you’re high-risk
Three things are worth holding onto. Most people do not need pancreatic cancer screening, and that is genuinely reassuring rather than a gap in care. If you are high-risk — a strong family history or an inherited gene change — surveillance with EUS or MRI may be appropriate, on a schedule matched to your specific risk. And the first step is never a scan you arrange yourself; it is genetic counseling, which tells you whether you qualify and connects you to the right program.
You have more control here than the fear suggests. Start by booking that conversation, and bring your family history with you. For the wider picture, our full pancreatic cancer guide covers symptoms, diagnosis, and treatment.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.