On This Page – Quick Medical Summary
When a close relative is diagnosed with pancreatic cancer, the first quiet fear is often about yourself or your children. Here is the honest starting point: most pancreatic cancer is not inherited. Roughly 1 in 10 cases is hereditary or familial, which means about 90% are not passed down through families.
This guide is built for three readers. If you are worried because a parent or sibling had pancreatic cancer, the family-history and risk sections are for you. If you already know you carry an inherited mutation like BRCA2, the sections on specific genes, testing, and screening will matter most. And if you or someone you love was recently diagnosed and a doctor mentioned genetic testing, the testing section explains why that is now standard.
A clear overview of pancreatic cancer from first signs to treatment gives the wider picture; this page focuses on the genetics.
ℹ️ Medical Disclaimer: This article is educational and does not diagnose disease, interpret your personal genetic results, or recommend specific testing, screening, or treatment for you. Inherited cancer risk, genetic testing decisions, and screening plans are individual medical matters — review them with a board-certified genetic counselor, oncologist, or your physician before acting.
What “hereditary pancreatic cancer” really means
Most pancreatic cancer happens by chance, not heredity. Hereditary pancreatic cancer refers to cases driven by a gene change you were born with and could pass to your children, and it makes up only part of the roughly 10% of cases with a family link.
Hereditary vs familial vs sporadic
The word genetic causes confusion. Nearly all cancer is genetic in the sense that it starts with DNA changes inside cells, but those changes are usually acquired during life, not inherited. Sporadic cancer — the large majority — has no inherited cause and does not run in families.
What counts as familial pancreatic cancer
Researchers split inherited risk into two groups. About 3% of all pancreatic cancers occur in people with a known inherited syndrome such as a BRCA2 mutation, while another roughly 7% are called familial pancreatic cancer — two or more first-degree relatives with the disease and no single identifiable gene to explain it.
📊 Clinical Data Point: About 10% of pancreatic cancers are hereditary or familial. — Source: Pancreatic Cancer Action Network.
How inherited risk is passed down
Most inherited pancreatic cancer genes follow an autosomal dominant pattern.
🔬 How It Works: Autosomal dominant means a parent who carries the gene change has about a 50% chance of passing it to each child. The inherited copy doesn’t cause cancer by itself — it removes one of the body’s safeguards, so a single later change in a cell is more likely to start a tumor.
Other causes and risk factors for pancreatic cancer, like smoking and chronic pancreatitis, act alongside or independently of inherited risk. The National Cancer Institute’s patient guide to pancreatic cancer lists inherited gene disorders among the established risk factors.
Which inherited genes raise pancreatic cancer risk?
Several inherited gene changes are linked to higher pancreatic cancer risk, and BRCA2 is the most studied. A BRCA2 mutation raises risk roughly 3 to 10 times above average; BRCA1 carries a smaller increase.
📊 Clinical Data Point: BRCA2 mutations are associated with a 3- to 10-fold increased risk of pancreatic cancer. — Source: Pancreatic Cancer Action Network.
BRCA2 and BRCA1
These are the same genes best known for hereditary breast and ovarian cancer. Most carriers never develop pancreatic cancer, but the lifetime risk is higher than average — estimates for BRCA2 generally fall around 5% to 10% depending on the study, with BRCA1 lower at roughly 2% to 3%.
PALB2 and ATM
PALB2 works closely with BRCA2 and appears in a small share of familial cases; ATM is another DNA-repair gene tied to moderately raised risk. The exact lifetime risk for each is still being defined.
CDKN2A (FAMMM) and STK11 (Peutz-Jeghers)
Some syndromes carry much higher risk. People with a CDKN2A mutation — familial atypical multiple mole melanoma, or FAMMM — and those with Peutz-Jeghers syndrome are among the highest-risk groups identified.
🔬 How It Works: BRCA2, PALB2, and ATM all help repair broken DNA. When that repair system is weakened, the tumors that form are often unusually sensitive to platinum chemotherapy and to a medication class called PARP inhibitors — which is why an inherited result can shape treatment.
| Gene / Syndrome | Associated Pancreatic Cancer Risk | Key Clinical Detail |
|---|---|---|
| BRCA2 | ~3–10× average; lifetime ~5–10% | Most common inherited link; can affect treatment options |
| BRCA1 | Modest increase; lifetime ~2–3% | Weaker link than BRCA2 |
| PALB2 | Found in ~3–4% of familial cases | Works with BRCA2; lifetime risk not yet well-defined |
| ATM | Present in ~1–5% of patients | Moderate-risk DNA-repair gene |
| CDKN2A / p16 (FAMMM) | Lifetime ~15–35% | Same gene also raises melanoma risk |
| STK11 (Peutz-Jeghers) | Lifetime ~11–36% | Among the highest relative risks; also causes GI polyps |
| PRSS1 (hereditary pancreatitis) | ~30–40% by age 70 (some estimates lower) | Risk rises sharply with smoking |
| MMR genes (Lynch syndrome) | Modest; ~3–4% or lower by age 70 | Magnitude debated; mainly a colorectal/uterine syndrome |
Figures verified against the Pancreatic Cancer Action Network, Johns Hopkins (National Familial Pancreatic Tumor Registry), and peer-reviewed literature indexed by the NIH. Estimates vary between studies.
The CDKN2A gene that raises pancreatic risk is the same one behind hereditary melanoma risk, so some families see both. Because an inherited mutation can affect therapy, germline results may influence pancreatic cancer treatment options.
✅ Patient Action: If pancreatic cancer or a known mutation runs in your family, ask a genetic counselor: “Based on my family’s pattern, which inherited cancer-gene panel is appropriate for me?”
How much does a family history raise your risk?
Family history is the single biggest clue to inherited risk, and the more close relatives affected, the higher the risk climbs. To read these numbers fairly, start with the baseline: an average person’s lifetime risk of pancreatic cancer is only about 1 in 64.
Risk by number of affected relatives
A landmark registry study quantified how risk rises with the number of affected first-degree relatives — parents, siblings, and children.
📊 Clinical Data Point: Pancreatic cancer risk is about 4.5 times higher with one affected first-degree relative, 6.4 times higher with two, and 32 times higher with three or more. — Source: Klein and colleagues, as cited by the International Cancer of the Pancreas Screening (CAPS) Consortium.
Why age of diagnosis matters
The relatives’ age matters too. When a family member developed pancreatic cancer before age 50, the risk to others rises further, and an early age of onset is one reason genetic counselors take these cases seriously.
Putting the numbers in perspective
A 32-fold increase sounds alarming, but it multiplies a small baseline. Even at the highest end, many people in these families never develop pancreatic cancer — the figure identifies who deserves closer attention, not who is destined for the disease.
Should you get genetic counseling and testing?
For anyone diagnosed with pancreatic cancer, the answer is now clear. The National Comprehensive Cancer Network recommends that every patient with pancreatic cancer be offered germline genetic testing, regardless of family history.
Why every pancreatic cancer patient is now advised to test
This changed because family history turned out to be a poor filter. Many people who carry an inherited mutation have no striking family history at all, so testing only the “obvious” families missed carriers whose results could guide treatment.
🩺 Physician Note: Current guidelines emphasize that a germline result can do two things at once — open up treatment options such as platinum chemotherapy or PARP inhibitors, and flag relatives who may benefit from their own testing.
Who else should consider counseling
If you have not had cancer but have a strong family pattern, counseling is worth discussing. It is often suggested for people with several first-degree relatives affected, a known mutation in the family, or a cluster of related cancers such as breast, ovarian, and pancreatic. Understanding what a positive BRCA result means can help you prepare, and a genetic risk assessment tool can help you organize your family history beforehand — though it is an orientation aid, not a medical test.
What genetic counseling involves
Counseling comes before testing for a reason. A trained counselor reviews your personal and family history, explains what a test can and cannot tell you, and helps you decide whether testing is right for you — a process described by both the American Cancer Society’s guide to genetic testing and a plain-language overview of genetic counseling.
✅ Patient Action: If you have pancreatic cancer, ask your oncologist: “Should I have germline genetic testing, and should my tumor be tested too?”
What high-risk people can do: screening and risk reduction
There is no proven way to prevent hereditary pancreatic cancer, but genuinely high-risk people can be watched closely. Major expert groups suggest surveillance for individuals whose estimated lifetime risk is roughly 5% or higher.
Who qualifies for surveillance
The CAPS Consortium identifies candidates by gene and family history — for example, people with Peutz-Jeghers syndrome, certain CDKN2A or BRCA2 carriers who also have an affected relative, and members of families with two or more affected first-degree relatives. Starting ages differ by gene, often earlier for higher-risk syndromes and around age 50 for others, but the right plan is individual.
How screening is done, and its limits
Surveillance uses imaging, not blood tests.
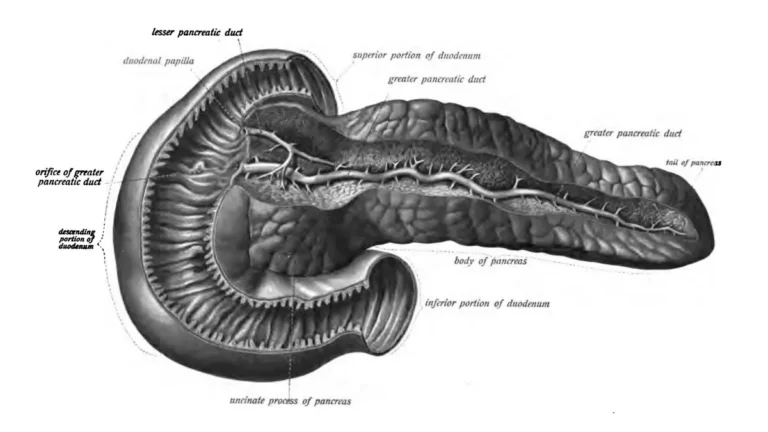
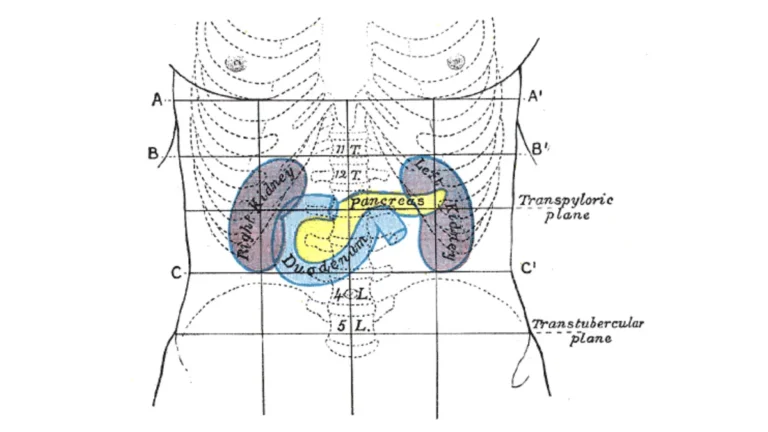
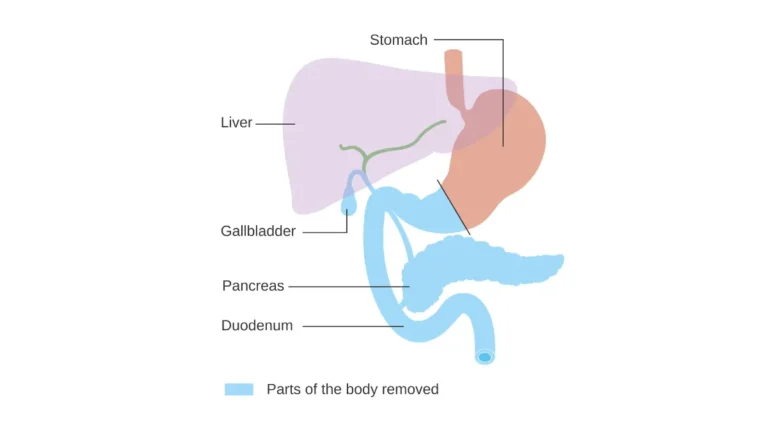
Adapted from AnatomyTOOL Leiden – Drawing Stomach, duodenum, pancreas – no labels, license under “Leiden – Drawing Stomach, duodenum, pancreas – no labels” by Ron Slagter, license: CC BY-NC-SA
🔬 How It Works: The two main tools are endoscopic ultrasound, which views the pancreas from inside the digestive tract, and MRI with MRCP, which images it without radiation. CT and ERCP are generally avoided for routine screening. If something suspicious turns up, how pancreatic cancer is diagnosed explains the next steps.
⚠️ Clinical Warning: Surveillance is not a guarantee and is meant only for genuinely high-risk people, ideally within a specialized program. Small pancreatic cysts are found in up to half of high-risk individuals, most are harmless, and a clear survival benefit from screening has not been firmly established.
Reducing risk where you can
Some risk is modifiable. Not smoking is the most consistent lever, and it matters especially in hereditary pancreatitis, where smoking can move the onset of cancer years earlier. High-risk individuals may also be eligible for pancreatic cancer screening studies and clinical trials.
✅ Patient Action: Ask a gastroenterologist or a high-risk pancreatic clinic: “Do I meet the lifetime-risk threshold for surveillance, and at what age should it start for my gene and family history?”
Having a mutation doesn’t mean you’ll get pancreatic cancer
If you carry an inherited mutation, the most important fact to hold onto is that risk is not destiny. Higher risk means closer attention is wise, not that the disease is coming.
Most carriers never develop pancreatic cancer
For most inherited mutations, the majority of carriers live their whole lives without pancreatic cancer. A positive result tells you your risk is above average and that screening or treatment decisions may differ — it does not predict your future.
When to talk to your doctor
Knowing the warning signs is still useful. If you are high-risk, learning the early symptoms of pancreatic cancer — such as persistent upper-abdominal or back pain, jaundice, or unexplained weight loss — helps you raise concerns early rather than wait.
✅ Patient Action: Bring a written family history to your next visit and ask your physician whether your personal and family pattern warrants referral to a genetic counselor.
Frequently asked questions about hereditary pancreatic cancer
1. Is pancreatic cancer hereditary or genetic?
All cancer is genetic because it begins with DNA changes, but only about 10% of pancreatic cancer is hereditary — caused by a gene change you inherited and could pass on. The other roughly 90% comes from changes acquired during life and does not run in families.
2. What percentage of pancreatic cancer is inherited?
About 10% of pancreatic cancers are hereditary or familial. Of those, roughly 3% occur in people with a known inherited syndrome such as a BRCA2 mutation, and about 7% are familial pancreatic cancer — two or more close relatives affected without a single identified gene.
3. Does the BRCA gene increase pancreatic cancer risk?
Yes. A BRCA2 mutation raises pancreatic cancer risk about 3 to 10 times above average, with an estimated lifetime risk around 5% to 10%; BRCA1 carries a smaller increase. Most carriers never develop it. A genetic counselor can explain what a result means for you.
4. If my parent had pancreatic cancer, will I get it?
Probably not. Having one first-degree relative with pancreatic cancer raises your risk roughly 4.5 times above an average baseline of about 1 in 64, but most people in these families never develop the disease. The risk identifies who deserves closer attention, not a certain outcome.
5. What is familial pancreatic cancer?
Familial pancreatic cancer means two or more first-degree relatives have had pancreatic cancer with no identifiable single gene to explain it. It accounts for about 7% of all cases. Risk rises with the number of affected relatives and when relatives were diagnosed before age 50.
6. Should I get genetic testing if a relative had pancreatic cancer?
It depends on your family pattern, so discuss it with a genetic counselor. Counseling is often suggested if you have several affected first-degree relatives, a known family mutation, or clustered breast, ovarian, and pancreatic cancers. Anyone diagnosed with pancreatic cancer is now advised to have germline testing.
7. At what age should high-risk people start pancreatic cancer screening?
It varies by gene and family history, so a specialist decides. Surveillance generally begins earlier for higher-risk syndromes like Peutz-Jeghers and around age 50 for some others, and only for people whose lifetime risk is about 5% or higher. Ask a gastroenterologist about your situation.
8. Can hereditary pancreatic cancer be prevented?
There is no proven prevention. For genuinely high-risk people, imaging surveillance with endoscopic ultrasound or MRI aims to catch problems early, though a clear survival benefit is not established. Not smoking is the most consistent way to lower risk, especially in hereditary pancreatitis.
9. Which genetic syndromes are linked to pancreatic cancer?
The main ones are hereditary breast and ovarian cancer (BRCA1/BRCA2), familial atypical multiple mole melanoma (CDKN2A), Peutz-Jeghers syndrome (STK11), hereditary pancreatitis (PRSS1), and Lynch syndrome (mismatch repair genes). PALB2 and ATM are also linked. Each carries a different level of risk.
10. Does pancreatic cancer skip generations?
Inherited pancreatic cancer genes are usually autosomal dominant, so each child of a carrier has about a 50% chance of inheriting the change. Cancer can appear to skip a generation because not everyone who inherits a mutation develops it — the gene passes on even when the disease does not.
11. If I have a gene mutation, will I definitely get pancreatic cancer?
No. A mutation raises your risk but does not guarantee cancer, and most carriers never develop pancreatic cancer. The result is useful because it can guide screening and, after a diagnosis, treatment choices. A genetic counselor can help you understand your specific risk.
The bottom line on inherited pancreatic cancer risk
Most pancreatic cancer is not inherited. About 1 in 10 cases has a family or genetic link, and even among people who carry a high-risk mutation, most never develop the disease — a mutation is a reason for attention, not a verdict.
If pancreatic cancer runs in your family, or you carry a known mutation, the most useful next step is a conversation with a genetic counselor or your physician, who can weigh your personal and family history and explain whether testing or surveillance fits your situation. Genetic information helps most when it leads to a clear, individual plan rather than worry. For the full picture of symptoms, diagnosis, and treatment, the complete pancreatic cancer overview is the place to continue.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.