On This Page – Quick Medical Summary
You just received a positive BRCA test result — here is what it actually means
There is a specific kind of silence that follows a positive BRCA gene test result. It lands differently than most medical news — because the word “positive” in genetic testing does not mean what most patients expect.
In my clinical practice as a gynecologic oncologist, the first thing I tell every patient who receives a positive BRCA result is this: you have not been diagnosed with cancer. You have received information — precise, actionable information — that can be used to protect your health in ways most unscreened individuals never have the opportunity to act on.
Understanding your BRCA result begins with the broader picture of how hereditary mutations connect to cancer development — a foundation laid in our guide to breast cancer stages and survival.
ℹ️ Medical Disclaimer: The genetic test result interpretations, lifetime risk estimates, risk-reduction procedures, chemoprevention agents, and insurance coverage information discussed in this article reflect current clinical guidelines and are provided for educational purposes only. Individual risk assessments, treatment decisions, surgical planning, and insurance determinations depend on factors including personal cancer history, specific variant data, family history density, reproductive history, and the judgment of your treating specialist. Consult a board-certified gynecologic oncologist and a certified genetic counselor before acting on any clinical information in this article.
What BRCA1 and BRCA2 mutations are — and why they matter
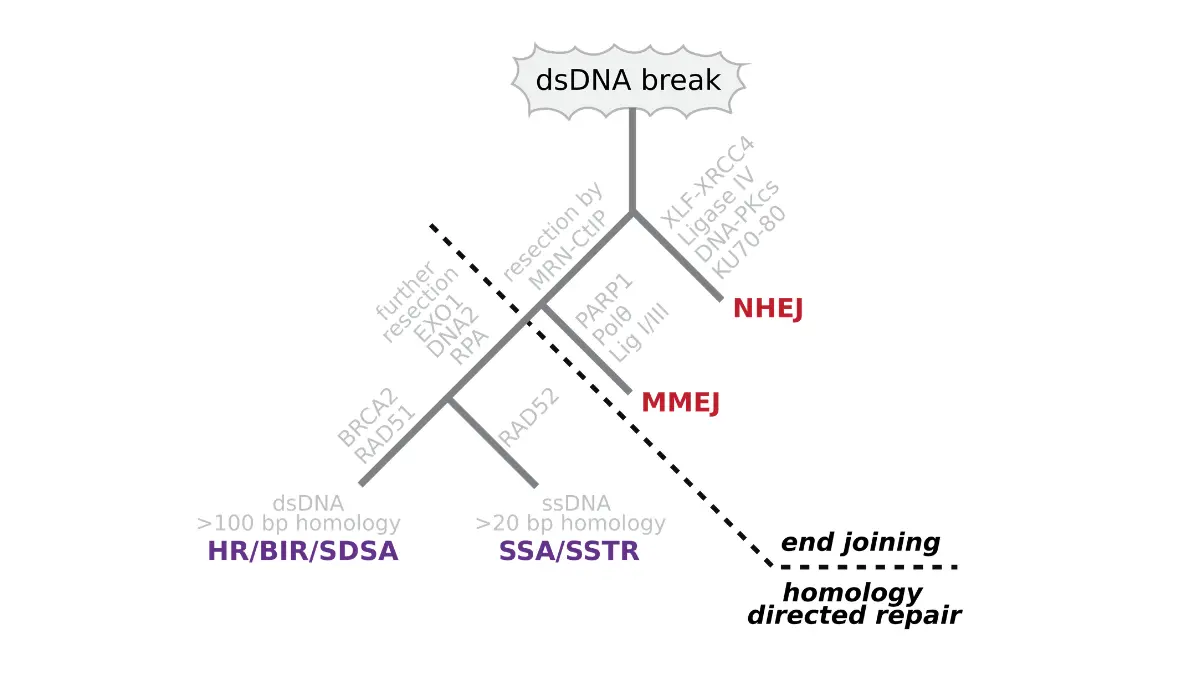
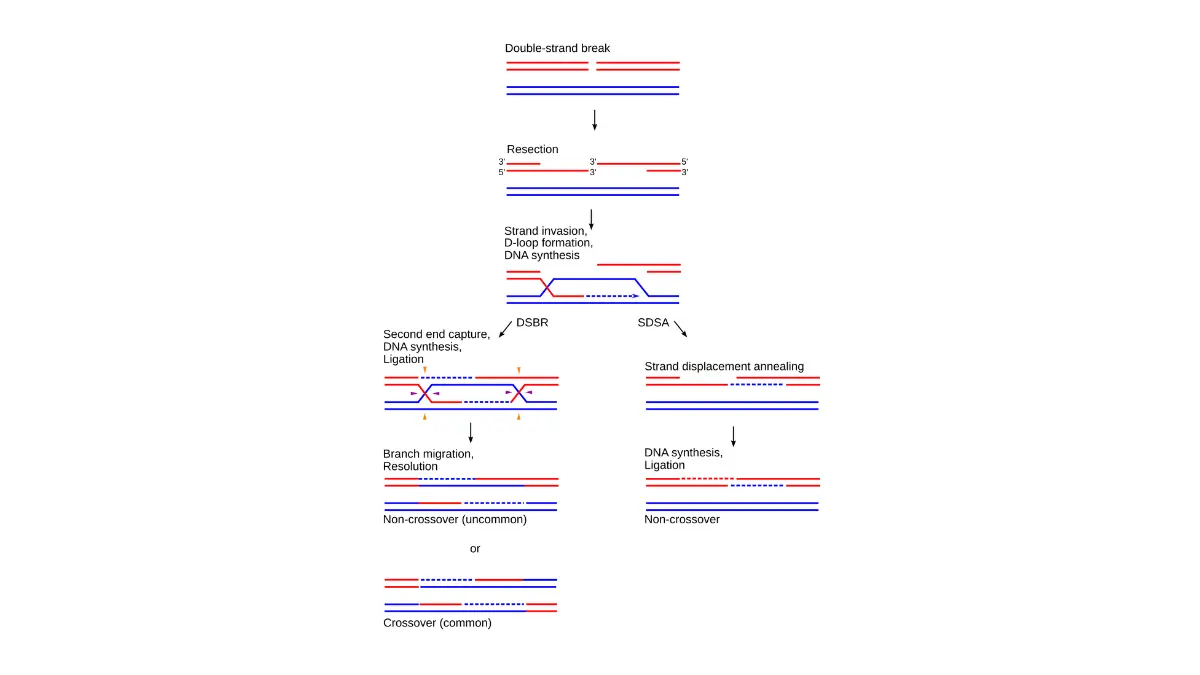
BRCA1 and BRCA2 are tumor suppressor genes whose normal function is to produce proteins that repair double-strand breaks in DNA — a type of molecular damage that, if left uncorrected, allows cancer-promoting mutations to accumulate across cell generations.
When a pathogenic variant disrupts the function of either gene, this repair checkpoint fails. Cells divide with accumulated genetic errors. Breast and ovarian tissue — particularly sensitive to this loss of repair capacity — faces substantially elevated malignant transformation risk over time.
Hereditary breast and ovarian cancer syndrome (HBOC) is the clinical term for the inherited condition defined by a pathogenic BRCA variant. Understanding the mechanism is not academic. It explains why surveillance catches disease earlier and why the timing of risk-reduction decisions matters.
How BRCA1 and BRCA2 protect your cells — and what happens when they don’t
The BRCA proteins function within the body’s homologous recombination repair (HRR) system — the molecular mechanism responsible for correcting the most severe class of DNA damage before a cell divides and copies its errors into daughter cells.
🔬 How It Works: Think of BRCA1 and BRCA2 as the spell-check function of your DNA. When they work normally, copying errors in your genetic code are caught and corrected before cell division. When a pathogenic BRCA variant is present, that spell-check is disabled — errors accumulate, are copied into daughter cells, and over time can drive cancer development. This is why BRCA mutations are called high-penetrance variants: the biological pathway from mutation to elevated cancer risk is direct and clinically well-established.
The Ashkenazi Jewish population carries a BRCA founder mutation at an estimated prevalence of approximately 1 in 40 — compared to approximately 1 in 300–500 in the general US population. This population-specific prevalence is one reason NCCN 2026 guidelines include Ashkenazi Jewish ancestry as a standalone criterion for BRCA gene testing referral.
Who should get a BRCA gene test: the 2026 NCCN criteria
NCCN 2026 Genetic/Familial High-Risk Assessment Guidelines recommend BRCA gene testing for individuals who meet one or more of the following criteria:
- Personal history of breast cancer diagnosed at or before age 50
- Personal history of ovarian, fallopian tube, or primary peritoneal cancer at any age
- Personal history of triple-negative breast cancer at any age
- Personal history of male breast cancer at any age
- A first-degree relative with a confirmed pathogenic BRCA1 or BRCA2 variant
- Ashkenazi Jewish ancestry with any first-degree relative diagnosed with breast or ovarian cancer
- Two or more close relatives on the same side of the family diagnosed with breast or ovarian cancer
Before scheduling a specialist appointment, use our hereditary cancer risk assessment tool to map your personal family history pattern — it helps you arrive at your first genetic counseling consultation with a structured clinical picture.
📊 Clinical Data Point: The Ashkenazi Jewish population carries a BRCA1 or BRCA2 founder mutation at a prevalence of approximately 1 in 40, compared to approximately 1 in 300–500 in the general US population. Source: NCI guide to BRCA1 and BRCA2 hereditary cancer, 2026.
A BRCA mutation is among the highest-impact breast cancer risk factors documented in hereditary oncology — but it interacts with additional clinical variables, including hormone exposure, reproductive history, and prior biopsy findings, that your genetic counselor will weigh during a full risk assessment.
✅ Patient Action: If your personal or family history matches any criterion above, consult an ABMG-certified genetic counselor to determine whether clinical-grade BRCA gene testing is appropriate for your situation before purchasing any at-home genetic screening option — direct-to-consumer kits use a different testing methodology than a physician-ordered multi-gene panel and do not capture all clinically significant variants.
What a positive BRCA test result actually means for you
A positive BRCA gene test result means a pathogenic variant has been identified in your BRCA1 or BRCA2 gene — significantly elevating your lifetime risk of developing breast and ovarian cancer compared to the general population, but not confirming that cancer is currently present or that it is inevitable.
This distinction is the most important clinical fact in this entire article. A genetic predisposition is not a diagnosis.
A positive BRCA result: predisposition, not diagnosis
Every person carries two copies of each gene — one inherited from each parent. A positive BRCA result means one copy carries a mutation that impairs its function. The remaining copy may still be functional.
The elevated cancer risk comes from the statistical probability that over a lifetime, sufficient additional genetic errors accumulate to override that remaining copy’s repair capacity. That process is neither instant nor certain. BRCA carriers who pursue NCCN-recommended surveillance and specialist-led risk management can meaningfully alter that trajectory, as documented across breast cancer survival rate data at every stage of disease caught through enhanced monitoring.
What a variant of uncertain significance (VUS) means — and what it does not mean
Variant of uncertain significance (VUS) is a laboratory classification that appears on some BRCA test reports. It is not a positive result. It means the laboratory identified a genetic change in BRCA1 or BRCA2 whose clinical significance has not yet been scientifically established.
⚠️ Clinical Warning: A VUS result must never trigger prophylactic mastectomy or risk-reducing salpingo-oophorectomy. These are irreversible surgical procedures. A VUS is not a confirmed pathogenic variant — the scientific community is still studying its implications. If your report includes a VUS, contact a board-certified genetic counselor who can check current reclassification databases, including ClinVar and LOVD, for the most recent evidence on your specific variant before any clinical management decision is made.
If you are experiencing any new breast changes alongside your BRCA result, use our symptom checker for a first clinical orientation before contacting your physician.
What a negative BRCA result means — and its clinical limits
A negative BRCA test result means no pathogenic variant was identified in the specific genes tested. It does not mean you are free from hereditary breast cancer risk entirely.
BRCA1 and BRCA2 are not the only genes associated with elevated hereditary breast cancer risk. High-penetrance variants in PALB2, TP53, CHEK2, and ATM are not captured on a BRCA-only panel. If your family history is strongly suggestive of hereditary cancer despite a negative BRCA result, your gynecologic oncologist may recommend expanded multi-gene panel testing.
Early warning signs that BRCA carriers should monitor are detailed in our guide to breast cancer symptoms and what warrants immediate evaluation. For a plain-language breakdown of how pathogenic, benign, and uncertain variant classifications are determined, the BRCA genetic testing overview on MedlinePlus explains laboratory terminology in patient-accessible terms.
✅ Patient Action: If your BRCA test returned a variant of uncertain significance, ask your physician to arrange a consultation with a board-certified genetic counselor who can access current variant reclassification databases — specifically ClinVar and the Leiden Open Variation Database (LOVD) — to determine whether new evidence has reclassified your specific variant since the test was processed.
BRCA1 vs. BRCA2: how your lifetime cancer risk compares
BRCA1 and BRCA2 mutations carry meaningfully different lifetime cancer risk profiles. The distinction is clinically significant — it directly determines surveillance start ages, the timing of risk-reduction surgery decisions, and which cancer types require monitoring beyond breast and ovarian.
📊 Clinical Data Point: The lifetime risk estimates below reflect population-level data from NCI SEER hereditary cancer surveillance through 2026. All figures represent cumulative lifetime risk to age 80 at the population level and must be interpreted alongside individual variables including family history density, reproductive history, and additional genetic variants. Source: NCI SEER hereditary cancer surveillance data, 2026.
Lifetime breast cancer risk: BRCA1 vs. BRCA2 vs. the general population
| Cancer Type | BRCA1 Lifetime Risk | BRCA2 Lifetime Risk | General Population |
|---|---|---|---|
| Breast cancer | 65–72% | 45–69% | ~13% |
| Ovarian cancer | 39–44% | 11–17% | ~1–2% |
| Contralateral breast cancer (after first primary) | ~40–60% | ~30–50% | ~6–10% |
| Male breast cancer | <2% | 6–8% | <0.1% |
Source: NCI SEER 2026 hereditary cancer surveillance data. All figures represent population-level lifetime risk to age 80.
Lifetime ovarian cancer risk by mutation type
The ovarian cancer risk differential between BRCA1 and BRCA2 is the most clinically significant distinction in this table. BRCA1 carriers face a lifetime ovarian cancer risk of 39–44% — compared to the general population’s 1–2% — a magnitude of difference that directly informs the timing recommendation for risk-reducing salpingo-oophorectomy (RRSO).
NCCN 2026 guidelines recommend considering RRSO for BRCA1 carriers between ages 35 and 40, and for BRCA2 carriers between ages 40 and 45, after childbearing is complete. This timing gap — five to ten years — is clinically deliberate and mutation-type specific.
🩺 Physician Note: “In my clinical practice, the ovarian cancer risk differential between BRCA1 and BRCA2 is the first table I want every patient to understand — because BRCA1 carriers need to make RRSO timing decisions in their mid-30s, while BRCA2 carriers typically have more time to plan. I have seen BRCA1 carriers delay this conversation until their mid-40s, believing they had the same timeline as BRCA2 carriers. They do not. The window for maximum risk reduction from RRSO closes with natural menopause.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
Other cancer risks associated with BRCA mutations
BRCA2 carriers carry an elevated lifetime risk of pancreatic cancer (approximately 3–5% vs. ~1% in the general population) and prostate cancer risk elevated above the general male baseline. BRCA1 carriers face a significantly elevated risk of contralateral breast cancer after a first primary breast cancer diagnosis.
✅ Patient Action: Ask your genetic counselor which cancer types are included in your NCCN-recommended surveillance protocol based on your specific mutation type. A BRCA2 carrier’s monitoring plan should explicitly address pancreatic cancer risk surveillance — not only breast and ovarian cancer monitoring. Consult a board-certified genetic counselor for a personalized risk calculation using validated models such as BOADICEA or CanRisk.
Your clinical next steps after a positive BRCA result
After a confirmed positive BRCA gene test, your clinical action pathway begins with four evidence-based steps supported by NCCN 2026 Genetic/Familial High-Risk Assessment Guidelines.
These steps are sequenced deliberately. The two most common clinical errors in newly positive patients — acting too quickly on surgical decisions before completing the counseling process, and waiting too long to initiate any surveillance — are both prevented by following this sequence.
Step 1: Schedule a certified genetic counseling appointment
Contact an ABMG-certified genetic counselor as your first step — before making any management decision. Your counselor will confirm your variant classification, calculate your personalized risk using validated models such as BOADICEA or CanRisk, and coordinate your specialist referral pathway.
Step 2: Request a referral to a gynecologic oncologist or high-risk breast program
A gynecologic oncologist or multidisciplinary high-risk breast program is the appropriate specialist setting for ongoing BRCA management. Your primary care physician can initiate this referral based on your positive result alone.
Step 3: Start your enhanced surveillance protocol
📊 Clinical Data Point: NCCN 2026 Genetic/Familial High-Risk Assessment Guidelines recommend annual breast MRI beginning at age 25 for BRCA1 carriers and between ages 25 and 30 for BRCA2 carriers, alternating with mammography every 6 months for high-risk surveillance. Source: NCCN 2026 Genetic/Familial High-Risk Assessment: Breast and Ovarian Guidelines.
Enhanced MRI surveillance is non-invasive, evidence-based, and recommended immediately — it does not require waiting for a surgical decision. BRCA carriers begin enhanced imaging significantly earlier than the general population schedule. For the full age-specific comparison, see our breast cancer mammogram screening age guide.
Step 4: Inform your first-degree relatives and initiate cascade testing
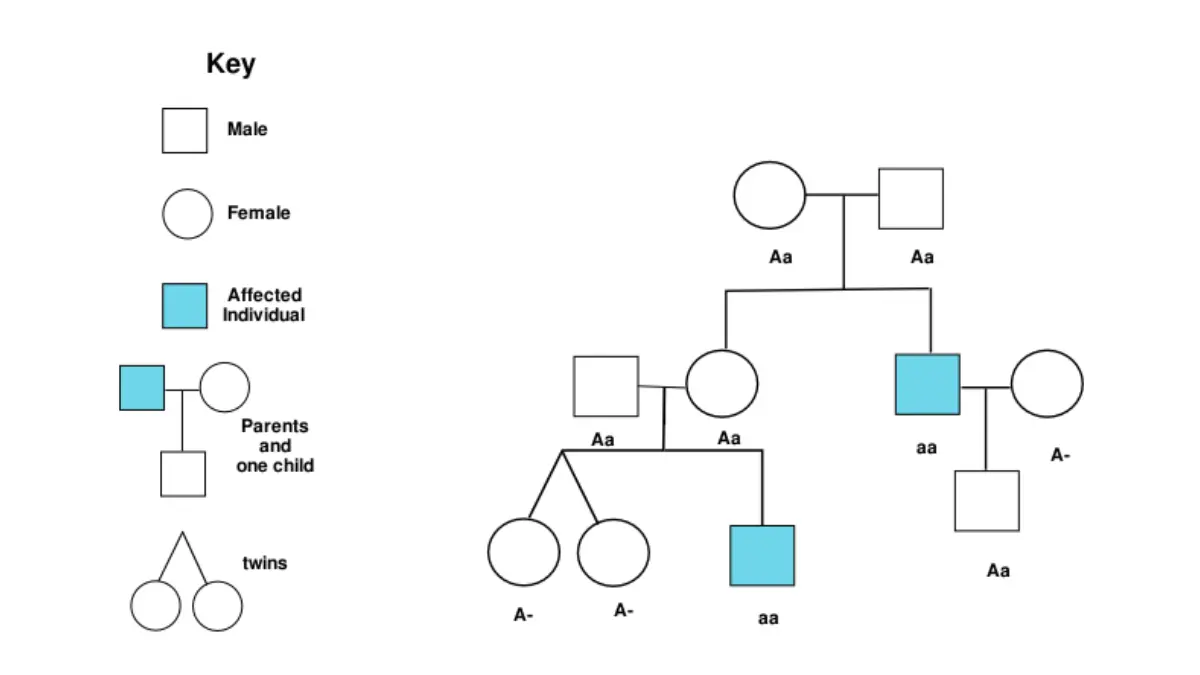
Each biological parent, sibling, and child of a BRCA-positive individual has a 50% probability of carrying the same pathogenic variant. Your genetic counselor will guide the family notification process — the counselor, not the patient alone, should lead this conversation to prevent misunderstanding of what the result means for relatives.
✅ Patient Action: Before making any decision about prophylactic mastectomy or risk-reducing salpingo-oophorectomy, consult a board-certified gynecologic oncologist. These are irreversible procedures requiring a full risk-benefit discussion that incorporates your specific mutation type, age, reproductive plans, and complete family history density.
Prevention and risk-reduction options for BRCA carriers
BRCA carriers have four primary risk-management strategies available. Understanding what each does — and does not — accomplish clinically is essential before your first specialist appointment.
Enhanced surveillance: what it involves and when to start
Enhanced surveillance — annual breast MRI plus mammography — is early detection, not risk reduction. It does not lower the probability of developing cancer. It dramatically increases the probability of catching cancer at a stage where treatment outcomes are substantially better.
This distinction matters. Choosing surveillance over prophylactic surgery is not a passive decision. It is an active, evidence-based clinical choice with a strong benefit-risk profile for many BRCA carriers.
Chemoprevention: tamoxifen, raloxifene, and what the evidence shows
Chemoprevention uses medication to reduce breast cancer risk in high-risk individuals. Tamoxifen is FDA-approved for risk reduction in premenopausal high-risk women. Raloxifene is FDA-approved for postmenopausal women. Both agents carry documented risk profiles — tamoxifen increases endometrial cancer risk and venous thromboembolism risk; raloxifene carries a similar thromboembolism profile.
⚠️ Clinical Warning: Olaparib (Lynparza) and talazoparib (Talzenna) are FDA-approved PARP inhibitors for BRCA-mutated metastatic breast cancer treatment. They are not chemoprevention agents for unaffected BRCA carriers. Using PARP inhibitors outside of an active cancer treatment context is not clinically supported and must not be undertaken without an oncologist’s direction. The distinction between tamoxifen (prevention) and PARP inhibitors (metastatic treatment) is one of the most common sources of patient confusion in BRCA care.
A detailed clinical comparison of chemoprevention agents is covered in our guide to tamoxifen vs. aromatase inhibitors for breast cancer.
Prophylactic surgery: mastectomy and salpingo-oophorectomy for BRCA carriers
Prophylactic mastectomy reduces breast cancer risk by approximately 90% in BRCA carriers. Risk-reducing salpingo-oophorectomy (RRSO) reduces ovarian cancer risk by approximately 80–96% and also reduces breast cancer risk in premenopausal carriers who undergo it before natural menopause. RRSO performed before menopause carries long-term implications for cardiovascular health, bone density, and sexual function — variables that must be reviewed with a specialist before any decision is made.
📊 Clinical Data Point: NCCN 2026 Genetic/Familial High-Risk Assessment Guidelines recommend risk-reducing salpingo-oophorectomy for BRCA1 carriers between ages 35 and 40, and for BRCA2 carriers between ages 40 and 45, after completion of childbearing. Source: NCCN 2026.
For the full clinical picture of mastectomy, including what surgeons discuss privately with patients, see our guide on what your doctor won’t tell you about mastectomy and the lumpectomy vs. mastectomy decision framework.
Insurance coverage and financial considerations for BRCA-related care
The Affordable Care Act (ACA) Section 2713 mandates coverage of preventive services rated Grade B or higher by the USPSTF. The USPSTF carries a Grade B recommendation for BRCA risk assessment, genetic counseling, and testing for women with a family history that increases risk — requiring most ACA-compliant health plans to cover these services without cost-sharing.
Coverage for risk-reducing surgery and enhanced MRI surveillance varies significantly by plan. BRCA carriers interested in investigational prevention strategies can search active BRCA clinical trials on ClinicalTrials.gov using “BRCA” as the condition filter.
✅ Patient Action: Prophylactic mastectomy and risk-reducing salpingo-oophorectomy are irreversible decisions with long-term implications. Before selecting any surgical risk-reduction strategy, consult a board-certified gynecologic oncologist and a plastic surgeon experienced in post-mastectomy reconstruction — this two-specialist pairing is the clinical standard for this decision.
What I tell my patients after a positive BRCA result
In my clinical practice as a gynecologic oncologist, the conversation that follows a positive BRCA gene test result is one of the most consequential I have with a patient — and one of the most frequently misunderstood moments in hereditary cancer care.
The clinical difference between risk and destiny
A positive BRCA result does not determine your medical future. It informs it.
BRCA carriers who pursue active specialist-led management face a dramatically different clinical trajectory than unscreened individuals with the same underlying mutation operating in the dark. Risk is a probability at the population level — it is influenced, meaningfully, by the clinical decisions you make in the next twelve months.
🩺 Physician Note: “The patients I worry about most are not the ones who call me frightened after their positive result. The ones who concern me are those who go quiet — who receive a positive BRCA result, feel overwhelmed, and do nothing for six months. That period of inaction is precisely when proactive specialist engagement is most valuable. A positive BRCA result is not a sentence. It is an opening — to monitor, to intervene, to stay ahead of a risk that previously had no clinical handle.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
What I want every patient to understand before making any decision
Two clinical errors dominate what I observe in newly positive BRCA patients. The first is moving immediately toward prophylactic surgery before completing the genetic counseling process. The second is receiving a positive result, feeling overwhelmed, and deferring all action — no surveillance, no referral, no family notification — for months or years.
Both are understandable responses to an emotionally charged moment. Both are preventable with early specialist engagement.
If you have received a positive BRCA result and have not yet been seen by a gynecologic oncologist or a hereditary cancer program, schedule that appointment now. Early engagement with a board-certified gynecologic oncologist is the single most impactful clinical step available to you in the first 90 days after a positive result.
Frequently asked questions about BRCA gene testing and positive results
1. What is a BRCA gene test?
A BRCA gene test analyzes your BRCA1 and BRCA2 genes for pathogenic variants — mutations that impair the genes’ DNA repair function and significantly elevate lifetime breast and ovarian cancer risk. The test uses next-generation sequencing and is typically ordered by a physician based on personal or family history criteria. It does not diagnose cancer. It identifies hereditary predisposition. Consult a board-certified genetic counselor to interpret your specific results.
2. What does it mean if I test positive for BRCA?
A positive BRCA gene test means a pathogenic variant has been confirmed in your BRCA1 or BRCA2 gene, significantly elevating your lifetime risk of breast cancer (up to 72% for BRCA1 carriers) and ovarian cancer relative to the general population. It does not mean cancer is present now or that it is certain. BRCA carriers who follow NCCN-recommended surveillance and specialist management can substantially alter their clinical risk trajectory. Consult a board-certified gynecologic oncologist to develop your personalized management plan.
3. What is the difference between BRCA1 and BRCA2?
BRCA1 and BRCA2 mutations carry different risk profiles. BRCA1 carriers face a lifetime breast cancer risk of approximately 65–72% and an ovarian cancer risk of 39–44%. BRCA2 carriers face a breast cancer risk of approximately 45–69% and an ovarian cancer risk of 11–17%. BRCA2 also carries an elevated male breast cancer risk of approximately 6–8%. These differences directly affect surveillance start ages and surgical risk-reduction timing. Consult a board-certified genetic counselor for personalized risk modeling using validated tools.
4. Does testing positive for BRCA mean I will definitely get cancer?
No. A positive BRCA gene test means your lifetime cancer risk is significantly elevated — not that cancer is certain. A meaningful proportion of BRCA carriers who follow NCCN-recommended enhanced surveillance and risk-reduction strategies do not develop breast or ovarian cancer during their lifetime. Your individual risk depends on your specific variant, age, reproductive history, and the management steps you pursue. Consult a board-certified genetic counselor for a personalized risk calculation before making any clinical decision.
5. Who should get a BRCA gene test?
NCCN 2026 guidelines recommend BRCA gene testing for individuals with a personal history of breast cancer before age 50, ovarian cancer at any age, triple-negative breast cancer, male breast cancer, a first-degree relative with a confirmed BRCA mutation, Ashkenazi Jewish ancestry with an affected first-degree relative, or multiple family members with breast or ovarian cancer on the same side of the family. Consult a board-certified genetic counselor before pursuing any at-home genetic screening option.
6. What is a variant of uncertain significance on a BRCA test?
A variant of uncertain significance (VUS) on a BRCA test is a genetic change whose clinical impact has not yet been established. It is not a positive result. A VUS should never justify prophylactic surgery — it is not a confirmed pathogenic variant. Classifications change as new evidence emerges. A board-certified genetic counselor can access current databases including ClinVar and LOVD to determine whether your specific variant has been reclassified since your test was processed.
7. What are my options after a positive BRCA result?
After a confirmed positive BRCA gene test, your evidence-based options include enhanced surveillance (annual breast MRI plus mammography), chemoprevention (tamoxifen for premenopausal, raloxifene for postmenopausal women), risk-reducing salpingo-oophorectomy, and prophylactic mastectomy. Enhanced surveillance is non-invasive and recommended immediately. Surgical options require a full risk-benefit discussion with a specialist before any decision is finalized. Clinical trial participation is available for BRCA carriers seeking investigational strategies. Consult a board-certified gynecologic oncologist before initiating any risk-reduction procedure.
8. Does insurance cover BRCA gene testing?
Most ACA-compliant plans must cover BRCA gene testing without cost-sharing for individuals meeting USPSTF Grade B criteria — which includes women with a personal or family history placing them at elevated hereditary breast cancer risk. Coverage for risk-reducing surgery and enhanced MRI surveillance varies significantly by plan. Review your specific policy with an insurance navigator before scheduling any procedure, and obtain written prior authorization confirmation for each service from your insurer before your appointment.
9. Can men develop breast cancer if they carry a BRCA mutation?
Yes. Male breast cancer is a documented risk for BRCA2 carriers, with a lifetime risk of approximately 6–8% — compared to less than 0.1% in the general male population. BRCA1 carriers carry a lower but still elevated male breast cancer risk. Men with a confirmed BRCA mutation should be referred to a genetic counselor and an oncologist familiar with male hereditary cancer syndromes, as surveillance protocols differ from those used for female carriers. Consult a board-certified oncologist experienced with male BRCA management.
10. What happens to my family members if I test positive for BRCA?
If you test positive for a BRCA mutation, each first-degree biological relative — parents, siblings, and children — has a 50% probability of carrying the same pathogenic variant. Your genetic counselor will guide you on how to communicate this to family members appropriately. Relatives who choose testing can then access the same surveillance and risk-reduction options available to you. Your counselor can provide a family notification letter detailing your specific variant to facilitate targeted cascade testing at lower cost.
11. What is cascade genetic testing?
Cascade genetic testing means systematically offering the BRCA gene test to biological relatives of someone who has already tested positive — beginning with first-degree relatives, who carry the highest probability of carrying the same variant. A genetic counselor can provide family members with a letter detailing the specific variant detected, enabling targeted single-variant testing at significantly lower cost than a full-panel screen. Family members can initiate cascade testing independently without the original patient’s physician referral.
Your BRCA result is clinical information — not a verdict
A positive BRCA gene test result is not a cancer diagnosis. It is medical information — precise, actionable, and in the right clinical hands, genuinely protective.
Three steps matter most in your next 90 days. Schedule a consultation with an ABMG-certified genetic counselor. Inform your first-degree relatives through your counselor’s guidance so they can access cascade testing. Begin the NCCN-recommended enhanced surveillance protocol appropriate for your specific mutation type — starting with annual breast MRI at the age specified for your variant.
Consult a board-certified gynecologic oncologist and a certified genetic counselor to develop a personalized management plan before initiating any risk-reduction procedure, chemoprevention regimen, or surgical intervention.
To complement what you have read here, our guide on how to read your BRCA results in 60 seconds walks through the specific laboratory language on your actual report. For a broader overview of hereditary breast cancer risk and family history patterns, the American Cancer Society guide to hereditary breast cancer and BRCA testing is a reliable patient-facing resource from a nationally recognized oncology organization.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.