On This Page – Quick Medical Summary
You just found out someone you love has breast cancer
Whether your spouse received her diagnosis this morning or your mother just finished her second cycle of chemotherapy, caregiver breast cancer support is not something most people are born knowing how to provide. It is a set of learnable, phase-specific skills. The fact that you are searching for guidance right now is already the most important step.
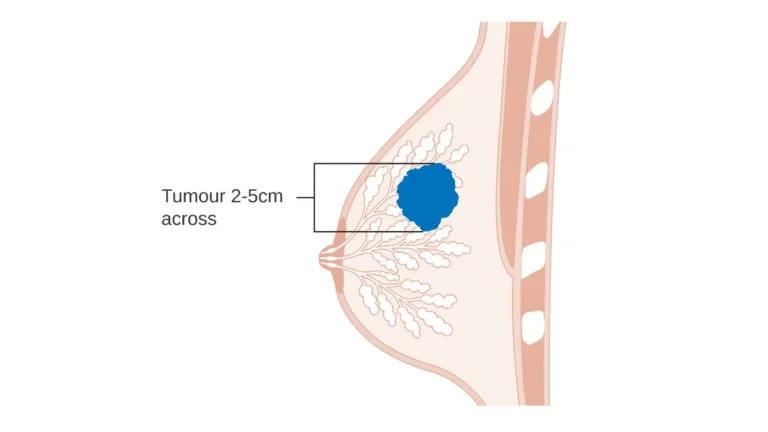
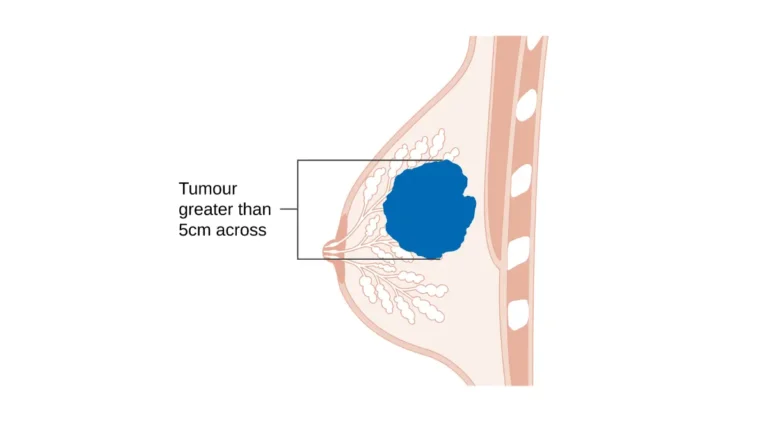
Understanding the diagnosis itself is the foundation of everything that follows. Our guide to breast cancer stages and survival explains every stage, treatment pathway, and what the prognosis data actually means in plain language.
ℹ️ Medical Disclaimer: The treatment protocols, medication information, surgical recovery guidance, insurance navigation content, and mental health intervention strategies discussed in this article reflect current clinical standards and are provided for educational purposes only. Individual treatment decisions, medication adjustments, surgical care plans, and diagnostic conclusions depend on the patient’s specific diagnosis, staging, comorbidities, laboratory results, and the recommendations of the treating oncology team. Consult a board-certified oncologist before acting on any treatment-related clinical information in this article. Caregivers experiencing persistent emotional distress or symptoms of depression should consult their own board-certified primary care physician.
What being a breast cancer caregiver actually means
Caregiver support is not one job. It is three distinct functions — and knowing which one the moment requires is the skill that separates effective caregiving from exhausted, well-intentioned chaos.
Supporting someone through breast cancer means providing three types of help, each with a different demand profile:
- Emotional presence — Being available, non-reactive, and emotionally regulated in your loved one’s worst moments. This is not the same as projecting relentless optimism.
- Practical logistics — Meals, transportation, medication tracking, household management, and appointment coordination throughout the treatment arc.
- Clinical navigation — Communicating with the oncology team, recognizing treatment-related red flags, and advocating appropriately in clinical settings without overstepping the patient’s autonomy.
The three functions of a breast cancer caregiver
The American Cancer Society guide for cancer caregivers identifies specific communication behaviors that patients consistently rate as helpful — and behaviors that consistently increase patient distress, regardless of the caregiver’s intention. The most common distress-causing behaviors share one pattern: decisions made for the patient rather than with her.
What the patient actually needs — and what they don’t
Your loved one’s need for autonomy does not disappear with a diagnosis. The single most useful question a caregiver can ask — and ask regularly, because the answer changes — is: “What would actually help most right now?”
Caregivers who understand the physical changes that can develop during treatment are better positioned to recognize what warrants an urgent call. The warning signs and symptoms of breast cancer provides the clinical baseline every caregiver should review.
✅ Patient Action: Before your next conversation with your loved one, ask directly: “What kind of support would actually help this week — and what would feel like too much?” Write the answer down and share it with other family members offering to assist. This single conversation reduces caregiver-patient friction more than almost anything else in the first weeks after diagnosis.
What to say — and what not to say — to someone with breast cancer
Words land differently after a breast cancer diagnosis. The gap between what a caregiver intends and what the patient experiences is real, documented in psycho-oncology research, and entirely preventable.
Phrases that genuinely help — and why they work
Emotional support after diagnosis does not require answers. These phrases work because they open a conversation rather than closing one:
- “I’m here for whatever you need — tell me specifically what that looks like.”
- “You don’t have to have it together around me.”
- “I’m bringing dinner Thursday — does that work for you?” (A specific offer the patient can simply say yes or no to.)
- “What would help most right now, today?”
What not to say: five phrases that consistently increase patient distress
Psycho-oncology literature consistently identifies these as patient-reported distress amplifiers, regardless of the caregiver’s intention:
- “Everything happens for a reason” — Imposes meaning the patient did not ask for and cannot yet access.
- “You’ll beat this” / “Stay positive” — Places emotional labor on the patient. She cannot always feel positive, and she should not have to perform optimism for your comfort.
- “I know how you feel” — You do not. No one does. Not even other survivors.
- “At least it was caught early” / “At least it’s the good kind” — There is no stage at which minimizing a cancer diagnosis is appropriate or accurate.
- “Have you tried [supplement / diet / alternative therapy]?” — Unsolicited treatment research is consistently rated as dismissive of the patient’s care team and intrusive to her clinical decisions.
🩺 Physician Note: “The caregivers who inadvertently make things harder are almost never unkind — they are terrified. Their fear becomes the patient’s burden to manage. Your role is not to project certainty you don’t have. It is to make your loved one feel less alone in the uncertainty.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
How to help during chemotherapy, radiation, and surgery
The active treatment phase is when the caregiver role becomes most clinically demanding — and when the gap between general goodwill and specific clinical knowledge is widest.
🔬 How It Works: Chemotherapy drugs target rapidly dividing cancer cells — but also suppress the bone marrow’s production of white blood cells. This creates neutropenia: a window when the patient’s ability to fight infection is severely compromised. The cardinal symptom caregivers must monitor at home is fever, because it is the earliest detectable signal of neutropenic crisis.
Caregiving through chemotherapy: what to watch, what to do
The most critical fact for every chemotherapy caregiver: a temperature of 100.4°F (38°C) or higher during active chemotherapy requires an immediate call to the oncology team’s after-hours line — not urgent care, not watchful waiting.
⚠️ Clinical Warning: A fever of 100.4°F (38°C) or higher in a patient on active chemotherapy is a potential neutropenic emergency. Call the oncology team’s after-hours line immediately. Do not drive to urgent care without calling first. Do not wait for a scheduled appointment. Delaying this call can be life-threatening.
Beyond fever surveillance, the caregiver’s clinical checklist during chemotherapy includes:
- Hydration tracking daily — Nausea and vomiting can cause rapid dehydration requiring IV fluids. Know your team’s threshold for escalating to IV hydration (typically inability to keep any fluids down for 12–24 hours — confirm with the oncologist).
- Maintaining the antiemetic schedule — Anti-nausea medications work most effectively taken on schedule, not reactively. A written medication log is a clinical tool.
- Minimizing infection exposure — During the post-infusion nadir window (typically 7–14 days), limit crowded environments, practice rigorous hand hygiene before patient contact, and keep the living space clean and ventilated.
The chemo side effects in breast cancer treatment guide covers every major chemotherapy reaction and what the oncology team can adjust. Caregivers can use our Symptom Checker to log daily symptom observations in an organized format before each oncology visit.
Following NCCN supportive care clinical guidelines clarifies which symptom thresholds require emergency escalation versus at-home management during each phase of the treatment cycle.
Supporting your loved one after surgery
Mastectomy and lumpectomy recovery both require specific caregiver tasks — surgical drain care, wound monitoring, and activity restriction management — that the patient often cannot perform independently. Our clinical guide to lumpectomy vs. mastectomy and what the recovery actually involves covers the post-surgical care protocol in detail.
Caregivers should also understand lymphedema risk after breast cancer surgery — a long-term complication that requires specific arm-care practices beginning immediately in the post-surgical period.
✅ Patient Action: Before the surgical date, ask the surgeon directly: “What are the specific signs of wound infection I should call about immediately — and what is your after-hours line?” Write down the exact answer. Consult the treating board-certified oncologist before adjusting any home care protocol, supplement, or medication during active treatment or post-surgical recovery.
Managing appointments, medications, and caregiving logistics
Breast cancer caregiving involves a logistical burden that the oncology system rarely prepares families for — and one that grows more complex as treatment extends over months.
How to be effective at oncology appointments
The most effective caregiver at an oncology visit arrives with three things: a written symptom log covering the period since the last appointment, one priority question identified in advance, and a way to take notes. Verbal recall in a clinical environment under emotional stress is unreliable. Written records are clinical tools, not extra effort.
Before every visit, reviewing specific questions to ask your breast cancer care team — organized by treatment phase — ensures you are asking what matters most at each stage of the arc.
Medication tracking, insurance, and financial navigation
Endocrine therapy — including tamoxifen and aromatase inhibitors, often prescribed for five to ten years after active treatment — requires a written log tracking drug name, dose, time, and reported side effects. Memory in this context is not a system.
Insurance denials for breast cancer treatment-related services are common. The oncology social worker and patient financial advocate can handle prior authorization appeals — but most caregivers do not know to request these services proactively.
✅ Patient Action: At the first oncology appointment, ask: “Do you have a financial navigator or oncology social worker on staff, and can we schedule a meeting?” Before modifying any medication schedule, supplement protocol, or home care plan, consult the treating board-certified oncologist or assigned breast cancer nurse navigator directly.
Who on the care team can actually help you
Three clinical roles exist specifically to support caregivers — and most caregivers never use them:
- Breast cancer nurse navigator — A licensed RN with oncology specialty training who coordinates the treatment plan, educates patients and caregivers on side effects and protocols, and serves as the clinical point of contact between scheduled appointments.
- Oncology social worker — Provides psychosocial support, connects caregivers with community resources, and assists with insurance navigation and financial aid applications.
- Patient financial advocate — Handles billing disputes, copay assistance program enrollment, and prior authorization support for denied treatment claims.
How to take care of yourself while caring for someone with cancer
Breast cancer caregivers need structured emotional support, explicit permission to acknowledge their own grief, and direct access to oncology social workers — because caregiver distress is a documented clinical condition, not evidence that the caregiver is failing at their role.
Caregiver burnout vs. secondary traumatic stress: knowing the difference
These are two distinct clinical conditions. The distinction matters because the appropriate intervention differs:
- Secondary traumatic stress — A trauma-spectrum response triggered by witnessing another person’s suffering. Symptoms include intrusive thoughts, hypervigilance, emotional numbing, and avoidance. This is a trauma response, not exhaustion.
- Caregiver burnout — A chronic stress depletion syndrome with gradual onset: deepening exhaustion, emotional detachment, and a declining sense of caregiving efficacy. This is a depletion response.
🩺 Physician Note: “The most common reason caregivers don’t seek help is the belief that doing so is a betrayal of the person they are caring for. From a clinical standpoint, the opposite is true. A caregiver who is decompensating cannot provide the sustained, attentive care that active treatment requires. Your health is a treatment variable.” — Dr. Alicia M. Thornton, MD, Internal Medicine and Preventive Health
Specific steps you can take this week
Sleep disruption is one of the earliest clinical signs of caregiver decompensation. Our Sleep Calculator helps quantify your sleep deficit — share the result with your own physician if disruption has persisted for more than two weeks.
The NCI resources for cancer caregivers provides evidence-based guidance on caregiver distress management, including referrals to licensed oncology social workers at no cost through most cancer center settings.
CancerCare free counseling services for caregivers connect caregivers with oncology social workers for individual and group counseling at no charge — a resource most caregivers discover too late.
✅ Patient Action: If you are experiencing persistent sleep disruption — fewer than five hours per night for more than two consecutive weeks — or inability to function in daily activities, seek evaluation from your own board-certified primary care physician immediately. If caregiver depression symptoms persist after active treatment ends, consult a licensed therapist with psycho-oncology experience.
Dr. Fairweather: the one thing breast cancer caregivers get wrong most often
In fifteen years of caring for women with breast cancer, the pattern I see most consistently is this: caregivers who have quietly taken over their loved one’s experience of illness, rather than supporting her through it.
From the clinic: what I tell every caregiver at diagnosis
The impulse comes from love. A caregiver sees suffering and wants to eliminate it — so they begin making decisions, filtering information, projecting certainty, filling every silence with optimism. The patient, who already feels she has lost control of her body, now loses control of how she is allowed to experience her own diagnosis. I call this caregiver autonomy erosion. It is the most common clinical mistake I observe, and it is entirely reversible.
The shift that changes everything
Your role is not to manage how your loved one feels about her diagnosis. Your role is to expand what is possible for her — while she remains the author of her own illness experience.
As active treatment ends, connect with the oncology team about a life after breast cancer survivorship care plan. The caregiver role does not end when chemotherapy does. It evolves — and so do its demands.
🩺 Physician Note: “I tell every caregiver the same thing at diagnosis: your loved one needs you to be sturdy, not strong. Strong means performing certainty. Sturdy means being present, stable, and honest — which is the only thing that actually helps over the long arc of treatment and recovery.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
Frequently asked questions about breast cancer caregiver support
1. How do I help my spouse or partner through breast cancer treatment?
A spousal caregiver breast cancer support role is uniquely demanding because proximity creates continuous engagement with no natural break. Partners have access other caregivers don’t: daily symptom observation, medication continuity, and the emotional intimacy that actively reduces patient isolation. Ask every week what form of support would help most — and resist the impulse to decide unilaterally. Consult the treating board-certified oncologist about any changes to the home care or medication protocol.
2. What do breast cancer caregivers struggle with most?
Caregiver breast cancer support is most taxing during active treatment. Research consistently shows that a substantial proportion of breast cancer caregivers experience clinically meaningful levels of anxiety and depression during this period. The most commonly reported struggles are persistent sleep disruption, progressive social isolation, and the sustained effort of managing their own emotional distress while remaining present for the patient. Consult your own board-certified primary care physician if distress persists beyond two consecutive weeks.
3. How do I take care of myself while supporting someone with cancer?
Three specific steps meaningfully improve caregiver sustainability: requesting an oncology social worker referral at your loved one’s cancer center, scheduling one appointment with your own physician this month to address your own health, and tracking your nightly sleep duration to identify whether deprivation has crossed a clinical threshold. Caregiver self-neglect is not dedication — it is a risk factor for caregiver collapse. Consult a board-certified primary care physician if caregiver fatigue affects daily functioning for more than two consecutive weeks.
4. What should I say to someone who was just diagnosed with breast cancer?
The most effective phrases after a breast cancer diagnosis open space rather than closing it. Say: “I’m here for whatever you need — tell me specifically what that looks like.” Or: “You don’t have to have it together around me.” Offer specifically rather than generally: “I’m bringing dinner Thursday — does that work?” Avoid filling silence with reassurance. Silence that communicates presence is more useful than words that communicate your own discomfort with the situation.
5. What phrases should I avoid saying to a cancer patient?
The phrases breast cancer patients most consistently report as distressing include: “Everything happens for a reason,” “You’ll beat this,” “Stay positive,” “I know how you feel,” “At least it was caught early,” and unsolicited suggestions about supplements, diets, or alternative treatments. These phrases are almost never unkind in intent. They are responses to the caregiver’s own fear — and the patient should not have to manage that fear on your behalf.
6. How do I support someone through chemotherapy side effects?
The most critical caregiver task during chemotherapy is fever surveillance. A temperature of 100.4°F (38°C) or higher during active chemotherapy requires an immediate call to the oncology team’s after-hours line — not urgent care, not watchful waiting. Beyond fever monitoring, track daily fluid intake, maintain the scheduled antiemetic regimen, and minimize infection exposure during the 7–14 day post-infusion nadir window. Consult the treating board-certified oncologist before managing any side effect beyond standard hydration and antiemetic protocols at home.
7. What resources are available specifically for breast cancer caregivers?
Three resources most caregivers discover too late: the oncology social worker embedded in most cancer centers (free — request a referral at the first appointment), CancerCare’s free individual and group caregiver counseling led by oncology social workers (available nationally by phone and online), and the NCI caregiver support page, which connects caregivers with evidence-based distress management resources. All three are available at any point in the treatment arc — not only at crisis moments.
8. Can I attend my loved one’s breast cancer appointments with her?
Yes — and caregiver presence at breast cancer appointments is clinically valuable. A caregiver serves as a second set of ears, a note-taker, and a source of between-visit symptom history the patient may not accurately recall under clinical stress. However, some patients prefer to attend specific consultations alone — particularly those involving prognosis, fertility, or major treatment decisions. The patient always retains this right, and a competent oncology team will always respect it.
9. How long does caregiver burnout typically last?
Caregiver burnout does not resolve on a fixed timeline. Recovery depends on whether the primary stressor — active treatment — has concluded, and on whether the caregiver has accessed clinical support. Burnout that develops during treatment often intensifies briefly after treatment ends, as the structure of the caregiving role dissolves without a clear transition. If burnout symptoms persist beyond the active treatment period, consult a licensed therapist with psycho-oncology experience for a structured recovery plan.
10. What does a breast cancer nurse navigator do for caregivers?
A breast cancer nurse navigator is a licensed registered nurse with oncology specialty training who coordinates the treatment plan, educates patients and caregivers on side effect protocols, and serves as the clinical point of contact between scheduled appointments. For caregivers specifically, the nurse navigator answers the question most caregivers are afraid to ask: “Is this symptom serious enough to call after hours?” They operate inside the oncology system — caregivers should not hesitate to contact them between visits.
11. How do I talk to children about a parent’s breast cancer diagnosis?
Age-appropriate language matters more than clinical completeness. For children under eight, say: “Mom is sick with something called breast cancer — the doctors are giving her special medicine to help her get better.” Maintain household routines as consistently as possible; stability is the most powerful source of reassurance for children during a parent’s breast cancer treatment. For children experiencing visible distress, request a referral to a child life specialist or oncology social worker through the cancer center.
Your role as a caregiver is a clinical contribution — not just an emotional one
The skills in this guide are not innate. They are learned. Every breast cancer caregiver who learns them — the clinical red flags, the communication frameworks, the self-care thresholds — makes a measurable difference to their loved one’s treatment experience and recovery trajectory.
As a gynecologic oncologist, I have watched caregivers change the quality of the entire treatment arc — not through medical expertise, but through sustained, informed, emotionally regulated presence. That is what effective caregiving looks like.
The next step is deepening your understanding of the diagnosis your loved one is navigating. Return to our full guide on how breast cancer is staged, treated, and survived — the clinical foundation that makes everything in this guide more actionable.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.