On This Page – Quick Medical Summary
What is lymphedema after breast cancer surgery?
Breast cancer-related lymphedema (BCRL) is an accumulation of lymph fluid in the arm, hand, or chest wall that develops when lymph nodes removed during breast cancer surgery can no longer drain fluid normally from the upper body.
If you are reading this because your arm feels heavier, tighter, or larger than usual after surgery, start with the signs and symptoms section — those observations need clinical assessment soon, not a waiting approach. If you are preparing for upcoming surgery and want to reduce your risk before the procedure, go directly to the prevention section. If you are a caregiver supporting a family member through recovery, the symptoms section and the long-term complications section carry the most actionable guidance.
BCRL is not a sign that something went wrong during your surgery. It is a recognized clinical consequence of lymph node removal — and when detected at an early stage, sometimes before any visible swelling appears, it is a condition most patients manage effectively with the right specialist support.
📊 Clinical Data Point: BCRL risk varies significantly by surgical approach — patients who undergo axillary lymph node dissection (ALND) carry a substantially higher lifetime risk than patients who receive sentinel lymph node biopsy (SLNB) alone. Your specific procedure type is the single most important risk variable in your individual prognosis.
For the clinical foundation connecting your breast cancer stage to your surgical approach and lymphedema risk, see our breast cancer stages and treatment overview.
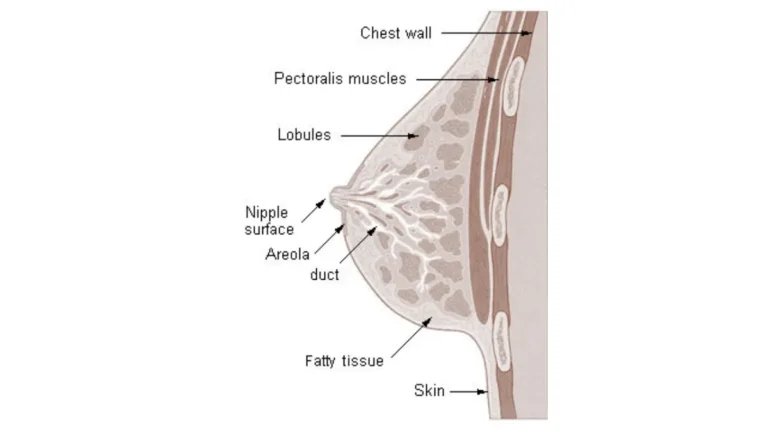
Why your lymphatic system matters after breast surgery
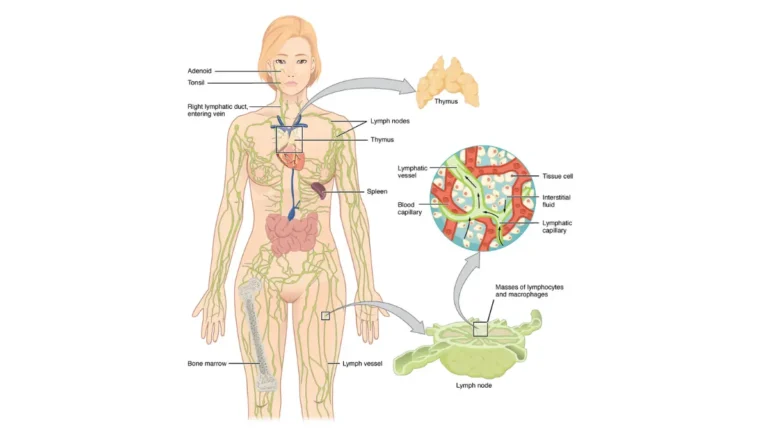
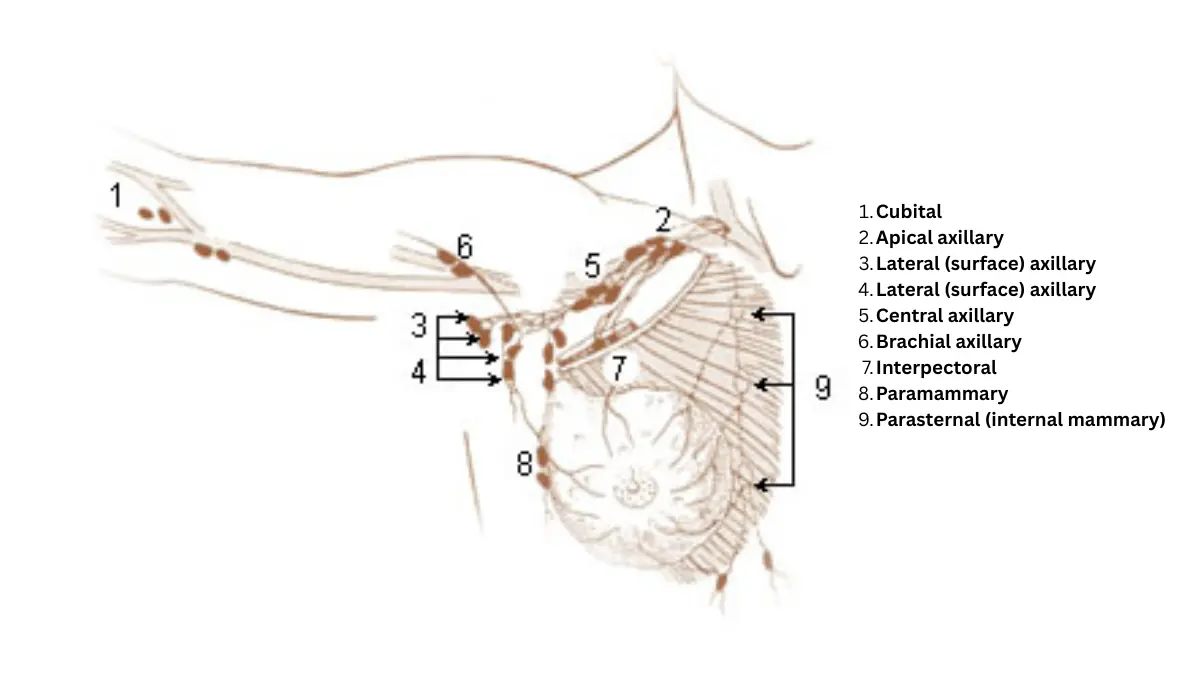
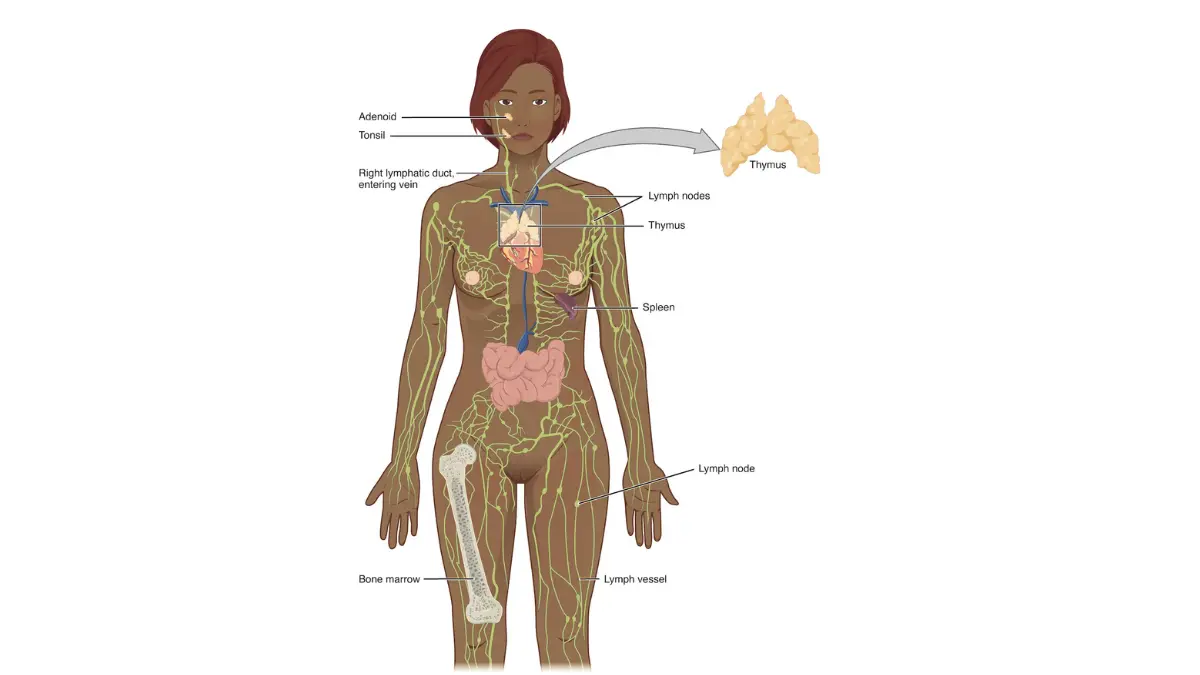
Your lymphatic system is a network of vessels and nodes that transports excess tissue fluid from the body back into circulation. When axillary lymph nodes are surgically removed, that drainage pathway is permanently altered in the treated region. Your remaining lymphatic vessels attempt to compensate, but they have finite capacity.
Who is most at risk and what this article covers
This article is written for patients who have had or are scheduled for a mastectomy or lumpectomy with axillary lymph node involvement, and for caregivers supporting them through recovery. Each section addresses the specific clinical question you are most likely to have at that point in your recovery journey.
ℹ️ Medical Disclaimer: The diagnostic criteria, staging classifications, treatment protocols, medication interactions, surgical procedure information, and insurance coverage details discussed in this article reflect current clinical guidelines as of May 2026 and are provided for educational purposes only. Individual diagnostic conclusions, treatment decisions, compression garment prescriptions, and surgical eligibility assessments depend on factors including patient history, comorbidities, lymph node pathology results, and specialist evaluation. Consult a board-certified gynecologic or surgical oncologist and a CLT-LANA–certified lymphedema therapist before acting on any clinical information in this article.
Why breast cancer surgery causes lymphedema
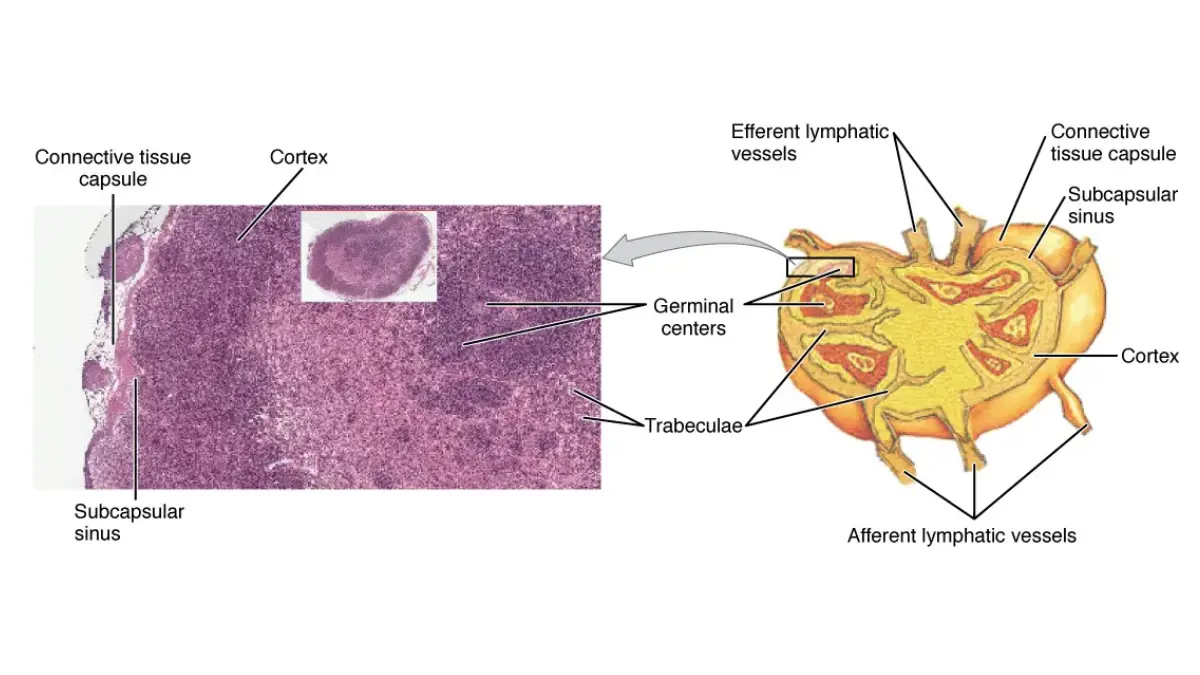
Lymph nodes are not simply passive filters — they are active transit stations in a fluid transport network. During axillary lymph node dissection, the surgical removal of nodes along the lymphatic drainage pathway creates a structural gap that cannot be naturally replaced. The lymphatic vessels that once drained into those nodes continue producing lymph fluid, but now have fewer routes to move it.
🔬 How It Works: Under normal anatomy, axillary lymph nodes collect lymph fluid from the arm, hand, and breast tissue and channel it into the thoracic duct for return to the bloodstream. When those nodes are removed, residual lymphatic vessels attempt to reroute drainage through collateral channels — but collateral capacity is limited. Over time, the interstitial space in the arm begins to accumulate the fluid those channels cannot clear, producing the chronic fluid overload that defines BCRL.
How lymph node removal disrupts normal drainage
The disruption is not immediate in most patients. In the weeks following surgery, post-operative inflammatory edema — a normal healing response — can temporarily mask early lymphedema signs. As inflammation resolves, the underlying lymphatic transport deficit becomes clinically detectable, often as a persistent heaviness or tightness before visible arm swelling begins.
🩺 Physician Note: “In my clinical experience, the intraoperative decision that most affects a patient’s lymphedema risk is one they are rarely told about afterward — whether the surgical team needed to clear additional axillary nodes beyond the sentinel node at the time of biopsy. A patient who went in expecting a sentinel node biopsy but ended up with a partial ALND based on intraoperative findings may have a substantially different risk profile than their preoperative counseling reflected. If you are unsure how many nodes were removed during your procedure, ask your surgeon’s office for the pathology report — it specifies the node count.” — Dr. Carolyn D. Fairweather, MD

ALND vs. SLNB: why your surgical approach changes your risk
The number of lymph nodes removed is the primary determinant of BCRL risk. Sentinel lymph node biopsy removes only the one to five sentinel nodes that drain the tumor site — the procedure least likely to disrupt the axillary drainage architecture. Axillary lymph node dissection removes the full axillary node bed — ten to twenty or more nodes — creating a far larger drainage disruption.
| Procedure | Nodes Removed | Estimated BCRL Lifetime Risk |
|---|---|---|
| Sentinel lymph node biopsy (SLNB) | 1–5 (sentinel nodes only) | ~5–7% |
| Axillary lymph node dissection (ALND) | 10–20+ (full axillary clearance) | ~20–40% |
Source: NCI lymphedema treatment overview
Axillary radiation following surgery adds an independent risk factor by inducing fibrosis in the remaining lymphatic vessels, further reducing their transport capacity. For a full comparison of how your surgical procedure affects your recovery trajectory, see our guide on lumpectomy versus mastectomy decisions and outcomes. Patients who had SLNB as part of their axillary staging can also review what that procedure involves in our sentinel lymph node biopsy guide.
📊 Clinical Data Point: Axillary radiation is an independent risk factor for BCRL, compounding the risk created by lymph node removal by inducing fibrosis in residual lymphatic vessels. Patients who received both ALND and axillary radiation represent the highest-risk group.
Signs your arm swelling might be lymphedema
When a patient calls my office weeks after surgery to describe an arm that feels “a little off,” the first thing I ask is not about the size of the arm. I ask whether they have noticed a heaviness, a tightness when fastening a watchband, or a sensation of fullness at the end of the day. Those early sensory signals — before any visible swelling — are the clinical window in which intervention produces the best long-term outcomes.
Early warning signs most patients overlook after breast cancer surgery
The most commonly missed early symptom of breast cancer-related lymphedema is not swelling at all. It is a persistent heaviness, warmth, or aching in the affected arm or hand that patients attribute to post-surgical soreness and never mention to their care team. Skin that feels firmer than usual over the back of the hand or the inner arm, or rings and watches that suddenly feel tighter without weight change, are also early indicators.
⚠️ Clinical Warning: Do not wait for your next scheduled appointment if you notice any of the following: one arm that is visibly larger than the other, pitting when you press a finger into the skin of your arm or hand, red streaking or warmth along the arm associated with fever, or swelling that does not resolve after 20 minutes of arm elevation. These findings require same-day or next-day contact with your breast cancer care team — not a monitoring-and-wait approach.
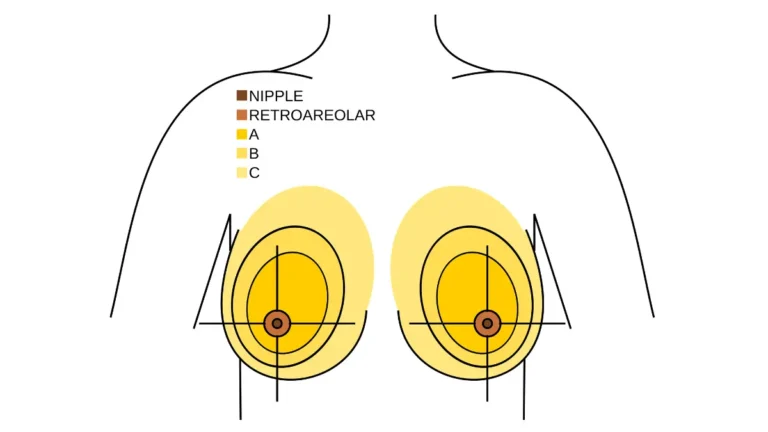
The arm circumference threshold that means call your care team
A circumference difference of 2 cm or more between your affected arm and your unaffected arm at any measuring point — or a limb volume increase of 200 mL or more compared to baseline — represents the clinical action threshold for reporting potential lymphedema. Your oncology care team should be measuring both arms at every follow-up visit. If they are not, ask specifically for a bilateral arm circumference measurement.
📊 Clinical Data Point: A 2 cm circumference difference or 200 mL limb volume increase triggers clinical lymphedema evaluation in most institutional protocols.The American Cancer Society’s lymphedema guide for breast cancer survivors provides patient-facing details on when swelling requires urgent care.
✅ Patient Action: Before your next appointment, document your symptoms using our symptom checker tool — record which arm is affected, when the heaviness or swelling began, whether it changes with position or time of day, and any recent triggers such as air travel, infection, or vigorous activity. A written symptom log gives your care team the clinical timeline they need to stage your lymphedema accurately and begin treatment at the earliest appropriate intervention point.
Axillary web syndrome (cording): the symptom many patients confuse with lymphedema
Axillary web syndrome, sometimes called cording, is a distinct post-surgical condition in which fibrous bands develop under the skin, running from the axilla toward the elbow or wrist. It feels like a tight cord pulling under the arm and is often visible as a raised line beneath the skin surface. Cording and lymphedema can coexist, but cording has a different management pathway — stretching, physical therapy, and in some cases scar mobilization — rather than the compression-and-drainage protocol used for lymphedema.
🩺 Physician Note: “Patients with cording frequently tell me they thought it was lymphedema and had been using compression inappropriately for weeks. Cording responds to guided stretching and physical therapy, and most cases resolve within weeks of appropriate treatment. Mismanaging cording with lymphedema protocols can delay resolution. If you feel a cord-like structure under your arm, ask your care team specifically whether this is cording or early lymphedema — they require different first-line management.” — Dr. Carolyn D. Fairweather, MD
✅ Patient Action: If you have noticed any arm swelling, heaviness, or skin changes that concern you, contact your breast surgical oncologist or breast cancer care navigator and request a formal referral to a board-certified lymphedema therapist with CLT-LANA certification. Do not wait for your next scheduled appointment — early intervention at Stage 0 or Stage I produces significantly better outcomes than delayed treatment at Stage II.
How doctors diagnose and stage lymphedema
Diagnosing breast cancer-related lymphedema follows a structured clinical pathway that most patients are not told about in advance. Knowing what each step measures — and what your results mean — allows you to ask the right questions at your specialist appointment rather than waiting passively to be told.
The four-step diagnostic pathway your care team should follow:
- Bilateral arm circumference measurement at multiple anatomical points — compares your affected arm to your unaffected arm and to your own pre-surgical baseline if one was established
- Bioimpedance spectroscopy — measures the electrical resistance of fluid in the affected limb to detect subclinical fluid changes before visible swelling appears
- L-Dex score interpretation — a standardized output from bioimpedance testing; a score at or above the clinical threshold indicates subclinical BCRL
- ISL staging classification — assigns your lymphedema to Stage 0, I, II, or III based on clinical examination findings, which determines your treatment protocol
The four-stage ISL classification your therapist will use
The International Society of Lymphology staging system is the globally recognized clinical framework for classifying lymphedema severity and directing treatment decisions.
| Stage | Clinical Features | First-Line Response |
|---|---|---|
| Stage 0 (Subclinical) | No visible swelling; abnormal bioimpedance L-Dex score; tissue heaviness | Immediate CLT-LANA referral; preventive CDT and compression |
| Stage I (Reversible) | Visible pitting swelling; resolves with arm elevation; no fibrosis | Urgent Phase 1 CDT; compression garment fitting |
| Stage II (Irreversible) | Non-pitting swelling; does not resolve with elevation; early fibrosis | Full CDT required; surgical consultation for LVA eligibility |
| Stage III (Lymphostatic Elephantiasis) | Severe fibrosis; skin changes; recurrent infections; significant limb enlargement | Intensive CDT and specialist surgical referral |
Source: International Society of Lymphology staging criteria
Bioimpedance spectroscopy: catching lymphedema before it becomes visible
Bioimpedance spectroscopy works by passing a low-level electrical current through the affected and unaffected limbs and measuring the resistance to flow. Because lymph fluid accumulates in the extracellular space before it creates visible swelling, the device detects early fluid changes before a patient or clinician can see or feel them.
🔬 How It Works: The device calculates an L-Dex score — a ratio of extracellular fluid resistance in the affected limb compared to the unaffected limb and the patient’s own pre-surgical baseline. A score at or above the clinically validated threshold (≥7.1 in current peer-reviewed literature indicates subclinical Stage 0 lymphedema. This is the diagnostic window in which treatment produces the most favorable long-term outcomes.
What your L-Dex score means and when it triggers treatment
An L-Dex score below the threshold means your fluid balance is currently within normal range. A score at or above the threshold means subclinical lymphedema is developing — even if your arm looks and feels completely normal. Patients who do not have a pre-surgical baseline measurement lose the most sensitive comparison point for this test.
📊 Clinical Data Point: The prospective surveillance model (PSM) — in which baseline bioimpedance is measured before surgery and monitored at each post-surgical follow-up — produces earlier detection of BCRL and better treatment response rates than the traditional symptom-triggered diagnostic approach. For patient-facing reference on lymphedema diagnosis and staging, see the MedlinePlus lymphedema reference for patients.
✅ Patient Action: Ask your breast surgical oncologist two specific questions at your next visit: (1) Was a pre-surgical bioimpedance baseline measurement taken before my procedure? (2) Is bioimpedance monitoring scheduled at my upcoming follow-up visits? If bioimpedance equipment is unavailable at your oncology center, ask for a referral to a CLT-LANA–certified lymphedema therapist who performs this assessment — early detection is the single most impactful intervention available.
Evidence-based treatment options for breast cancer lymphedema
Complete decongestive therapy (CDT) is the first-line treatment for lymphedema after breast cancer surgery, classified as a Category 1 recommendation in the NCCN Survivorship Guidelines. CDT is not a single treatment — it is a two-phase protocol delivered by a CLT-LANA–certified therapist that addresses both the acute fluid burden and the long-term maintenance requirement.
📊 Clinical Data Point: NCCN Survivorship Guidelines classify complete decongestive therapy as Category 1 for the management of breast cancer-related lymphedema. This is the highest level of clinical evidence designation, indicating both strong evidence quality and uniform NCCN expert panel consensus. Patients who accept a compression sleeve prescription as their complete treatment plan are receiving Phase 2 maintenance therapy without completing the Phase 1 intensive protocol that sets the long-term outcome trajectory.
Complete decongestive therapy: the gold standard first-line treatment
CDT is structured in two phases. Phase 1 (intensive) is a clinic-based program — typically two to four weeks of daily or near-daily sessions — combining manual lymphatic drainage, multilayer compression bandaging, therapeutic exercise, and meticulous skin care to reduce limb volume and prepare the tissue for long-term management. Phase 2 (maintenance) is a patient-self-administered lifelong program using compression garments, self-MLD, and ongoing skin care to preserve the gains achieved in Phase 1.
🩺 Physician Note: “The Phase 1 versus Phase 2 distinction is the most important clinical detail that patients who receive lymphedema diagnoses are rarely told. In my referral experience, a significant number of breast cancer patients who come to me years post-surgery have been wearing a compression sleeve since their initial diagnosis without ever having completed a Phase 1 intensive CDT course. Their lymphedema has often progressed to Stage II — not because CDT failed, but because only half of CDT was ever applied. If you have been given a compression sleeve without a formal Phase 1 referral, ask your oncologist specifically to evaluate whether a full CDT course is indicated.” — Dr. Carolyn D. Fairweather, MD
Pneumatic compression devices: when and how they are used
Pneumatic compression devices — pump systems that apply sequential compression to the arm through an inflatable sleeve — are used as an adjunct to CDT rather than as a standalone treatment. They help move lymph fluid from the periphery toward central drainage pathways during Phase 2 maintenance. The FDA has cleared several devices for home use in lymphedema management; a CLT-LANA therapist should evaluate whether a device prescription is appropriate for your specific stage and presentation.
For a comprehensive overview of post-treatment side effects that may accompany your breast cancer recovery alongside lymphedema, our guide to managing chemotherapy side effects in breast cancer addresses the full spectrum of physical sequelae. Our physical therapy overview explains how CDT fits within the broader physical rehabilitation landscape for cancer recovery.
Surgical options for lymphedema: who qualifies for LVA or VLNT
Lymphovenous anastomosis (LVA) and vascularized lymph node transfer (VLNT) are microsurgical procedures that create new drainage pathways for lymph fluid. LVA is most effective when performed at Stage 0 or Stage I — before significant fibrosis has altered tissue architecture — because early-stage tissue retains the pliability needed for anastomosis. VLNT involves transplanting healthy lymph nodes from a donor site to the axilla and is indicated for more advanced fibrotic cases. These are not first-line options; they are specialist-referred, staging-gated procedures considered when CDT has reached its management ceiling.
✅ Patient Action: Before accepting a prescription for a compression garment as your complete lymphedema management plan, ask your oncologist for a formal referral to a board-certified lymphedema therapist (CLT-LANA) and confirm whether your health plan covers a full Phase 1 CDT course under ICD-10 code I97.2. Patients interested in surgical lymphedema options can search for open lymphedema clinical trials on ClinicalTrials.gov to identify centers offering LVA or VLNT in investigational or expanded-access settings.
How to reduce your risk of lymphedema before and after breast surgery
The strongest evidence for reducing BCRL risk does not come from post-surgical precautions alone — it comes from a pre-surgical decision and a measurement taken before the first incision.
The prospective surveillance model (PSM) is a systematic approach in which bioimpedance baseline measurements are taken before surgery and repeated at every post-surgical follow-up visit. Published data from 2026 peer-reviewed studies consistently show that patients enrolled in a PSM program have earlier BCRL detection rates and significantly better treatment response at identification compared to patients diagnosed by symptom-triggered evaluation alone. Earlier detection means treatment begins at Stage 0 or Stage I — the window in which outcomes are most favorable.
Before surgery: why getting a baseline measurement changes everything
The pre-surgical bioimpedance baseline is the most impactful preventive step available to any patient before a scheduled breast cancer procedure — and it costs nothing beyond a clinical device reading. Without a pre-surgical baseline, post-surgical bioimpedance readings have only population norms as a comparison point. With a baseline, your care team has your personal pre-disease fluid ratio to detect even subtle increases that population averages would miss.
✅ Patient Action: Before your surgery date, ask your surgical oncologist two specific questions: (1) Am I a candidate for sentinel lymph node biopsy instead of axillary lymph node dissection — or has staging already determined that ALND is necessary? (2) Can a pre-surgical bioimpedance baseline measurement be taken at my pre-operative visit? These two steps are the most evidence-supported preventive actions available before your procedure. For a complete picture of what your mastectomy recovery involves beyond lymphedema, our guide to what your surgeon may not tell you about mastectomy covers the recovery factors most patients encounter unprepared.
After surgery: the precautions that reduce your lifetime lymphedema risk
The evidence-based post-surgical precautions for BCRL risk reduction are specific — not generic “be careful” advice. Avoid blood pressure cuffs, blood draws, and injections in the affected arm for life. Protect the arm from cuts, burns, and insect bites, as infection in a lymphedema-risk limb can trigger acute BCRL onset. Wear a well-fitted compression sleeve during air travel, which creates a low-pressure environment that promotes fluid accumulation in the arm.
Exercise, weight, and hydration: the modifiable risk factors that matter most
Current NCCN Survivorship Guidelines support progressive resistance exercise as a safe and beneficial component of lymphedema management — replacing older guidance to avoid upper-body exercise after axillary surgery. Begin with light resistance, wear your fitted compression garment during activity, and advance gradually under CLT-LANA guidance. Adequate hydration supports lymphatic flow — use our water intake calculator to determine a specific daily fluid target for your body weight and activity level. A BMI above 30 is an independent predictor of lymphedema progression; use our BMI calculator and discuss a realistic weight maintenance strategy with your care team if this applies to your situation.
📊 Clinical Data Point: Progressive resistance training in breast cancer survivors with lymphedema does not exacerbate BCRL severity and is associated with improved functional outcomes and quality of life in 2026 peer-reviewed literature. Unsupervised high-intensity upper-body exertion without a compression garment remains inadvisable regardless of current NCCN guidance on supervised programs.
What your doctor may not tell you about long-term lymphedema
Most clinical conversations about breast cancer-related lymphedema focus on what to do right after surgery. Far fewer address what happens to untreated or inadequately treated lymphedema over years — and the one infection complication that constitutes a life-threatening emergency requiring same-day emergency care, not a phone call to your care coordinator.
Why untreated lymphedema gets worse: the fibrosis progression timeline
Stage I lymphedema that is managed with compression alone — without completing a full Phase 1 CDT intensive course — can progress to Stage II through a process of progressive tissue fibrosis. This is not inflammation. It is a structural remodeling of the extracellular matrix in which fibrous tissue gradually replaces the pliable interstitial space, creating the non-pitting firmness characteristic of Stage II. Once fibrosis is established at Stage II, the eligibility criteria for microsurgical options such as lymphovenous anastomosis narrow significantly — because the tissue quality needed for successful anastomosis depends on a pre-fibrotic structural environment.
🩺 Physician Note: “I have seen patients present for a first lymphedema specialist consultation two years post-mastectomy with Stage II disease that was Stage I at their last oncology visit — not because their oncologist missed it, but because no one had referred them to a CLT-LANA therapist for a formal CDT course. The Stage I window is the most important intervention opportunity in the entire BCRL clinical arc. If you are currently at Stage I and have not completed Phase 1 CDT, please ask your oncologist for a CLT-LANA referral today — not at your next scheduled appointment.” — Dr. Carolyn D. Fairweather, MD
Breast cancer radiation to the axillary region is an additional fibrosis trigger that can accelerate this process in patients who received nodal irradiation. Our guide to breast cancer radiation therapy side effects covers the overlap between radiation-induced fibrosis and lymphedema risk in greater clinical detail.
Cellulitis and lymphangitis: the infection emergency that requires the ER
A lymphedema-affected arm has reduced immune surveillance capacity and is significantly more susceptible to bacterial skin infections. Cellulitis — a spreading bacterial skin infection — and lymphangitis — infection that spreads along the lymphatic channels themselves — are the two infections that can progress to septicemia within hours in a lymphedema patient.
⚠️ Clinical Warning: If you develop a fever above 100.4°F (38°C) combined with any of the following in your affected arm — redness, warmth, red streaking, or skin that looks inflamed and feels hot to the touch — go to the nearest emergency department immediately. Do not call your oncologist’s office and wait for a callback. Do not drive yourself if you already feel unwell. Lymphangitis can progress to sepsis within hours. This is a medical emergency.
The psychological weight of managing a chronic post-cancer condition is also a legitimate clinical concern. Asking your oncology care team for a referral to a licensed clinical social worker or breast cancer support group is not optional add-on care — it is a recognized component of comprehensive survivorship management.
Frequently asked questions about lymphedema after breast cancer surgery
1. What are the first signs of lymphedema after breast cancer surgery?
The earliest sign of lymphedema after breast cancer surgery is often sensory rather than visual — a persistent arm heaviness, tightness when fastening a watchband, or a feeling of fullness at the end of the day before any swelling is visible. A circumference difference of 2 cm or more in the affected arm compared to your unaffected side, or skin that pits when pressed and does not immediately refill, are the clinical thresholds requiring prompt care-team contact. Consult a board-certified lymphedema therapist (CLT-LANA) if these signs persist beyond 48 hours.
2. Can lymphedema from breast cancer go away on its own?
Lymphedema after breast cancer surgery rarely resolves without formal intervention. Stage 0 and Stage I BCRL — detected before significant fibrosis develops — can achieve meaningful improvement with a full complete decongestive therapy (CDT) program. Later stages involve irreversible tissue changes that require lifelong active management. The most important prognostic variable is how quickly formal treatment begins after the first clinical signs appear. Consult a board-certified lymphedema therapist (CLT-LANA) for staging and a personalized treatment plan.
3. How soon after surgery does lymphedema develop?
Lymphedema after breast cancer surgery can appear anywhere from weeks to years after the procedure. Some patients develop symptoms within the first three months; others notice changes two or more years post-surgery, often following a trigger such as infection, injury, air travel, or vigorous arm activity. This wide onset window is why bilateral arm circumference monitoring continues at every oncology follow-up appointment. Report any new arm swelling, firmness, or heaviness to your care team rather than waiting for your next scheduled visit.
4. What are the four stages of lymphedema?
The International Society of Lymphology defines four lymphedema stages. Stage 0 is subclinical — bioimpedance spectroscopy detects fluid changes before visible swelling appears. Stage I involves reversible pitting swelling that resolves with elevation. Stage II shows non-pitting swelling with early fibrosis that does not respond to elevation. Stage III presents with severe fibrosis, skin changes, and recurrent infection. Stages 0 and I respond best to complete decongestive therapy. Consult a board-certified lymphedema therapist (CLT-LANA) to confirm your current stage and treatment options.
5. What is the best treatment for lymphedema after breast cancer surgery?
Complete decongestive therapy (CDT) is the first-line treatment for lymphedema after breast cancer surgery, classified Category 1 by the NCCN Survivorship Guidelines. CDT combines an intensive clinic-based phase — manual lymphatic drainage, multilayer compression bandaging, exercise, and skin care — followed by lifelong maintenance compression and self-drainage. A compression sleeve alone without completing the intensive CDT phase is not complete treatment. Consult a board-certified lymphedema therapist (CLT-LANA) to begin a formally staged CDT program.
6. Does everyone who has breast cancer surgery develop lymphedema?
Not all breast cancer surgery patients develop lymphedema. Risk depends primarily on the number of lymph nodes removed and whether axillary radiation was part of the treatment plan. Axillary lymph node dissection (ALND) carries significantly higher lifetime risk than sentinel lymph node biopsy (SLNB). Additional risk factors include BMI above 30 and post-surgical infection. Ask your surgical oncologist specifically what your procedure-based risk level is and what surveillance protocol your care team recommends for your specific case.
7. How long do I need to wear a compression sleeve after breast cancer surgery?
There is no fixed endpoint for compression garment use following lymphedema treatment after breast cancer surgery. Patients with confirmed BCRL typically require lifelong compression precautions — particularly during air travel, vigorous exercise, and repetitive arm activities. Garment specifications, including compression class and fit, are reassessed at each lymphedema therapy visit as limb volume changes over time. Consult a board-certified lymphedema therapist (CLT-LANA) before reducing or discontinuing your compression garment regimen — unsupervised changes in compression often lead to volume rebound.
8. Can lymphedema get worse over time if I do not treat it?
Lymphedema after breast cancer surgery can worsen without adequate treatment. Stage I BCRL can advance to Stage II as progressive fibrosis permanently alters tissue structure — a change that reduces eligibility for surgical options such as lymphovenous anastomosis. Complete decongestive therapy (CDT) remains beneficial at Stage II for symptom management, but it cannot reverse established fibrosis. Beginning treatment at Stage 0 or Stage I produces measurably better long-term outcomes than initiating treatment at Stage II or later.
9. What exercises are safe with breast cancer-related lymphedema?
Exercise is safe and beneficial for patients managing lymphedema after breast cancer surgery. Current NCCN Survivorship Guidelines support progressive resistance training as a recommended management component — correcting older guidance to avoid upper-body exercise after axillary surgery. Begin with light resistance while wearing a fitted compression garment and advance gradually over weeks. Consult a board-certified lymphedema therapist (CLT-LANA) before beginning any new exercise program to ensure the intensity level and garment fit are appropriate for your current ISL stage.
10. Is lymphedema treatment covered by insurance or Medicare after breast cancer surgery?
Many lymphedema treatments following breast cancer surgery are covered by insurance. Medicare Part B covers manual lymphatic drainage and compression garments when lymphedema is documented with ICD-10 code I97.2 and physician-prescribed. Some plans require prior authorization for pneumatic compression pump devices. Confirm coverage specifics with your insurer before beginning complete decongestive therapy (CDT), and ask your oncology care coordinator to provide the diagnosis code and formal prescription documentation your plan requires to approve coverage.
11. What is a certified lymphedema therapist and how do I find one?
A board-certified lymphedema therapist with CLT-LANA certification has completed specialized clinical training in complete decongestive therapy and passed a standardized national examination. Not all physical or occupational therapists hold this credential — CLT-LANA specifically indicates formal training in manual lymphatic drainage, compression bandaging, and lymphedema staging for breast cancer-related presentations. Ask your breast surgical oncologist for a direct referral, or contact the Lymphatic Education and Research Network to locate a CLT-LANA–certified provider in your geographic area.
Your next step starts with one conversation with your care team
Breast cancer-related lymphedema is not a condition you have to accept without a management plan. The clinical evidence is unambiguous: early detection — at Stage 0 or Stage I, before fibrosis alters tissue architecture — produces dramatically better long-term outcomes than treatment initiated after visible progression.
The single most impactful step available to you right now, regardless of where you are in your recovery, is to ask your oncologist for a referral to a board-certified lymphedema therapist with CLT-LANA certification. Do not accept a compression sleeve prescription as a complete answer if you have not completed a Phase 1 CDT intensive course.
If you are not yet certain whether what you are experiencing qualifies as lymphedema, document your symptoms in our free symptom checker tool and bring that written log to your next appointment. Your care team can act on a structured symptom record far more efficiently than a verbal description reconstructed from memory.
Stay informed. Sign up for physician-reviewed updates from the mymedicineadvisor.com advisory board.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.