On This Page – Quick Medical Summary
What breast cancer recurrence really means — and what to do right now
Breast cancer recurrence is not a single outcome. It covers three clinically distinct situations — each with a different prognosis, a different treatment plan, and a very different meaning for your life right now.
Not all recurrences are equal. Local recurrence, when cancer returns near the original tumor site, is frequently treated with curative intent. That distinction matters, and this article explains it.
If you are experiencing any new or unexplained symptom after breast cancer treatment, contact your oncologist immediately — do not wait for your next scheduled appointment.
ℹ️ Medical Disclaimer: The diagnostic criteria, treatment options, medication information, and surgical procedures discussed in this article reflect current clinical guidelines and are provided for educational purposes only. Individual diagnostic conclusions, treatment decisions, and medication choices depend on factors including patient history, comorbidities, receptor status, imaging findings, and specialist assessment. Consult a board-certified gynecologic oncologist or medical oncologist before acting on any clinical information in this article. This content does not constitute a diagnosis or a treatment recommendation for any individual patient.
The three types of breast cancer recurrence — and why the difference matters
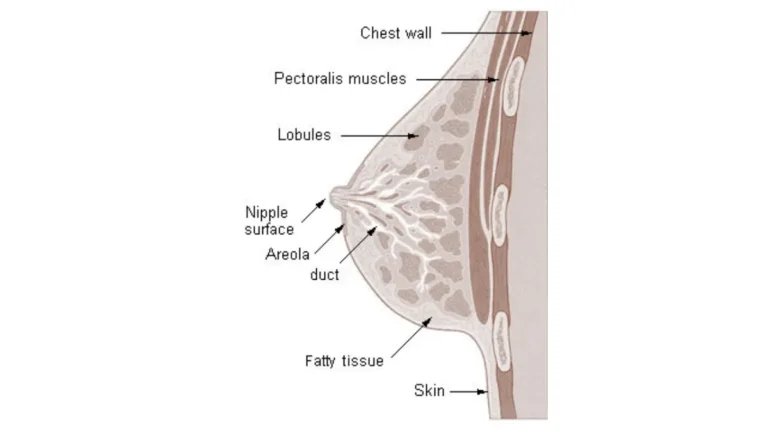
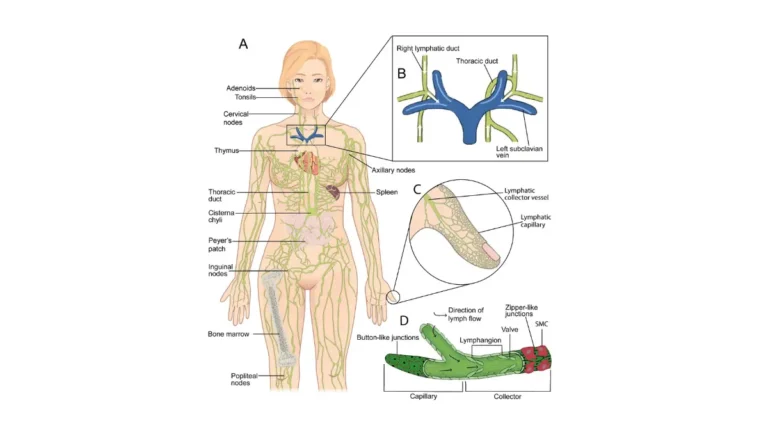
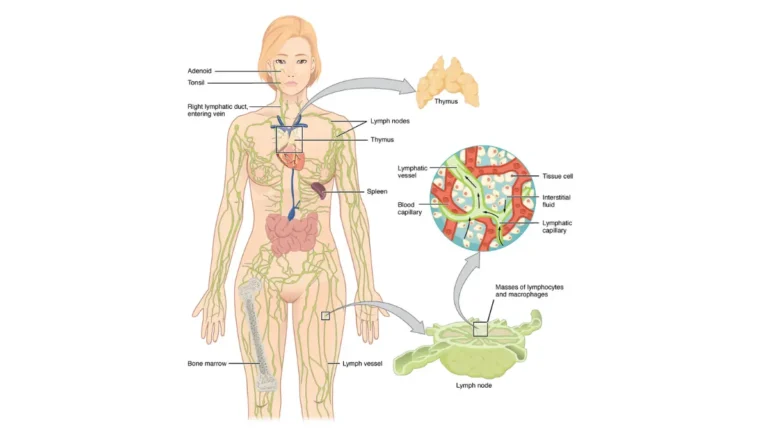
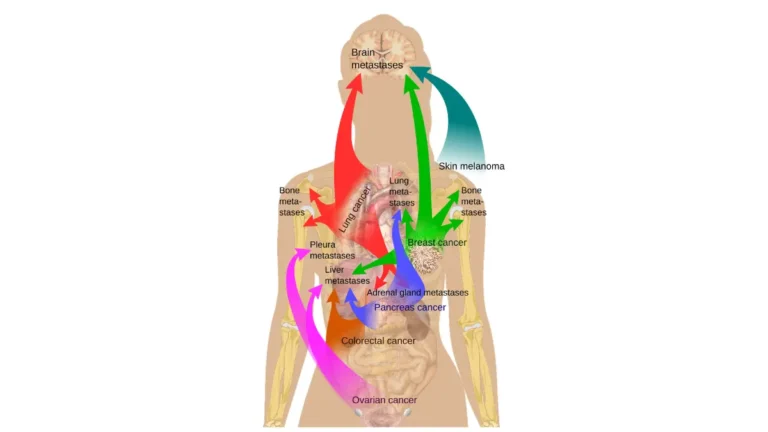
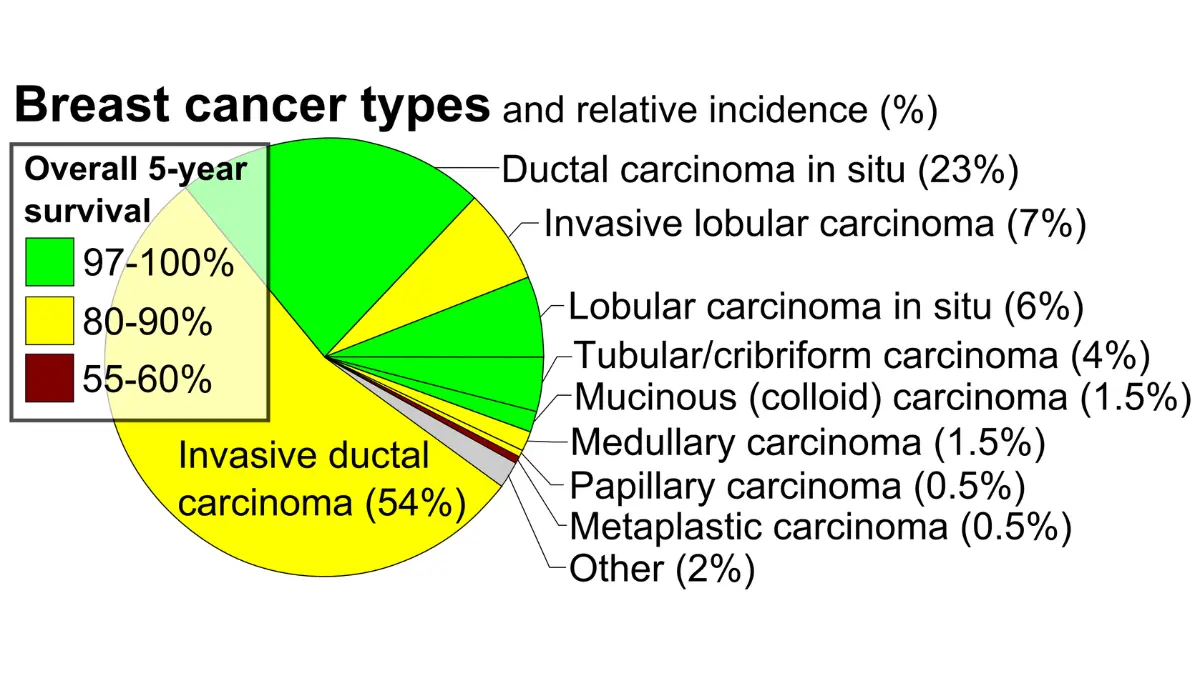
Local breast cancer recurrence means cancer has returned to the breast tissue, chest wall, or skin near the original tumor site. Regional recurrence means cancer cells have reached the lymph nodes under the arm or near the collarbone. Distant recurrence — also called metastatic breast cancer — means cancer has spread through the bloodstream or lymph system to organs including the bones, lungs, liver, or brain. Each type carries a meaningfully different prognosis and requires a different treatment approach.
Local recurrence: cancer returns to the breast or chest wall
Local recurrence is the most treatable form. Surgery, radiation, or a combination of both is often used with curative intent. It is not a metastatic diagnosis, and patients should not assume the worst when this type is confirmed.
Regional recurrence: cancer returns to nearby lymph nodes
Regional recurrence means cancer has moved beyond the breast but has not yet reached distant organs. Systemic therapy is typically added to locoregional treatment to prevent progression to distant sites.
Distant recurrence: cancer spreads to bones, lungs, liver, or brain
Distant recurrence constitutes a stage IV diagnosis. The bones are the most common first site of distant recurrence in breast cancer, followed by the lungs, liver, and brain. Treatment shifts to systemic therapy with the goal of long-term disease control rather than cure.
Why your receptor status at recurrence may be different than before
This is the detail most patients do not expect. The hormone receptor and HER2 status of a recurrent tumor — confirmed by new biopsy — may differ from the original tumor. Clonal selection under prior endocrine or chemotherapy pressure can shift the tumor’s biological profile. Your oncologist must test the recurrent tissue directly; the original receptor profile cannot be assumed.
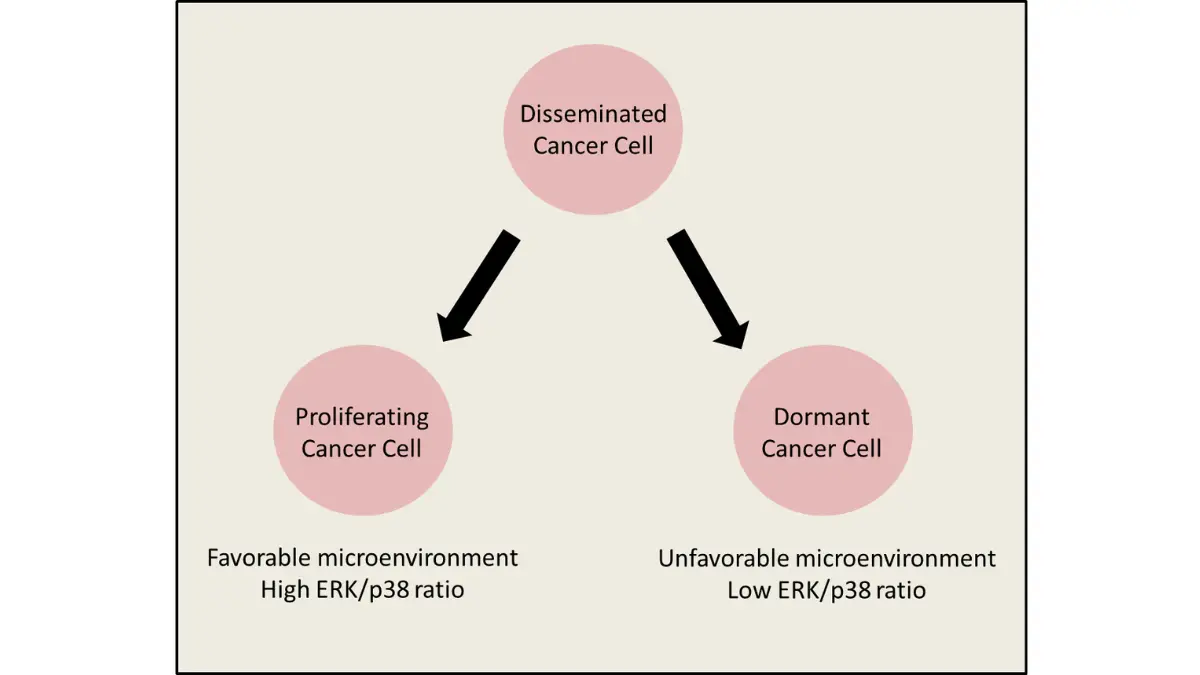
🔬 How It Works: When breast cancer cells are exposed to endocrine therapy over months or years, cells that do not depend on estrogen for growth are more likely to survive and proliferate. This is why an ER-positive primary tumor can recur as ER-negative — and why treatment for the recurrence may look completely different from the treatment that worked the first time.
Understanding how your original cancer was staged helps explain your current recurrence risk — review our complete guide to breast cancer stages and survival to see how stage at diagnosis affects future recurrence probability.
If you carry a BRCA1 or BRCA2 mutation identified at original diagnosis, your recurrence risk profile differs from the general breast cancer population — use our Genetic Risk Assessment Tool to understand how hereditary factors affect your monitoring plan.
📊 Clinical Data Point: The American Cancer Society advises that hormone receptor and HER2 status at the time of recurrence — not at the time of original diagnosis — is the primary determinant of recurrence treatment selection.
✅ Patient Action: If you have received a recurrence diagnosis, ask your oncologist specifically: “Will you perform a new biopsy of the recurrent tissue to confirm current receptor status before treatment begins?” If a new biopsy has not been discussed, request that conversation. Treatment selected without current receptor profiling may not be appropriate for your recurrent tumor.
Warning signs that breast cancer may have come back
The most important thing to understand about recurrence warning signs is this: some symptoms that belong on this list are easy to dismiss. Bone aches, fatigue, and chest tightness are also common side effects of aromatase inhibitors and radiation recovery. Knowing the difference — and knowing when the threshold has been crossed — is where this section focuses.
Local recurrence warning signs: new lumps, skin changes, and chest wall symptoms
- A new lump or thickening at the scar site, in the remaining breast tissue, or on the chest wall — even if it does not hurt
- Skin changes near the original tumor site: redness, dimpling, thickening, or a rash that does not resolve within two weeks
- A new lump in the armpit on the same side as the original tumor
Regional recurrence warning signs: new lumps near the arm or collarbone
- A new lump or swelling under the arm (axilla) that was not present before
- Swelling or a new fullness near the collarbone on the treated side
- Persistent arm heaviness or swelling that is new or worsening
Distant recurrence warning signs: bone pain, shortness of breath, and neurological symptoms
- Persistent bone pain — especially in the spine, hips, or ribs — that does not improve within two to three weeks and is not explained by a recent injury
- Shortness of breath at rest or with minimal exertion, or a new cough that does not resolve
- Unexplained weight loss of more than 5% of body weight over four to six weeks
- Jaundice, upper right abdominal pain, or new abdominal bloating
- Headaches, new vision changes, confusion, or weakness in an arm or leg
The difference between aromatase inhibitor side effects and true recurrence symptoms
🩺 Physician Note: In my practice, the most common reason patients delay reporting a potential recurrence is that they attribute bone pain to their aromatase inhibitor. Joint aches and bone discomfort are real side effects of agents like anastrozole and letrozole. But the key clinical distinction I use with my patients is this: aromatase inhibitor side effects tend to be bilateral, symmetrical, and present across multiple joints simultaneously. True bone metastasis pain is typically localized, unilateral, progressive, and not relieved by changing position or activity. If your bone pain is focused in one area, worsening over weeks, and does not follow the pattern of your usual joint aches — report it immediately.
When to call your oncologist the same day — and when to go to the emergency room
⚠️ Clinical Warning: Go to the nearest emergency room immediately if you experience sudden severe headache, new vision changes, sudden confusion, arm or leg weakness, or a seizure. These are neurological emergency symptoms that require urgent evaluation — in a breast cancer patient, they can indicate brain metastasis and cannot wait for an office appointment. Do not call your oncologist first. Go to the ER.
Contact your oncologist within 24 hours for any new lump, persistent unexplained bone pain, new shortness of breath, or weight loss that does not have an obvious explanation. These symptoms do not constitute an overreaction. Early reporting consistently expands available treatment options.
If you are unsure whether a new symptom warrants an immediate call, use our Symptom Checker as a first-step self-assessment — then call your oncologist regardless of the result if your concern persists.
Some of the early warning signals that appear after treatment overlap with the original breast cancer warning signs — particularly new lumps and skin changes — and should be evaluated the same way.
How doctors diagnose breast cancer recurrence — step by step
Diagnosing breast cancer recurrence requires a structured clinical and imaging evaluation — and one step that surprises many patients: a biopsy is required even when imaging results strongly suggest recurrence. Your oncologist will typically follow these five steps.
Step 1: Clinical exam and symptom history
Your oncologist will review your complete symptom history — when it started, how it has changed, and how it compares to prior side effects. A physical examination assesses any new lumps, skin changes, lymph node enlargement, or signs of organ involvement.
Step 2: Imaging — which scans are ordered and why
The imaging ordered depends on your symptoms. A PET-CT scan provides whole-body metabolic imaging to identify active disease at any site. Bone scan is used when skeletal pain is the primary symptom. MRI is preferred for brain or spinal evaluation. Mammogram remains part of the workup when local recurrence in residual breast tissue is suspected.
Step 3: Tumor marker blood tests — what they do and do not tell you
CA 15-3 and CA 27.29 are the two tumor markers most commonly used in breast cancer surveillance. Elevated levels support a clinical suspicion of recurrence but do not confirm it. These markers are used to monitor treatment response once recurrence is confirmed — not to establish the diagnosis on their own.
🔬 How It Works: Tumor markers are proteins shed by cancer cells into the bloodstream. Their levels can rise from many causes, and they can remain normal even when recurrence is present. A rising marker with stable imaging — or a stable marker with suspicious imaging — both require biopsy to resolve. Neither result overrules the other.
Step 4: Biopsy confirmation — why it is required even when imaging is definitive
Biopsy of the recurrent tissue is the clinical standard of care. Imaging cannot replace it. The reason is critical: receptor status may have changed since original diagnosis, and treatment selection for the recurrence depends on the receptor profile of the current tumor — not the original one.
📊 Clinical Data Point: Per current clinical standards supported by the National Cancer Institute, biopsy confirmation of recurrent tissue is required before any treatment decision for recurrent breast cancer.
Step 5: Receptor status testing on the new biopsy tissue
The biopsy specimen is tested for ER, PR, and HER2 status. Results from this new pathology report — not the original diagnosis report — determine which treatment regimen your oncologist will recommend.
✅ Patient Action: Before proceeding with any treatment for suspected recurrence, ask your oncologist two specific questions: “Has biopsy confirmed the recurrence?” and “Has receptor status been tested on the new tissue sample?” Both confirmations must precede treatment. A recurrence diagnosis based on imaging alone, without biopsy, is incomplete.
Treatment options for recurrent breast cancer — matched to your recurrence type
Treatment for recurrent breast cancer is determined first by recurrence type — local, regional, or distant — and then by the receptor profile confirmed on the new biopsy. The regimen that treated your original cancer may not be the right choice now. The following breakdown follows the framework supported by NCCN clinical guidelines for recurrent breast cancer, updated in 2026.
Local and regional recurrence: surgery, radiation, and systemic therapy
Local recurrence after lumpectomy is typically managed with mastectomy when feasible, followed by systemic therapy to reduce the risk of distant spread. Local recurrence after prior mastectomy requires radiation and systemic therapy. Our guide to lumpectomy vs. mastectomy explains the surgical considerations in detail.
Hormone receptor-positive (ER+/PR+) distant recurrence: CDK4/6 inhibitors and endocrine therapy
The current standard first-line approach for ER+/HER2-negative distant recurrence combines a CDK4/6 inhibitor — palbociclib (Ibrance), ribociclib (Kisqali), or abemaciclib (Verzenio) — with an aromatase inhibitor or fulvestrant, depending on prior endocrine therapy history. These are oral agents that have demonstrated significant progression-free survival benefit over endocrine therapy alone. Our comparison of tamoxifen vs. aromatase inhibitors covers the endocrine therapy landscape in full.
📊 Clinical Data Point: CDK4/6 inhibitors including palbociclib, ribociclib, and abemaciclib are FDA-approved treatments for hormone receptor-positive, HER2-negative advanced and metastatic breast cancer. Abemaciclib carries an additional FDA approval for early-stage high-risk HR+ breast cancer adjuvant therapy.
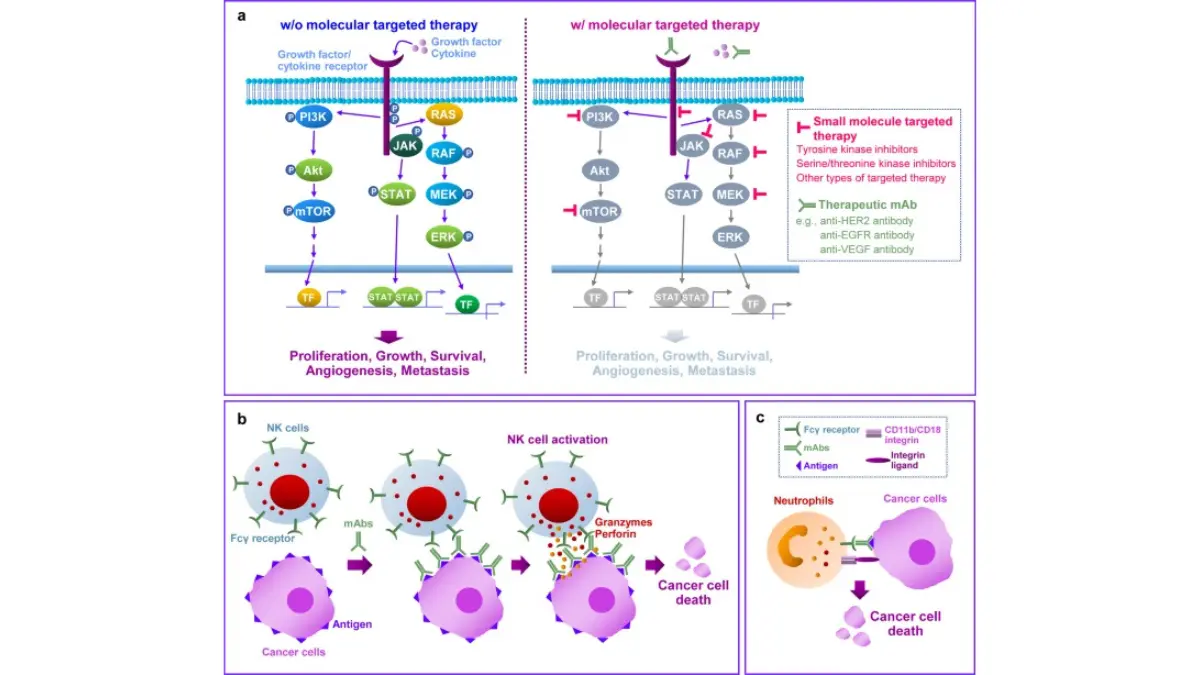
HER2-positive distant recurrence: trastuzumab, pertuzumab, and antibody-drug conjugates
HER2-positive distant recurrence is treated with HER2-targeted combination regimens. First-line therapy for most patients involves trastuzumab-based combinations or trastuzumab deruxtecan (Enhertu). Our dedicated guide to HER2-positive breast cancer explains the current targeted therapy landscape. Selection among agents depends on prior HER2-targeted treatment history, organ function, and NCCN recommendation level for your specific clinical scenario.
Triple-negative distant recurrence: chemotherapy, immunotherapy, and sacituzumab govitecan
Triple-negative breast cancer recurrence has fewer targeted options but several FDA-approved systemic choices. Sacituzumab govitecan (Trodelvy) is an antibody-drug conjugate approved for metastatic triple-negative breast cancer and HR+/HER2-low disease. Immunotherapy-chemotherapy combinations are indicated in PD-L1-positive triple-negative recurrence. Our full guide to triple-negative breast cancer covers the current treatment options and clinical trial landscape. Clinical trial eligibility should be discussed at every recurrence appointment for this subtype.
What “second-line” treatment means — and how NCCN guidelines determine your next step
Second-line therapy refers to the regimen used when first-line treatment stops controlling the disease. This is not treatment failure — it is a predictable part of managing recurrent breast cancer as a chronic condition. Current NCCN clinical guidelines for recurrent and metastatic breast cancer are updated to reflect new FDA approvals and define the evidence-based sequence for each receptor subtype. For patients requiring systemic chemotherapy at any recurrence stage, our detailed guide to breast cancer chemotherapy explains the agents used and what to expect.
✅ Patient Action: Treatment selection for recurrent breast cancer must be made by a board-certified oncologist using your biopsy-confirmed receptor status, prior treatment history, organ function, and current performance status. Ask your oncologist specifically: “Which 2026 NCCN guideline-recommended regimen applies to my recurrence subtype, and what is the planned second-line option if the first stops working?”
Survival rates for recurrent breast cancer — what the data actually shows
Survival statistics for recurrent breast cancer vary significantly by recurrence type, receptor status, and the treatment era in which you are diagnosed. The numbers below represent population-level data — not individual predictions — and must be interpreted with that context intact.
Local recurrence survival rates — what the numbers mean for you
Local-only recurrence carries a substantially more favorable prognosis than distant recurrence. Patients with confirmed local recurrence who are treated with surgery, radiation, and appropriate systemic therapy have 5-year relative survival rates that are meaningfully higher than those with distant spread.
Distant recurrence survival rates — and why they are improving
Distant recurrence survival rates have improved meaningfully with the introduction of CDK4/6 inhibitors, antibody-drug conjugates, and next-generation HER2-targeted agents over the past decade. Patients treated in 2026 with these agents have access to options that did not exist five years ago. That improving trajectory is clinically significant — historical figures from earlier years underestimate the current prognosis for many patients.
📊 Clinical Data Point: The NCI SEER database is the standard reference for US breast cancer survival statistics by recurrence type and stage. All survival figures in this article reflect 2026 NCI data.
Why your individual prognosis differs from the population average
Receptor status, response to first-line therapy, organ function, access to clinical trials, and overall health all modify individual prognosis significantly. A population average is the starting point — not the answer — for understanding your personal outlook. Our dedicated guide to breast cancer survival rates by stage and subtype provides the full statistical framework with clinical context.
What percentage of breast cancer survivors experience recurrence — and when
Recurrence risk is highest in the first three years for hormone receptor-negative breast cancer. For hormone receptor-positive breast cancer, the risk is lower early but persists — and remains clinically meaningful — beyond ten years from original diagnosis. This is why annual follow-up appointments and surveillance imaging remain important indefinitely, not just in the first five years after treatment.
Patients with recurrent breast cancer who have progressed on standard therapies may be eligible for active clinical trials evaluating next-generation targeted agents and immunotherapy combinations. Trial eligibility should be discussed at every recurrence appointment regardless of current treatment line.
Our guide to metastatic breast cancer treatment covers the full clinical management framework for patients with distant recurrence.
✅ Patient Action: Survival rate statistics are population-level data. Ask your board-certified oncologist: “Given my specific receptor status, prior treatment history, and current organ function, what does my individual prognosis look like — and how does clinical trial access affect that picture?”
What your oncologist wants you to know about breast cancer recurrence
The question every patient asks when they hear the word “recurrence” is some version of: Is this the end? I will give you the honest clinical answer. For local recurrence — no, and often not by a significant margin. For distant recurrence, the honest answer is more complex: it is serious, it requires aggressive and sustained treatment, but it is also a clinical situation in which meaningful life with treatment is the reality for many patients, not a rare exception.
The question every patient asks — and what the honest clinical answer is
A recurrence diagnosis is not the same diagnosis you received the first time. The biology may have changed. The treatment options have expanded. The landscape in 2026 is not the landscape of five or ten years ago. The patients who navigate recurrence most effectively are those who arrive at their appointment having already written down their symptoms, their questions, and the names of the specific tests they want discussed.
Why a recurrence diagnosis is the beginning of a new treatment plan, not the end
Your oncologist is not starting over — they are adapting a treatment strategy to a changed clinical situation. That is what oncology is. Every person on my advisory board approaches recurrence as a new clinical problem with a specific solution, not as a failed outcome.
If you carry a BRCA1 or BRCA2 mutation, your recurrence management also involves genetic counseling — our guide to understanding a positive BRCA gene test result explains what that conversation looks like.
What to bring to your next oncology appointment
Bring a written symptom log with dates, duration, and a description of each symptom. Bring a list of five specific questions — at minimum: (1) Has recurrence been confirmed by biopsy? (2) What is the current receptor status? (3) Which NCCN 2026 guideline-recommended regimen applies to my subtype? (4) Am I eligible for a clinical trial? (5) What is the second-line plan? Bring a caregiver or trusted person to help you retain what is said.
🩺 Physician Note: In my experience, no symptom report to your oncologist is ever an overreaction. The clinical cost of reporting a symptom that turns out to be benign is a reassuring phone call. The clinical cost of not reporting a symptom that was early recurrence is a delayed diagnosis. Report everything. Let us sort it out.
If you are an older patient or are managing treatment-related fatigue or peripheral neuropathy, a medical alert device provides both safety and peace of mind for family caregivers monitoring your daily wellbeing during active systemic treatment.
✅ Patient Action: If you have any concern — however small — that your breast cancer may have returned, contact your oncologist the same day. Do not wait for your next scheduled appointment. Early evaluation consistently expands available treatment options.
Frequently asked questions about breast cancer recurrence
1. Can breast cancer come back after I finished treatment?
Yes. Breast cancer recurrence can occur at any point after treatment — even years after completing chemotherapy, radiation, or hormone therapy. Hormone receptor-positive breast cancer carries a persistent recurrence risk that extends well beyond the first five years. Annual surveillance appointments and imaging remain important indefinitely. Contact your oncologist promptly if you notice any new or unexplained symptoms between scheduled visits. Consult a board-certified oncologist about your personal recurrence risk timeline.
2. How soon after treatment can breast cancer come back?
Recurrence timing depends primarily on receptor status. Hormone receptor-negative tumors carry the highest risk in the first one to three years after treatment. Hormone receptor-positive cancers present a lower early risk but a sustained long-term risk — some recurrences occur ten, fifteen, or even twenty years after original diagnosis. This extended risk is the reason lifelong follow-up is recommended. Consult a board-certified oncologist to understand your individual recurrence timeline risk.
3. What are the survival rates for recurrent breast cancer?
Survival rates for recurrent breast cancer vary significantly by type. Local recurrence treated with surgery and systemic therapy carries a substantially more favorable 5-year survival rate than distant recurrence. Distant recurrence survival has improved meaningfully with CDK4/6 inhibitors and antibody-drug conjugates. Population survival statistics do not predict individual outcomes — receptor status, treatment response, and trial access all modify the picture. Consult a board-certified oncologist for prognosis specific to your recurrence subtype.
4. Can breast cancer recurrence be cured?
Local breast cancer recurrence is often treated with curative intent — the clinical goal is complete elimination of the recurrent disease. Distant recurrence is currently managed as a chronic condition in most patients; cure is rarely achieved, but prolonged disease control with maintained quality of life is a realistic goal with modern systemic therapies. Individual outcomes depend on receptor status, prior treatment history, and response to therapy. Consult a board-certified oncologist about your specific treatment goals.
5. What are the treatment options for recurrent breast cancer?
Treatment is matched to recurrence type and receptor status confirmed by new biopsy. ER-positive distant recurrence is typically treated with a CDK4/6 inhibitor — palbociclib, ribociclib, or abemaciclib — combined with an aromatase inhibitor or fulvestrant. HER2-positive recurrence uses trastuzumab-based or trastuzumab deruxtecan regimens. Triple-negative recurrence may use sacituzumab govitecan (Trodelvy) or chemotherapy with immunotherapy. Consult a board-certified oncologist to identify the NCCN guideline-recommended first-line regimen for your subtype.
6. How is recurrent breast cancer diagnosed?
Diagnosing breast cancer recurrence requires imaging — PET-CT, bone scan, or MRI depending on symptoms — followed by biopsy confirmation. Biopsy is required even when imaging is strongly suggestive because receptor status may have changed since original diagnosis, and treatment selection depends on the current profile. Tumor marker tests such as CA 15-3 support surveillance but do not confirm recurrence alone. Consult a board-certified oncologist to direct the diagnostic workup based on your specific symptom presentation.
7. What percentage of breast cancer survivors experience recurrence?
Recurrence rates vary by original stage, tumor subtype, and treatment received. Hormone receptor-negative breast cancer carries a higher early recurrence risk. Hormone receptor-positive cancer carries a lower short-term but sustained long-term risk. No single population percentage applies to every patient — your individual risk depends on your original tumor characteristics, the treatment you received, and how long you have been in remission. Consult a board-certified oncologist for your personal recurrence probability estimate.
8. Does recurrent breast cancer spread faster than the original tumor?
The aggressiveness of recurrent breast cancer depends on its receptor status at recurrence — not necessarily the original tumor profile. Triple-negative recurrence tends to progress more rapidly than hormone receptor-positive recurrence. CDK4/6 inhibitors significantly slow progression in ER-positive metastatic disease. Receptor status may change at recurrence due to clonal selection, which is why a new biopsy is required. Consult a board-certified oncologist to assess the biological behavior of your specific recurrent tumor.
9. What questions should I ask my oncologist about breast cancer recurrence?
At a recurrence evaluation appointment, ask: (1) Has biopsy confirmed the recurrence with current receptor status? (2) Which 2026 NCCN guideline-recommended treatment applies to my recurrence subtype? (3) What are the second-line options if first-line therapy stops working? (4) Am I eligible for any active clinical trials? (5) What follow-up schedule do you recommend going forward? Preparing these questions before the appointment significantly improves the clinical information you receive and take home.
10. Is a new lump after breast cancer treatment always recurrence?
No. Not all new lumps following breast cancer treatment are recurrences. Fat necrosis, scar tissue changes, seroma, and benign cysts can produce lumps that clinically and radiologically resemble recurrence. Biopsy is the only way to confirm or rule out a recurrence diagnosis definitively. Never assume a new lump is benign without clinical evaluation, and never assume it is malignant without pathology confirmation. Consult a board-certified oncologist or breast surgeon — do not wait for a scheduled follow-up.
11. Does breast cancer recurrence mean it is stage 4?
No. Breast cancer recurrence is not automatically a stage 4 diagnosis. Local recurrence — cancer returning to the breast, chest wall, or skin near the original site — is not metastatic and is not classified as stage IV. Regional recurrence to nearby lymph nodes is also not automatically stage IV. Distant recurrence, when cancer spreads to organs such as the bones, lungs, or liver, does constitute a stage IV metastatic diagnosis. Ask your oncologist specifically how your recurrence is classified and what that means for your treatment pathway.
What to do next if you think breast cancer may have come back
If you are experiencing symptoms consistent with recurrence — a new lump, persistent bone pain, unexplained shortness of breath — contact your oncologist today. Not tomorrow. Today.
If your cancer has been confirmed as returned, this article is your preparation tool for the next appointment, not a substitute for it. Bring your symptom log. Write your questions. Know your receptor subtype. Know which treatment the NCCN 2026 guidelines recommend for that subtype.
Local recurrence and distant recurrence are not the same diagnosis, do not carry the same prognosis, and do not require the same treatment. That distinction — understanding where the cancer has returned and what the new biopsy shows — is the foundation of every decision that follows.
Your oncologist is not starting over. They are adapting. And in 2026, the tools available for that adaptation are more powerful than they have ever been.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.