On This Page – Quick Medical Summary
You got a dense breast letter — here’s what it actually means
The call I receive most often in my gynecologic oncology practice starts the same way. A woman reads me a phrase from her mammogram results letter — usually “heterogeneously dense” or “extremely dense” — and asks, quietly, whether she should be frightened.
The honest answer is: not immediately. But you deserve more than reassurance. You deserve a precise explanation of what those words mean clinically, how much they affect your actual cancer risk, and the exact steps to take before your next appointment.
Dense breast tissue cancer risk is real, measurable, and manageable — when you have accurate information before you sit down with your physician.
If you are also experiencing a new breast symptom alongside your density finding — a lump, nipple discharge, or skin change — use our Symptom Checker to organize what to report at your next appointment.
Your breast density is one piece of a larger clinical picture. If screening does detect something significant, our guide to breast cancer staging and what comes next explains what every stage means for treatment planning.
ℹ️ Medical Disclaimer: The diagnostic criteria, supplemental screening options, cancer risk data, and insurance information discussed in this article reflect current clinical guidelines and are provided for educational purposes only. Dense breast tissue assessment, BI-RADS classification interpretation, supplemental imaging modality selection, and lifetime breast cancer risk calculation each require individualized evaluation by a board-certified physician — including a radiologist, gynecologic oncologist, or breast specialist with access to your complete clinical record, reproductive history, and prior imaging.
Insurance coverage for supplemental screening varies by state law and individual plan. Consult a board-certified gynecologic oncologist, breast radiologist, or your primary care physician before making any screening or clinical decision based on this article. Nothing in this article constitutes a diagnosis, a treatment plan, or individualized medical advice for any specific patient.
What dense breast tissue is — the BI-RADS scale explained
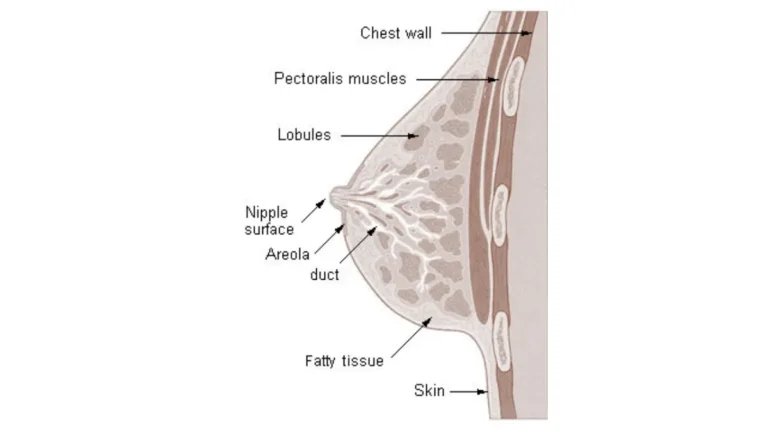
Dense breast tissue means your breast contains more fibroglandular tissue than fatty tissue — a radiological finding classified by a board-certified radiologist using the American College of Radiology’s four-category BI-RADS density scale, ranging from almost entirely fatty (A) to extremely dense (D). Approximately 40% of US women who undergo mammography are classified as BI-RADS C or D, making dense breast tissue one of the most common radiological findings in women’s screening health. Your results letter will state your specific category; everything that follows in your clinical care depends on which one it is.
The four BI-RADS breast density categories on your mammogram report
- BI-RADS A — Almost entirely fatty: The breast is composed predominantly of fatty tissue with minimal fibroglandular components. Mammographic sensitivity is high in this category, and density does not independently elevate cancer risk.
- BI-RADS B — Scattered areas of fibroglandular tissue: Some fibroglandular tissue is present, but fatty tissue still predominates. Mammographic sensitivity remains strong. Density at this level does not significantly elevate cancer risk.
- BI-RADS C — Heterogeneously dense: More than half the breast consists of fibroglandular tissue. Mammographic sensitivity begins to decrease meaningfully. This category is classified as “dense” under current ACR criteria and triggers the federal density notification requirement.
- BI-RADS D — Extremely dense: The breast is almost entirely fibroglandular with very little fatty tissue present. Mammographic sensitivity is substantially reduced. This category carries the highest density-associated cancer risk and typically warrants a dedicated supplemental screening conversation.
🔬 How It Works: Mammography uses X-rays — fatty tissue absorbs them and appears dark on imaging, while fibroglandular tissue absorbs fewer X-rays and appears white. Early breast tumors also appear white on a 2D mammogram. In a predominantly fatty breast, a white tumor mass creates clear contrast against a dark background. In an extremely dense breast, the same tumor is invisible against a white field of fibroglandular tissue — a physics limitation called the masking effect, and the core clinical reason why dense breast tissue changes your screening needs.
Why dense tissue and a breast lump are completely different things
Dense breast tissue is a description of the overall composition of your breast — the ratio of fibroglandular to fatty tissue across the entire breast as seen on mammography. A breast lump is a discrete, palpable or imaging-detected mass at a specific location within the breast. They are categorically different findings. Dense tissue can make a lump significantly harder to identify on mammography, but the tissue itself is not a lump, a tumor, or evidence of cancer. If you have recently received a mammogram result and want to understand the full BI-RADS scoring system — including what callback categories mean — our guide to understanding your mammogram BI-RADS score and what callbacks require explains the complete classification.
How common is dense breast tissue — and are you in the majority?
Dense breast tissue is more prevalent than most patients expect. Current screening data consistently places the proportion of US women with BI-RADS C or D density at approximately 40% of those who undergo mammography — meaning dense breast tissue is not an unusual finding but a characteristic shared by a substantial portion of the screening population. Knowing your specific BI-RADS category is what matters clinically, not whether density itself is common.
✅ Patient Action: If your results letter states BI-RADS C (heterogeneously dense) or BI-RADS D (extremely dense), ask your radiologist or ordering physician at your next appointment: “Based on my density category and full risk profile, do I qualify for supplemental screening?” That single question is the clinical pivot point this article is designed to help you reach.
How much does dense breast tissue actually raise your cancer risk?
Women with extremely dense breasts (BI-RADS D) face approximately 2 to 2.5 times the breast cancer risk of women with predominantly fatty breasts (BI-RADS A), independent of family history or other known risk factors. This elevated risk exists for two compounding reasons: dense tissue is both a direct biological cancer risk factor and a radiological masking factor — meaning it raises the probability of cancer while simultaneously reducing the ability of the primary screening tool to detect it.
Your cancer risk by BI-RADS density category — the numbers
📊 Clinical Data Point: Women with extremely dense breast tissue (BI-RADS D) carry approximately 2–2.5 times the breast cancer incidence risk of women with predominantly fatty breasts (BI-RADS A), with intermediate risk elevations for BI-RADS B and C. Source: NCI data on breast density and cancer risk.
| BI-RADS Category | Tissue Composition | Relative Cancer Risk vs. BI-RADS A | Mammographic Sensitivity | Clinical Action |
|---|---|---|---|---|
| A — Almost entirely fatty | <25% fibroglandular | Baseline (1×) | High (~85–90%) | Standard annual mammogram |
| B — Scattered fibroglandular | 25–50% fibroglandular | Slightly elevated (~1.1–1.2×) | Modest impact | Standard annual mammogram |
| C — Heterogeneously dense | 51–75% fibroglandular | Moderately elevated (~1.5–2×) | Meaningful reduction | Discuss supplemental screening |
| D — Extremely dense | >75% fibroglandular | Substantially elevated (~2–2.5×) | Substantial reduction | Supplemental screening warranted |
Source: ACR BI-RADS classification system; NCI breast density risk data
How dense tissue affects what your mammogram can and cannot detect
Mammographic sensitivity — the ability of a mammogram to identify cancer when it is present — drops significantly in extremely dense breasts. Standard 2D mammography achieves approximately 85–90% sensitivity in mostly fatty breasts. In extremely dense breasts, that figure can fall to 60–70%, meaning a substantial proportion of cancers in BI-RADS D breasts produce no visible finding on the mammogram at all. These missed cancers are called interval cancers — tumors that become clinically apparent between screening cycles, often at a more advanced stage than cancers detected on routine screening.
🔬 How It Works: The masking effect is a physics problem, not a technology failure. Fibroglandular tissue and soft-tissue tumors have similar X-ray absorption characteristics — both appear white on a 2D mammogram. In a mostly fatty breast, a white tumor creates visible contrast against dark background tissue. In an extremely dense breast, the same tumor disappears into a white field of fibroglandular tissue. Researchers have spent the past decade developing supplemental imaging modalities specifically designed to circumvent this white-on-white detection failure.
When dense breasts combine with other risk factors: compounded risk
Dense breast tissue does not operate in isolation. A woman with BI-RADS D density who also carries a BRCA1 or BRCA2 mutation, has a first-degree relative with breast cancer, or has a prior atypical biopsy result faces compounded lifetime breast cancer risk that places her in a categorically different clinical situation — one that requires a different level of surveillance intensity than density alone would indicate. The Tyrer-Cuzick risk model, a validated tool used by oncologists to calculate individualized lifetime breast cancer risk, incorporates breast density alongside genetic, reproductive, and family history variables to generate a single lifetime risk percentage that determines the appropriate screening protocol.
Before your next specialist appointment, use our Genetic Risk Assessment Tool to document your personal and family history — this gives your physician the full picture required to calculate your actual lifetime risk score.
Dense tissue can also conceal the early breast cancer warning signs that imaging alone may miss — physical changes that clinical awareness or self-exam may detect even when a mammogram cannot.
For women with dense breasts and a family history that suggests inherited risk, understanding what a positive BRCA gene test result means for your screening and surveillance plan is the next critical step to take before your specialist appointment.
✅ Patient Action: If you have dense breasts (BI-RADS C or D) and any compounding factor — a first-degree relative with breast cancer diagnosed before age 50, a known BRCA1 or BRCA2 mutation, or a prior biopsy showing atypical ductal hyperplasia or lobular carcinoma in situ — request a dedicated risk assessment appointment with a board-certified gynecologic oncologist or breast surgeon, not a routine mammogram follow-up. These two appointments serve fundamentally different clinical purposes.
Does breast density change over time — and can you lower it?
One of the first questions I hear in consultation after a patient receives her dense breast notification is whether this is permanent. The clinical answer is nuanced — and in some respects genuinely encouraging.
How menopause and age affect breast density naturally
Breast density is not a fixed characteristic for life. As women age and transition through menopause, declining estrogen levels trigger fibroglandular tissue regression — a natural process in which glandular elements involute and are gradually replaced by fatty tissue. Many women see their BI-RADS category shift from C to B, or from D to C, in the years following menopause. This is a well-documented pattern in longitudinal mammography cohorts and represents a meaningful improvement in both density-associated cancer risk and mammographic sensitivity for the women who experience it. The transition does not happen in every patient, and its pace varies considerably by individual.
🔬 How It Works: Estrogen drives the growth and maintenance of fibroglandular tissue throughout the reproductive years. After menopause, sustained low estrogen levels allow fibroglandular tissue to gradually involute and be replaced by fatty tissue — shifting the breast composition toward the lower end of the BI-RADS scale. This is the same hormonal mechanism that explains why premenopausal women have higher average breast density than postmenopausal women across population screening data.
Does HRT, alcohol, or BMI affect your breast density?
The hormonal relationship that enables natural density reduction after menopause is also precisely why hormone replacement therapy (HRT) can reverse or prevent that reduction. Women who take combined estrogen-progestin HRT after menopause often maintain or increase their breast density — the progestin component in particular supports fibroglandular tissue maintenance that would otherwise regress. This interaction is clinically significant and is frequently not explained in standard mammogram result letters. Moderate alcohol consumption has shown a modest association with higher breast density in some research populations; lower body mass index — which reduces the ratio of fatty to fibroglandular tissue — has also been associated with higher relative density in some studies.
⚠️ Clinical Warning: If you are currently taking or considering combined estrogen-progestin hormone replacement therapy and have BI-RADS C or D breast density, this interaction requires explicit discussion with both your prescribing physician and your radiologist — not as two separate conversations, but as a coordinated clinical review of whether HRT is affecting your mammographic sensitivity and whether your screening interval or supplemental imaging should be adjusted as a result.
What no lifestyle change can do — and what that means for screening
No supplement, dietary protocol, or exercise intervention has been shown in clinical trials to reliably shift breast density to a lower BI-RADS category. This is not a gap in research — it is a consistent finding across multiple study populations over decades of investigation. Waiting for density to change before pursuing supplemental screening is not a clinically sound strategy, and no physician should advise it.
✅ Patient Action: If you are currently on HRT and have BI-RADS C or D density, bring this combination to the explicit attention of both your prescribing physician and your radiologist before your next mammogram cycle. Ask specifically: “Is my current HRT affecting my mammographic density, and should we adjust my screening interval or add supplemental imaging to account for this?” Both specialists need to weigh in — not one or the other.
What supplemental screening you should ask for — and how to get it
Supplemental screening for dense breasts is not one-size-fits-all. Your BI-RADS density category and personal risk profile together determine whether supplemental ultrasound, 3D mammography (tomosynthesis), contrast-enhanced mammography, or breast MRI is the clinically appropriate next step — and the modality selection matters, because each has different cancer detection rates, false-positive rates, cost profiles, and insurance coverage structures.
Supplemental screening options for BI-RADS C: what the evidence supports
The most commonly recommended first-line supplemental modality for women with BI-RADS C or D density who do not have additional high-risk markers is supplemental ultrasound. Ultrasound uses sound waves rather than X-rays and is not subject to the white-on-white masking problem of standard 2D mammography — making it capable of detecting lesions that mammography cannot visualize in dense tissue. Automated breast ultrasound (ABUS) provides standardized whole-breast imaging and is increasingly covered by insurance in states with dense breast mandate laws; hand-held ultrasound (HHUS) allows real-time targeted assessment directed by the radiologist in the room.
Digital breast tomosynthesis (DBT) — commonly called 3D mammography — is a second evidence-supported option for women with BI-RADS C density. DBT acquires breast images in thin sequential slices rather than a single flat projection, reducing the tissue overlap that causes the masking effect and improving cancer detection rates compared to 2D mammography in dense tissue. For some BI-RADS C patients with no additional risk factors, upgrading from 2D to DBT as the primary mammogram may be the radiologist’s first supplemental recommendation before adding ultrasound.
📊 Clinical Data Point: Current American Cancer Society guidance recommends that women with dense breast tissue discuss the benefits and limitations of supplemental screening with their physician, as coverage, availability, and clinical appropriateness of specific modalities vary by location, risk profile, and insurance plan. Source: American Cancer Society guidelines on dense breast screening.
When breast MRI is and isn’t appropriate for dense tissue patients
Breast MRI offers the highest sensitivity of any currently available breast imaging modality — but it is not appropriate for all dense breast patients. Current American College of Radiology and Society of Breast Imaging guidance reserves annual breast MRI for women whose calculated lifetime breast cancer risk exceeds 20%, as determined by a validated risk model such as Tyrer-Cuzick or IBIS. BRCA-positive patients, women with chest radiation exposure before age 30, and women with multiple first-degree relatives with breast or ovarian cancer are the populations for whom annual MRI is most strongly supported. Extremely dense breasts alone — without these additional high-risk markers — do not typically qualify a patient for annual MRI under current ACR eligibility criteria.
✅ Patient Action: Before scheduling any supplemental imaging, request a formal lifetime risk calculation from a board-certified radiologist or gynecologic oncologist — not just your primary care physician. Ask specifically: “Can you calculate my lifetime breast cancer risk using a validated model and tell me which supplemental modality is appropriate for my BI-RADS category and that risk score?” This is the foundation of an individualized, evidence-based supplemental screening plan.
The FDA notification rule — what your letter must now tell you by law
Since September 2024, all US mammography facilities accredited under the federal Mammography Quality Standards Act (MQSA) are legally required to include each patient’s BI-RADS breast density category in their mammogram results summary. This rule closed a long-standing gap in which millions of US women received normal mammogram results each year without being informed that their dense tissue had substantially reduced the test’s ability to detect cancer. If your most recent results letter did not include your density category, contact your mammography facility in writing and request it — you are entitled to this information under federal law.
📊 Clinical Data Point: The FDA’s final rule on mammography density reporting was finalized in March 2023 and required full compliance at all MQSA-accredited facilities by September 2024. Source: FDA mammography density notification requirements.
Insurance coverage for dense breast supplemental screening by state
Insurance coverage for supplemental breast imaging varies significantly across the United States. More than 30 states have enacted dense breast legislation requiring insurers to cover supplemental imaging modalities — typically ultrasound — for patients who receive a dense breast notification from their mammography facility. Coverage under these laws does not always extend to breast MRI unless additional high-risk criteria are met. Medicare covers supplemental ultrasound when medically ordered by a physician. Before scheduling any supplemental imaging, verify your specific plan’s dense breast benefits directly with your insurer and confirm whether a physician order or prior authorization is required for the modality being recommended.
Before adding supplemental imaging to your screening plan, review the recommended mammogram screening schedule by age and risk level to confirm you are on the appropriate baseline screening plan first.
Risk factors that make dense breasts more dangerous — and what to do about them
Dense breast tissue elevates cancer risk independently — but its clinical impact is compounded substantially when additional risk factors are present. Knowing which compounding factors apply to your specific situation determines whether you need standard supplemental screening or a dedicated high-risk surveillance protocol with substantially different imaging intensity and interval.
BRCA mutation carriers with dense breasts: a distinct high-risk category
Women who carry a pathogenic BRCA1 or BRCA2 mutation and also have BI-RADS C or D breast density occupy a distinct high-risk category requiring a surveillance protocol substantially more intensive than standard dense breast management. Current NCCN guidance for known BRCA1/2 carriers recommends annual breast MRI beginning at age 25–30 and annual mammography beginning at age 30 — not supplemental ultrasound as a first-line addition, but MRI from the outset, regardless of what the density category alone would have indicated. The mutation, not the density, drives the surveillance protocol for this population.
Black women with dense breast tissue face a particularly compounded risk profile — dense tissue is more prevalent in younger Black women, and breast cancer in Black women is more frequently diagnosed at advanced stages with higher associated mortality rates. Our article on breast cancer risk and racial disparities in Black women covers this critical clinical and health equity dimension in depth.
Prior atypical biopsy and dense tissue — when supplemental screening is not enough
A history of atypical ductal hyperplasia (ADH) or lobular carcinoma in situ (LCIS) on a prior breast biopsy significantly elevates lifetime breast cancer risk — independently of breast density. When atypical pathology and BI-RADS C or D density are both present, the combined lifetime risk calculation using a validated model frequently exceeds 20%, placing the patient in ACR-criteria MRI-eligible territory. This is a clinical combination that primary care physicians sometimes do not flag proactively when reviewing mammography results. If you have both findings documented in your medical history and have not undergone a formal lifetime risk calculation, request one explicitly at your next specialist appointment.
Chest radiation history and density: what oncologists monitor differently
Women who received mantle field or chest radiation before age 30 — most commonly as treatment for Hodgkin’s lymphoma — carry substantially elevated lifetime breast cancer risk that is independent of and additive to density-associated risk. Current NCCN guidance recommends annual breast MRI plus annual mammography beginning 8 years after radiation exposure and no later than age 30 for this population. This is a numerically smaller group, but the risk elevation is sufficient that their surveillance protocol parallels that of known BRCA carriers in terms of MRI inclusion and initiation age. Understanding your complete breast cancer risk factors and how multiple factors interact gives you the full clinical picture before your next consultation.
✅ Patient Action: If you have dense breasts and any of the three compounding factors described above — BRCA mutation status, prior atypical biopsy, or a history of chest radiation before age 30 — do not wait for a routine referral. Request a dedicated risk consultation with a board-certified genetic counselor or gynecologic oncologist to calculate your lifetime breast cancer risk using a validated model before your next screening cycle begins. The resulting risk score changes which imaging protocol is appropriate for you.
A gynecologic oncologist’s perspective on dense breast risk and next steps
I want to share the clinical reasoning I actually use when a patient with dense breasts sits across from me in the consultation room — because it differs substantially from what the standard mammogram report communicates.
What I tell every patient who calls after getting a dense breast letter
The most common misconception I correct after a patient receives her dense breast notification is this: she believes that because her mammogram came back “normal,” she is cancer-free. A normal mammogram in a woman with extremely dense breasts means no cancer was detected by that test on that day — it does not mean no cancer is present. The false-negative rate of standard 2D mammography in extremely dense breasts is real, clinically significant, and the precise reason the FDA required facilities to begin disclosing density to patients. My first clinical task after a dense breast consultation letter is helping the patient understand that the mammogram is reporting what it was capable of seeing — not what is definitively there.
🩺 Physician Note: When a 47-year-old patient with BI-RADS D density and no family history sits across from me after her notification letter, the first thing I do is not order an MRI. I calculate her Tyrer-Cuzick lifetime risk score using her full reproductive history, body mass index, prior biopsy record, and detailed family cancer history. If that score falls below 20%, I recommend supplemental automated breast ultrasound — ABUS — as the most evidence-appropriate, insurance-accessible first step. MRI is reserved for patients whose risk calculation and clinical picture justify its higher cost and higher recall rate. That individualized decision is exactly what the notification letter cannot provide on its own — and what a specialist consultation can.
The clinical decision I make that most standard mammogram reports don’t support
The standard mammogram report classifies your density. What it does not do is calculate your lifetime risk, recommend a specific supplemental modality, or route you to the right specialist for a comprehensive discussion. Those three steps require a clinician who has your complete medical record and uses a validated risk model. If you have BI-RADS D density and your physician has simply noted it in your chart without discussing a supplemental screening plan, that is a gap in your care — one you have both the right and the clinical information to close.
For patients interested in contributing to advancing screening science and accessing emerging modalities, a search of active clinical trials on dense breast supplemental screening may identify enrollment opportunities in your area.
Dense breast tissue and cancer risk: your questions answered
1. What does it mean to have dense breast tissue?
Dense breast tissue means your breast contains more fibroglandular tissue than fatty tissue — a radiological finding your radiologist classifies into four BI-RADS categories, from almost entirely fatty (A) to extremely dense (D). Your results letter will specify your category. Dense tissue is not a tumor or a diagnosis; it is a structural characteristic that directly affects your cancer risk level and your supplemental screening plan going forward.
2. Does dense breast tissue always mean higher cancer risk?
Dense breast tissue cancer risk varies by BI-RADS category. Women with BI-RADS D density carry approximately 2 to 2.5 times the breast cancer risk of women with predominantly fatty breasts. Women with BI-RADS C have a moderate but measurable risk elevation. BI-RADS A and B are not associated with significant density-related risk increase. Consult a board-certified gynecologic oncologist to assess your complete individual risk profile, including factors beyond density alone.
3. What are the four types of breast density on a mammogram?
The four BI-RADS breast density categories are: BI-RADS A (almost entirely fatty — lowest density), BI-RADS B (scattered areas of fibroglandular tissue), BI-RADS C (heterogeneously dense — more than half the breast is fibroglandular), and BI-RADS D (extremely dense — the highest density category). Categories C and D are classified as “dense” under current American College of Radiology criteria and trigger the federal density notification requirement and supplemental screening discussions.
4. Do I need an ultrasound if I have dense breasts?
Most women with BI-RADS C or D density benefit from supplemental ultrasound in addition to their annual mammogram. Automated breast ultrasound and hand-held ultrasound can detect cancers that standard mammography misses in dense tissue. Whether ultrasound is appropriate for you depends on your full risk profile, not density category alone. Consult a board-certified radiologist or gynecologic oncologist to determine whether supplemental ultrasound is the right next step for your specific situation.
5. Does insurance cover supplemental breast screening for dense breasts?
Coverage varies significantly. More than 30 states have enacted dense breast legislation requiring insurers to cover supplemental imaging for patients with dense tissue. Medicare and many commercial plans cover supplemental ultrasound when medically ordered. No federal mandate currently requires universal supplemental screening coverage. Verify your specific plan’s dense breast benefits directly with your insurer before scheduling, and confirm whether a physician order or prior authorization is required for your prescribed modality.
6. Can dense breast tissue go away on its own?
Dense breast tissue commonly decreases after menopause, as declining estrogen causes fibroglandular tissue to involute and be replaced by fatty tissue, often shifting the BI-RADS category lower. This is not guaranteed and varies considerably by individual. Hormone replacement therapy can maintain or increase density even post-menopause. Discuss how your current hormonal status affects your breast density with your prescribing physician and radiologist before your next screening cycle begins.
7. Is dense breast tissue the same as a breast lump?
Dense breast tissue and a breast lump are fundamentally different findings. Dense tissue describes the overall composition of the breast — more fibroglandular than fatty — across the entire breast as seen on mammography. A lump is a discrete, palpable or imaging-detected mass at a specific location. Dense tissue can make lumps significantly harder to detect on mammography. If you discover a new lump or firm area in your breast, contact your physician immediately — do not wait for your next scheduled mammogram.
8. What is the FDA rule about dense breast notification letters?
Since September 2024, all US mammography facilities accredited under the federal Mammography Quality Standards Act are required to include your BI-RADS breast density category in every mammogram results summary. This rule ensures all women know whether they have dense tissue and can discuss supplemental options with their physician. If your results letter did not include your density category, contact your mammography facility in writing and request it — you are entitled to this information under federal law.
9. Should I get a breast MRI if I have dense breasts?
Breast MRI is not automatically recommended for dense breasts alone. Current American College of Radiology guidance reserves MRI for women whose calculated lifetime breast cancer risk exceeds 20%, including BRCA-positive patients, those with chest radiation history, and those with multiple first-degree relatives with breast or ovarian cancer. Dense breasts without additional risk factors typically qualify for supplemental ultrasound first, not MRI. Consult a board-certified radiologist to calculate your individual lifetime risk before requesting MRI.
10. How does dense breast tissue affect mammogram accuracy?
Dense breast tissue reduces mammogram accuracy through the masking effect — fibroglandular tissue and early tumors both appear white on standard 2D mammography, making tumors invisible within dense white tissue. Mammographic sensitivity is substantially lower in extremely dense breasts than in mostly fatty ones — a pattern consistently confirmed across decades of breast imaging research. Consult a board-certified breast radiologist about whether 3D mammography or supplemental ultrasound would meaningfully improve cancer detection for your specific density category.
11. What lifestyle changes can reduce breast density?
No lifestyle intervention is proven to reliably shift breast density to a lower BI-RADS category. Moderating alcohol intake, maintaining a healthy body weight, and avoiding exogenous hormones may modestly influence density in some women, but none of these changes replace the need for supplemental screening in BI-RADS C or D patients.
Do not delay your screening protocol while attempting lifestyle modification. Discuss any planned hormonal or lifestyle changes with your gynecologist and radiologist so your screening plan can be adjusted accordingly.
Your dense breast results are a starting point — here is your next step
Receiving a dense breast notification can feel alarming. It should not. Dense breast tissue is a common finding, a measurable risk factor, and a manageable clinical reality — when you approach it with accurate information and the right specialist in your corner.
Three steps before your next appointment. First, locate your BI-RADS category on your results letter — it will be stated as A, B, C, or D, or described in the corresponding plain-language terms. Second, bring that category to a dedicated supplemental screening conversation with a board-certified radiologist or gynecologic oncologist, not a general follow-up call. Third, ask for a formal lifetime risk calculation using a validated model before any imaging decision is made.
Understanding breast cancer survival rates by stage and subtype gives you the full picture of what early detection means — and why getting the screening question right before anything is found matters enormously for long-term outcomes.
✅ Patient Action: Schedule a dedicated risk consultation with a board-certified gynecologic oncologist or breast radiologist within the next 30 days if you have BI-RADS C or D density and have not yet discussed supplemental screening. This is not a routine follow-up — it is a specific clinical conversation about what your density category warrants, and your physician needs to have your complete record in hand to answer it correctly.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.