On This Page – Quick Medical Summary
What stage 4 breast cancer really means for you
Stage 4 breast cancer, also called metastatic breast cancer, occurs when cancer cells have spread from the breast to distant organs — most commonly the bones, lungs, liver, or brain. This stage is confirmed when imaging or biopsy reveals cancer in a distant site beyond the breast and regional lymph nodes, and it requires systemic treatment to manage disease throughout the body.
According to the American Cancer Society’s 2026 breast cancer statistics, stage 4 breast cancer represents a distinct clinical category requiring a fundamentally different treatment framework from all earlier stages.
Metastatic vs. advanced: what’s the clinical difference?
“Advanced” breast cancer describes locally aggressive stage 3 disease that has not yet spread to distant organs. Stage 4 is defined by confirmed distant metastasis — cancer in a distant organ, confirmed by imaging or biopsy. That single distinction changes every treatment decision in the patient’s care.
Why a stage 4 diagnosis is not the same as no treatment options
In my clinic, patients arriving after a stage 4 diagnosis often believe meaningful treatment is no longer available. The 2026 clinical evidence does not support that belief.
FDA-approved options — including CDK4/6 inhibitors, antibody-drug conjugates, and PARP inhibitors — have measurably changed the stage 4 outlook for many patients. For a complete overview of how breast cancer is staged and what each stage means clinically, see our guide to breast cancer stages and survival.
✅ Patient Action: If you or a loved one has received a stage 4 breast cancer diagnosis, schedule an appointment with a board-certified medical oncologist or gynecologic oncologist to review your complete biomarker test results and discuss treatment eligibility before any care decisions are made.
ℹ️ Medical Disclaimer: The diagnostic criteria, treatment options, medication information, clinical trial guidance, and insurance considerations discussed in this article reflect current 2026 clinical evidence and are provided for educational purposes only. Individual diagnostic conclusions, treatment decisions, medication choices, clinical trial eligibility, and insurance coverage determinations depend on patient history, biomarker profile, comorbidities, prior treatment history, and specialist assessment. Consult a board-certified medical oncologist or gynecologic oncologist before acting on any clinical information in this article.
Stage 4 breast cancer survival rates: the 2026 data
The 5-year relative survival rate for stage 4 breast cancer varies dramatically by molecular subtype — and the combined figure for all stage 4 patients obscures this reality in ways that can mislead a newly diagnosed patient.
5-year survival rates by breast cancer subtype
| Molecular Subtype | Primary Treatment Driver | Key Clinical Detail |
|---|---|---|
| HR+/HER2- | CDK4/6 inhibitors + endocrine therapy | Outcomes improving significantly with CDK4/6 combinations vs. prior era |
| HER2-positive | Anti-HER2 agents + trastuzumab deruxtecan | ADC therapies have shifted survival curves upward |
| Triple-negative (TNBC) | Immunotherapy + sacituzumab govitecan | PD-L1-positive patients benefit most from pembrolizumab addition |
| BRCA-mutated | PARP inhibitors | Requires confirmed germline BRCA1/2 mutation for PARP inhibitor eligibility |
📊 Clinical Data Point: 5-year relative survival by molecular subtype — Source: NCI SEER database, 2026.
What “median survival” really means — and what it doesn’t
A median survival figure marks the point at which half the study population is still alive. It is a population midpoint — not your individual ceiling, and not your prognosis.
SEER datasets reflect patients treated with regimens that predate today’s 2026 therapies. CDK4/6 inhibitor combinations and newer ADC protocols have shifted outcomes upward for multiple subtypes — improvements that older datasets cannot yet fully reflect.
🩺 Physician Note: “When a patient asks how long they have, my answer is always the same: population medians are not individual predictions. The biomarkers in your specific tumor, the regimens you are eligible for today, and your performance status matter far more than any average figure drawn from a dataset collected before these therapies existed.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
For a full statistical breakdown across all breast cancer stages, see our guide to breast cancer survival rates by stage.
✅ Patient Action: Before interpreting any survival statistic in relation to your own diagnosis, consult a board-certified medical oncologist who can contextualize these figures against your specific subtype, biomarker profile, and eligibility for 2026-approved therapies.
How doctors diagnose and classify stage 4 breast cancer
At stage 4, biomarker testing is not a step in the treatment process — it is the foundation of every decision that follows. Your tumor’s molecular profile determines which therapies apply and which do not.
The four main subtypes and what each means for treatment
| Molecular Subtype | Key Biomarker Result | Primary 2026 Treatment Class |
|---|---|---|
| HR+/HER2- | ER or PR positive; HER2 negative | CDK4/6 inhibitors + endocrine therapy |
| HER2-positive | HER2 IHC 3+ or FISH-amplified | Anti-HER2 agents + antibody-drug conjugates |
| Triple-negative (TNBC) | ER-negative, PR-negative, HER2-negative | Immunotherapy + sacituzumab govitecan |
| HR+/HER2+ | Both ER/PR-positive and HER2-positive | Anti-HER2 + endocrine combination |
Why biomarker testing is not optional at stage 4
In my clinic, I explain to every newly diagnosed stage 4 patient that genomic profiling is the map that guides every decision we make together. The minimum required panel at metastatic diagnosis includes HER2 (IHC, then FISH if IHC 2+), ER/PR hormone receptor status, BRCA1/2 germline genetic testing, PIK3CA mutation testing (if HR+/HER2-), and PD-L1 expression testing (if TNBC).
Each test result changes the treatment algorithm. Testing must be performed on the most recent tumor sample — not an archived biopsy from the original diagnosis, which may no longer reflect current tumor biology.
If your family history includes breast or ovarian cancer, use our Genetic Risk Assessment Tool to evaluate your hereditary risk before a genetics consultation. For a full explanation of BRCA gene test results and what a positive result means for your treatment options, see our dedicated guide.
Signs and symptoms of metastatic breast cancer by organ site
- Bone metastasis: Deep, persistent bone pain — often in the spine, hips, or femur — that worsens at rest or at night
- Lung metastasis: Unexplained shortness of breath, a persistent dry cough, or new chest discomfort unrelated to exertion
- Liver metastasis: Right-side abdominal pain or fullness, unexplained fatigue, or early jaundice (yellowing of skin or whites of the eyes)
- Brain metastasis: Persistent headaches, new vision changes, unexplained balance problems, or focal neurological symptoms
For a comprehensive review of how symptoms differ across breast cancer stages, see our guide to early and advanced breast cancer symptoms.
✅ Patient Action: Before starting any treatment for stage 4 breast cancer, ask your oncologist to confirm that a full biomarker panel — including HER2 IHC/FISH, ER/PR, BRCA1/2 germline testing, PIK3CA mutation testing (if HR+/HER2-), and PD-L1 testing (if TNBC) — has been completed on your most recent tissue sample, not an older archived biopsy.
2026 FDA-approved treatments for stage 4 breast cancer
In 2026, FDA-approved treatment options for stage 4 breast cancer are determined by molecular subtype. Your HER2, ER/PR, BRCA, and PIK3CA status determines which therapies apply:
- HR+/HER2- → CDK4/6 inhibitors plus endocrine therapy
- HER2-positive → anti-HER2 agents and antibody-drug conjugates
- Triple-negative (TNBC) → immunotherapy and sacituzumab govitecan
- BRCA-mutated → PARP inhibitors
For the complete current list of approved agents and updated indications, see the FDA-approved breast cancer therapies resource.
HR+/HER2- breast cancer: CDK4/6 inhibitors and endocrine therapy
Palbociclib (Ibrance), ribociclib (Kisqali), and abemaciclib (Verzenio) are FDA-approved CDK4/6 inhibitors that block the G1/S checkpoint in the cell cycle, preventing cancer cells from replicating. Each is used in combination with an aromatase inhibitor or fulvestrant as the standard first-line approach for most HR+/HER2- metastatic patients. Where a PIK3CA mutation is confirmed, alpelisib (Piqray) plus fulvestrant is an additional FDA-approved option. For a comparison of endocrine therapy options, see our guide to tamoxifen vs. aromatase inhibitors.
HER2-positive metastatic breast cancer: ADCs and anti-HER2 agents
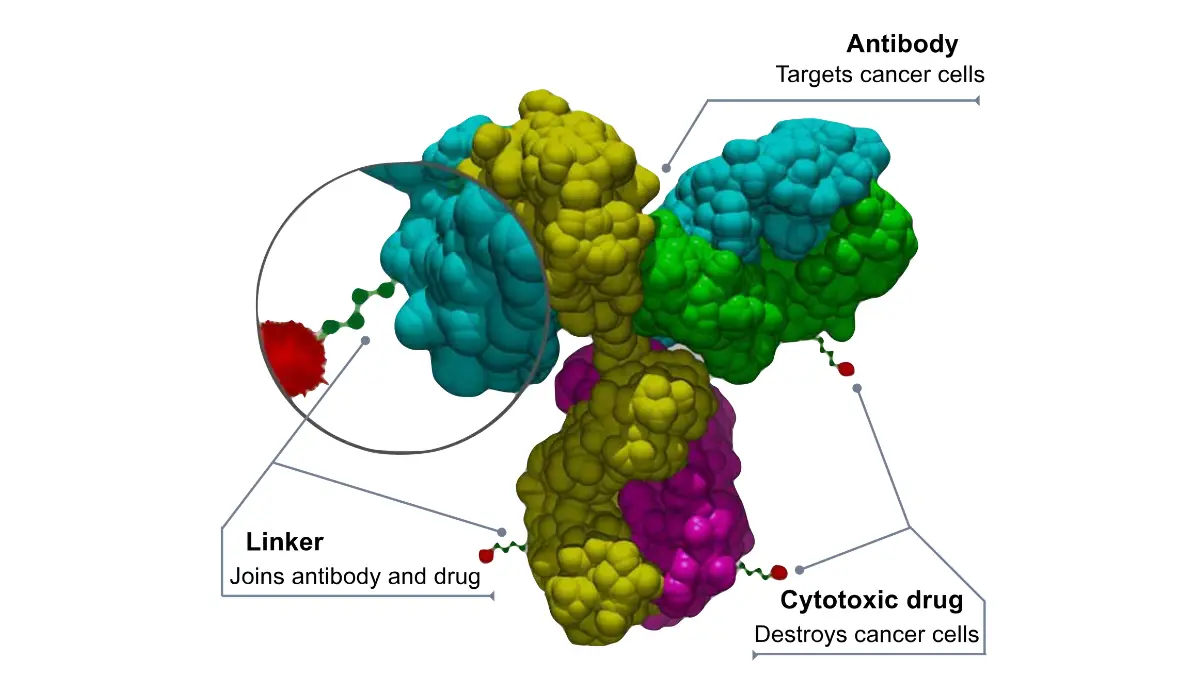
Trastuzumab deruxtecan (T-DXd, Enhertu) is the central second-line treatment in HER2-positive metastatic breast cancer — an antibody-drug conjugate that delivers a chemotherapy payload directly to HER2-expressing cells and, through the bystander effect, to neighboring tumor cells that may not express HER2.
🔬 How It Works: T-DXd uses the anti-HER2 antibody trastuzumab as a guided delivery vehicle. Once it locks onto the HER2 receptor on the cancer cell’s surface, it releases its chemotherapy payload inside the cell. The released drug then diffuses outward to neighboring cells — including HER2-negative ones — and kills them. This is the bystander effect, and it is why T-DXd reaches tumors that earlier HER2-targeted agents could not.
For the complete anti-HER2 therapy sequence — including pertuzumab, tucatinib, and T-DXd combinations — see our guide to HER2-positive breast cancer treatment.
Triple-negative breast cancer: immunotherapy and sacituzumab govitecan
Sacituzumab govitecan (Trodelvy) is an FDA-approved ADC for triple-negative breast cancer that targets the TROP2 protein. For PD-L1-positive TNBC patients, pembrolizumab (Keytruda) combined with chemotherapy is FDA-approved in the first-line setting. For a complete overview of treatment options specific to this subtype, see our guide to triple-negative breast cancer.
BRCA-mutated breast cancer: PARP inhibitors
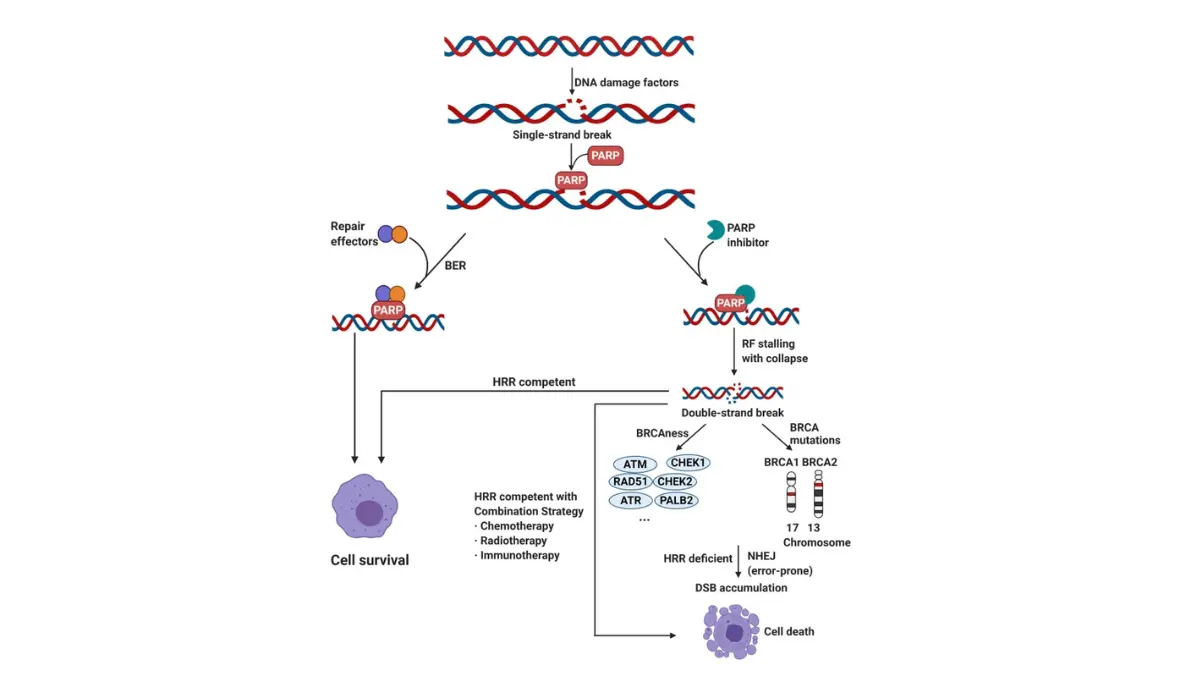
Olaparib (Lynparza) and talazoparib (Talzenna) are FDA-approved PARP inhibitors for patients with confirmed germline BRCA1 or BRCA2 mutations and HER2-negative metastatic breast cancer. These drugs exploit the tumor’s inability to repair DNA — a vulnerability caused directly by the BRCA mutation — triggering cancer cell death through a mechanism called synthetic lethality.
✅ Patient Action: Treatment selection for stage 4 breast cancer must be made with a board-certified medical oncologist who has reviewed your complete biomarker profile, prior treatment history, and current performance status. Never rule out or select a treatment based on reading alone.
When breast cancer spreads: managing bone, liver, lung, and brain
When stage 4 breast cancer reaches specific organ sites, systemic treatment typically continues — but targeted interventions are added to protect organ function and prevent serious complications.
Bone metastasis: preventing fractures and managing pain
Bone metastasis is among the most common stage 4 sites in breast cancer. Zoledronic acid — a bisphosphonate — and denosumab — a RANK-L inhibitor — are the two primary bone-modifying agents used to prevent skeletal-related events (fractures, spinal cord compression, hypercalcemia) while systemic therapy continues. Denosumab blocks RANK-L, the signaling protein that activates osteoclasts and drives bone destruction. Zoledronic acid binds directly to bone mineral and suppresses osteoclast recruitment.
🩺 Physician Note: “Patients with bone metastasis frequently arrive in my clinic with undertreated pain and no bone-modifying agent in place. My first clinical question is always: has a bisphosphonate or denosumab been started alongside systemic therapy? Delaying this step meaningfully increases skeletal-related event risk.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
Brain metastasis: what patients need to know in 2026
For HER2-positive patients with brain metastasis, trastuzumab deruxtecan has demonstrated documented central nervous system (CNS) activity — meaning it reaches the brain at clinically meaningful concentrations. Stereotactic radiosurgery — targeted radiation directed at individual brain lesions without whole-brain irradiation — is the preferred local treatment for oligometastatic CNS disease.
Leptomeningeal disease, in which cancer cells infiltrate the cerebrospinal fluid surrounding the brain and spinal cord, is a distinct diagnosis from brain metastasis and requires separate clinical management.
If you or a family member is experiencing new neurological symptoms, use our Symptom Checker to document them before the next oncology appointment. For a full overview of treatment approaches at stage 4, see our guide to metastatic breast cancer treatment options.
⚠️ Clinical Warning: New persistent headaches, sudden vision changes, unexplained balance problems, or focal neurological symptoms in a patient with a known stage 4 diagnosis require immediate oncologist contact. Do not wait for a scheduled appointment — these may signal brain metastasis requiring urgent imaging and treatment adjustment.
✅ Patient Action: If you are experiencing new or worsening bone pain, unexplained shortness of breath, right-side abdominal discomfort, or any new neurological symptom, report these to your oncologist immediately — do not wait for the next scheduled visit.
How to find a stage 4 breast cancer clinical trial in 2026
Clinical trial participation is not a last resort — it is a legitimate treatment option at any line of therapy, including first-line. Many 2026 trials give patients access to next-generation ADC combinations, novel PARP inhibitor protocols, and investigational immunotherapy regimens before FDA approval.
Clinical trials are a real treatment option — not a last resort
In my practice, I discuss trial eligibility with every stage 4 patient at first consultation — not when other options are exhausted. The best trials today are not experiments; they are structured pathways to the next standard of care.
Step-by-step: how to search for trials that match your subtype
- Go to ClinicalTrials.gov to search active metastatic breast cancer clinical trials
- Enter “breast cancer” in the Condition or Disease field
- Filter by Phase III under Study Phase
- Add your subtype keyword — “triple-negative,” “HER2-positive,” or “BRCA-mutated” — in the Other Terms field
- Set Recruitment Status to “Recruiting”
- Enter your zip code or state under Location to find geographically accessible trials
- Click any result, review the eligibility criteria, and contact the Study Coordinator listed at the bottom of the trial page
Your oncologist must review your eligibility — including prior treatment lines, biomarker status, organ function, and performance status — before you contact any trial site. If you are enrolling in a trial, review your insurance plan’s oncology trial coverage using a health insurance comparison tool before committing, as standard-of-care costs during trial participation may still fall to your insurer.
✅ Patient Action: Before enrolling in any clinical trial, consult your treating oncologist to confirm your eligibility. Prior treatment history, biomarker results, and organ function all determine whether a specific trial is appropriate for you at this time.
A gynecologic oncologist’s perspective on living with stage 4
Stage 4 breast cancer is not only a medical challenge — it is a life challenge, and the treatment decisions it demands extend far beyond drug selection.
Goals-of-care conversations: what to ask your oncologist
🩺 Physician Note: “One of the most important conversations I have with every stage 4 patient is about what they most want to preserve — whether that is time with family, the ability to keep working, or maintaining cognitive clarity during treatment. These goals shape every regimen decision we make together. I have never had a patient regret having this conversation early.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
Bring these specific questions to your oncologist about goals of care:
- “If this regimen causes significant fatigue that prevents me from working or caring for my family, what is our next option that better preserves my quality of life?”
- “At what point would you recommend transitioning from active disease management to palliative-focused care, and what would that transition look like?”
- “Can I see a palliative care specialist now — not later — to manage symptoms and side effects alongside my systemic treatment?”
Quality of life during treatment: what the data doesn’t show
Palliative care integration from the time of diagnosis — not at end of life — is associated with better quality-of-life outcomes and, in some studies, extended overall survival. Early referral to a palliative care specialist does not mean giving up; it means managing the full burden of illness alongside active treatment
Side effects that survival statistics cannot capture — fatigue, cognitive effects from systemic therapy, emotional distress — are real and should be discussed with your care team from the first appointment, not after they become debilitating. For a comprehensive review of what to expect, see our guide to chemotherapy side effects in breast cancer.
✅ Patient Action: If goals-of-care conversations have not yet been initiated with your oncology team, ask to schedule a dedicated appointment with both your oncologist and a palliative care specialist — these conversations should begin at diagnosis, not at end of life.
Stage 4 breast cancer: your questions answered by physicians
1. What is the life expectancy for stage 4 breast cancer?
Life expectancy for stage 4 breast cancer varies significantly by molecular subtype per 2026 NCI SEER data. HER2-positive and HR+/HER2- patients tend to have different survival trajectories than triple-negative patients. These are population medians — not individual predictions. Your biomarker profile and eligibility for 2026-approved therapies matter more than any average figure. Consult a board-certified medical oncologist to interpret this data in the context of your specific diagnosis.
2. Can stage 4 breast cancer go into remission?
Complete remission is uncommon in metastatic breast cancer, but partial response and stable disease — meaning the tumor shrinks measurably or stops progressing — are documented, achievable goals. CDK4/6 inhibitors and antibody-drug conjugates have produced meaningful partial responses across multiple subtypes. Oncologists typically use “stable disease” rather than remission at stage 4, but this status can be sustained for extended periods with ongoing systemic treatment.
3. What is the best treatment for metastatic breast cancer?
The best stage 4 breast cancer treatment is always subtype-specific: HR+/HER2- patients typically receive a CDK4/6 inhibitor plus endocrine therapy; HER2-positive patients receive anti-HER2 agents or trastuzumab deruxtecan; triple-negative patients are treated with sacituzumab govitecan or pembrolizumab; and BRCA-mutated patients are eligible for PARP inhibitors. No single regimen is universally best. Consult a board-certified medical oncologist who has reviewed your complete biomarker profile before selecting any regimen.
4. Is stage 4 breast cancer always terminal?
Stage 4 breast cancer is life-limiting but not universally fatal in a short timeframe. Many patients live for years — sometimes many years — with active systemic treatment. The clinical distinction between “terminal” (imminently life-ending) and “chronic managed disease” is real and meaningful. CDK4/6 inhibitor combinations have advanced the chronic-disease model for HR+/HER2- metastatic patients, and newer ADC therapies continue to shift this picture.
5. What new breast cancer drugs were approved or updated in 2026?
The FDA’s breast cancer drug approval pipeline in 2026 includes ongoing indication updates for CDK4/6 inhibitors, antibody-drug conjugates, and PARP inhibitors — and may include entirely new agents. Ask your oncologist specifically whether any 2026 approvals or updated indications apply to your molecular subtype.
6. How is HER2-positive stage 4 breast cancer different from other types?
HER2-positive metastatic breast cancer overexpresses the HER2 protein, giving patients access to anti-HER2 targeted therapies — trastuzumab, pertuzumab, tucatinib — and to HER2-directed antibody-drug conjugates like trastuzumab deruxtecan unavailable to HER2-negative patients. HER2-positive patients may also benefit from T-DXd’s documented CNS activity in brain metastasis. Consult a board-certified medical oncologist to review your HER2 status and plan the full therapy sequence.
7. What does stage 4 breast cancer feel like?
Symptoms depend on the metastatic site. Bone involvement causes deep, persistent bone pain worsening at rest. Lung metastasis produces shortness of breath and chronic cough. Liver involvement may cause right-side abdominal pain or early jaundice. Brain metastasis causes persistent headaches, vision changes, or balance problems. Some patients have minimal symptoms, discovered only on imaging. Use our Symptom Checker to document your symptoms before your next oncology appointment.
8. Is chemotherapy still used for stage 4 breast cancer?
Yes — chemotherapy remains an active treatment in stage 4 breast cancer, particularly in triple-negative disease and after targeted therapies are exhausted. It is also the active payload in antibody-drug conjugates like trastuzumab deruxtecan and sacituzumab govitecan — making it central to some of the most effective 2026 regimens. For a full overview, see our guide to breast cancer chemotherapy. Consult a board-certified medical oncologist before any chemotherapy decision.
9. How do BRCA mutations affect stage 4 breast cancer treatment?
BRCA1 and BRCA2 mutations create homologous recombination deficiency — a DNA repair vulnerability that PARP inhibitors exploit through synthetic lethality. Olaparib and talazoparib are FDA-approved for confirmed germline BRCA1/2-mutated, HER2-negative metastatic breast cancer. BRCA status also carries hereditary implications for family members. Consult a board-certified medical oncologist and a genetic counselor to discuss how your BRCA mutation affects both treatment options and your family’s cancer risk.
10. Can surgery treat stage 4 breast cancer?
Surgery is not the primary treatment for metastatic breast cancer, but it plays a role in specific scenarios — resection of a solitary bone lesion, spinal stabilization for vertebral instability, or palliative mastectomy in select cases — after multidisciplinary team review. Systemic therapy remains the treatment backbone at stage 4. Consult a board-certified medical oncologist and a surgical oncologist to determine whether any surgical intervention applies to your specific case.
11. How do I find a clinical trial for stage 4 breast cancer in 2026?
Go to ClinicalTrials.gov, enter “breast cancer” in the condition field, filter by Phase III, add your subtype keyword, set recruitment status to “Recruiting,” and enter your zip code. Review eligibility criteria on each trial page, then contact the listed Study Coordinator. Your oncologist must confirm your eligibility — prior treatment lines, biomarker status, and organ function — before you contact any trial site.
What to do next after a stage 4 breast cancer diagnosis
A stage 4 breast cancer diagnosis comes with a great deal of information to absorb in a short period of time. The 2026 treatment landscape — CDK4/6 inhibitors, antibody-drug conjugates, PARP inhibitors, and immunotherapy — offers more options than any prior era, matched to your specific molecular subtype.
Your three most important next steps:
- Schedule an appointment with a board-certified medical oncologist or gynecologic oncologist who specializes in breast cancer
- Request a full biomarker panel before treatment begins — HER2, ER/PR, BRCA1/2, PIK3CA, and PD-L1
- Ask your oncologist specifically about clinical trial eligibility at your first appointment
✅ Patient Action: Bring this guide to your first oncology appointment. Ask: “Has my tumor been tested for HER2, ER/PR, BRCA1/2, PIK3CA, and PD-L1? Which 2026 FDA-approved options apply to my specific subtype, and am I eligible for any active clinical trials?”
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.