What Alcohol Really Does to Your Breast Cancer Risk
Alcohol raises breast cancer risk 7–10% per drink — no safe threshold exists. See how estrogen, DNA damage, and BRCA status amplify that risk.
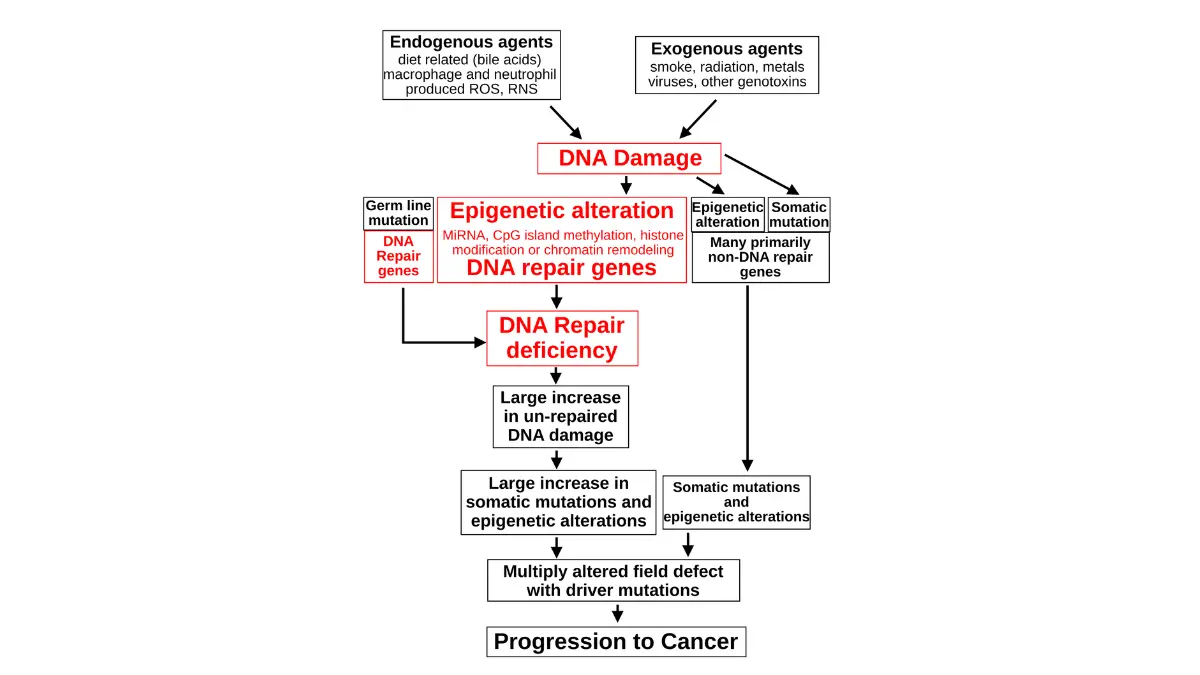
Figure: DNA damage and carcinogenesis progression from DNA repair deficiency to cancer development. Adapted from Wikimedia Commons Diagram Damage to Cancer Wiki 300dpi, licensed under CC BY-SA 3.0.
What does alcohol actually do to your breast cancer risk?
Alcohol and breast cancer risk are not loosely associated — alcohol is a confirmed Group 1 carcinogen, meaning the scientific evidence for causation meets the highest classification standard used by international regulatory bodies. This is not a matter of ongoing debate.
ℹ️ Medical Disclaimer: The diagnostic criteria, risk quantification data, treatment interaction information, and medication guidance discussed in this article reflect current 2026 clinical evidence and are provided for educational purposes only. Individual breast cancer risk, screening frequency decisions, treatment modifications, and alcohol cessation plans depend on factors including personal medical history, genetic profile, tumor subtype, comorbidities, and specialist assessment. Consult a board-certified gynecologic oncologist, medical oncologist, or primary care physician before acting on any clinical information in this article — including decisions about alcohol cessation during active treatment.
How alcohol damages breast tissue at the cellular level
Alcohol raises breast cancer risk through three confirmed biological pathways — and understanding them changes how seriously you take the phrase “just one drink.”
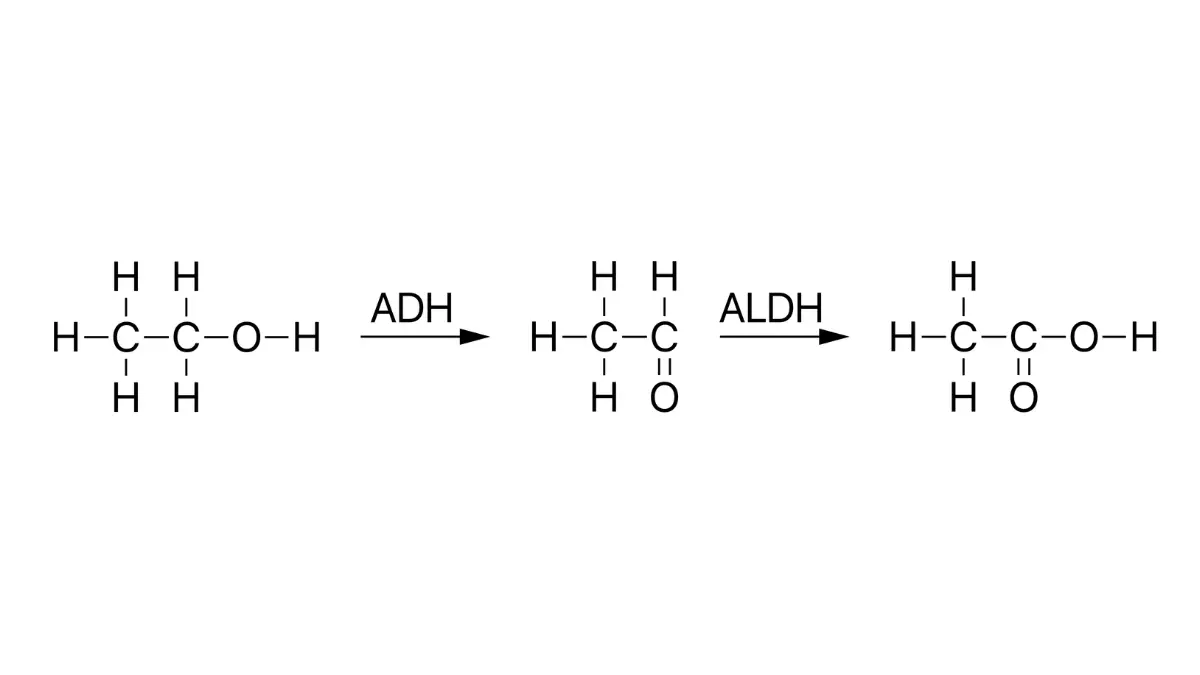
🔬 How It Works: When you drink, your body converts ethanol to acetaldehyde via an enzyme called alcohol dehydrogenase. Acetaldehyde is a direct-acting carcinogen that forms structural bonds with your DNA — called DNA adducts — inside breast epithelial cells. These adducts disrupt the normal copying of genetic information, creating the mutations that can trigger cancerous growth.
Figure: Ethanol metabolism pathway showing ADH and ALDH enzymatic conversion of ethanol to acetaldehyde and acetate. Adapted from Wikimedia Commons Ethanol metabolism, released into the public domain.
At the same time, ethanol independently upregulates aromatase, the enzyme that converts androgens to estrogen in hepatic and adipose tissue. This raises circulating estradiol, which acts as a growth signal for estrogen receptor-positive breast tumors. A third pathway compounds the first two: alcohol depletes folate, a nutrient essential to the DNA methylation and repair process that corrects damage before it becomes permanent.
These three pathways operate simultaneously and independently. A patient in my practice once asked whether cutting back to weekends “resets” the damage. The honest answer is that acetaldehyde exposure is cumulative, not episodic — the molecular insults accumulate even when drinking is intermittent.
For a complete picture of modifiable and non-modifiable breast cancer risk factors, the mechanisms covered here connect to a broader risk profile your physician should review with you.
📊 Clinical Data Point: Ethanol is classified as a Group 1 carcinogen by the International Agency for Research on Cancer (IARC) — the highest tier of carcinogen classification, indicating sufficient evidence of causation in humans. Source: IARC Monographs on the Identification of Carcinogenic Hazards to Humans, 2026 current classification.
How much does alcohol actually raise your breast cancer risk?
Each additional alcoholic drink consumed daily raises breast cancer risk by approximately 7–10%, according to 2026 NCI dose-response analysis — a risk that accumulates linearly with each additional drink.
📊 Clinical Data Point: Dose-response analysis from 2026 NCI and updated World Cancer Research Fund data confirms: each daily alcoholic drink raises breast cancer risk approximately 7–10%. Women consuming 3 or more drinks per day face up to 50% elevated relative risk compared to non-drinkers. Estimated alcohol-attributable breast cancer diagnoses in the US annually: approximately 44,000. Source: National Cancer Institute, alcohol and cancer risk data, 2026; World Cancer Research Fund International, 2026 Continuous Update Project.
The dose-response relationship: 1 drink, 2 drinks, 3+ drinks per day
Daily Drinks
Approximate Relative Risk Increase
Subtype Most Affected
Key Clinical Detail
1 drink/day
~7–10%
ER-positive
Risk begins with light consumption — no zero-risk threshold established
2 drinks/day
~14–20%
ER-positive, PR-positive
Aromatase pathway compound effect at sustained intake
3+ drinks/day
Up to ~50%
All subtypes, ER-positive highest
Acetaldehyde burden + estrogen elevation both clinically significant
Source: NCI 2026 dose-response data
Is any amount of alcohol truly safe for breast cancer risk?
The honest answer based on 2026 evidence: no safe lower threshold has been established. The dose-response relationship is approximately linear, meaning a woman drinking three glasses of wine per week faces a materially different risk elevation than a woman drinking three per day — but neither is at zero risk from alcohol.
This is not cause for catastrophizing a glass of champagne at a wedding. It is cause for an informed, honest conversation with your physician about where alcohol fits in your personal risk picture.
✅ Patient Action: Women consuming three or more alcoholic drinks per day should ask their primary care physician or board-certified oncologist for a formal breast cancer risk assessment — including a discussion of whether your alcohol intake, combined with other factors like BMI and family history, places you in a higher-screening-frequency category.
Does alcohol hit hormone receptor-positive breast cancer harder?
Alcohol is a particularly dangerous risk factor for women with estrogen receptor-positive (ER+) breast cancer because ethanol directly upregulates aromatase — the enzyme responsible for producing the estrogen that fuels ER-positive tumor growth.
ER-positive and PR-positive tumors: why anything that raises estrogen raises your risk
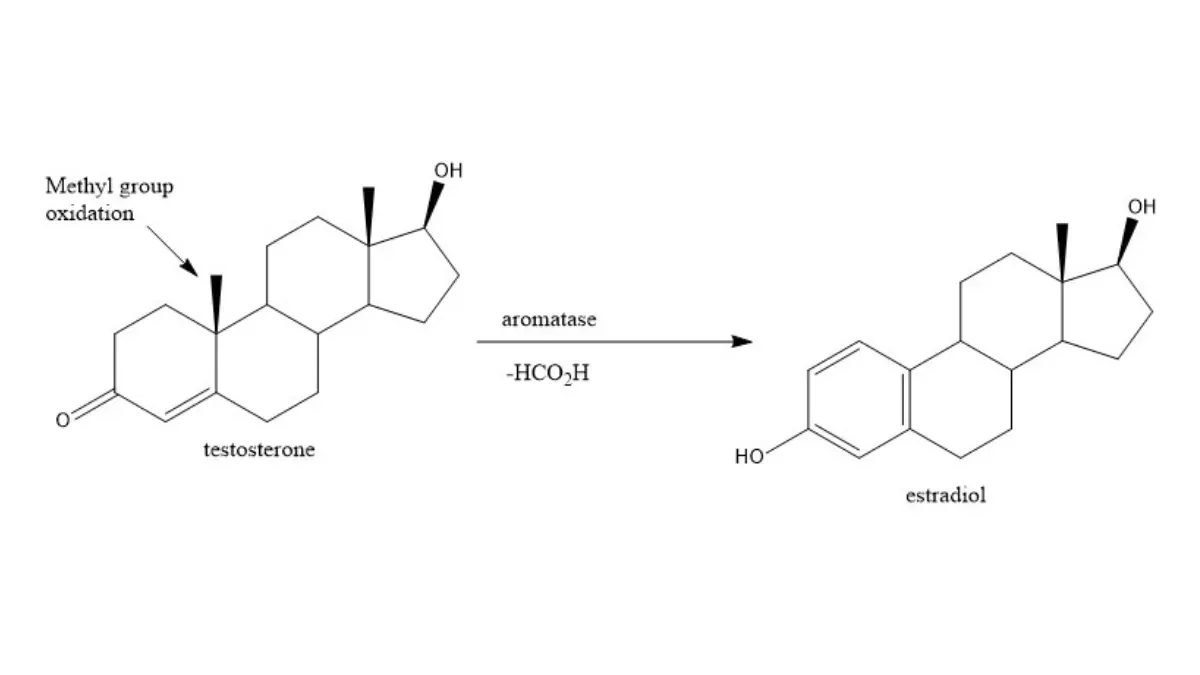
Figure: Aromatase-mediated conversion of testosterone to estradiol. Adapted from Wikimedia Commons Estradiol synthesis, licensed under CC BY-SA 4.0.
The aromatase pathway makes alcohol mechanistically distinct from most other lifestyle risk factors for ER-positive disease. When ethanol upregulates hepatic and peripheral aromatase, the result is increased conversion of androgens to estradiol in breast tissue, liver, and adipose tissue. For a woman with ER-positive breast cancer, that elevated estradiol is a direct growth signal at the tumor’s own receptor — not a distant environmental insult, but a molecular accelerant at the point of disease.
ER-positive breast cancer accounts for the large majority of US breast cancer diagnoses, making this the pathway that affects the greatest number of patients. PR-positive tumors share this vulnerability through related hormonal signaling.
🩺 Physician Note: When I counsel a patient newly diagnosed with ER-positive disease who drinks moderately, the conversation is direct: the alcohol you are consuming is biochemically feeding the mechanism your cancer depends on. Cessation is not a lifestyle suggestion in this context — it is a treatment-adjacent decision. I tell patients this not to generate guilt about the past, but to give them real agency over their biology going forward.
HER2-positive and triple-negative patients: the acetaldehyde pathway still applies
Women with HER2-positive breast cancer or triple-negative breast cancer do not have the estrogen amplification mechanism — but alcohol’s acetaldehyde-mediated DNA damage pathway applies to all breast cancer subtypes. The magnitude is different; the risk is not absent.
✅ Patient Action: Patients with confirmed ER-positive or PR-positive breast cancer should discuss alcohol cessation urgently with their board-certified gynecologic oncologist or medical oncologist — specifically ask: “Does my alcohol intake counteract any aspect of my hormonal therapy?”
Who faces the highest alcohol-related breast cancer risk?
Alcohol’s carcinogenic effect is not uniform across all women — four specific profiles face compounded risk that the standard 7–10% per-drink figure does not fully capture.
BRCA1 and BRCA2 carriers: does alcohol make genetic risk significantly worse?
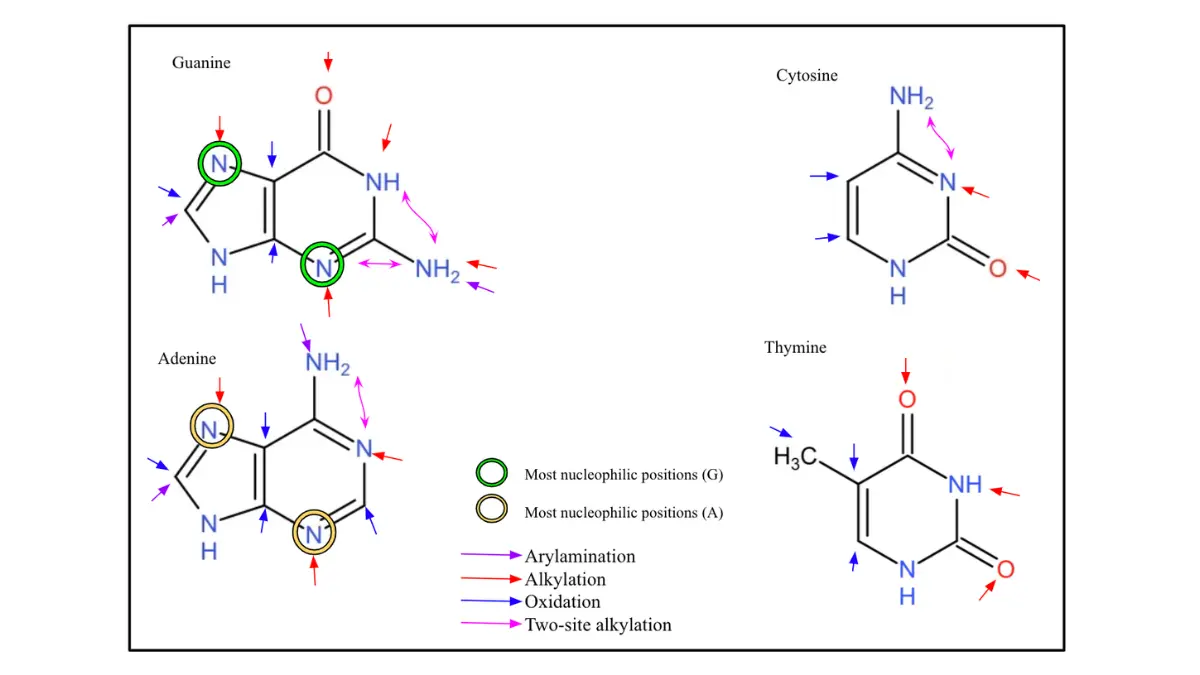
BRCA1 and BRCA2 proteins are essential components of the homologous recombination DNA repair pathway — the same pathway responsible for correcting acetaldehyde-induced DNA adducts in breast epithelial cells. In women with BRCA1/BRCA2 mutations, this repair mechanism is structurally compromised.
The clinical consequence: the same amount of alcohol produces more net DNA damage in a BRCA carrier than in a non-carrier, because the molecular machinery that would normally repair that damage is deficient by genetic design. The risk amplification is mechanistic, not merely statistical.
Figure: Nucleic acid DNA adduct formation showing nucleophilic attack positions on DNA bases. Adapted from Wikimedia Commons Nucleic Acids in DNA Adduct Formation, licensed under CC BY-SA 4.0.
📊 Clinical Data Point: BRCA1 and BRCA2 mutations impair homologous recombination DNA repair — the pathway that corrects acetaldehyde-mediated DNA adduct damage from alcohol. This represents a mechanistic compounding of alcohol-related breast cancer risk in BRCA carriers beyond the population-level dose-response figures. Source: NCI genetic and environmental cancer risk interaction data, 2026.
Postmenopausal women, HRT users, and high BMI: stacking the risk factors
Three additional profiles face compounded risk through the shared estrogen-amplification pathway.
Postmenopausal women on hormone replacement therapy (HRT): Both HRT and alcohol independently raise circulating estrogen. Used together, they create additive estrogen loading that exceeds either factor alone — a compounding effect any prescribing physician should discuss explicitly with patients who drink.
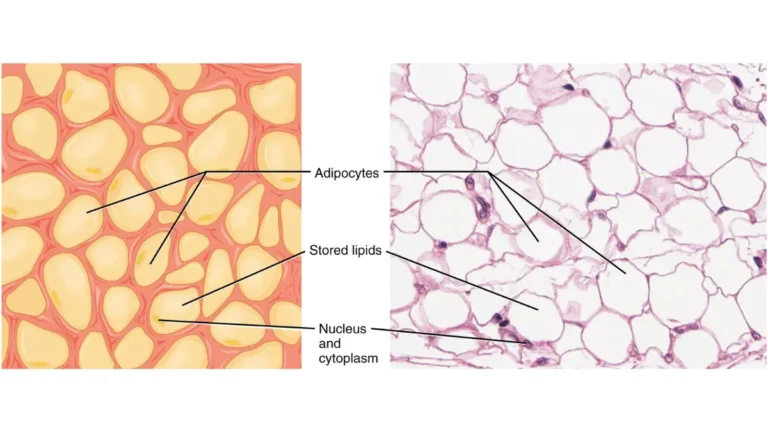
Women with BMI above 30: Adipose tissue is itself a site of aromatase activity. Women with elevated body fat already carry higher baseline aromatase output and circulating estrogen. Alcohol raises aromatase activity further, compounding an already elevated hormonal environment. Calculate your BMI using our free BMI Calculator to understand where you sit on this co-risk factor.
Long-duration heavy drinkers: Cumulative acetaldehyde exposure — measured in years and decades, not individual episodes — determines the total DNA damage burden. Duration matters alongside quantity.
📊 Clinical Data Point: The CDC alcohol and public health data tracks alcohol-attributable cancer mortality annually, including breast cancer-specific burden. Source: CDC alcohol and public health surveillance data, 2026.
✅ Patient Action: BRCA1 or BRCA2 mutation carriers who drink any amount of alcohol should consult a board-certified genetic counselor and a gynecologic oncologist — ask specifically: “Given my BRCA status and my drinking history, what does my individualized breast cancer risk profile look like, and does alcohol cessation change my risk-reduction plan?”
Can stopping drinking actually lower your breast cancer risk?
2026 prospective evidence confirms that women who achieve sustained alcohol cessation experience a measurable reduction in breast cancer risk — with hormonal biomarker improvements detectable within months and statistically significant risk reduction observed over years of abstinence.
This is the question most patients have been building toward since they opened this article. The answer is yes — and it is grounded in biology, not optimism.
What 2026 research shows about risk reversal after stopping drinking
When alcohol is removed, three things happen in sequence. Aromatase activity begins to normalize, reducing circulating estradiol. Folate levels recover, restoring DNA methylation and repair capacity. And the ongoing accumulation of acetaldehyde-mediated DNA adducts stops.
🩺 Physician Note: In my practice, patients who commit to sustained cessation — not reduction to “moderate,” but complete cessation — report measurable changes in energy, sleep quality, and hormonal symptoms within weeks. Clinically, I track biomarker changes at their three-month follow-up. The hormonal normalization is real, and it matters biologically for ER-positive patients in particular.
The evidence is clearer for complete cessation than for reduction. Cutting from three drinks per day to one is not equivalent to stopping — the aromatase upregulation and acetaldehyde accumulation pathways remain active at lower doses.
Practical steps your physician would recommend for alcohol reduction
Discuss a structured cessation timeline with your primary care physician — abrupt cessation is safe for most social drinkers but warrants medical guidance if your intake is high.
Add folate-rich foods — leafy greens, legumes, fortified grains — to accelerate the restoration of DNA repair capacity.
Use the cessation window intentionally. The months after stopping are when hormonal biomarkers shift most rapidly — this is also when breast cancer prevention strategies for diet and lifestyle have their highest impact.
Schedule a breast cancer risk reassessment with your physician at six months post-cessation, specifically to revisit your screening frequency.
✅ Patient Action: Women who drink regularly and want to lower their breast cancer risk should ask their primary care physician or board-certified internist: “Given my drinking history and my other risk factors, what is the most evidence-based cessation strategy for me, and when should I expect my next screening to reflect a reduced-risk profile?”
If you have breast cancer, should you drink during treatment?
As a gynecologic oncologist, I am asked about alcohol during treatment more often than almost any other lifestyle question. The answer has a pharmacological precision that matters — and “just don’t drink” understates why.
Alcohol and tamoxifen: the CYP2D6 interaction your oncologist may not explain
Tamoxifen is a prodrug. It requires hepatic conversion via the CYP2D6 enzyme pathway to produce its active metabolite, endoxifen — the compound responsible for blocking estrogen receptors in tumor cells. Chronic alcohol intake inhibits CYP2D6 enzyme activity.
The clinical consequence: reduced CYP2D6 function from alcohol use may lower endoxifen plasma concentrations, potentially compromising tamoxifen’s therapeutic efficacy. You may be taking the drug correctly and still receiving a subtherapeutic benefit because alcohol is suppressing its activation. This is why I tell patients: drinking while on tamoxifen is not a lifestyle choice — it may be affecting your treatment response.
For a complete comparison of tamoxifen versus aromatase inhibitors and how each works, that article covers the mechanism and selection criteria in detail.
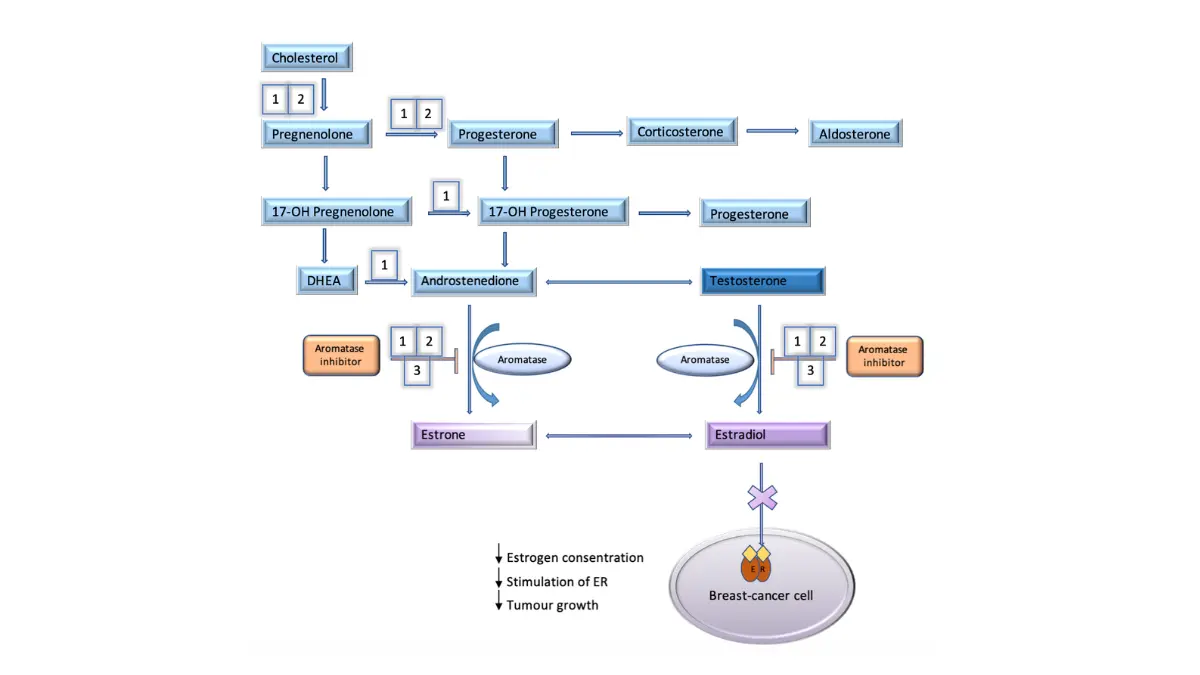
⚠️ Clinical Warning: Alcohol combined with aromatase inhibitor therapy creates direct pharmacological opposition. Aromatase inhibitors work by suppressing estrogen production — alcohol raises estrogen by upregulating the same aromatase enzyme the drug is designed to inhibit. Drinking during aromatase inhibitor therapy is not a minor lifestyle concern; it may be actively undermining your treatment’s mechanism of action.
Figure: Metabolic pathways of estrogen production showing aromatase enzyme action and inhibitor blockade. Adapted from Wikimedia Commons Metabolic pathways of estrogen production, licensed under CC BY-SA 4.0.
Alcohol during chemotherapy: why even moderate drinking complicates treatment
During breast cancer chemotherapy, alcohol presents three compounding risks. It increases hepatotoxic burden on a liver already processing cytotoxic agents. It may worsen chemotherapy-induced peripheral neuropathy, which is already a common and distressing side effect. And it may impair immune reconstitution between treatment cycles, when your body’s ability to recover is critical.
📊 Clinical Data Point: Alcohol-drug interactions in oncology patients are documented in current NCI breast cancer pharmacological guidelines. Source: NCI breast cancer treatment information — current 2026 guideline edition.
✅ Patient Action: Any patient currently receiving tamoxifen, aromatase inhibitors, or chemotherapy for breast cancer must ask their treating oncologist at their next appointment: “Does my alcohol intake affect the efficacy or safety of my specific treatment regimen?” Do not consume any alcohol during active treatment without this explicit conversation.
Frequently asked questions about alcohol and breast cancer risk
1. Does alcohol cause breast cancer?
Yes. Alcohol is classified as a Group 1 carcinogen by the International Agency for Research on Cancer — the highest classification tier, indicating sufficient evidence of direct causation in humans, not merely association. Alcohol and breast cancer risk are linked through three confirmed biological pathways: acetaldehyde-mediated DNA damage, aromatase-driven estrogen elevation, and folate depletion that impairs DNA repair. The risk is dose-dependent and begins with even light consumption.
2. How much does alcohol increase breast cancer risk?
Each alcoholic drink consumed daily raises breast cancer risk by approximately 7–10%, according to 2026 NCI dose-response analysis. Women drinking three or more drinks per day face up to 50% elevated relative risk compared to non-drinkers. The relationship is approximately linear — each additional daily drink adds measurable risk. No safe lower threshold for alcohol and breast cancer risk has been established in current 2026 evidence.
3. Is red wine safer than beer or spirits for breast cancer risk?
No. The active carcinogen in all alcoholic beverages is ethanol — the same molecule regardless of the beverage type. Red wine’s polyphenols, including resveratrol, have been studied but do not neutralize ethanol’s carcinogenic effects on breast tissue in human clinical data. Your alcohol and breast cancer risk is determined by how much ethanol you consume, not by which drink delivers it. Beer, wine, and spirits carry equivalent risk per standard drink.
4. Does alcohol affect hormone receptor-positive breast cancer differently?
Yes — significantly. Alcohol raises estrogen levels by upregulating aromatase, the enzyme that produces estradiol. For women with ER-positive or PR-positive breast cancer, this elevated estrogen is a direct growth signal for their tumor subtype. Alcohol is a higher-magnitude risk factor for hormone receptor-positive disease than for other subtypes, because the estrogen-amplification pathway is specific to ER-positive and PR-positive tumors. Consult a board-certified gynecologic oncologist or medical oncologist about alcohol cessation if your diagnosis is ER-positive or PR-positive.
5. Can stopping drinking lower my breast cancer risk?
Yes. Sustained alcohol cessation produces measurable biological changes: aromatase activity normalizes, circulating estradiol decreases, and folate-dependent DNA repair capacity recovers. Hormonal biomarker improvements are detectable within months of stopping. Statistically meaningful breast cancer risk reduction has been observed over years of sustained abstinence in prospective data. Complete cessation shows stronger benefit than reduction to moderate drinking. Consult a primary care physician or board-certified internist to build a physician-supervised cessation plan.
6. How does alcohol raise estrogen levels?
Ethanol upregulates aromatase — the enzyme that converts androgens to estrogen — in hepatic and adipose tissue, increasing circulating estradiol throughout the body. This effect is detectable at moderate drinking levels and compounds with other estrogen-raising factors, including excess body weight and hormone replacement therapy. For women with ER-positive breast cancer, this aromatase upregulation is a direct mechanism linking alcohol and breast cancer risk at the tumor biology level, not just at the population statistics level.
7. Should breast cancer survivors drink alcohol?
Current 2026 oncology guidance strongly recommends alcohol avoidance for breast cancer survivors, particularly those with ER-positive disease or those on hormonal therapy. Even light drinking raises breast cancer recurrence risk through the estrogen pathway and may compromise tamoxifen or aromatase inhibitor efficacy through pharmacological interference. The risk is not theoretical — it is mechanistically specific to the treatment regimens most survivors are on. Consult your treating oncologist specifically about alcohol and breast cancer recurrence risk before resuming any drinking.
8. Does alcohol interact with tamoxifen?
Yes — through a clinically significant pharmacological mechanism. Tamoxifen requires hepatic conversion via the CYP2D6 enzyme to its active metabolite, endoxifen. Chronic alcohol intake inhibits CYP2D6 activity, which may reduce endoxifen plasma concentrations and compromise tamoxifen’s therapeutic efficacy. This is not a minor drug interaction warning — it may mean your cancer treatment is delivering subtherapeutic benefit. Any patient on tamoxifen must consult their treating oncologist before consuming any amount of alcohol.
9. What is a safe amount of alcohol for BRCA1 or BRCA2 mutation carriers?
No established safe threshold exists for BRCA1 or BRCA2 carriers. The BRCA1/2 DNA repair deficit means that acetaldehyde damage from alcohol is repaired less efficiently than in non-carriers — because the homologous recombination pathway that repairs these DNA adducts is structurally compromised by the mutation. The risk amplification is mechanistic, not merely additive. Current clinical guidance recommends complete alcohol avoidance for confirmed BRCA carriers. Consult a board-certified genetic counselor and gynecologic oncologist to build an individualized risk management plan.
10. Does drinking during chemotherapy affect treatment outcomes?
Yes — through three compounding mechanisms. Alcohol increases hepatotoxic burden on a liver already processing cytotoxic chemotherapy agents. It may worsen chemotherapy-induced peripheral neuropathy, which is already a common treatment side effect. And it may impair immune reconstitution between treatment cycles, reducing the body’s ability to recover between doses. Even moderate drinking during active breast cancer chemotherapy is not considered clinically safe. Any patient in active chemotherapy must consult their oncologist before consuming any alcohol whatsoever.
11. How many breast cancer cases are linked to alcohol each year in the US?
Current NCI and CDC data estimate approximately 44,000 US breast cancer diagnoses annually are attributable to alcohol — making alcohol and breast cancer risk one of the most significant modifiable risk factors in oncology. This represents a meaningful portion of the roughly 300,000+ new US breast cancer diagnoses each year. Importantly, this burden is entirely preventable — unlike genetic risk factors, alcohol consumption is a modifiable behavior that can be addressed through cessation.
What to do now with this information
Alcohol and breast cancer risk is the rare category of cancer risk where one clear, modifiable action — stopping or significantly reducing alcohol — produces measurable biological benefit within months.
Three facts deserve to leave this article with you. First, alcohol is a confirmed carcinogen with a dose-dependent relationship to breast cancer, not a contested association. Second, if you have ER-positive disease or are on tamoxifen or aromatase inhibitors, alcohol is not a lifestyle choice — it has direct mechanistic relevance to your treatment and your tumor biology. Third, cessation works. The biological mechanisms that make alcohol dangerous are the same mechanisms that normalize when drinking stops.
If you drink regularly and have any personal or family history of breast cancer, understanding your full breast cancer risk reduction options is the logical next step after this conversation. For survivors navigating what comes after treatment, our guide to life after breast cancer addresses the long-term risk modification questions that matter most.
Schedule that conversation with your physician this week — not to generate guilt about past choices, but to build a forward-looking plan specific to your biology.
How this was made
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.
Researched and written from recognised health sources
Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Important notice
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.