On This Page – Quick Medical Summary
What breast cancer clinical trials mean for your treatment options
Breast cancer clinical trials are research studies that test new treatments, new combinations of approved therapies, or new approaches to surgery and supportive care in patients with confirmed diagnoses. They are not last resorts. They are not experiments without oversight. Every treatment considered standard of care for breast cancer today was first proven to work through exactly this process.
📊 Clinical Data Point: More than 310,000 new invasive breast cancer diagnoses are projected in US women in 2026, making it the most commonly diagnosed cancer in American women. — Source: American Cancer Society 2026 breast cancer statistics
If you are still tracking unexplained symptoms, use our Symptom Checker to organize your history before your first oncology appointment. For a full clinical foundation, our guide to breast cancer stages and survival rates explains what each diagnosis stage means for your treatment path before you evaluate any trial option.
ℹ️ Medical Disclaimer: The clinical trial phase descriptions, eligibility criteria, enrollment procedures, experimental therapy information, insurance coverage rules, and patient rights discussed in this article reflect current 2026 clinical guidelines and federal law and are provided for educational purposes only. Individual eligibility for any specific clinical trial is determined by the trial’s principal investigator through a formal screening process — not by patient self-assessment. Treatment decisions, medication choices, and enrollment decisions depend on individual diagnosis, cancer subtype, comorbidities, prior treatment history, and specialist evaluation. Consult a board-certified oncologist or gynecologic oncologist before acting on any clinical information in this article.
The four phases of breast cancer clinical trials explained
Breast cancer clinical trials are conducted in four phases, each designed to answer a different scientific question about a new therapy:
| Phase | Primary Goal | Typical Enrollment | What It Means for You |
|---|---|---|---|
| Phase I | Safety — establishing maximum tolerated dose | 20–80 patients | Highest uncertainty — tests whether the drug is safe, not whether it works |
| Phase II | Preliminary efficacy and optimal dosing in a specific cancer type | 100–300 patients | Early signal of activity; still limited safety data for large populations |
| Phase III | Efficacy vs. standard-of-care in a large randomized controlled trial | 300–3,000+ patients | Direct head-to-head with current best treatment — the trial closest to a normal treatment experience |
| Phase IV | Long-term safety surveillance after FDA approval | Thousands | Drug is already approved — monitors for rare or delayed adverse effects |
📊 Clinical Data Point: Phase III breast cancer clinical trials must demonstrate a statistically significant improvement in progression-free survival or overall survival versus the standard-of-care comparator arm to meet FDA approval requirements. — Source: NCI breast cancer treatment guidelines
Phase I and Phase II: testing safety and early efficacy signals
Phase I trials are not designed to test whether a drug works. Their primary endpoint is the maximum tolerated dose, established by administering the experimental agent in progressively higher amounts to small patient cohorts.
Most patients who are currently in treatment and considering a trial are best suited for Phase II or Phase III — not Phase I. Phase I carries a level of therapeutic uncertainty that requires specialist-level risk assessment before any enrollment decision.
🔬 How It Works: In a Phase I dose-escalation design, small cohorts receive progressively higher doses of an experimental agent. Researchers monitor for dose-limiting toxicities — adverse effects severe enough to halt further dose increases. The dose just below that threshold becomes the maximum tolerated dose carried into Phase II testing.
Phase III and Phase IV: large-scale comparison against standard of care
Phase III trials randomize patients to either the experimental arm or the control arm. In breast cancer Phase III trials, the control arm is almost never a placebo — it is the current standard-of-care regimen. A Phase IV trial monitors a therapy that is already FDA-approved for long-term or rare adverse effects not captured in pre-approval studies.
What it means when your oncologist recommends a Phase III trial specifically
When a specialist recommends a Phase III trial, they are telling you that the experimental therapy has cleared Phase I and Phase II review and that sufficient preliminary evidence exists to test it against existing best treatment in a large patient population. Understanding what those benchmarks look like in your diagnosis context helps you evaluate the comparison — review breast cancer survival rates by stage for the current clinical picture.
✅ Patient Action: Before enrolling in a Phase I trial, ask your oncologist: “What is the primary endpoint of this trial — dose-finding or efficacy — and what are the documented safety findings from Phase I data on related compounds in this drug class?” This question establishes whether you are entering a safety study or a benefit study, which changes the risk calculus completely. Consult a board-certified oncologist before enrolling in any Phase I trial to review the dose-escalation protocol and your prior treatment history.
Who qualifies for breast cancer clinical trials: eligibility criteria
Eligibility for breast cancer clinical trials is determined by a combination of inclusion and exclusion criteria established by the trial sponsor and verified through formal screening by the principal investigator. Most trials require confirmation of the following before screening begins:
- Confirmed breast cancer diagnosis with pathology documentation of subtype (ER, PR, and HER2 status)
- Defined number of prior treatment lines received (most Phase III trials specify first-line, second-line, or later-line eligibility)
- Confirmed biomarker testing results where required — BRCA mutation status, HER2 amplification, PD-L1 expression, or comprehensive genomic profiling
- ECOG performance status within the trial’s specified threshold (typically ECOG 0–2 for Phase II and Phase III trials)
- Adequate organ function — kidney, liver, cardiac, and bone marrow function within protocol-defined laboratory ranges
Common inclusion criteria: stage, confirmed subtype, and prior treatment lines
Eligibility criteria are highly trial-specific, but the framework above applies broadly across most Phase II and Phase III breast cancer trials in 2026. Stage, histologic subtype, and the number of prior systemic therapies received are the three most consistent gatekeepers.
Some trials require biomarker confirmation by a CLIA-certified laboratory before the screening visit — your pathology report alone is not always sufficient. If your BRCA mutation status has not been formally tested, knowing that result can significantly expand your trial options. Learn what a positive BRCA gene test result means for your treatment planning, and use our Genetic Risk Assessment Tool to understand your hereditary breast cancer risk profile before your eligibility screening appointment.
Common exclusion criteria: performance status, organ function, and washout periods
Exclusion criteria protect patient safety. Most trials exclude patients with active central nervous system metastases, significant organ dysfunction, prior exposure to the same drug class being tested, or inadequate washout periods after recent chemotherapy — typically 21 to 28 days.
🩺 Physician Note: “In my clinical experience, the exclusion criterion patients most often overlook is the washout period. A patient who just finished a chemotherapy cycle may be clinically eligible in every other respect but cannot enroll until the minimum time since last treatment has passed. I always ask patients who are interested in a trial to tell me the exact date of their last systemic treatment — that single piece of information often determines whether we’re looking at a two-week window or an eight-week wait.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
What ECOG performance status is and how to ask your doctor about yours
ECOG performance status is a standardized 0–4 scale used by oncologists and trial investigators to measure a patient’s level of daily function. Most Phase II and Phase III trials require an ECOG score of 0, 1, or 2.
| ECOG Score | Functional Status | Trial Eligibility Impact |
|---|---|---|
| 0 | Fully active — no restriction on activity | Eligible for most Phase I, II, and III trials |
| 1 | Restricted in strenuous activity; ambulatory; able to carry out light work | Eligible for most Phase II and III trials |
| 2 | Ambulatory; capable of self-care; unable to carry out work; up >50% of waking hours | Eligible for select Phase II trials; Phase I eligibility varies |
| 3 | Limited self-care; confined to bed or chair >50% of waking hours | Generally excluded from most interventional trials |
| 4 | Completely disabled; unable to carry out any self-care | Generally excluded from all interventional trials |
✅ Patient Action: Ask your oncologist at your next appointment: “What is my current ECOG performance status score, and does that score qualify me for the Phase II or Phase III trials you are considering?” Most patients do not know this score exists — asking by name signals clinical self-advocacy and opens a more specific eligibility conversation. Consult a board-certified oncologist before assuming you are ineligible based on any single criterion — many eligibility thresholds have protocol-specific exceptions for patients with stable comorbidities.
How to find and enroll in a breast cancer clinical trial: step by step
Enrolling in a breast cancer clinical trial involves five steps, beginning with a targeted search on ClinicalTrials.gov, the NCI’s federally maintained registry of every active US clinical trial:
- Search ClinicalTrials.gov — filter by condition (“breast cancer”), recruiting status (“recruiting”), phase (II or III for most patients), and ZIP code to generate a relevant shortlist within your geographic reach
- Review the eligibility criteria for each result — the “Eligibility” tab lists inclusion and exclusion criteria in full; compare them against your pathology report and treatment history
- Contact the trial site — call the listed study coordinator and request a formal screening appointment; bring your complete medical records and pathology documentation
- Complete formal screening — the trial team will review your records, confirm your biomarker status if required, and determine whether you meet all inclusion criteria
- Review and sign the informed consent document — the final step before enrollment; the document is IRB-reviewed and must explain all known risks, the randomization process, and your right to withdraw at any time
🩺 Physician Note: “In my practice, I walk patients through the ClinicalTrials.gov search interface during our consultation — most are surprised to discover they can filter simultaneously by cancer type, ZIP code, and phase, narrowing hundreds of listings to a relevant shortlist in under three minutes. The filter that most patients miss is ‘Study Results’ — filtering for trials that have results posted shows you which investigators at which centers have the most active research records in your subtype.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
Step 1: Search ClinicalTrials.gov by subtype, stage, and location
The NCI maintains ClinicalTrials.gov as the authoritative federal registry for all active US clinical trials. Use the condition field (“breast cancer” or the specific subtype), the recruiting status filter, and the ZIP code or distance field together. Save the NCT number of any trial you want to discuss — that number is the unique identifier your oncologist will use to pull the protocol.
Some surgical trials evaluate new margin protocols alongside systemic therapy — patients already researching lumpectomy versus mastectomy outcomes may find relevant surgical trials within the same ClinicalTrials.gov search results.
Step 2: Contact the trial site and request a screening appointment
The study coordinator listed on each ClinicalTrials.gov entry is your direct point of contact. Have your diagnosis date, pathology report summary (ER/PR/HER2 status, grade, stage), and prior treatment history ready for that initial call.
Step 3: Understanding informed consent — what you’re agreeing to and your right to withdraw
Informed consent is an IRB-reviewed legal document — not a contract. It must disclose all known risks of the experimental treatment, the randomization process, which treatment you will receive if assigned to the control arm, and the Data Safety Monitoring Board’s stopping rules. You have the federally protected right to withdraw from a clinical trial at any time, for any reason, without any penalty to your access to standard medical care. That right cannot be waived.
✅ Patient Action: Before signing the informed consent form, ask the principal investigator two specific questions: “What is the randomization ratio, and if I am assigned to the control arm, will I receive the current NCCN 2026 standard-of-care regimen or a modified version?” and “If the experimental arm demonstrates superior results mid-trial, will crossover to the experimental therapy be offered to control arm patients?” Consult a board-certified oncologist before signing any informed consent document for a clinical trial.
Active breast cancer clinical trials in 2026: what’s available by subtype
In 2026, the most active breast cancer clinical trial categories concentrate in three subtype-specific areas, each driven by a distinct therapeutic mechanism:
| Subtype | Primary 2026 Trial Focus | Key Drug Classes | Best For Patient Profile |
|---|---|---|---|
| HER2-positive | Antibody-drug conjugates (ADCs), bispecific antibodies, novel HER2-directed combinations | Trastuzumab deruxtecan (T-DXd), HER2-targeted bispecifics | HER2-amplified patients who have received prior HER2-directed therapy |
| Triple-negative (TNBC) | Checkpoint immunotherapy combinations, PARP inhibitors, ADC-immunotherapy doublets | Pembrolizumab combinations, olaparib, talazoparib | PD-L1-positive (CPS ≥10) or BRCA1/2-mutated TNBC patients |
| HR-positive/HER2-negative | CDK4/6 inhibitor backbone combinations, AKT/PI3K pathway inhibitors, novel endocrine strategies | Ribociclib, abemaciclib, palbociclib combinations; alpelisib | Metastatic or endocrine-resistant ER-positive patients |
📊 Clinical Data Point: The FDA’s 2026 breast cancer drug approval activity has been concentrated in the HER2-positive indication, with multiple ADC and bispecific antibody programs advancing through late-stage trials. — Source: FDA-approved breast cancer therapies
HER2-positive breast cancer trials: antibody-drug conjugates and bispecific antibodies
HER2-positive breast cancer has the most technically sophisticated trial landscape in 2026. Antibody-drug conjugates exploit HER2 receptor overexpression as a delivery mechanism — the antibody binds to HER2, and the conjugated cytotoxic payload is released directly inside the tumor cell. This mechanism produces responses in tumors that have developed resistance to standard HER2 receptor blockade. For a full clinical overview of HER2-positive disease and current approved treatment options, see our dedicated guide to HER2-positive breast cancer.
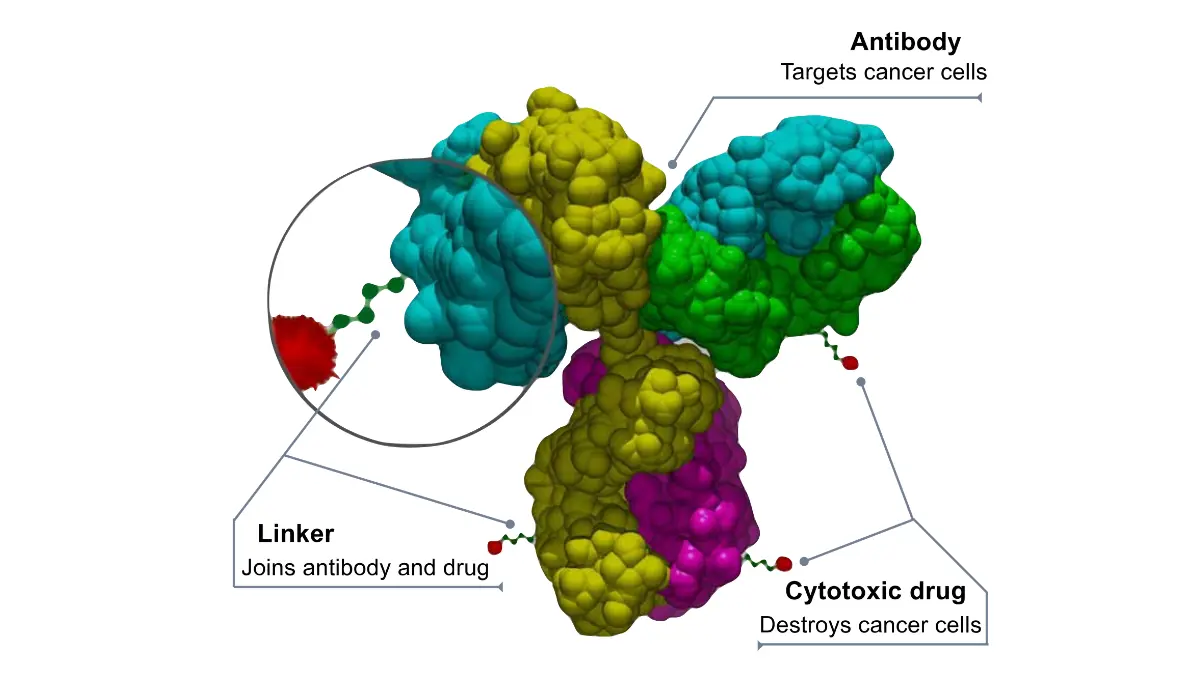
🔬 How It Works: An antibody-drug conjugate (ADC) consists of three components: a monoclonal antibody targeting a tumor surface protein (HER2 in this case), a linker molecule, and a cytotoxic drug payload. When the antibody binds to the HER2 receptor on the cancer cell surface, the entire complex is internalized, the linker cleaves inside the cell, and the cytotoxic payload is released — delivering a concentrated dose of chemotherapy directly within the tumor cell while limiting systemic toxicity.
Triple-negative breast cancer trials: checkpoint inhibitors and PARP inhibitors
Triple-negative breast cancer has the largest active immunotherapy trial pool in 2026. TNBC lacks estrogen receptor, progesterone receptor, and HER2 overexpression — the absence of targetable receptors means immune activation strategies become the primary investigational focus. Eligibility for checkpoint inhibitor trials typically requires PD-L1 expression confirmed by combined positive score (CPS), with CPS ≥10 representing the threshold where pembrolizumab combinations have demonstrated the strongest Phase III response data. BRCA1/2-mutated TNBC patients have additional eligibility for PARP inhibitor trials. Our guide to triple-negative breast cancer covers the current treatment landscape for patients with this subtype.
HR-positive/HER2-negative and metastatic breast cancer: CDK4/6 and novel endocrine strategies
HR-positive/HER2-negative trial activity in 2026 focuses on overcoming acquired endocrine resistance in the metastatic setting — the point at which CDK4/6 inhibitor combinations stop controlling disease and next-line options are required. Novel PI3K/AKT pathway inhibitors, oral selective estrogen receptor degraders (SERDs), and antibody-drug conjugates targeting alternative receptors are all in active Phase III evaluation.
🩺 Physician Note: “I want patients to understand that subtype-specific eligibility in 2026 trials is far more granular than just ER-positive or HER2-positive. In my clinical practice, I have seen patients denied screening eligibility because their biomarker testing was incomplete — specifically, PD-L1 expression by the required assay platform was not part of their original pathology workup. Confirm with your oncologist whether your current biomarker profile matches the specific assay requirements listed in any trial’s eligibility criteria before traveling to a screening appointment.” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
For patients managing advanced or metastatic breast cancer, understanding which systemic therapies are already approved helps you evaluate what a new trial is adding — see our full guide to metastatic breast cancer treatment options.
⚠️ Clinical Warning: Subtype-specific trial eligibility — particularly for HER2-positive and TNBC immunotherapy trials — requires biomarker confirmation by a CLIA-certified laboratory using a protocol-specified assay platform. Clinical assessment of HER2 status or PD-L1 status alone does not satisfy most 2026 trial enrollment requirements. Telehealth oncology platforms at NCI-designated cancer centers now offer biomarker-informed trial-matching consultations for patients without local access to a specialist.
✅ Patient Action: Before pursuing any subtype-specific trial, ask your oncologist: “Has my tumor been tested for HER2 amplification, ER/PR expression, PD-L1 CPS score, and BRCA1/2 mutation status using the specific assay platforms required by the trials we are considering?” Most 2026 Phase III trials require confirmed biomarker status through CLIA-certified testing — not just the subtype documented in your original diagnosis report. Consult a board-certified breast oncologist or gynecologic oncologist before enrollment in any subtype-targeted trial.
Clinical trial costs, insurance coverage, and your patient rights
Under the Affordable Care Act Section 2709, most private health insurance plans in the United States are required to cover routine patient care costs associated with participation in approved clinical trials. Covered routine costs include:
- Physician visits and examinations required by the trial protocol
- Standard laboratory tests and imaging that would be covered as routine care outside the trial
- Hospitalizations required by the trial protocol that would otherwise qualify as standard covered care
- Anesthesia and surgical services for protocol-required procedures
📊 Clinical Data Point: Medicare Part A and Part B also cover routine patient care costs in qualifying clinical trials under CMS policy — a coverage mandate that applies to breast cancer trials meeting federal qualification criteria. — Source: CMS clinical trial coverage policy
What the Affordable Care Act requires insurers to cover in clinical trials
ACA Section 2709 does not require insurers to cover the investigational drug, device, or experimental intervention itself — those costs are typically borne by the trial sponsor. What the law mandates is coverage for the routine care costs a patient would incur regardless of trial participation.
What the trial sponsor typically pays vs. what falls to the patient
The trial sponsor — typically a pharmaceutical company, a cooperative group, or an NCI program — covers the experimental agent, protocol-required imaging or laboratory tests beyond standard care, and research administration costs. Understanding which cost category applies to each element of your care requires a written breakdown from the trial coordinator before consent.
✅ Patient Action: Before signing the informed consent form, ask the trial coordinator for a written cost breakdown that identifies: which costs the sponsor covers, which costs your insurance plan covers under ACA Section 2709, and whether any out-of-pocket costs apply based on your specific plan’s deductible, copay, or network structure. Health insurance comparison tools can help you evaluate whether your current plan explicitly covers clinical trial participation as mandated. Consult a board-certified oncologist and your trial coordinator before enrolling to confirm cost allocation in writing.
Your patient rights during a trial: withdrawal, safety data access, and continued standard care
Institutional Review Board oversight is the structural patient protection layer in every FDA-regulated clinical trial. The IRB reviews the consent document, monitors adverse event reporting, and has the authority to halt the trial if patient safety is compromised. You have three non-negotiable patient rights regardless of which trial you join: the right to withdraw at any time without penalty to your standard care access, the right to receive safety information as it becomes available during the trial, and the right to continue receiving standard care if the trial is stopped early.
What your oncologist wants you to know before enrolling in a trial
A breast cancer clinical trial is not a sign that standard care has failed. That is the single most important thing I want every patient who reads this article to understand.
I am Dr. Carolyn D. Fairweather, MD, the Founder and Chief Medical Advisor of mymedicineadvisor.com and a board-certified specialist in gynecologic oncology. I have guided patients through clinical trial enrollment decisions at every stage of breast cancer — from newly diagnosed patients considering neoadjuvant trial participation before surgery to patients with metastatic disease evaluating Phase III options after second-line therapy.
🩺 Physician Note: “One of my most formative clinical trial conversations involved a Stage III TNBC patient who was preparing to enter second-line chemotherapy when a multidisciplinary tumor board review at an NCI-designated cancer center identified an active Phase III neoadjuvant immunotherapy trial matching her confirmed PD-L1 CPS and BRCA status.
The question that changed her treatment course was this: ‘If I am randomized to the control arm, will I receive the current NCCN 2026 standard neoadjuvant chemotherapy regimen, or a modified version?’ The answer — that control arm patients received current NCCN-standard neoadjuvant therapy — meant she had everything to gain and nothing to lose by participating. She enrolled. I tell that story to every patient who tells me they are not a ‘trial person.'” — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
Three questions every patient should ask before signing consent
- “What is the randomization ratio, and if I am assigned to the control arm, will I receive the full current NCCN Guidelines 2026 standard-of-care regimen?”
- “What are the protocol stopping rules — what would cause the Data Safety Monitoring Board to halt the trial, and what happens to my care if that occurs?”
- “If the experimental arm demonstrates superior results during the trial, will patients in the control arm be offered crossover access to the experimental therapy?”
These are not aggressive or unusual questions. Every competent principal investigator expects them. A site that cannot answer all three clearly is a site worth reconsidering.
When a clinical trial is the strongest clinical choice — not the last resort
The NCCN 2026 guidelines explicitly list clinical trial participation as an appropriate consideration alongside standard-of-care options at multiple treatment decision points — not as a fallback after standard options have been exhausted. Randomized controlled trials at Phase III offer patients the rigorous oversight, structured safety monitoring, and multidisciplinary tumor board access that community oncology practices may not routinely provide.
✅ Patient Action: Consult a board-certified breast oncologist or gynecologic oncologist before making any final clinical trial enrollment decision — the right trial for your specific subtype, stage, and treatment history can only be identified through a specialist-led biomarker review and protocol evaluation. Download our pre-appointment question checklist to bring to your next oncology consultation.
Frequently asked questions about breast cancer clinical trials
1. What is a clinical trial for breast cancer?
A breast cancer clinical trial is a research study that tests a new treatment, a new combination of approved therapies, or a new approach to surgery, radiation, or supportive care in patients with confirmed breast cancer diagnoses. Trials are conducted in four phases — Phase I through Phase IV — each testing a different clinical question. Oversight comes from an Institutional Review Board and the FDA. Consult a board-certified oncologist to determine which trial phase is appropriate for your current diagnosis and treatment history.
2. How do I find breast cancer clinical trials near me?
Search ClinicalTrials.gov using the condition field (“breast cancer” or your specific subtype), the recruiting status filter (set to “recruiting”), and your ZIP code or preferred distance. The results include the trial phase, eligibility criteria, and contact information for each study site. Your oncologist can also run a protocol search using your confirmed subtype and biomarker status. Before your search, review current breast cancer mammogram screening guidelines if you have not yet had a complete diagnostic workup confirming your subtype.
3. Who qualifies for a breast cancer clinical trial?
Eligibility depends on your confirmed cancer subtype, disease stage, number of prior treatment lines received, ECOG performance status (most Phase II and III trials require a score of 0, 1, or 2), organ function laboratory values, and protocol-required biomarker test results. Exclusion criteria commonly include active brain metastases, inadequate organ function, and prior chemotherapy within the required washout period of 21 to 28 days. Consult a board-certified oncologist or the trial’s principal investigator to confirm your eligibility — never self-exclude based on a single criterion without specialist review.
4. Are breast cancer clinical trials safe?
All FDA-regulated breast cancer clinical trials require Institutional Review Board approval, written informed consent, and ongoing safety monitoring by an independent Data Safety Monitoring Board. Phase II and Phase III trials have pre-existing safety data from earlier phases. Phase I trials carry the most uncertainty — they are testing safety for the first time in humans. No trial is risk-free, and no responsible investigator will claim otherwise. IRB oversight means patients can withdraw at any time, and trial stoppage protocols exist to protect participants if unexpected safety signals emerge during the study.
5. Do clinical trials pay for my treatment costs?
The trial sponsor — typically a pharmaceutical company, cooperative group, or NCI program — covers the experimental agent, protocol-specific laboratory tests, and research administration costs. Under the Affordable Care Act Section 2709, your health insurance plan is required to cover routine patient care costs such as physician visits, standard lab work, and imaging associated with trial participation. Out-of-pocket costs vary by plan, deductible, and network status. Ask your trial coordinator for a written cost breakdown before signing consent to clarify exactly who covers each component of your care.
6. What is a Phase 3 breast cancer clinical trial?
A Phase 3 breast cancer clinical trial is a large, randomized study that directly compares an experimental treatment against the current standard-of-care regimen in hundreds to thousands of patients. Patients are randomly assigned to either the experimental arm or the control arm. In most breast cancer Phase 3 trials, the control arm receives active standard therapy — not a placebo. The primary endpoint is typically a statistically significant improvement in progression-free survival or overall survival. Consult a board-certified oncologist to evaluate whether a specific Phase 3 trial’s comparator arm matches what you would receive outside the trial.
7. Can I join a trial if I’ve already had chemotherapy?
In most cases, yes — prior chemotherapy does not automatically disqualify you from a clinical trial. However, trial protocols specify which prior treatment lines are permitted and how many. A required washout period of 21 to 28 days after your last chemotherapy cycle applies to most Phase II and III trials. Some trials specifically require prior chemotherapy as an inclusion criterion — for example, a trial targeting endocrine-resistant metastatic breast cancer may require at least one prior line of systemic therapy. Consult a board-certified oncologist to match your specific treatment history against the eligibility criteria of any trial you are considering.
8. What happens if I want to drop out of a clinical trial?
You can leave a breast cancer clinical trial at any time, for any reason, without any penalty to your access to standard medical care. This right is a non-negotiable condition of FDA-regulated research and is explicitly stated in every IRB-approved informed consent document. Withdrawing from a trial does not affect your relationship with your oncologist, your insurance coverage, or your eligibility for other trials in the future. The trial team will typically conduct a safety follow-up visit after withdrawal to document your health status, but participation in that visit is voluntary.
9. Will I receive a placebo instead of real treatment?
In breast cancer clinical trials, a pure placebo-only control arm is rare. Most Phase II and Phase III breast cancer trials assign the control arm patients to receive the current standard-of-care regimen — an active treatment, not an inert substance. When a placebo is used, it is typically added to an active therapy backbone in both arms so that neither group receives less treatment than they would outside the trial. The randomization process, what both arms receive, and the probability of assignment to each arm are disclosed in full in the informed consent document before you agree to participate.
10. Does my health insurance cover clinical trial participation?
Under the Affordable Care Act Section 2709, most private health insurance plans are federally required to cover routine patient care costs associated with approved clinical trial participation. Medicare Part A and B also cover qualifying clinical trial routine care costs under CMS policy. What insurance does not cover is the experimental agent itself — that is covered by the trial sponsor. Coverage specifics depend on your plan’s deductible structure, copay requirements, and network status. Ask your trial coordinator for a written cost allocation summary, and verify your plan’s clinical trial coverage provisions before your first screening visit.
11. How long does a breast cancer clinical trial last?
Duration varies significantly by phase. Phase I trials typically run one to two years. Phase II trials run two to three years. Phase III trials — the most common for patients in active treatment — often run three to seven years from enrollment open to final data readout, though individual patient participation may be shorter depending on the protocol’s primary endpoint timing and stopping rules.
Metastatic disease trials may involve ongoing treatment until disease progression or unacceptable toxicity. Your personal participation period is defined by the trial protocol and disclosed in the informed consent document. Consult a board-certified oncologist to understand what the time commitment means for your specific situation and treatment goals.
Your next step toward breast cancer clinical trial enrollment
You now have a working knowledge of the four trial phases, the specific eligibility criteria that will determine your screening outcome, the five-step enrollment process, the 2026 trial landscape for your subtype, your federal insurance rights, and the three questions every oncologist expects a prepared patient to ask.
The clinical trial conversation is an act of informed self-advocacy. It belongs at the beginning of the treatment planning process — not at the end.
At your next oncology appointment, bring three things: your complete pathology report documenting your subtype and biomarker status, the NCT numbers of one or two trials that match your subtype from your ClinicalTrials.gov search, and the specific questions from Section 7. That preparation takes thirty minutes. The conversation it opens can change what treatment you receive.
For patients who have completed treatment and are transitioning to recovery and monitoring, our guide to life after breast cancer covers what to expect from surveillance, recurrence monitoring, and long-term follow-up care.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.