On This Page – Quick Medical Summary
Why breast cancer screening by state matters in 2026
For millions of American women, the question is not whether to get a mammogram — it is how to afford one.
Breast cancer screening finds this disease at its most treatable stage, yet cost barriers and conflicting guideline messaging stop women from scheduling year after year.
According to the NCI’s breast cancer incidence data, breast cancer is among the most commonly diagnosed cancers in American women — and detection at an early, localized stage is the single most reliable variable in improving long-term outcomes.
When a screening result requires follow-up, understanding what happens after an abnormal mammogram result can prepare you for the next conversation with your care team.
ℹ️ Medical Disclaimer: The screening protocols, program eligibility requirements, and insurance coverage information discussed in this article are provided for educational purposes only. Individual screening decisions — including when to begin mammography, which imaging modality is appropriate, whether supplemental screening is warranted, and which federal or state program benefits apply to your specific situation — depend on personal health history, family history, current insurance coverage, and specialist assessment.
Medicaid, Medicare, and ACA marketplace coverage terms vary by plan and state; verify your specific benefits directly with your insurer or Medicaid office before scheduling any procedure. Consult a board-certified gynecologic oncologist or primary care physician before acting on any clinical recommendation in this article. If you are experiencing breast symptoms — including a new lump, skin dimpling, nipple discharge, or persistent breast pain — do not wait for your scheduled annual screening. Contact your healthcare provider immediately.
What the 2026 mammogram guidelines actually say by age
The U.S. Preventive Services Task Force recommends that women at average risk receive annual breast cancer screening beginning at age 40.
This Grade B recommendation — the highest endorsement level for a preventive health service — resolves years of conflicting age-start guidance by aligning the recommended start age with evidence that earlier screening prevents more deaths across the full population of American women.
USPSTF 2026 vs. ACS: which guideline does your doctor follow?
The USPSTF breast cancer screening recommendation statement calls for annual screening from age 40.
The ACS mammography screening guidelines give women a patient-choice framework at ages 40–44 with a strong recommendation to begin annual screening by age 45, continuing annually through age 54 before considering biennial screening.
Most hospital-based oncology programs have aligned with the 40-start age. For a full comparison of age-specific scheduling frameworks and what they mean for your screening calendar, the article on mammogram starting age and screening schedules by risk level provides the breakdown by decade and risk tier.
High-risk screening: when the protocol changes at age 30
Women with a calculated lifetime breast cancer risk of 20% or greater — determined using a validated model such as Tyrer-Cuzick or BRCAPRO — qualify for a separate high-risk protocol.
This protocol begins at age 30 and includes both annual breast MRI with contrast and an annual screening mammogram.
How family history changes your mammogram starting age
A first-degree relative — mother, sister, or daughter — diagnosed with breast or ovarian cancer before age 50 is a direct clinical prompt to discuss formal risk modeling before you reach your standard average-risk starting age.
✅ Patient Action: Before your first screening appointment, use our Genetic Risk Assessment Tool to evaluate whether your family history places you in the high-risk category. If your result suggests elevated risk, ask a board-certified gynecologic oncologist specifically: “What is my calculated lifetime breast cancer risk using a validated model, and does that change my screening start age or imaging protocol?”
📊 Clinical Data Point: The USPSTF assigns a Grade B recommendation — the highest preventive services endorsement level — to annual breast cancer screening beginning at age 40 for women at average risk. Source: USPSTF breast cancer screening recommendation statement.
Screening mammogram vs. diagnostic: what’s the difference in 2026?
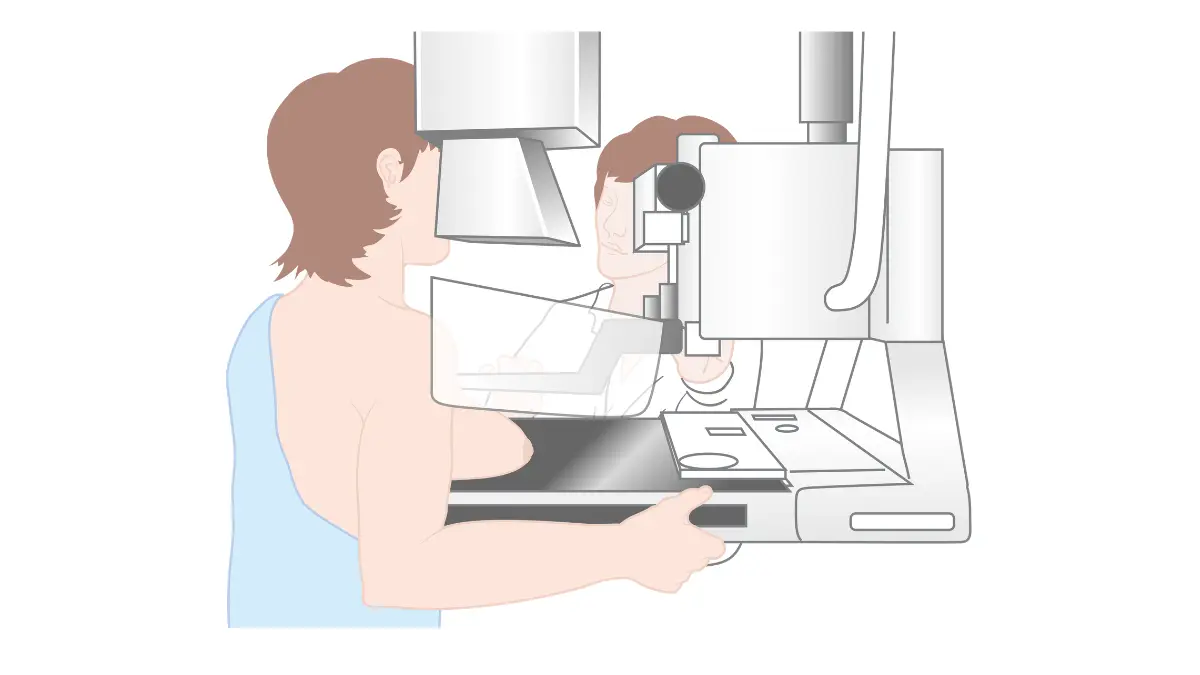
A screening mammogram is a routine imaging exam performed on women with no current breast symptoms. A diagnostic mammogram is ordered when a physician needs to evaluate a specific lump, prior abnormal finding, or area of concern.
The distinction is financially critical: screening mammograms qualify for zero cost-sharing under ACA-compliant plans, while diagnostic mammograms are typically subject to deductibles and coinsurance.
2D digital mammogram vs. 3D tomosynthesis: which should you request?
Digital breast tomosynthesis (DBT) — commonly called a 3D mammogram — acquires multiple thin-slice X-ray images of the breast from different angles.
This eliminates tissue overlap that causes conventional 2D imaging to miss small tumors, particularly in women with dense breast tissue.
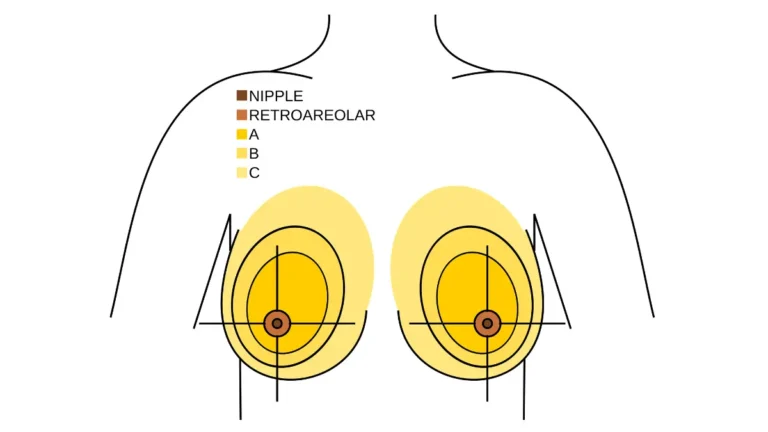
🔬 How It Works: In a 3D mammogram, the X-ray tube moves in an arc over the compressed breast, capturing images from multiple angles that are digitally reconstructed into thin cross-sectional slices. In women with heterogeneously dense or extremely dense breast tissue (BI-RADS Categories C and D), this multi-angle acquisition eliminates the tissue superimposition that causes 2D imaging to obscure small early-stage cancers — the same principle as CT imaging vs. a flat X-ray for chest evaluation.
What a dense breast tissue result actually means for your next scan
The Mammography Quality Standards Act (MQSA) now requires all certified mammography facilities to notify patients in writing when their breast density falls into Category C (heterogeneously dense) or Category D (extremely dense).
This notification does not mean cancer is present. It means supplemental screening — typically breast ultrasound — may improve detection sensitivity for your next scan.
For detailed guidance on what a dense breast result means for your ongoing screening plan, the article on dense breast tissue and cancer risk explains the clinical significance and your supplemental screening options.
When your doctor orders a diagnostic mammogram instead
Symptoms that prompt a diagnostic order — a new lump, nipple discharge, skin dimpling, or unexplained breast asymmetry — require evaluation outside the standard screening schedule.

If you notice a breast change before your next scheduled mammogram, use our Symptom Checker to evaluate whether your symptom warrants contacting your provider before your annual appointment.
Recognizing breast cancer warning signs between scheduled screenings can be the difference between a diagnostic evaluation that finds something early and a wait that allows disease to progress.
✅ Patient Action: Ask your screening facility specifically: “Do you offer 3D tomosynthesis, and will it be covered under my plan as part of my annual screening?” Women whose prior mammogram report lists breast density as Category C or D should ask their radiologist or gynecologic oncologist directly: “Is supplemental ultrasound or breast MRI warranted for my risk history?” Do not wait for the facility to raise the question.
How to find free or low-cost mammograms in your state in 2026
Every U.S. state and territory participates in the CDC’s National Breast and Cervical Cancer Early Detection Program (NBCCEDP), which funds free and low-cost mammograms for eligible women across all 50 states and the District of Columbia.
What is the NBCCEDP and who qualifies?
The NBCCEDP serves women aged 40 to 64 who are uninsured or underinsured and whose household income falls at or below 250% of the federal poverty level (FPL).
Women who are underinsured — meaning their health plan does not adequately cover preventive mammography — may also qualify even if they carry some form of coverage.
The income threshold that unlocks free mammograms in every state
The 250% FPL income threshold is updated annually by the Department of Health and Human Services. Women above this threshold who remain uninsured should explore ACA marketplace plans, which cover annual screening mammograms at zero cost-sharing as a federally required preventive service.
Federally qualified health centers (FQHCs) offer sliding-scale mammography for women who do not qualify for NBCCEDP based on income but cannot afford full-cost screening.
Step-by-step: how to access your state’s free screening program
- Verify eligibility — confirm your age (40–64), insurance status (uninsured or underinsured), and household income relative to 250% of the current federal poverty level.
- Locate your state’s program — use the CDC’s NBCCEDP program locator to find your state’s lead agency, eligibility intake process, and scheduling contact.
- Call to schedule — contact your state’s program directly to confirm current program availability, appointment slots, and required documentation.
- Bring required documentation — most programs require proof of income (pay stub, tax return, or self-attestation form), age verification, and confirmation of insurance status.
What to do if you don’t qualify for NBCCEDP
Women who earn above the NBCCEDP threshold but remain uninsured are not without options. ACA marketplace enrollment — open during November enrollment windows and during qualifying life-event special enrollment periods — provides access to plans that cover breast cancer screening at no cost under the preventive services mandate.
📊 Clinical Data Point: The CDC’s NBCCEDP funds free and low-cost breast cancer screening in all 50 states, the District of Columbia, and U.S. territories. Income eligibility threshold: at or below 250% of the federal poverty level. Age eligibility: 40–64. Source: CDC National Breast and Cervical Cancer Early Detection Program guidelines.
Does your insurance cover a mammogram? Medicaid, Medicare, and ACA rules in 2026
Under ACA Section 2713, all health insurance plans sold through the ACA marketplace — and most employer-sponsored plans — must cover annual screening mammograms for women aged 40 and older at zero cost-sharing.
No copay. No deductible. No coinsurance — provided the exam is performed at an in-network, MQSA-certified facility and coded correctly as a preventive screening.
ACA-compliant insurance: mammograms at zero cost since 2010
This zero-cost mandate has been federal law since the ACA’s preventive services provision took effect. If your plan is ACA-compliant and your mammogram is ordered and coded as preventive screening, you should owe nothing at the point of service.
Medicaid mammogram coverage: expansion state vs. non-expansion state
In Medicaid expansion states — currently 40 states plus the District of Columbia — Medicaid must cover screening mammograms with no cost-sharing for eligible women. In non-expansion states, Medicaid coverage terms for mammography vary and may include cost-sharing provisions.
Verify your state’s current Medicaid expansion status before assuming full zero-cost coverage applies.
Medicare Part B: what’s covered and what costs extra
Medicare Part B covers one annual screening mammogram for women aged 40 and older with no cost-sharing required. Women aged 35–39 are covered for one baseline mammogram under Part B.
For current benefit details, review Medicare mammogram coverage under Part B and confirm your specific plan’s cost-sharing terms before scheduling.
When you might still owe a copay for a mammogram
The most common billing surprise in breast cancer screening is this: a physician orders a screening mammogram, but the facility codes the claim as diagnostic.
That single coding change converts a zero-cost preventive visit into a claim subject to your deductible and coinsurance — even on an ACA-compliant plan.
⚠️ Clinical Warning: Before your mammogram, confirm with both the ordering physician and the imaging facility that the exam will be coded as a screening mammogram — not a diagnostic mammogram. If a prior abnormal finding or breast symptom exists in your record, ask specifically: “How will this visit be coded on my claim?” An unexpected diagnostic code activates cost-sharing that the ACA’s preventive mandate does not cover.
✅ Patient Action: Call your insurer’s member services line before scheduling and ask: “Is an annual screening mammogram at [facility name] fully covered at zero cost-sharing under ACA preventive services with my current plan?” If your coverage status is unclear, ask your primary care physician or gynecologist to confirm the correct procedure order language before the appointment is made.
High-risk groups, family history, and screening disparities in 2026
Breast cancer screening guidelines were written for the average-risk population. They do not account for every woman equally — and understanding where the standard protocol ends is as important as knowing when it begins.
Black and Hispanic women: why screening disparities persist and what 2026 data shows
Black women in the United States face a breast cancer mortality rate substantially higher than white women — not because they are diagnosed more often, but because they are more likely to be diagnosed with aggressive subtypes and at later stages.
A significant driver of this disparity is the higher prevalence of triple-negative breast cancer among Black women — a subtype characterized by aggressive behavior, limited hormonal treatment options, and a stronger case for earlier, more frequent screening.
For a detailed clinical overview of how race-related biology and screening access combine to create outcome disparities, the article on breast cancer risk and outcomes in Black women provides the full picture.
📊 Clinical Data Point: Black women in the United States face breast cancer mortality rates significantly higher than white women, driven by higher rates of triple-negative breast cancer and disparities in early screening access. Source: NCI SEER program data.
BRCA1 and BRCA2 carriers: why your screening starts at 30
Women with a confirmed BRCA1 or BRCA2 pathogenic variant — or a calculated lifetime risk of 20% or greater — require a protocol that starts earlier and uses more sensitive imaging.
High-risk screening begins at age 25–30 with annual breast MRI with contrast and at age 30 with annual mammography. Standard NBCCEDP programs do not fulfill this dual-modality protocol.
For guidance on interpreting a positive result and what it means for your screening schedule, the article on BRCA gene test results and what to do next provides the clinical walkthrough.
✅ Patient Action: Women with a confirmed BRCA1 or BRCA2 pathogenic variant, or a lifetime breast cancer risk of 20% or greater, should consult a board-certified genetic counselor and gynecologic oncologist before reaching average-risk starting age. Ask specifically: “What dual-modality screening protocol applies to my BRCA status, and what is the earliest age at which I should begin annual MRI?”
Helping an elderly or immigrant family member access screening
NBCCEDP-funded programs are available to all eligible women regardless of immigration or documentation status, per current CDC program guidelines.
Caregivers navigating the enrollment process on behalf of a family member can find practical guidance — including how to communicate with a screening program on a family member’s behalf — in the article on supporting a loved one through breast cancer diagnosis and care.
Dr. Fairweather’s clinical perspective: why women delay screening — and what that delay costs
In my practice as a gynecologic oncologist, I encounter the same three barriers to mammography scheduling year after year: cost uncertainty, scheduling friction, and fear of a positive result.
Cost uncertainty is the most solvable — which is precisely why Sections 4 and 5 of this article exist. The other two require a direct clinical answer.
The three reasons patients delay mammograms (and what they cost at diagnosis)
Scheduling friction — the sense that a preventive appointment is lower priority than everything else in a week — is responsible for more preventable late-stage diagnoses in my patient population than any access barrier.
Fear of a positive result is equally damaging. I understand it completely. But a fear-driven delay does not change the biology of a tumor that is growing — it changes only the stage at which it is found.
🩺 Physician Note: In my experience, the most dangerous delay is not the one caused by an access barrier. It is the delay caused by a woman who has insurance, knows her mammogram is overdue, and is not ready to know the answer. I have never had a patient tell me she wished she had found out later. I have watched women wish they had found out sooner.
What I tell every patient who says she doesn’t have time to schedule this year
I tell her one thing: a screening mammogram takes 20 minutes.
The gap between Stage I and Stage IV outcomes — documented consistently in breast cancer survival rates by stage — is not a statistical abstraction. It is the clinical argument for scheduling before symptoms appear.
How early-stage detection changes the surgical conversation
Detection at Stage I changes not just the prognosis but the range of choices available at the treatment table.
Women identified through annual screening at an early stage have access to the full spectrum of surgical treatment options, including lumpectomy as an alternative to full mastectomy, with favorable reconstruction and recovery outcomes that later-stage detection forecloses.
Frequently asked questions about breast cancer screening by state
1. What is the NBCCEDP and how does it work?
The CDC’s National Breast and Cervical Cancer Early Detection Program funds free and low-cost mammograms in every U.S. state. It serves uninsured and underinsured women aged 40 to 64 whose household income falls at or below 250% of the federal poverty level. Each state has a designated lead agency that manages eligibility intake and appointment scheduling. Contact your state’s NBCCEDP program directly to confirm current capacity and required documentation.
2. At what age should I get my first mammogram?
The USPSTF recommends annual breast cancer screening beginning at age 40 for women at average risk. The American Cancer Society supports patient choice from age 40, with a strong recommendation to begin annually by 45. Women with a first-degree relative diagnosed with breast or ovarian cancer before 50, or a known BRCA variant, may need to begin screening as early as age 30. Consult a board-certified gynecologic oncologist to confirm the starting age appropriate for your risk profile.
3. Are mammograms free with ACA-compliant insurance?
Under ACA Section 2713, marketplace and most employer-sponsored plans must cover annual screening mammograms at zero cost-sharing for women aged 40 and older. No copay, deductible, or coinsurance applies — provided the exam is performed at an in-network facility and coded correctly as a preventive screening, not a diagnostic procedure. Confirm the coding with both your ordering physician and the imaging facility before your appointment.
4. How often should I get a mammogram after my first?
For average-risk women, the USPSTF recommends annual breast cancer screening from age 40 through age 74. The ACS allows biennial screening after age 55 if preferred and no significant findings have required follow-up. Women with dense breast tissue, a prior biopsy, or a first-degree family history may require annual imaging regardless of age. Consult your gynecologic oncologist to confirm the frequency appropriate for your clinical history.
5. What if I can’t afford a mammogram and I’m uninsured?
If you are uninsured and your income is at or below 250% of the federal poverty level, you likely qualify for free breast cancer screening through your state’s NBCCEDP-funded program. Search online for your state name and “NBCCEDP breast cancer program” to locate your state’s lead agency intake line. If you earn above the NBCCEDP threshold, ask your primary care physician for a referral to a federally qualified health center offering sliding-scale mammography fees.
6. How do I find a free mammogram program near me?
Search for your state name combined with “NBCCEDP breast cancer screening program” to find your state’s lead agency contact. You can also call the NCI’s cancer information line at 1-800-4-CANCER to be connected to your state’s funded mammogram access program. Most state NBCCEDP programs allow direct scheduling by phone without requiring a physician referral. Bring proof of income and age verification to your appointment intake call.
7. What income level qualifies for a free mammogram?
The CDC’s NBCCEDP income threshold is set at or below 250% of the federal poverty level, updated annually by HHS. Women who are underinsured — meaning their plan does not adequately cover preventive mammograms — may also qualify even with existing coverage. Contact your state’s NBCCEDP lead agency directly to confirm the current annual income limit for your household size; thresholds differ slightly by state based on program capacity.
8. Does Medicare cover 3D mammograms?
Medicare Part B covers one annual screening mammogram for women aged 40 and older at no cost-sharing. Coverage for 3D mammography (digital breast tomosynthesis) has expanded in recent years; confirm with your imaging facility whether DBT is billed within the standard screening coverage or as an additional code that may trigger cost-sharing. Log in to your Medicare account or call 1-800-MEDICARE to verify your current imaging benefit before scheduling.
9. What is the difference between a screening and a diagnostic mammogram?
A screening mammogram is a routine exam for women with no current breast symptoms — typically two to four standard views per breast. A diagnostic mammogram is ordered when a physician needs to evaluate a specific lump, symptom, or prior abnormality and involves additional imaging views. Diagnostic mammograms typically do not qualify for zero-cost ACA preventive coverage. Consult a board-certified radiologist or gynecologic oncologist to confirm which exam has been ordered before your appointment.
10. Are 3D mammograms better than 2D for dense breasts?
Digital breast tomosynthesis (DBT) improves cancer detection in women with dense breast tissue by eliminating tissue overlap that causes 2D mammograms to miss small tumors. Women with BI-RADS Category C or D breast density — documented on prior mammogram reports — benefit most from 3D imaging, which also reduces false-positive recall rates. Ask your radiologist whether your breast density classification makes tomosynthesis the preferred modality. Consult a gynecologic oncologist if supplemental ultrasound or breast MRI is also warranted.
11. My family has a BRCA mutation — when should I start screening?
Women with a confirmed BRCA1 or BRCA2 pathogenic variant begin a dual-modality protocol: annual breast MRI with contrast starting at age 25–30, and annual mammography starting at age 30. This high-risk screening schedule is not covered under standard NBCCEDP programs and requires coordination between a board-certified genetic counselor and gynecologic oncologist. Consult a gynecologic oncologist before reaching average-risk starting age to establish your personalized screening timeline.
Your next step: schedule your mammogram this week
Knowing the guidelines removes the confusion. Scheduling removes the risk.
If you are uninsured or underinsured, contact your state’s NBCCEDP-funded program this week — eligibility takes minutes to confirm, and the appointment you make today changes what is possible at diagnosis.
If you carry insurance, verify your annual mammogram is coded as preventive, confirm zero cost-sharing with your insurer, and book the appointment before the end of this month.
If your family history or a prior test result places you in a higher-risk category, the article on breast cancer risk factors and who is most at risk is the right next read before your first screening conversation.
A mammogram takes 20 minutes. In 2026, the path to one has never been more clearly mapped.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.