On This Page – Quick Medical Summary
What Black women need to know about breast cancer risk
Breast cancer in Black women is more likely to involve a biologically aggressive subtype, more likely to be diagnosed at an advanced stage, and more likely to be fatal than the same diagnosis in white women — even when income, insurance status, and health behaviors are equal. That disparity has two distinct and simultaneous causes: tumor biology and healthcare access. This article addresses both with clinical specificity.
It was written by a board-certified gynecologic oncologist because the answers you are looking for require a physician’s voice — not a pamphlet.
If a new breast change prompted this search, use our Symptom Checker to identify whether your symptoms warrant urgent clinical evaluation before reading further.
ℹ️ Medical Disclaimer: The mortality statistics, tumor biology explanations, screening age recommendations, treatment protocols, and medication information in this article reflect current clinical evidence and are provided for educational purposes only. Diagnostic conclusions — including tumor receptor status, cancer stage, and genetic risk classification — depend on pathology results, imaging, and full clinical history reviewed by a qualified specialist.
Treatment decisions, including chemotherapy regimens, immunotherapy eligibility, surgical planning, and clinical trial enrollment, must be made in direct consultation with a board-certified oncologist. Screening timeline recommendations depend on individual risk factors only a physician can fully assess. Insurance coverage for genetic testing, breast MRI, and clinical trials varies by plan and requires direct verification. Consult a board-certified gynecologic oncologist or breast oncologist before acting on any clinical information in this article.
The breast cancer mortality gap: what 2026 data shows by race
Black women in the United States die from breast cancer at significantly higher rates than white women — a disparity documented across income levels, insurance categories, and geographic regions. According to the NCI SEER database, this gap is present at every stage of disease and widens most sharply at Stage III and Stage IV, where treatment complexity and institutional resources matter most.
Survival rates by stage: Black women vs. white women
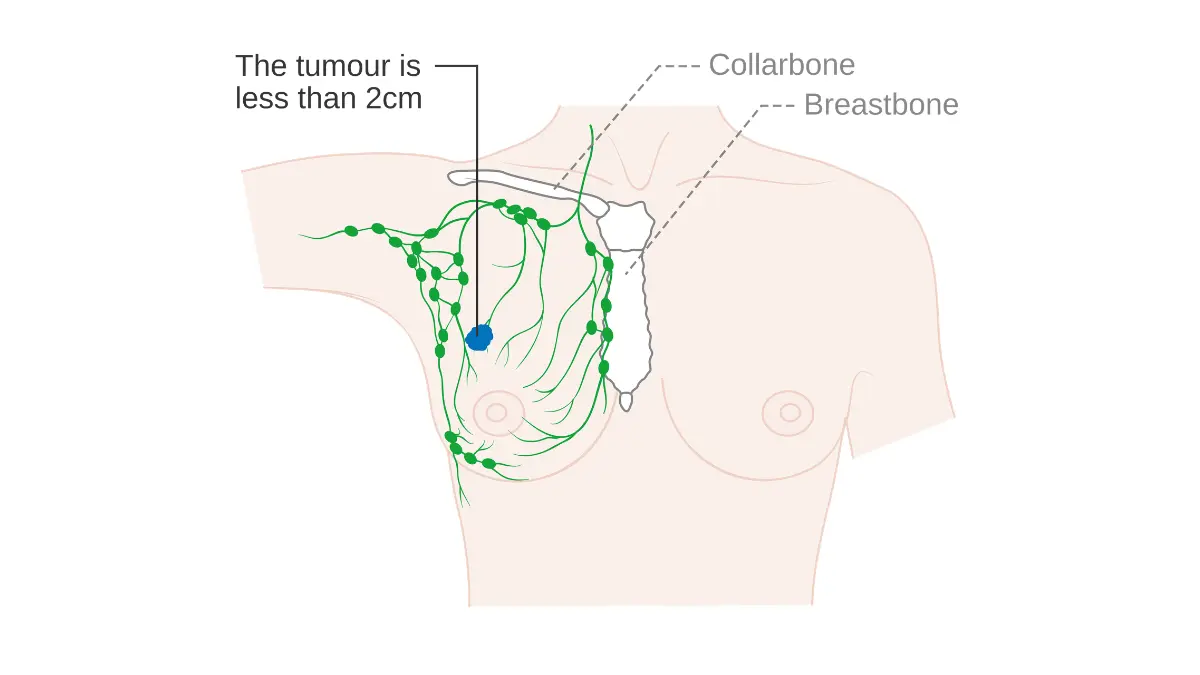
The mortality gap is not uniform across all stages. At Stage I — when cancer is confined to the breast and has not spread to lymph nodes — survival outcomes are strongly favorable across all demographic groups. The disparity becomes clinically significant beginning at Stage II and accelerates at Stage III and beyond.
📊 Clinical Data Point: The NCI SEER database tracks breast cancer five-year relative survival rates by race, ethnicity, and stage. Per 2026 NCI breast cancer statistics and racial survival data, Black women show measurably lower five-year overall survival than white women at Stage II, III, and IV. The disparity is smallest at Stage I and largest at metastatic disease. — Source: National Cancer Institute SEER Database, 2026
For the complete context of how staging affects individual prognosis, see our guide to breast cancer stages and survival — the parent resource for this article.
Why the gap exists: tumor biology and treatment access together
Two distinct mechanisms drive the disparity — and both must be named.
The first is tumor biology. Black women are diagnosed with triple-negative breast cancer (TNBC) at a substantially higher rate than white women. TNBC is biologically more aggressive, grows faster, lacks the molecular targets that standard hormone therapies exploit, and is associated with a higher rate of lymph node involvement at diagnosis.
The second is systemic access. Black women experience longer average delays from initial symptom presentation to confirmed diagnosis, lower rates of referral for high-risk genetic screening, and significantly reduced access to NCI-designated comprehensive cancer centers where molecular tumor boards, pembrolizumab protocols, and clinical trials are available.
📊 Clinical Data Point: Per CDC breast cancer surveillance data by race and ethnicity (2026 cancer surveillance cycle), Black women are diagnosed with invasive breast cancer at younger average ages than white women, and present more frequently at Stage II or Stage III at time of initial diagnosis. — Source: Centers for Disease Control and Prevention, 2026
What late-stage diagnosis means for survival outcomes
Late-stage diagnosis is not a personal failure. It is a predictable consequence of biologically aggressive tumor subtypes combined with inadequate screening frequency, screening access, and time-to-care.
🩺 Physician Note: Population-level survival statistics are a description of what happened to other people under different circumstances — not a prediction of your individual outcome. What the data documents is a system that has historically underserved Black women at the screening stage, the referral stage, and the treatment stage. Your outcome depends on what the clinical decisions look like from this point forward.
Our full breakdown of breast cancer survival rates by stage and subtype provides the denominator context that raw mortality figures cannot — stage at diagnosis is the single strongest predictor of individual outcome.
Triple-negative breast cancer: why this subtype matters more for Black women
Triple-negative breast cancer (TNBC) is the breast cancer subtype most directly linked to the mortality disparity in Black women. Understanding what “triple-negative” means in clinical terms is not optional for any Black woman navigating a new diagnosis, a family history of breast cancer, or a conversation about screening.
What “triple-negative” means for your treatment options
TNBC is defined by the simultaneous absence of three molecular markers: estrogen receptors (ER−), progesterone receptors (PR−), and HER2 protein overexpression (HER2−). These three markers are the targets that the most commonly used breast cancer therapies exploit.
🔬 How It Works: Estrogen receptor-positive cancers are treated with tamoxifen or aromatase inhibitors — medications that starve the tumor by blocking estrogen signaling. HER2-positive cancers respond to trastuzumab (Herceptin) and related antibody therapies that attack the HER2 receptor directly. A triple-negative tumor lacks all three of these molecular handles. Tamoxifen cannot work when there are no estrogen receptors to block. Trastuzumab cannot work when HER2 protein is absent. This eliminates an entire class of highly effective, comparatively well-tolerated targeted therapies from the option menu — leaving neoadjuvant chemotherapy as the primary systemic treatment, with immunotherapy added for eligible patients.
For a complete breakdown of TNBC treatment pathways and expected outcomes, see our guide to triple-negative breast cancer: diagnosis, prognosis, and treatment options.
How common is TNBC in Black women vs. white women?
TNBC is diagnosed in Black women at a substantially higher rate than in white women — a disparity documented across multiple NCI surveillance cycles.
This difference in subtype prevalence is not fully explained by access disparities or socioeconomic factors. It reflects a real biological difference in tumor distribution between demographic populations — one that is documented, not contested.
Inflammatory breast cancer: a separate high-risk subtype
Inflammatory breast cancer (IBC) is a distinct, rapidly progressing subtype diagnosed at higher rates in Black women than in white women. IBC does not present as a palpable lump.
Key warning signs include: breast redness covering one-third or more of the breast surface; warmth or heaviness without a localized mass; peau d’orange skin texture (orange-peel dimpling); rapid swelling developing over days to weeks; and a flattened or inverted nipple not present previously.
⚠️ Clinical Warning: IBC can be missed on standard 2D mammography because there is often no discrete mass to detect. If you develop any combination of these signs over days to weeks — regardless of a recent normal mammogram — seek urgent clinical evaluation. Inflammatory breast cancer can reach Stage III within weeks of symptom onset. This is not a diagnosis to investigate at your convenience.
For the complete clinical presentation and diagnostic criteria, see our guide to inflammatory breast cancer symptoms and urgent warning signs.
Is breast cancer more aggressive in Black women — and what does that actually mean?
TNBC carries a higher mitotic rate, lower differentiation grade, and greater likelihood of lymph node involvement at diagnosis than hormone receptor-positive breast cancer. Black women are diagnosed with TNBC at a higher rate. The combination produces more aggressive average tumor behavior at the population level.
What it does not mean: every Black woman’s cancer is aggressive, or that any individual patient’s prognosis is determined by her race rather than her specific tumor’s pathology report.
✅ Patient Action: Ask your oncologist: “What are my tumor’s ER, PR, and HER2 receptor statuses, and how does that classification change which therapies are available to me?” The receptor status on your pathology report determines your entire treatment menu. You have the right to a clear answer before any treatment discussion proceeds.
🩺 Physician Note: In my experience, newly diagnosed Black patients are rarely told upfront that TNBC is more prevalent in their demographic group — and almost never told why that changes the treatment algorithm. This is information every Black woman with a new breast cancer diagnosis deserves before she leaves her oncologist’s office for the first time.
Breast cancer screening for Black women: when to start and what to ask
Breast cancer screening recommendations are not one-size-fits-all — and for Black women, the standard average-risk protocol may be insufficient. Your screening start age, modality, and frequency depend on your personal risk tier, your family history, and your genetic test results.
Average-risk screening: age 40 annual mammogram (2026 ACS guideline)
For Black women at average risk — no first-degree relatives diagnosed before age 50, no known BRCA pathogenic variant, no prior high-risk biopsy — the 2026 American Cancer Society guidelines recommend annual mammography beginning at age 40.
📊 Clinical Data Point: Per the 2026 American Cancer Society breast cancer screening guidelines: annual mammography is recommended beginning at age 40 for average-risk women. The 2026 NCCN Clinical Practice Guidelines in Oncology recommend annual mammography beginning at age 40 as the clinical standard for average-risk women. — Source: American Cancer Society, 2026; NCCN Clinical Practice Guidelines in Oncology, Breast Cancer, 2026

For a detailed breakdown of screening age thresholds by risk category, see our guide to breast cancer mammogram screening age: what the 2026 guidelines actually say.
Before your next appointment, use our Genetic Risk Assessment Tool to document your personal and family history — the data your physician needs to place you in the correct screening risk tier.
High-risk screening: BRCA carriers and dense breast tissue protocol
For Black women at high risk — defined by confirmed BRCA1 or BRCA2 pathogenic variant status, a first-degree relative diagnosed before age 50, or a lifetime breast cancer risk exceeding 20% by validated risk modeling — the 2026 NCCN guidelines recommend annual breast MRI plus annual mammography beginning at age 25–30, or 10 years before the youngest first-degree relative’s age at diagnosis, whichever comes first.
Dense breast tissue — classified as Category C (heterogeneously dense) or Category D (extremely dense) on BI-RADS — reduces standard 2D mammography sensitivity for detecting TNBC at early stages. Digital breast tomosynthesis (3D mammography) is the preferred screening modality for women with Category C or D density.
✅ Patient Action: At your next mammogram, ask: “What is my breast density classification, and does my result qualify me for supplemental ultrasound or digital tomosynthesis at my next screening cycle?” Your radiologist’s density report is a clinical document, not a footnote.
What genes increase breast cancer risk in Black women (BRCA1, BRCA2, PALB2)
BRCA1 and BRCA2 pathogenic variants confer the highest lifetime breast cancer risk and are specifically associated with triple-negative breast cancer subtype — BRCA1 in particular. PALB2 is a secondary high-risk gene with a documented breast cancer risk elevation sufficient to meet NCCN screening referral criteria in 2026.
🔬 How It Works: BRCA1 and BRCA2 encode tumor suppressor proteins responsible for repairing double-strand DNA breaks. When either gene carries a pathogenic variant, that repair mechanism fails — allowing cancerous mutations to accumulate uncorrected. TNBC is disproportionately associated with BRCA1 mutations because BRCA1-deficient cells are particularly susceptible to estrogen receptor-negative, rapidly proliferating tumor phenotypes.
Our guide to understanding BRCA gene test positive results explains what a positive result or variant of uncertain significance (VUS) means for your screening timeline and treatment eligibility.
When to ask for a screening MRI — and what your insurance requires
Most commercial insurance plans and Medicare cover annual breast MRI for women who meet documented high-risk criteria: typically a lifetime risk above 20% by validated models (Tyrer-Cuzick or IBIS) or a confirmed BRCA1/BRCA2 pathogenic variant. Physician documentation of risk classification is required before insurance authorization.
✅ Patient Action: Before your next appointment, use these exact words with your OB-GYN or primary care physician: “Based on my family history, do I qualify for BRCA genetic testing, and does my risk profile meet the threshold for annual breast MRI under my current insurance plan?” These two questions determine whether you receive standard or high-risk protocol — and whether your insurer covers the difference.
Treatment options for triple-negative breast cancer in Black women
The standard first-line treatment for high-risk early-stage TNBC is neoadjuvant chemotherapy — delivered before surgery to shrink the tumor, assess treatment response, and reduce the risk of distant recurrence. For patients whose tumors meet specific molecular criteria, two FDA-approved agents materially expand the option menu.
Neoadjuvant chemotherapy: the first-line standard for TNBC
Most TNBC patients begin with an anthracycline- and taxane-based chemotherapy regimen delivered before surgery. Achieving a pathologic complete response (pCR) — meaning no residual invasive cancer at the time of surgery — is strongly associated with improved long-term outcomes and is now a primary benchmark in TNBC treatment planning.
For a clinical overview of what chemotherapy involves and what side effects the evidence documents, see our guide to chemotherapy side effects in breast cancer: what patients need to know.
Pembrolizumab for PD-L1-positive TNBC: what your pathology report needs to show
Pembrolizumab (Keytruda), a PD-L1 inhibitor, is FDA-approved for addition to neoadjuvant chemotherapy in high-risk early-stage TNBC, based on the KEYNOTE-522 clinical trial. Eligibility requires that your tumor’s PD-L1 combined positive score (CPS) meets the threshold specified in the current 2026 FDA labeling — the exact CPS threshold must be verified against the updated label at the time of writing.
📊 Clinical Data Point: Per FDA oncology drug approval information for pembrolizumab in TNBC: pembrolizumab added to neoadjuvant chemotherapy demonstrated significantly improved pathologic complete response rates in high-risk early-stage TNBC. All labeling thresholds must be confirmed against the current 2026 FDA label before citing specific CPS values. — Source: U.S. Food and Drug Administration, 2026
Olaparib for BRCA-mutated TNBC: who qualifies and what it means
Olaparib (Lynparza) is an FDA-approved PARP inhibitor for patients with confirmed germline BRCA1 or BRCA2 pathogenic variants and HER2-negative breast cancer. Eligibility requires a validated genetic test confirming germline status — family history alone is not sufficient for prescribing eligibility.
🔬 How It Works: PARP inhibitors exploit a specific vulnerability in BRCA-mutated cancer cells. Normal cells have two functioning DNA repair pathways; BRCA-mutated tumor cells have already lost one. Blocking PARP — the backup repair enzyme — eliminates the only remaining repair mechanism inside the tumor cell, driving its death while sparing normal cells that retain intact BRCA function.
Why where you’re treated determines which options are on the table
NCI-designated comprehensive cancer centers have molecular tumor boards, clinical trial enrollment infrastructure, and established pembrolizumab protocol delivery experience. Community hospitals — where many Black patients receive care due to geographic or insurance barriers — may not have all three. This institutional gap is a documented and independent contributor to the treatment disparity.
✅ Patient Action: Before finalizing care at any facility, ask: “Does this center have a molecular tumor board, and does it have established experience delivering the KEYNOTE-522 pembrolizumab protocol?” If the answer to either question is no, consult a board-certified medical oncologist at an NCI-designated center — in person or via a telehealth oncology platform — for a second opinion before your treatment plan is finalized.
For Black women diagnosed at Stage IV, our guide to metastatic breast cancer treatment options and current FDA-approved regimens details the systemic therapy landscape for advanced disease.
How healthcare access barriers affect breast cancer outcomes for Black women
The mortality gap is not explained by tumor biology alone. Documented systemic barriers — geographic distance from comprehensive cancer centers, insurance coverage gaps, and delays in time-to-diagnosis — each contribute independently to worse outcomes, compounding the biological disadvantage of higher TNBC prevalence.
Time from diagnosis to treatment: how delays affect survival
Delays exceeding 60–90 days from confirmed diagnosis to first treatment are associated with stage progression in biologically aggressive subtypes like TNBC. Black women experience longer median time-to-treatment initiation than white women across multiple healthcare systems — a disparity not attributable to patient reluctance.
⚠️ Clinical Warning: If more than six weeks have passed since your breast cancer diagnosis and you have not received a confirmed treatment plan from a medical oncologist, contact your referring physician immediately and request an urgent referral to an NCI-designated comprehensive cancer center. Do not wait for the next available appointment at a facility that cannot confirm it has molecular tumor board capacity.
Comprehensive cancer centers vs. community hospitals: what the difference means for TNBC
NCI-designated comprehensive cancer centers provide: molecular tumor boards that review receptor profiling and CPS scoring; clinical trial enrollment access; and KEYNOTE-522 pembrolizumab protocol experience. Patients at community hospitals without these capabilities may not receive the full FDA-approved option menu for their diagnosis — not because those options are unavailable, but because the institution lacks the infrastructure to deliver them.
Are there clinical trials specifically enrolling Black women with breast cancer?
Yes. Active trials — including studies specifically designed to address racial disparities in TNBC enrollment — are searchable through the ClinicalTrials.gov registry for active breast cancer studies, filterable by subtype, stage, and location. Clinical trial enrollment is a treatment pathway, not a last resort. Ask your oncologist whether you qualify before a community hospital treatment plan is finalized.
What a caregiver can advocate for on behalf of a Black woman with breast cancer
Three concrete steps before the first oncology appointment:
- Request a written copy of the full pathology report including ER, PR, and HER2 receptor status and any molecular test results that have been ordered.
- Ask the referring physician whether BRCA genetic testing has been ordered and whether a referral to an NCI-designated comprehensive cancer center has been formally considered.
- Verify that the treating facility has experience with neoadjuvant chemotherapy plus pembrolizumab protocol delivery before the first treatment appointment is scheduled.
✅ Patient Action: If geographic or financial barriers limit access to an NCI-designated center, consult a board-certified medical oncologist via a telehealth oncology platform for a second opinion before committing to a community hospital treatment plan. A second opinion is a clinical right, not an insult to the referring physician.
What I tell every Black woman I see about her breast cancer risk
The one question I always answer before any data discussion
The question I hear most often — in almost every clinical setting — is some version of: “Is my cancer worse because I’m Black?”
The clinical answer is direct: TNBC is more prevalent in Black women, and TNBC is biologically more aggressive than hormone receptor-positive breast cancer. That is a documented biological reality. The equally true clinical reality is that the healthcare system has historically failed Black women at the screening stage, the referral stage, and the treatment delivery stage — producing worse outcomes that are not inevitable.
Both truths belong in the same sentence. Neither one cancels out the other.
🩺 Physician Note: Before I share any survival statistic with a patient, I tell her this: population averages describe what happened to other people under different circumstances. Your outcome is shaped by what the clinical decisions look like from this point forward — starting with whether you have all the information, and whether your care team has all the tools.
What I want every Black woman reading this to do this month
Call your OB-GYN this week. Use these exact words: “I want to discuss my breast cancer risk, my screening start age, and whether I qualify for BRCA genetic testing based on my family history.”
If you have already been diagnosed: before agreeing to any treatment plan, ask for three specific pieces of information — your tumor’s PD-L1 CPS score, your germline BRCA mutation status, and whether you are being managed at a center with molecular tumor board access. Those three answers determine your full clinical menu.
Understanding the full range of known breast cancer risk factors that inform an individual risk assessment can help you walk into that conversation prepared.
Frequently asked questions about breast cancer in Black women
1. Why do Black women have a higher risk of dying from breast cancer?
Breast cancer in Black women carries higher mortality rates than in white women due to two simultaneous clinical mechanisms: a substantially higher prevalence of triple-negative breast cancer — a biologically aggressive subtype with a narrower treatment menu than hormone receptor-positive cancers — and documented systemic disparities in screening access, time from symptom to confirmed diagnosis, and delivery of comprehensive cancer center care. Both mechanisms operate at the same time and compound each other’s impact on survival.
2. What is triple-negative breast cancer and how does it specifically affect Black women?
Triple-negative breast cancer lacks estrogen receptors, progesterone receptors, and HER2 protein overexpression — the three targets that hormone therapies and HER2-directed agents require. Tamoxifen, aromatase inhibitors, and trastuzumab are not effective for TNBC. Black women are diagnosed with this subtype at significantly higher rates than white women, narrowing the treatment menu from the point of diagnosis. Consult a board-certified breast oncologist to confirm your receptor status and PD-L1 score before any treatment plan is finalized.
3. When should Black women start getting mammograms?
For average-risk Black women, the 2026 American Cancer Society guidelines recommend annual mammography beginning at age 40. For high-risk women — including BRCA1 or BRCA2 pathogenic variant carriers, or those with a first-degree relative diagnosed before age 50 — the 2026 NCCN guidelines recommend annual breast MRI plus annual mammography beginning at age 25–30, or 10 years before the youngest first-degree relative’s diagnosis age. Consult a board-certified breast oncologist or breast radiologist to confirm your personal screening start age based on your documented risk tier.
4. Is breast cancer more aggressive in Black women?
Triple-negative breast cancer — diagnosed at higher rates in Black women — is biologically more aggressive than hormone receptor-positive breast cancer: it carries a higher mitotic rate, lower differentiation grade, and greater likelihood of lymph node involvement at diagnosis. This subtype prevalence difference explains most of the observed aggressiveness disparity at the population level. An individual patient’s tumor aggressiveness is determined by her specific pathology report, receptor status, and tumor grade — not by her race alone.
5. What genes increase breast cancer risk in Black women?
BRCA1 and BRCA2 pathogenic variants carry the highest lifetime breast cancer risk. BRCA1 is specifically associated with triple-negative breast cancer subtype. PALB2 is a secondary high-risk gene meeting NCCN 2026 screening referral criteria. Genetic testing eligibility is determined by personal and family history — it is not a routine part of every breast cancer workup. Consult a board-certified genetic counselor to determine whether your history qualifies you for BRCA1, BRCA2, and PALB2 testing under current 2026 NCCN guidelines.
6. What are the survival rates for breast cancer in Black women?
Five-year overall survival for breast cancer in Black women is highest at Stage I — where outcomes are strongly favorable across demographic groups — and declines progressively with advancing stage. The disparity between Black and white women’s survival rates is smallest at Stage I and widest at Stage III and Stage IV, where access to comprehensive cancer center resources and molecular-guided therapy selection has the greatest individual impact. Stage at diagnosis, tumor subtype, and treatment setting are the three factors most strongly associated with individual outcome.
7. What treatments are available for triple-negative breast cancer?
For high-risk early-stage TNBC, standard treatment is neoadjuvant anthracycline- and taxane-based chemotherapy, with pembrolizumab (Keytruda) added for patients whose tumors express PD-L1 at a qualifying combined positive score per 2026 FDA labeling. For patients with confirmed germline BRCA1 or BRCA2 mutations, olaparib (Lynparza) is an FDA-approved PARP inhibitor. Consult a board-certified medical oncologist at an NCI-designated comprehensive cancer center to confirm which regimen applies to your specific pathology report and mutation status.
8. Are there clinical trials enrolling Black women with breast cancer?
Yes. Active breast cancer clinical trials — including studies specifically designed to address racial disparities in TNBC enrollment and outcomes — are searchable through the ClinicalTrials.gov registry, filterable by cancer subtype, disease stage, and geographic location. Comprehensive cancer centers have significantly higher clinical trial enrollment availability than community hospitals. Clinical trial participation is a frontline treatment pathway. Ask your board-certified oncologist whether you qualify for an active TNBC trial before finalizing a treatment plan at a community facility.
9. How does healthcare access affect breast cancer outcomes for Black women?
Three independently documented mechanisms worsen outcomes: geographic distance from NCI-designated comprehensive cancer centers with molecular tumor boards and pembrolizumab protocol experience; insurance coverage gaps limiting access to breast MRI screening and genetic testing; and longer median time from initial symptom presentation to confirmed diagnosis. These systemic barriers compound the biological disadvantage of higher TNBC prevalence. Access to molecular tumor profiling and a comprehensive cancer center are the two factors most likely to change an individual patient’s outcome at the treatment stage.
10. What questions should Black women ask their oncologist about breast cancer?
Before agreeing to any treatment plan, ask five questions: What are my tumor’s ER, PR, and HER2 receptor statuses? What is my PD-L1 combined positive score? Have I been tested for germline BRCA1, BRCA2, and PALB2 mutations? Am I eligible for a referral to an NCI-designated comprehensive cancer center? What active clinical trials apply to my specific diagnosis and stage? Consult a board-certified breast oncologist and bring this list to your first appointment — the answers to these questions determine your full treatment menu.
11. Can inflammatory breast cancer occur more often in Black women?
Yes. Inflammatory breast cancer — a rare but rapidly progressing subtype — is diagnosed at higher rates in Black women. IBC presents without a palpable lump. Key warning signs include breast redness, warmth, swelling, heaviness, and peau d’orange skin texture developing over days to weeks — signs that standard mammography can miss because there is no discrete mass to detect. If you develop any of these changes suddenly, consult a board-certified breast oncologist for urgent evaluation. Do not wait for a routine screening appointment.
Your next step starts with one phone call
The data on breast cancer in Black women is not a verdict — it is a description of what has happened to Black women who lacked access to the information, the screening protocols, and the specialized care that changes outcomes.
You now have the information. The biology of TNBC, the staging gap, the BRCA risk architecture, the FDA-approved treatments, the 2026 screening age thresholds, and the five questions that unlock your full clinical menu — this article contains all of it, written by a board-certified gynecologic oncologist.
The next step is the simplest one. Call your OB-GYN or primary care physician this week. Ask for a breast cancer risk assessment. Ask whether you qualify for BRCA testing. If you have already been diagnosed, request three specific pieces of information before agreeing to any plan: your PD-L1 CPS score, your BRCA mutation status, and confirmation that your care setting has molecular tumor board access.
Recognizing early breast cancer signs and what warrants immediate clinical attention is one more tool you can use to act earlier.
Early specialist engagement is not overreaction. It is the most evidence-supported decision any Black woman can make with this diagnosis — or before it.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.