On This Page – Quick Medical Summary
Male breast cancer symptoms most men dismiss as nothing
Most men who find this article believe, at some level, that breast cancer cannot affect their body. That belief — and the diagnostic delay it creates — is the primary reason male breast cancer is found at a later, harder-to-treat stage far more often than it should be.
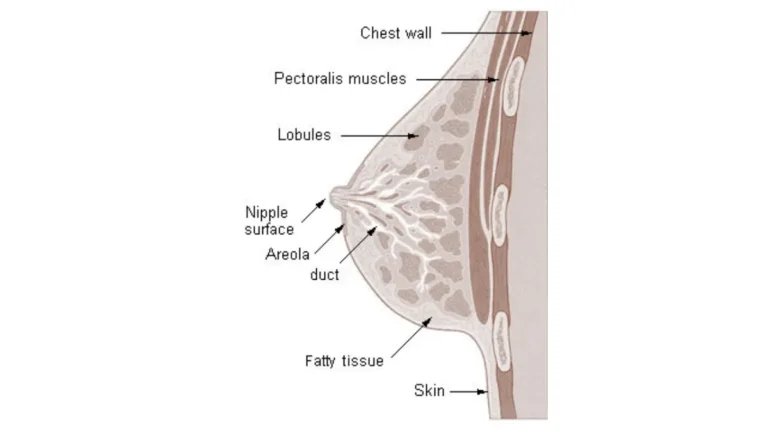
Men have glandular breast tissue. That tissue can become malignant. And because most men attribute the earliest warning signs to a minor injury or a hormonal change, the window for the most effective treatment is frequently missed.
In my clinical experience, male patients who present with breast cancer have almost universally delayed evaluation by more than a year. Every one of them attributed their initial lump to a minor injury or assumed, because every cultural message they had ever received told them so, that this diagnosis was impossible.
It is not impossible. And earlier evaluation meaningfully changes what is available to you.
For the full clinical picture of how staging determines treatment and prognosis, see our guide to breast cancer stages and survival.
ℹ️ Medical Disclaimer: The diagnostic criteria, treatment options, and medication information — including tamoxifen, aromatase inhibitors, and biopsy procedures — discussed in this article reflect current clinical guidelines and are provided for educational purposes only. Diagnostic conclusions, treatment decisions, and medication choices depend on individual patient history, imaging results, biopsy findings, and specialist assessment. Consult a board-certified oncologist or breast surgeon before acting on any clinical information in this article.
What are the warning signs of male breast cancer?
Male breast cancer symptoms include a painless, firm lump beneath or around the nipple, nipple retraction, skin dimpling, and spontaneous nipple discharge — warning signs that most male patients attribute to benign causes and delay reporting by an average of 12 months or longer.
Creative Commons Attribution-Share Alike 4.0 International
📊 Clinical Data Point: Approximately 75–80% of male breast cancer cases present with a palpable lump as the first reported symptom, per 2026 NCI surveillance data. A meaningful proportion present through nipple or skin changes alone, without a detectable mass.
What a malignant breast lump feels like in men
A suspicious breast lump in men is typically:
- Hard and firm — not soft, spongy, or rubbery to the touch
- Non-tender — the absence of pain is a red flag, not reassurance
- Unilateral — present on one side of the chest only
- Fixed — does not move freely under pressure; may feel attached to surrounding tissue or overlying skin
- Irregularly shaped — not smooth or symmetrically rounded
- Located near or beneath the nipple — though eccentric positioning, off-center from the areola, is also common in malignant presentations
None of these characteristics can confirm malignancy. Only imaging and biopsy can do that. But any lump matching two or more of these criteria warrants same-week evaluation.
Symptoms that appear without a lump
Not every breast cancer symptom in men involves a palpable mass. Warning signs that appear without a lump include:
- Nipple retraction — the nipple pulls inward rather than projecting outward
- Spontaneous nipple discharge — particularly bloody or clear fluid; discharge provoked only by squeezing is less clinically urgent than unprovoked discharge
- Skin dimpling or puckering — visible surface changes over the chest or areola
- Paget’s disease of the nipple — eczema-like crusting, scaling, or redness at the areola, frequently misidentified as a dermatological condition and treated with topical creams for a year or more before biopsy is ordered
Understanding the full range of common breast cancer warning signs — including how they differ by presentation type — can help you prepare targeted questions before your first appointment.
When male breast cancer symptoms require same-week evaluation
⚠️ Clinical Warning: Any man who notices a firm, non-tender, unilateral breast lump — regardless of how small — should contact a physician within one week. Painless does not mean harmless. A small lump is not a safe lump. Watchful waiting is not an appropriate management strategy for an undiagnosed breast mass in a male patient.
Before your appointment, use our Symptom Checker to document exactly what you are experiencing, when it began, and how it has changed over time. Bringing this timeline to your appointment directly informs the imaging decision.
The American Cancer Society’s male breast cancer patient guide provides a complementary overview of warning signs and next steps for patients and caregivers.
✅ Patient Action: Before your appointment, write down when you first noticed the lump or change, whether it has grown or shifted, and whether any skin or nipple changes have appeared alongside it. A written symptom timeline is one of the most useful things you can bring to a physician evaluating a breast complaint.
Gynecomastia vs. male breast cancer: how to tell the difference
Gynecomastia — benign enlargement of male breast tissue caused by hormonal imbalance — is the most common reason men dismiss a breast change as nothing. It is also the most clinically dangerous reason.
The two conditions can feel similar on self-examination. They cannot be reliably differentiated without clinical evaluation and imaging.
🔬 How It Works: Gynecomastia develops when the androgen-to-estrogen ratio in the male body shifts — through natural testosterone decline with age, liver dysfunction that impairs estrogen catabolism, or certain medications including antihypertensives, antiulcer drugs, and hormone therapies. The result is soft, bilateral glandular tissue growth beneath the areola. This is physiologically distinct from a malignant mass, but the two can overlap on self-examination — which is why clinical evaluation, not self-assessment, is the only reliable differentiator.
Physical examination features of gynecomastia
Gynecomastia typically presents as soft or rubbery bilateral breast tissue, centrally located directly beneath the areola on both sides, and often tender or sensitive to pressure. It tends to be symmetric and is associated with a known or identifiable hormonal trigger. Tenderness is a common feature — not a reassuring one — because malignant lumps, by contrast, are characteristically non-tender.
Red flags that distinguish a malignant lump from gynecomastia
| Feature | Gynecomastia | Malignant Lump |
|---|---|---|
| Consistency | Soft to rubbery | Hard, firm |
| Laterality | Bilateral (both sides) | Unilateral (one side only) |
| Location | Central, directly subareolar | May be eccentric, off-center |
| Tenderness | Usually present | Usually absent |
| Mobility | Moves freely under pressure | Fixed to tissue or skin |
| Skin changes | Absent | Dimpling or retraction possible |
| Nipple involvement | Rarely | Retraction or discharge possible |
Invasive ductal carcinoma is the predominant histologic type in male breast cancer and the malignancy most likely to underlie a unilateral, hard, fixed lump. For more on the clinical implications of this diagnosis, see our article on invasive ductal carcinoma: cure rate and treatment by stage.
Why self-diagnosis is unreliable and what evaluation actually involves
The table above describes characteristic presentations. Exceptions exist in both directions. A malignant lump can occasionally be tender. Gynecomastia can present unilaterally. These exceptions are precisely why self-examination is a screening behavior — not a diagnostic tool.
✅ Patient Action: Any unilateral breast lump, any lump that is eccentric to the nipple, or any lump associated with nipple retraction or skin changes must be evaluated by a board-certified breast surgeon. Do not attempt to differentiate gynecomastia from malignancy on the basis of tenderness alone — tenderness is an unreliable differentiator in clinical practice.
The NCI’s male breast cancer treatment information page outlines the physical examination and imaging criteria applied in clinical evaluation of male breast presentations.
How male breast cancer is diagnosed: what to expect
Male breast cancer diagnosis follows a four-step clinical pathway — physical examination, diagnostic imaging, tissue biopsy, and pathologic staging — with each step determined by findings from the prior, per the 2026 NCCN Clinical Practice Guidelines in Oncology.
Step 1: Clinical examination and imaging
- Physical breast examination — the physician manually assesses the mass for size, consistency, mobility, skin involvement, and axillary lymph node status
- Diagnostic mammogram — ordered as the initial imaging study in most presentations; sensitivity is somewhat lower in men than women due to reduced tissue volume
- Breast ultrasound — frequently the preferred primary imaging modality in male patients; reliably distinguishes solid masses from cysts with high resolution at low tissue depth
📊 Clinical Data Point: Per 2026 NCCN Clinical Practice Guidelines in Oncology, any palpable breast mass in a male patient warrants formal diagnostic evaluation — not observation or watchful waiting. Imaging modality selection is determined by presentation characteristics.
For context on how breast cancer mammogram screening guidelines apply by age and risk category, our dedicated guide explains when diagnostic versus screening mammography is indicated.
Step 2: Biopsy — what the procedure involves
If imaging identifies a suspicious solid mass, core needle biopsy is the preferred tissue sampling technique. It uses local anesthesia, takes approximately 15–20 minutes, and recovers sufficient tissue for full receptor profiling — estrogen receptor (ER), progesterone receptor (PR), and HER2 status — results that determine which systemic therapy carries the strongest evidence base.
Fine-needle aspiration cytology may precede core biopsy in certain presentations. A positive biopsy confirms malignancy. It does not confirm spread.
🩺 Physician Note: When I review biopsy results with male patients for the first time, the question I hear most often is: “Does positive mean it has spread?” It does not. Biopsy answers one question — whether the tissue contains cancer cells. How far the disease has traveled is answered separately through staging imaging and, often, a sentinel lymph node evaluation. These are two distinct steps, and conflating them is one of the most common sources of unnecessary panic in the days after a positive biopsy result.
Step 3: What biopsy results show and what happens next
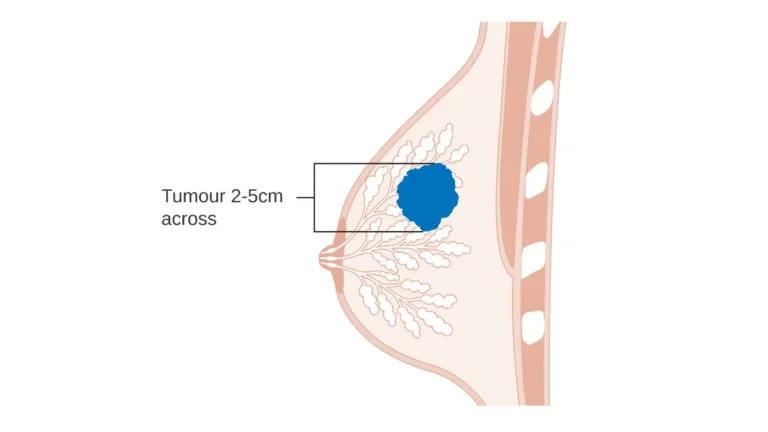
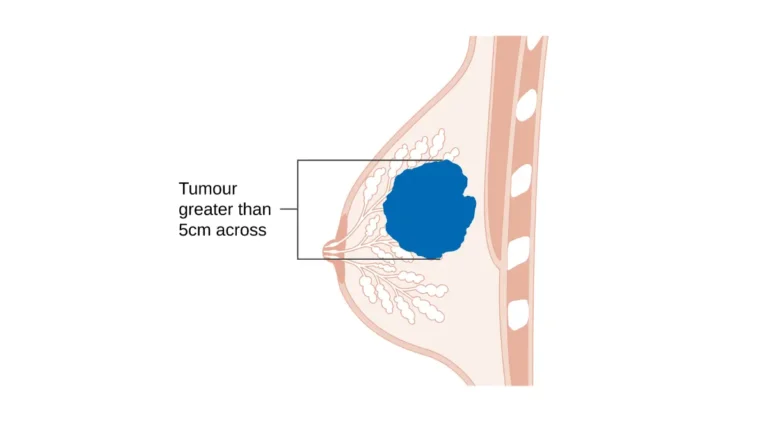
A confirmed positive biopsy triggers full TNM staging — tumor size (T), regional lymph node involvement (N), and distant metastasis (M) — which produces the stage classification that determines the entire treatment plan.
For a step-by-step guide to understanding your biopsy results timeline and report, including what each result category means and how long each stage of evaluation typically takes, our dedicated guide covers the full process.
✅ Patient Action: If your primary care physician does not order imaging after you report a palpable breast lump, request a referral to a board-certified breast surgeon or oncologist. Per 2026 NCCN guidelines, a palpable breast mass in a man warrants formal diagnostic evaluation — not monitoring at home.
What puts men at higher risk for breast cancer?
Male breast cancer risk is driven by a combination of genetic, hormonal, and environmental factors. The highest-risk profiles in male patients include BRCA2 mutation carriers, men with Klinefelter syndrome, and those over age 60.
Genetic risk: BRCA2 mutation and male breast cancer
BRCA2 mutation is the most clinically significant hereditary risk factor for male breast cancer. Men receive their BRCA2 result most commonly because a female family member was tested — not because their own breast cancer risk was evaluated. That gap has clinical consequences.
📊 Clinical Data Point: Men carrying a BRCA2 mutation face a lifetime breast cancer risk of approximately 6–8%, compared to less than 0.1% in the general male population — a difference of 60–80 times background risk, per 2026 clinical genetic data.
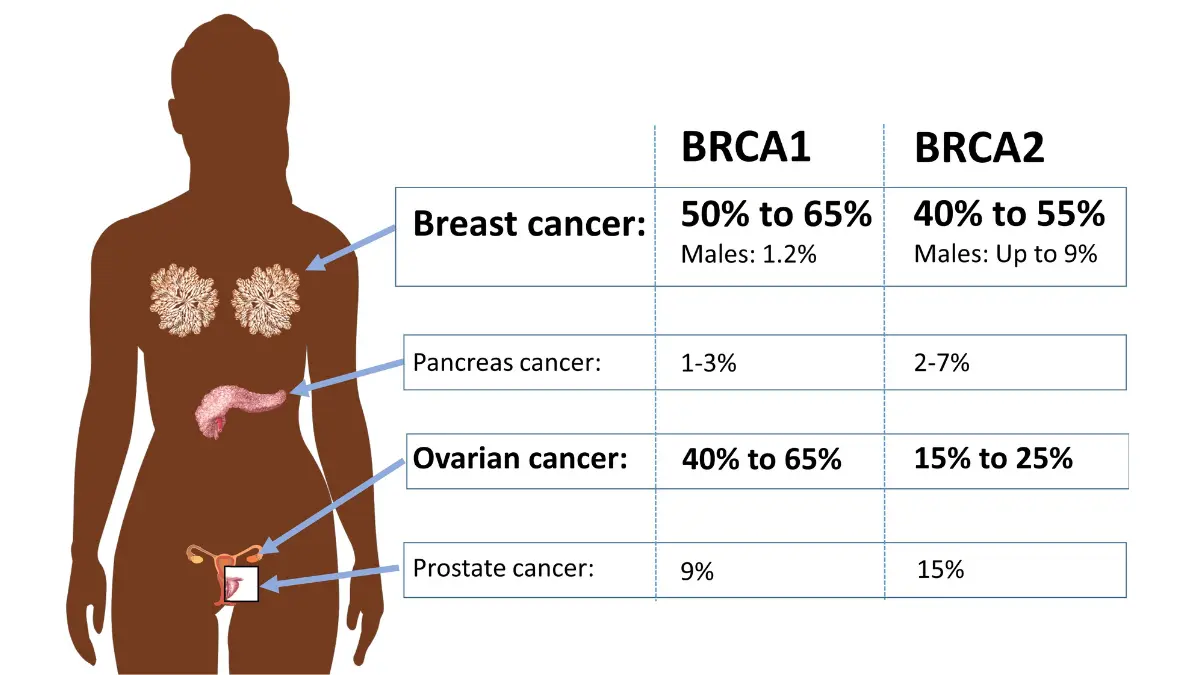
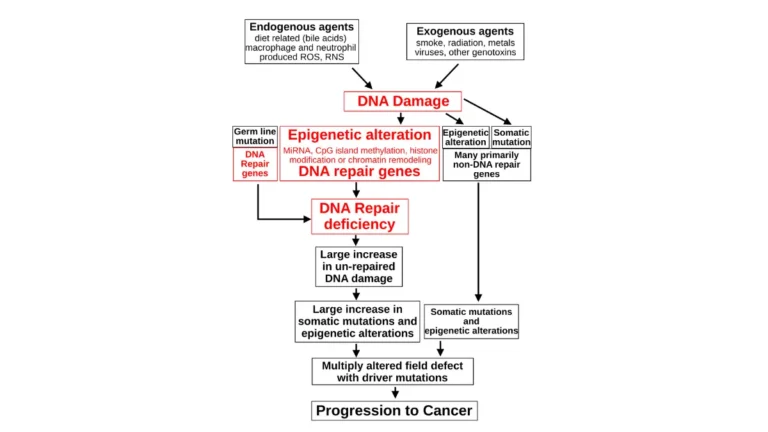
🔬 How It Works: BRCA2 encodes a tumor suppressor protein essential for DNA double-strand break repair. When this gene is mutated, breast epithelial cells accumulate DNA damage that normal repair mechanisms cannot correct — eventually driving malignant transformation. The mechanism is identical to the one that elevates breast and ovarian cancer risk in women carrying BRCA2 mutations. Men who test positive carry the same biological vulnerability; they are simply never told to look for it.
If you have received a positive BRCA2 result and are uncertain what it means for your personal cancer risk, our article on what a positive BRCA gene test result means covers the clinical implications and recommended next steps.
Non-genetic risk factors for breast cancer in men
Additional breast cancer risk factors in male patients include:
- Klinefelter syndrome (47,XXY karyotype) — extra X chromosome disrupts androgen-to-estrogen balance; estimated 20–50 times background male breast cancer risk
- Chronic liver disease — impairs hepatic estrogen catabolism, raising circulating estrogen levels
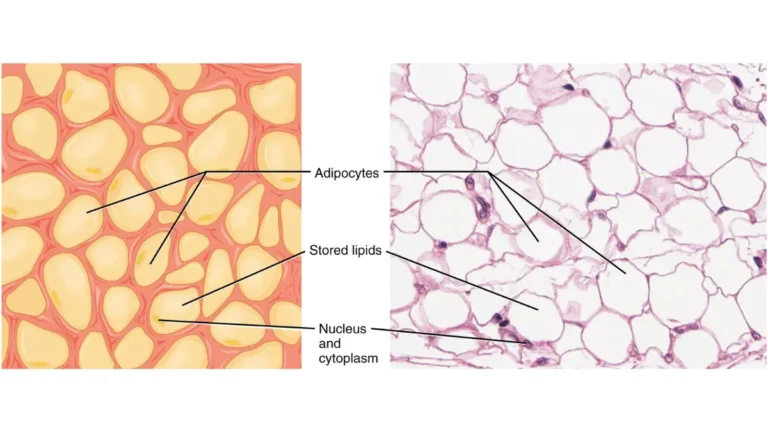
- Obesity — increases peripheral conversion of androgens to estrogen via aromatization in adipose tissue
- Prior chest radiation exposure — a documented carcinogenic exposure to breast tissue
- Exogenous estrogen therapy — historically used for prostate cancer treatment; relevant in current gender-affirming hormone therapy contexts
For a comprehensive review of how each breast cancer risk factor is quantified and how individual risk profiles are assessed clinically, our dedicated guide covers both male and female risk stratification.
Who should consider genetic counseling and hereditary cancer screening
Men with a first-degree female relative diagnosed with premenopausal breast cancer or ovarian cancer should discuss BRCA2 genetic testing with a board-certified genetic counselor or oncologist. Carrier status changes both surveillance frequency and risk-reduction strategy per 2026 NCCN guidelines.
✅ Patient Action: Use our Genetic Risk Assessment Tool to evaluate your hereditary cancer risk based on family history and known genetic factors. Bring the results to your next physician appointment as a structured starting point for a genetic counseling conversation.
Male breast cancer survival rates by stage: what the data shows
Male breast cancer survival is directly and decisively stage-dependent. Men diagnosed at Stage I have an estimated 5-year relative survival rate exceeding 95%. By Stage IV, that figure falls to approximately 24%.
The difference between those two numbers is, in large part, a function of how long a man waited before seeking evaluation.
📊 Clinical Data Point:
| Stage | Disease Extent | 5-Year Relative Survival Rate |
|---|---|---|
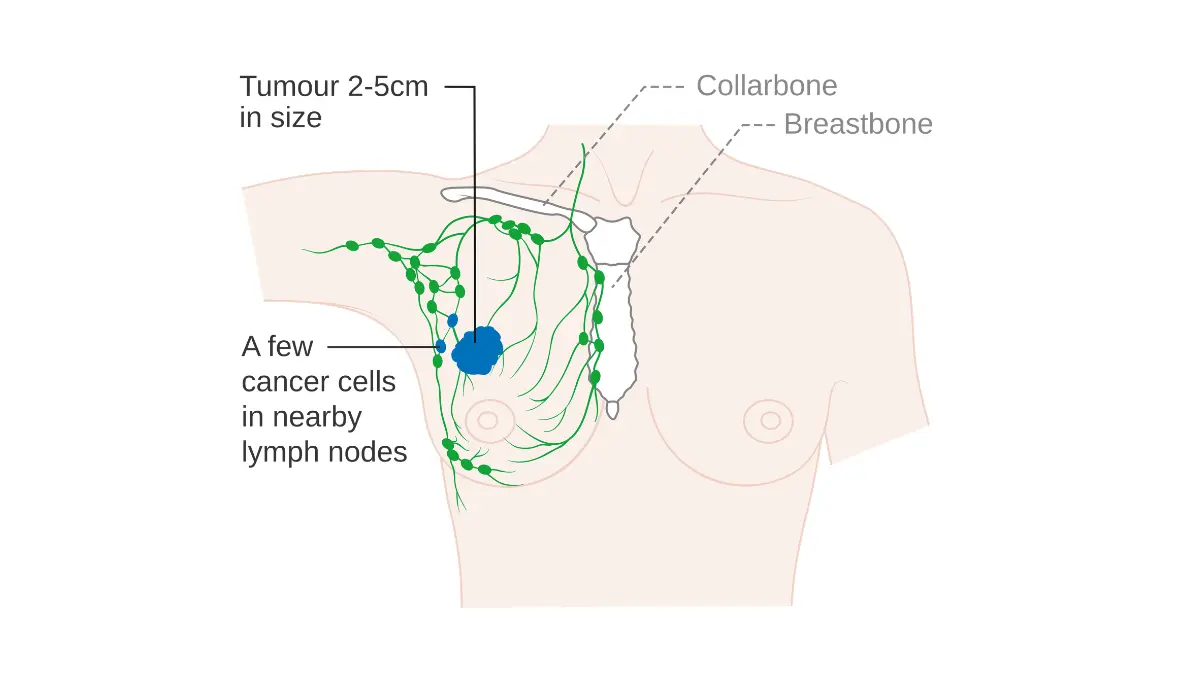
| Stage I | Localized — tumor confined to breast tissue | ~96% |
| Stage II | Regional — limited lymph node involvement | ~84% |
| Stage III | Regional — extensive lymph node or chest wall involvement | ~66% |
| Stage IV | Distant — metastatic spread confirmed | ~24% |
Source: NCI SEER database, 2026 data.
For a deeper analysis of breast cancer survival rates by stage across the full patient population — including how survival trends have shifted over recent treatment cycles — our dedicated guide covers the complete SEER data landscape.
Creative Commons Attribution-Share Alike 4.0 International
Why male breast cancer is often diagnosed at a later stage than female breast cancer
The survival differential between Stage I and Stage III above is not primarily a feature of male disease biology. It reflects the diagnostic delay pattern that characterizes male breast cancer presentation.
Men present at a later stage on average not because male breast cancer grows faster or behaves more aggressively at equivalent stage — but because men wait. The 12–18-month average delay documented in clinical series is a behavioral and awareness gap. Every stage earlier at diagnosis represents a meaningful upward shift in the survival probability table above.
The NCI SEER cancer statistics database provides the 2026-published incidence and survival data underlying these figures.
What happens after a male breast cancer diagnosis — and why acting early matters
A note from the physician author: what male patients most often ask
The question I hear most from male patients after a breast cancer diagnosis is this: “Did I wait too long?”
In most cases — even men who delayed evaluation by 12 months or more — meaningful treatment options remain available. But the stage at which treatment begins is directly correlated with how long the wait was. Earlier detection does not simply feel better. It changes what is available.
If you are reading this as a partner or spouse of a man who has been dismissing a lump: your concern is clinically warranted. And this article exists, in part, to give you the evidence-based case to make.
Treatment options for male breast cancer at a glance
Male breast cancer treatment follows the same general framework as female breast cancer, calibrated to receptor status and stage:
- Surgery — modified radical mastectomy is the most common surgical approach in male patients; breast-conserving surgery is appropriate in select presentations based on tumor-to-breast-volume ratio
- Adjuvant endocrine therapy — tamoxifen is the standard agent for hormone receptor-positive (ER+) disease, which represents the majority of male breast cancers; aromatase inhibitors are less effective in men due to incomplete estrogen suppression without concurrent GnRH analog
- Chemotherapy — indicated in node-positive or high-risk presentations; regimen selection is guided by receptor profile and staging
- Radiation therapy — added following surgery in locally advanced cases or when chest wall involvement is present
Our dedicated comparison of how tamoxifen compares to aromatase inhibitors in breast cancer treatment explains the pharmacological basis for tamoxifen preference in male patients. For a full breakdown of surgical options, see our guide to lumpectomy vs. mastectomy.
Clinical trials and investigational options for male breast cancer
📊 Clinical Data Point: Male breast cancer represents approximately 1% of all breast cancer diagnoses in the United States, with an estimated 2,800–3,000 new cases per year in American men, per 2026 NCI data.
Men diagnosed with breast cancer who meet eligibility criteria may qualify for investigational treatment programs. Reviewing active male breast cancer clinical trials on ClinicalTrials.gov provides the current registry of ongoing studies.
✅ Patient Action: Before agreeing to any systemic treatment, ask your oncologist three specific questions: (1) What is my tumor’s hormone receptor status — ER, PR, and HER2? (2) Does my stage and receptor profile warrant chemotherapy in addition to surgery? (3) Is tamoxifen the appropriate endocrine agent for my case, or is a clinical trial a better option based on my presentation?
Frequently asked questions about male breast cancer symptoms
1. What does a male breast cancer lump feel like?
A malignant breast lump in men is typically hard, firm, and non-tender — fixed to surrounding tissue or skin, present on one side only, and often positioned near or beneath the nipple. Unlike the soft, bilateral, centrally placed tenderness of gynecomastia, a malignant lump does not move freely under pressure and does not respond to anti-inflammatory treatment. Consult a board-certified breast surgeon for evaluation of any firm, persistent, unilateral breast lump.
2. Can men get breast cancer without a lump?
Yes. A meaningful proportion of male breast cancer cases present without any palpable mass. Nipple retraction — when the nipple pulls inward — spontaneous nipple discharge, particularly if bloody or clear, Paget’s disease of the nipple (eczema-like scaling at the areola), and skin dimpling over the chest can all represent a malignant presentation without a detectable lump. Any nipple or skin change that persists beyond two weeks warrants evaluation by a board-certified physician.
3. What is the survival rate for male breast cancer?
Male breast cancer survival is stage-dependent. Per 2026 NCI SEER data, estimated 5-year relative survival rates are approximately 96% for Stage I, 84% for Stage II, 66% for Stage III, and 24% for Stage IV disease. Survival varies further by receptor status, tumor grade, and treatment received. The stage at diagnosis is the single most modifiable variable — and it is determined largely by how quickly evaluation is sought after symptoms appear.
4. Is male breast cancer hereditary?
BRCA2 mutation is the most significant hereditary risk factor for male breast cancer. Men carrying a BRCA2 mutation face an estimated lifetime breast cancer risk of approximately 6–8%, compared to less than 0.1% in the general male population — a difference of 60–80 times background risk. Approximately 10–15% of male breast cancers are associated with an inherited mutation. Men with a first-degree female relative with breast or ovarian cancer should discuss genetic testing with a board-certified genetic counselor or oncologist.
5. How is male breast cancer diagnosed?
Male breast cancer diagnosis follows a sequential pathway: physical breast examination, then diagnostic mammogram and/or ultrasound, followed by core needle biopsy for tissue sampling and full receptor profiling, and finally TNM pathologic staging. Each step is determined by findings from the prior step, per 2026 NCCN guidelines. A positive biopsy confirms malignancy — additional staging imaging separately answers whether and how far the disease has spread. Consult a board-certified oncologist before proceeding with any biopsy or staging evaluation.
6. What is the difference between gynecomastia and male breast cancer?
Gynecomastia typically presents as soft, bilateral, tender tissue centrally beneath the areola — driven by an androgen-to-estrogen imbalance. A malignant breast lump is typically hard, unilateral, non-tender, and fixed to surrounding tissue, and may sit eccentrically off-center from the nipple. These are characteristic presentations — exceptions exist in both directions. Because self-examination cannot reliably differentiate the two, any firm unilateral lump must be evaluated by a board-certified breast surgeon regardless of tenderness.
7. At what age do men usually get breast cancer?
The median age at male breast cancer diagnosis is approximately 67–72 years per 2026 NCI SEER data, with risk increasing progressively after age 50. Men with BRCA2 mutations or Klinefelter syndrome may develop breast cancer at younger ages. Men aged 40 and over with a known genetic or familial risk factor should discuss risk-stratified monitoring with a board-certified oncologist or genetic counselor, rather than waiting for a symptom to appear.
8. How common is breast cancer in men?
Male breast cancer accounts for approximately 1% of all breast cancer diagnoses in the United States, with an estimated 2,800–3,000 new cases annually among American men per 2026 NCI data. Despite its relative rarity, the condition carries a significant diagnostic delay burden — men wait an average of 12 months or more before seeking evaluation, contributing to a later-stage distribution at diagnosis compared to female breast cancer.
9. Should a man be worried about a breast lump?
Any firm, non-tender, unilateral breast lump in men warrants physician evaluation — not because most lumps are malignant (many are not), but because self-examination cannot reliably distinguish a malignant from a benign presentation. Male breast cancer symptoms — particularly a painless, fixed lump — are frequently dismissed for months to years, contributing to a later average stage at diagnosis. Contact a board-certified breast surgeon or oncologist within one week of noticing any persistent, firm breast change.
10. What are the treatment options for male breast cancer?
Male breast cancer treatment is guided by hormone receptor status and disease stage. Surgery — most commonly modified radical mastectomy — is the primary intervention. For ER-positive disease, tamoxifen is the standard adjuvant endocrine agent per 2026 NCCN guidelines; aromatase inhibitors are less effective in men due to incomplete estrogen suppression without concurrent GnRH analog therapy. Chemotherapy is added in node-positive or high-risk cases. Radiation follows surgery in locally advanced presentations. Consult a board-certified oncologist before making any treatment decision.
11. Does male breast cancer have the same symptoms as female breast cancer?
Male breast cancer shares the same core warning signs as female breast cancer — a palpable lump, nipple retraction, nipple discharge, skin dimpling, and Paget’s disease of the nipple — because the underlying cancer biology is similar. The critical clinical difference is not symptom profile but patient response: male patients dismiss these symptoms at a significantly higher rate, contributing to a later average stage at diagnosis. Any persistent chest or nipple symptom in a man should be evaluated promptly by a board-certified physician.
Male breast cancer is rare — but the symptoms are real, and early action matters
Male breast cancer is rare. It is also real, detectable, and carries the same biological warning signs as female breast cancer — signs that appear weeks to months before the disease advances to a harder-to-treat stage.
If anything in this article describes a symptom you have been dismissing, the appropriate next step is a physician evaluation. A firm, non-tender, unilateral breast lump does not become less likely to be malignant because you wait.
A board-certified breast surgeon or oncologist can evaluate any breast change with imaging and, if warranted, biopsy — typically within one to two weeks of a referral.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.