On This Page – Quick Medical Summary
You’ve just been diagnosed with breast cancer during pregnancy — here’s what to do first
Breast cancer and pregnancy can coexist — and in most cases, effective treatment is possible without harming your baby. A diagnosis of pregnancy-associated breast cancer (PABC) arrives with two fears at once: fear for your own survival, and fear for your child. You are not facing an impossible choice.
If you’ve noticed a new breast change during pregnancy and aren’t certain it requires urgent evaluation, use our Symptom Checker to assess whether your symptoms need same-day clinical attention. For a complete overview of which breast changes are red flags during pregnancy, our guide to breast cancer warning signs that warrant immediate evaluation covers every sign to watch for.
⚠️ Clinical Warning: A new breast lump, nipple discharge, skin dimpling, or persistent axillary swelling during pregnancy should never be attributed to normal hormonal changes without clinical evaluation. Contact a board-certified gynecologic oncologist within 48 hours — delayed diagnosis is the most common and most preventable cause of worse outcomes in PABC.
ℹ️ Medical Disclaimer: The diagnostic criteria, chemotherapy protocols, surgical options, treatment timing frameworks, medication safety data, and survival information discussed in this article reflect current clinical guidelines and are provided for educational purposes only. Diagnostic conclusions, treatment decisions, and medication choices depend on your specific tumor biology, gestational age, hormone receptor status, HER2 status, nodal involvement, and overall health. Consult a board-certified gynecologic oncologist and a maternal-fetal medicine specialist before acting on any clinical information in this article. This article does not constitute a determination of insurance coverage for any treatment or procedure.
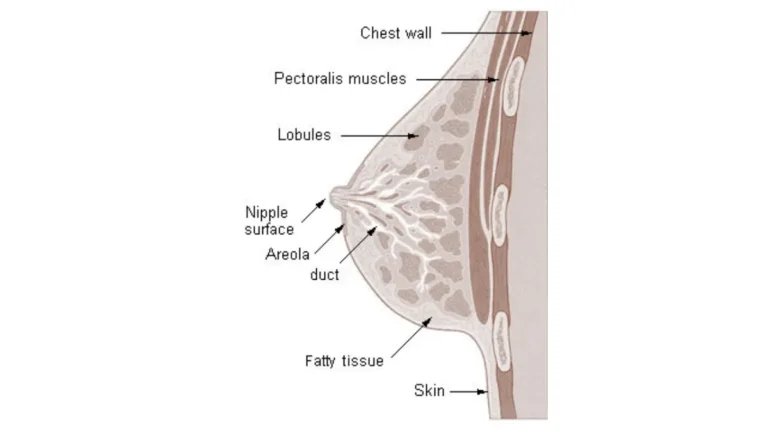
What is pregnancy-associated breast cancer and how is it diagnosed safely?
Pregnancy-associated breast cancer (PABC) is defined as breast cancer diagnosed during pregnancy or within 12 months of delivery — making it the most common malignancy diagnosed during gestation.
📊 Clinical Data Point: PABC occurs in approximately 1 in 3,000 pregnancies — Source: National Cancer Institute, 2026.
Normal pregnancy changes — breast engorgement, increased glandular density, and hormonal stimulation — can mask a growing tumor on clinical examination and reduce imaging sensitivity. This is why PABC is often diagnosed at a later stage than breast cancer in non-pregnant patients: not because the cancer grows faster, but because the signs are more easily overlooked.
Why pregnancy makes breast cancer harder to detect
Pregnant breast tissue is denser and more vascular, which reduces the accuracy of both clinical breast examination and standard ultrasound. When ultrasound findings are equivocal, MRI without gadolinium contrast is the recommended next imaging modality per 2026 ACOG guidance. Gadolinium is avoided during pregnancy due to limited data on fetal exposure at placental crossing concentrations — this is a precautionary limitation, not a confirmed harm.
Which breast cancer subtypes are most commonly diagnosed during pregnancy
Invasive ductal carcinoma is the most common histologic subtype in PABC. Hormone receptor-positive (HR+), triple-negative, and HER2-positive disease all occur during pregnancy. A full receptor panel — estrogen receptor (ER), progesterone receptor (PR), and HER2 — must be performed on all PABC biopsy specimens, because receptor status determines every treatment decision that follows.
How a safe diagnosis is confirmed without harming the fetus
Core needle biopsy under local anesthesia, guided by ultrasound, is considered safe in all three trimesters and is the standard confirmatory diagnostic step. This procedure should not be delayed based on gestational age — waiting for delivery to confirm a diagnosis adds weeks to a timeline that may not allow for delay.
Once your biopsy is confirmed, understanding your cancer’s stage is the most important next step. Our complete guide to breast cancer stages and what each stage means for your treatment plan explains how staging determines the sequence and urgency of your options. If you have a personal or family history of breast or ovarian cancer, use our Genetic Risk Assessment Tool to evaluate your BRCA1/BRCA2 mutation status — a result that directly influences the surgical approach your oncologist recommends in PABC.
For supplementary clinical detail on staging protocols and imaging safety standards used at NCI-designated cancer centers, see the National Cancer Institute’s clinical overview of breast cancer during pregnancy
✅ Patient Action: If you notice a new breast lump, nipple change, or axillary swelling during pregnancy, ask your OB the following at the same appointment: “I want a breast ultrasound today and a same-day referral to a breast surgical oncologist — not a wait-and-watch approach.” Do not accept watchful waiting as an answer for a new, persistent breast mass during pregnancy.
Is chemotherapy safe during pregnancy? A trimester-by-trimester breakdown
Chemotherapy safety during pregnancy depends entirely on gestational age. First-trimester exposure carries the highest fetal risk due to active organogenesis, while administration from the second trimester onward is generally considered clinically acceptable under specialist supervision per 2026 NCCN guidelines.
🔬 How It Works: Organogenesis — the formation of fetal organ systems from undifferentiated cells — occurs primarily between weeks 4 and 10 of gestation. Cytotoxic chemotherapy agents interfere with rapid cell division, making this the most vulnerable window for malformation risk. After week 14, organ formation is complete and the primary biological process shifts to fetal growth, which substantially reduces teratogenic risk for most chemotherapy agents.
First trimester: why chemotherapy is avoided before week 14
In my clinical practice, the first question every newly diagnosed pregnant patient asks is whether chemotherapy will harm her baby. The honest answer depends entirely on gestational age. Cytotoxic chemotherapy before week 14 carries a major fetal malformation risk estimated between 10–20%, a threshold that makes first-trimester administration clinically unacceptable except in life-threatening emergencies.
Second and third trimester: which regimens are considered safe
| Chemotherapy Agent | Trimester 1 | Trimesters 2–3 | Key Clinical Note |
|---|---|---|---|
| Doxorubicin + Cyclophosphamide (AC regimen) | Contraindicated | Generally acceptable after week 14 | Most studied regimen in PABC; major malformation rate estimated <4% after week 14 |
| Taxanes (paclitaxel, docetaxel) | Contraindicated | Acceptable in selected cases per specialist assessment | Less 2026 fetal safety data than AC |
| Trastuzumab (Herceptin) | Contraindicated | Contraindicated | Causes oligohydramnios and fetal renal development disruption — all trimesters |
| Tamoxifen | Contraindicated | Contraindicated | Teratogenic; defer all endocrine therapy until after delivery |
Doxorubicin (Adriamycin) + cyclophosphamide — the AC regimen — is the most studied chemotherapy combination in pregnancy. It is the standard first-line choice for eligible second- and third-trimester patients at major cancer centers with PABC experience.
Drugs contraindicated throughout pregnancy: trastuzumab and endocrine therapy
Trastuzumab (Herceptin) is contraindicated in all three trimesters. Its mechanism of fetal harm involves disruption of HER2-mediated fetal renal tubular development, producing oligohydramnios — a dangerous reduction in amniotic fluid — at a rate that makes exposure in any trimester unacceptable. Tamoxifen is similarly contraindicated throughout pregnancy due to documented teratogenicity in multiple 2026 follow-up analyses.
Patients with HER2-positive disease diagnosed during pregnancy face a specific targeted therapy gap — our guide to HER2-positive breast cancer treatment and what targeted therapy means for your plan covers the complete post-delivery treatment sequence. For a full overview of how chemotherapy is structured across all breast cancer subtypes, our guide to breast cancer chemotherapy protocols and what each regimen targets provides essential background.
For the evidence base behind second-trimester chemotherapy administration and required fetal monitoring protocols, see the American College of Obstetricians and Gynecologists’ clinical guidance on cancer treatment during pregnancy
✅ Patient Action: Before agreeing to any chemotherapy regimen during pregnancy, ask your oncologist three specific questions: (1) What is my exact gestational age, and does it fall within the safe treatment window per 2026 NCCN guidelines? (2) Has my tumor been fully profiled for ER, PR, HER2, and histologic grade — and does my subtype allow any delay? (3) Is a maternal-fetal medicine specialist co-managing my chemotherapy plan from the first cycle?
Surgery for breast cancer during pregnancy: what’s possible and when
Both modified radical mastectomy and lumpectomy can be performed safely during pregnancy, with the second trimester (weeks 14–28) identified as the optimal surgical window in 2026 clinical protocols. Organogenesis is complete, fetal anesthetic risk is at its lowest point relative to gestational age, and the uterus has not yet significantly restricted the surgical field.
🔬 How It Works: General anesthesia administered during the second trimester is managed with continuous fetal heart rate monitoring and optimized maternal positioning to maintain adequate placental blood flow. The selection of specific anesthetic agents requires input from a maternal-fetal medicine specialist before surgery — not as a formality, but because some agents cross the placenta at concentrations requiring real-time fetal monitoring protocols.
Mastectomy vs. lumpectomy: which is safer during pregnancy?
Both procedures carry comparable maternal and fetal safety profiles in the second trimester. The clinical distinction is that lumpectomy is typically followed by radiation therapy — and radiation must be deferred until after delivery in all pregnant patients. For patients who cannot accept a post-delivery radiation phase, mastectomy becomes the more practical single-stage surgical solution.
For a complete comparison of long-term outcomes, reconstruction options, and what changes a surgeon’s recommendation, our guide to lumpectomy vs. mastectomy — the factors that determine the right choice covers every clinical variable.
The optimal trimester for breast cancer surgery — and why
The second trimester is preferred. First-trimester surgery should be deferred until week 14 when tumor biology allows a brief delay, because the organogenesis window is not yet closed. Third-trimester surgery is technically feasible but carries increased anesthesia complexity due to aortocaval compression from the gravid uterus — manageable, but requiring additional maternal-fetal medicine planning.
How anesthesia and sentinel node biopsy are safely modified during pregnancy
Sentinel lymph node biopsy technique differs in pregnant patients. Technetium-99m — a low-radiation radioisotope — is considered safe during pregnancy per 2026 NCCN protocols because fetal radiation exposure from this agent falls well below the threshold associated with developmental harm. Blue dye mapping agents — isosulfan blue and methylene blue — are avoided during pregnancy due to anaphylaxis risk and the absence of confirmed 2026 fetal safety data for either agent.
✅ Patient Action: Before scheduling any breast cancer surgery during pregnancy, confirm two non-negotiable requirements with your surgical team: (1) A maternal-fetal medicine specialist must be involved in pre-operative planning — not consulted after the fact. (2) Your surgical oncologist must have documented experience with pregnancy-associated breast cancer cases. If either condition is not met, request a transfer to an NCI-designated cancer center.
When should treatment start — and does the pregnancy need to end early?
Treatment delay is not universally safe. Your oncologist evaluates tumor biology — hormone receptor status, HER2 status, histologic grade — gestational age at diagnosis, and nodal involvement before determining whether any deferral is clinically acceptable. In triple-negative or high-grade disease, a delay beyond four weeks from confirmed diagnosis is generally not recommended per 2026 NCCN guidelines.
How your oncologist decides when to start treatment — the exact clinical factors
Brief deferral is typically acceptable in: low-grade tumors, hormone receptor-positive disease, clinically early-stage findings, and patients approaching 35 weeks gestation where delivery is imminent. Deferral is generally not acceptable in: triple-negative breast cancer, high-grade disease, node-positive findings at any gestational age, and first- or early second-trimester diagnoses in any aggressive subtype.
Triple-negative disease during pregnancy carries the narrowest acceptable delay window of any molecular profile — our guide to triple-negative breast cancer prognosis and why treatment timing is different for this subtype explains the specific biological urgency. If your care team has asked you to monitor fetal growth between prenatal appointments during active treatment, use our Fetal Growth Percentile Calculator to track your baby’s size against standard gestational benchmarks.
What happens when breast cancer is diagnosed in the third trimester?
At 34–36 weeks gestation with a high-grade or node-positive diagnosis, early delivery may be considered after assessment of fetal lung maturity and NICU availability. This decision requires consensus between your gynecologic oncologist and your maternal-fetal medicine specialist — it is not a unilateral oncology recommendation. Earlier in the third trimester, chemotherapy can often be continued through pregnancy with fetal monitoring.
Does breast cancer treatment ever require ending the pregnancy?
Pregnancy termination is rarely if ever required or recommended for breast cancer treatment, per 2026 NCCN guidelines. Early delivery at 35 weeks or later to initiate full systemic therapy is a distinct clinical decision — sometimes necessary, fundamentally different from termination, and only appropriate after maternal-fetal medicine review.
📊 Clinical Data Point: Per 2026 NCCN guidance, delivery before 35 weeks gestational age is generally not recommended solely to facilitate chemotherapy administration — the risks of significant prematurity typically outweigh the benefit of earlier treatment access — Source: NCCN 2026.
Patients seeking a PABC-specific clinical trial can search the registry of clinical trials currently enrolling patients with breast cancer during pregnancy to identify studies open at major cancer centers.
✅ Patient Action: If your oncologist recommends early delivery to accelerate cancer treatment, ask two specific questions before agreeing: (1) What is my baby’s estimated fetal lung maturity at the proposed delivery gestational age? (2) Does this facility have a NICU capable of supporting a delivery at that gestational age — and if not, can I be transferred to one that does?
Survival rates for breast cancer during pregnancy: what the 2026 data shows
Survival rates for PABC are comparable to age-matched non-pregnant patients when treatment begins without significant delay, according to 2026 NCI SEER database analysis. The historical perception that PABC carries inherently worse outcomes reflects delayed diagnosis — not a biological effect of pregnancy on tumor behavior.
Does being pregnant make breast cancer more dangerous?
No. Pregnancy does not accelerate tumor biology in the majority of cases. Historically worse aggregate outcomes in PABC research reflect later stage at diagnosis — because breast changes are frequently attributed to pregnancy rather than evaluated — not any intrinsic growth advantage conferred by the pregnant hormonal environment.
Stage-by-stage survival rates for pregnancy-associated breast cancer
| Stage at PABC Diagnosis | 5-Year Relative Survival Rate | Source |
|---|---|---|
| Stage I | ~99% | NCI SEER 2026 |
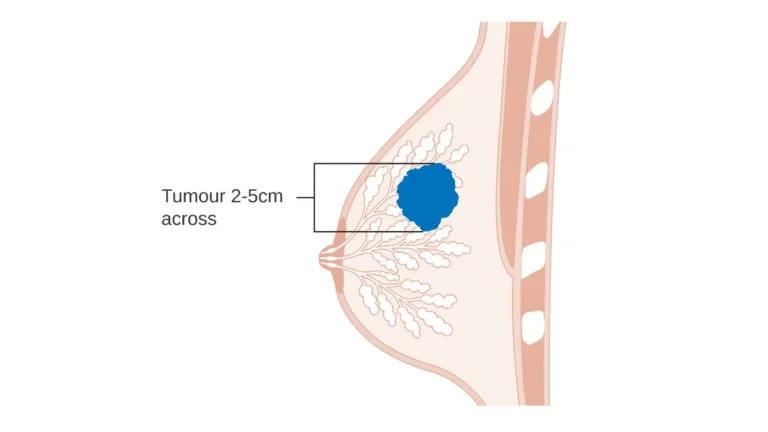
| Stage II | ~86% | NCI SEER 2026 |
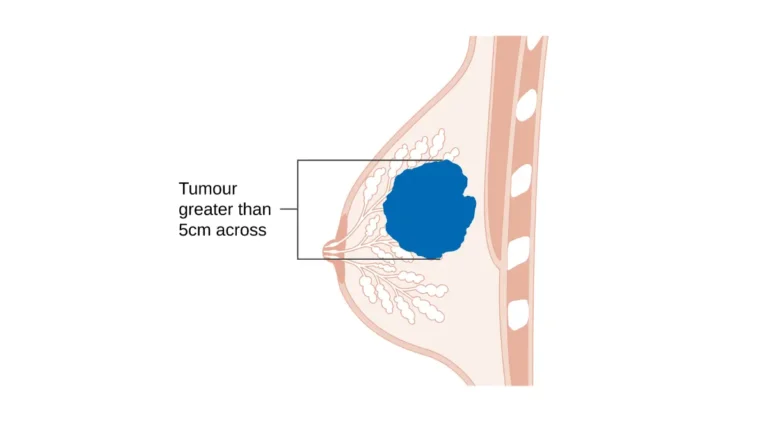
| Stage III | ~57% | NCI SEER 2026 |
| Stage IV | ~28% | NCI SEER 2026 |
For stage-by-stage survival context across all breast cancer subtypes, our guide to breast cancer survival rates by stage — what the numbers mean for your specific diagnosis provides the full breakdown your oncologist will use in your prognosis conversation.
What the research shows about fetal outcomes after maternal cancer treatment
Infants born to mothers who received second- or third-trimester chemotherapy do not show significantly increased rates of major congenital malformation per 2026 follow-up data. They do show higher rates of preterm delivery, low birth weight, and NICU admission — outcomes that require explicit pre-delivery planning with your maternal-fetal medicine team, not assumptions.
For the American Cancer Society’s 2026 stage-by-stage breast cancer survival statistics, see the American Cancer Society’s breast cancer statistics and survival data.
📊 Clinical Data Point: Per 2026 data analysis, PABC survival rates are not statistically worse than age-matched non-pregnant controls when treatment is initiated without significant delay — Source: NCI SEER database, 2026.
✅ Patient Action: For a personalized prognosis based on your tumor biology, stage, receptor status, and gestational age, ask your oncologist: “Where does my specific profile place me within the 2026 PABC survival data — and how does our planned treatment timeline compare to the timeline in the studies that generated these rates?”
A gynecologic oncologist’s perspective on treating breast cancer during pregnancy
In my clinical experience, the single factor that most consistently predicts a good outcome for both mother and baby — beyond tumor biology — is access to a coordinated multidisciplinary PABC team within the first two weeks of diagnosis. A gynecologic oncologist operating independently of a maternal-fetal medicine specialist is a structural risk, regardless of individual expertise.
If you’ve received a BRCA1 or BRCA2 positive result alongside your PABC diagnosis, understanding how that changes your surgical options is essential before any procedure is scheduled. Our guide to BRCA gene test positive results and what every option actually means covers the full decision tree from prophylactic interventions to modified surgical approaches.
Why a multidisciplinary care team is non-negotiable for PABC
A complete PABC team includes, at minimum: a gynecologic oncologist, a medical oncologist, a breast surgical oncologist, a maternal-fetal medicine specialist, and an oncology social worker. Per 2026 NCCN guidelines, if your current treatment center cannot assemble this team, you have the right to request a referral to an NCI-designated cancer center with documented PABC program experience.
Can you breastfeed after breast cancer treatment during pregnancy?
Breastfeeding during active chemotherapy is contraindicated due to documented drug transfer into breast milk. After treatment completion, breastfeeding feasibility depends directly on surgical approach: lumpectomy generally preserves capability on the treated side; mastectomy eliminates it on that side. Discuss your breastfeeding goals explicitly with your gynecologic oncologist before finalizing any surgical plan.
🩺 Physician Note: “The patients I have seen navigate pregnancy-associated breast cancer with the best outcomes — for themselves and their babies — are almost always those who asked, at the very first oncology appointment, whether a maternal-fetal medicine specialist would be co-managing their care from day one. That single question changes how the entire treatment plan is assembled.” — Dr. Carolyn D. Fairweather, MD (Gynecologic Oncology)
✅ Patient Action: Before your first oncology appointment, download our free “11 Questions to Ask Your Oncologist If You’re Pregnant with Breast Cancer” checklist via our newsletter — available on the mymedicineadvisor.com homepage. Bring it printed, write on it, and ask every question on it. A specialist who is uncomfortable with a prepared patient is not the right specialist for a PABC case.
Frequently asked questions about breast cancer and pregnancy
1. What is pregnancy-associated breast cancer (PABC)?
Pregnancy-associated breast cancer is breast cancer diagnosed during pregnancy or within 12 months of delivery, occurring in approximately 1 in 3,000 pregnancies — making it the most common malignancy diagnosed during gestation. Treatment is possible in most cases without ending the pregnancy, provided specialist care begins promptly.
2. Can chemotherapy during pregnancy cause birth defects?
Chemotherapy carries the highest birth defect risk in the first trimester when organogenesis is active. After week 14, the AC regimen (doxorubicin + cyclophosphamide) carries an estimated major malformation rate below 4% per 2026 clinical data — a risk that must be weighed against the risk of untreated breast cancer during pregnancy. Consult a board-certified gynecologic oncologist and maternal-fetal medicine specialist before beginning any chemotherapy regimen.
3. What trimester is safest for breast cancer surgery?
The second trimester (weeks 14–28) is the safest window for breast cancer surgery during pregnancy. Organogenesis is complete, fetal anesthetic risk is at its lowest, and the uterus has not yet significantly obstructed the surgical field. First-trimester surgery should be deferred to week 14 when tumor biology permits. Consult a board-certified breast surgical oncologist with documented PABC experience before scheduling any surgical procedure.
4. Is it safe to delay breast cancer treatment while pregnant?
It depends entirely on tumor biology and gestational age. Triple-negative breast cancer and high-grade disease generally cannot be safely delayed beyond four weeks from confirmed diagnosis per 2026 NCCN guidance. Low-grade, hormone receptor-positive disease approaching 35 weeks gestation may allow a brief deferral. Consult a board-certified gynecologic oncologist and maternal-fetal medicine specialist before any delay decision is made.
5. Does pregnancy cause breast cancer to spread faster?
No direct evidence supports the claim that pregnancy accelerates breast cancer biology. Larger tumors at PABC diagnosis reflect delayed clinical detection — breast changes attributed to pregnancy rather than evaluated — not faster tumor growth caused by pregnancy hormones. When treatment begins without significant delay, survival rates are comparable to age-matched non-pregnant patients per 2026 data.
6. What happens when breast cancer is diagnosed in the third trimester?
At 34–36 weeks, early delivery may be considered after assessing fetal lung maturity to allow full systemic breast cancer treatment post-delivery. Earlier in the third trimester, chemotherapy can often be continued through pregnancy with fetal monitoring. Treatment options depend on gestational age, tumor grade, nodal status, and HER2 and receptor profile. Consult a board-certified gynecologic oncologist and maternal-fetal medicine specialist for a delivery timing assessment.
7. Can you get a mammogram when you’re pregnant?
Yes — mammography during pregnancy is considered safe with abdominal lead shielding. Breast ultrasound is typically the first imaging step because it avoids radiation entirely. When ultrasound is inconclusive, MRI without gadolinium contrast is the next recommended modality per 2026 ACOG guidance. Consult a board-certified breast surgical oncologist if any imaging finding requires further evaluation or biopsy planning.
8. What type of breast cancer is most common during pregnancy?
Invasive ductal carcinoma is the most frequently diagnosed histologic subtype in PABC. Hormone receptor-positive, triple-negative, and HER2-positive disease all occur during pregnancy. A full receptor panel — estrogen receptor, progesterone receptor, and HER2 — must be performed on every PABC biopsy specimen, as receptor status determines the entire treatment sequence. Consult a board-certified gynecologic oncologist for a complete tumor profile interpretation.
9. Can you breastfeed after breast cancer treatment during pregnancy?
Breastfeeding during active chemotherapy is contraindicated due to drug transfer into breast milk at concentrations that reach the nursing infant. After treatment completion, breastfeeding feasibility depends on surgical approach: lumpectomy generally preserves capability on the treated side, while mastectomy eliminates it on that side. Discuss your breastfeeding goals explicitly with your gynecologic oncologist and a board-certified lactation consultant before finalizing your surgical decision.
10. Is breast cancer during pregnancy always terminal?
No — breast cancer and pregnancy do not equal a terminal prognosis. Survival rates for PABC are comparable to age-matched non-pregnant patients when treatment begins without significant delay. Stage at diagnosis is the strongest prognostic factor — not pregnancy itself. Stage I PABC carries an approximately 99% five-year survival rate per 2026 NCI SEER data.
11. How is breast cancer treated after giving birth?
After delivery, the complete treatment range becomes available. Radiation therapy, deferred during pregnancy, can begin within weeks of delivery. Trastuzumab (Herceptin) for HER2-positive disease is resumed immediately post-delivery. Endocrine therapy — tamoxifen or aromatase inhibitors — for hormone receptor-positive disease begins after delivery and completion of chemotherapy. Consult your gynecologic oncologist and medical oncologist together at your first post-delivery appointment to finalize the post-pregnancy treatment plan.
What to do next if you’ve been diagnosed with breast cancer during pregnancy
Healthy babies are born to mothers with breast cancer and pregnancy diagnoses every year at major cancer centers. Stage at diagnosis — not pregnancy itself — determines your prognosis. Treatment does not have to wait until after delivery in most cases.
Your three immediate steps:
- Contact a board-certified gynecologic oncologist with documented PABC experience within 48 hours of receiving your biopsy result. Do not wait for your next scheduled prenatal appointment — these are two separate care tracks that must begin running simultaneously, not sequentially.
- Request a maternal-fetal medicine co-consult at the same time. This is not a secondary referral — it is a simultaneous consultation that begins the multidisciplinary team process from day one.
- Bring your complete pathology report to both appointments. This means your biopsy result, hormone receptor status (ER and PR), and HER2 result. If any of these are not yet available, ask your referring physician to expedite them before your oncology appointment.
To monitor your health throughout treatment, our Pregnancy Weight Gain Calculator tracks gestational weight within healthy ranges by trimester — a tool useful for patients managing nutrition during active treatment.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.