On This Page – Quick Medical Summary
What does obesity have to do with breast cancer risk?
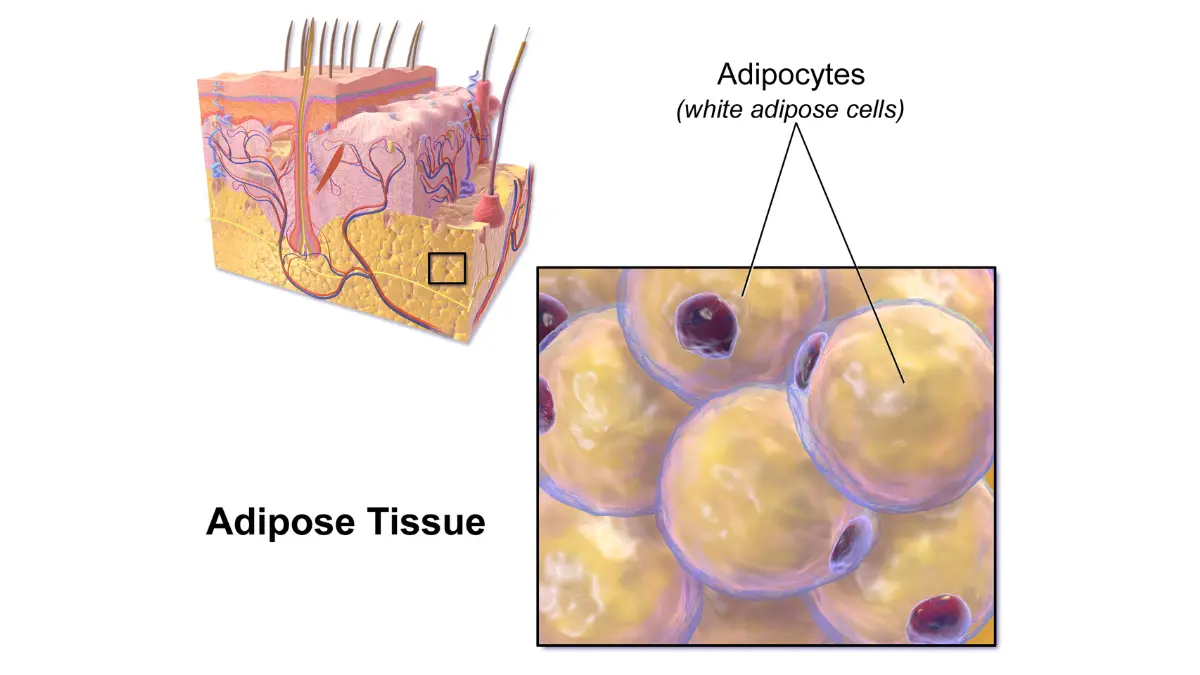
Obesity and breast cancer are not loosely correlated. They are connected through a precise hormonal pathway. Adipose tissue — the clinical term for body fat — actively produces estrogen through an enzyme called aromatase. After menopause, when the ovaries stop functioning, adipose tissue becomes the body’s primary estrogen source. The more adipose tissue a woman carries, the higher her circulating estrogen — and elevated estrogen is a direct driver of hormone receptor-positive (HR+) breast cancer, the most common breast cancer type in the US.
This is not a distant theoretical risk. It is a mechanism that shapes how I counsel patients in my clinic every week, and it is one of the few breast cancer risk factors you can actually change.
This article is part of a broader clinical series — for context on staging, prognosis, and what to expect at each disease phase, see our complete breast cancer stages and survival guide.
ℹ️ Medical Disclaimer: The hormonal mechanisms, BMI thresholds, treatment options, medication information — including aromatase inhibitors and GLP-1 receptor agonists — and risk reduction strategies discussed in this article reflect 2026 clinical guidelines and are provided for educational purposes only. Individual cancer risk assessments, diagnostic conclusions, weight management plans, and medication choices depend on your personal health history, comorbidities, tumor subtype, test results, and specialist assessment. Consult a board-certified gynecologic oncologist or primary care physician before acting on any clinical information in this article.
How fat tissue raises estrogen — and why that matters for breast cancer
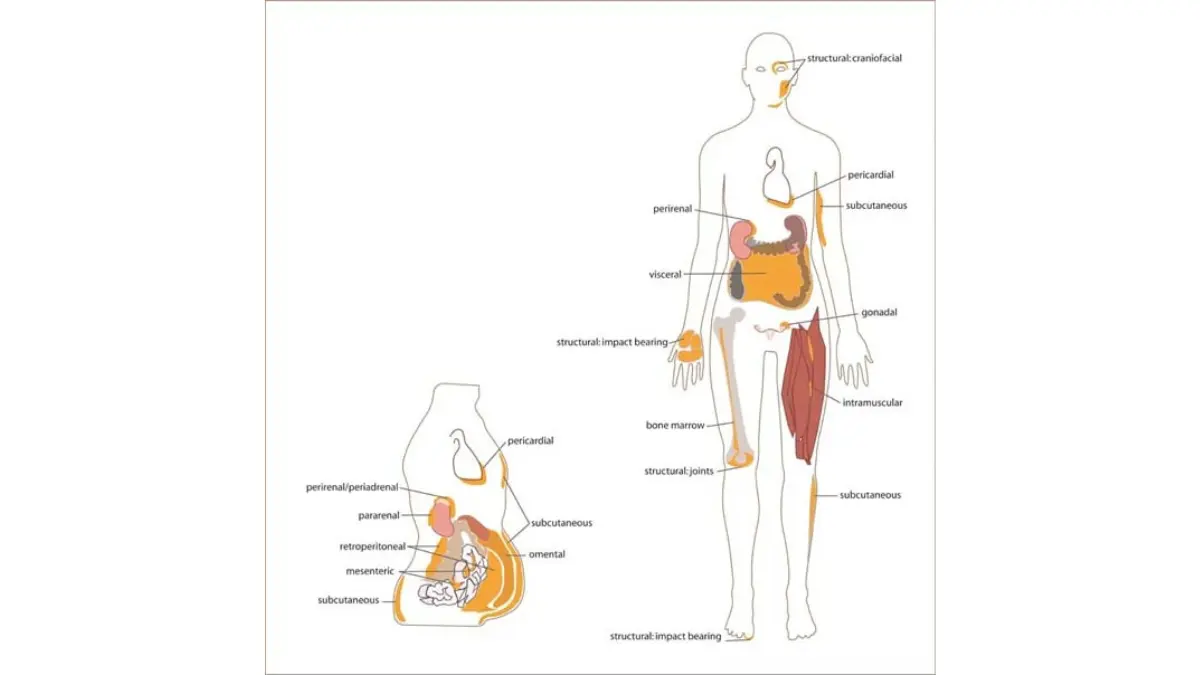
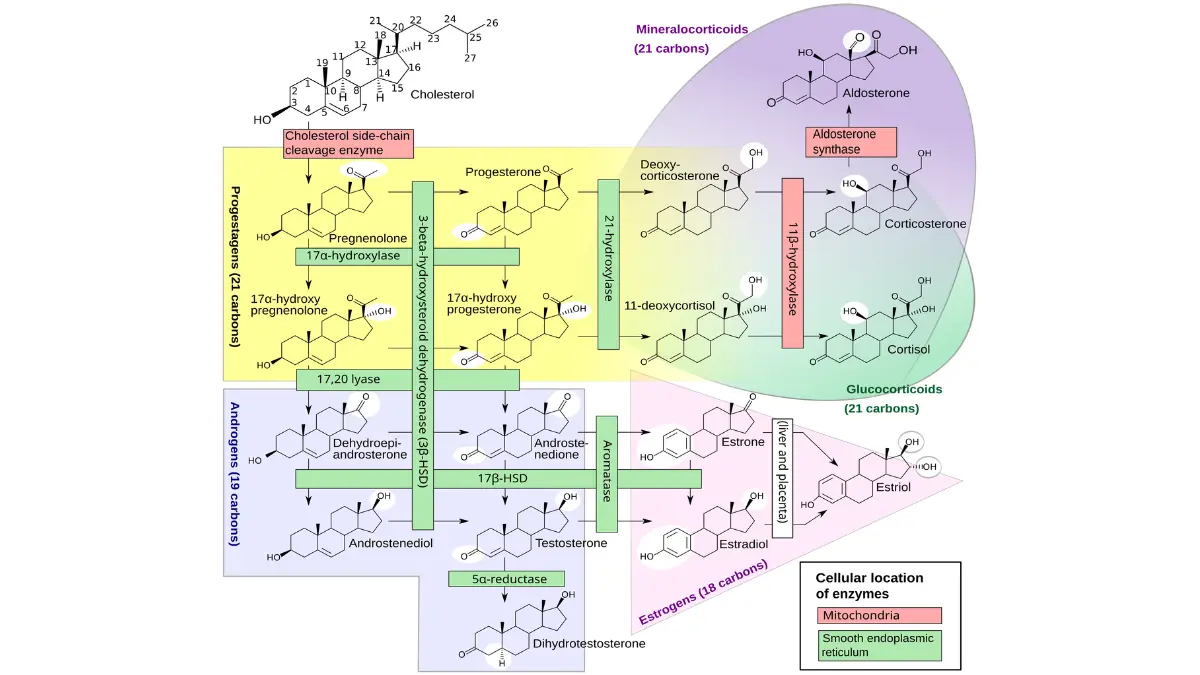
Obesity raises breast cancer risk primarily by activating the aromatase enzyme inside fat cells, which converts androgens — male sex hormones present in all women — into estradiol, the most biologically active form of estrogen. This process does not require the ovaries. It happens directly inside adipose tissue throughout the body, continuously, at a rate that scales with how much adipose tissue a woman carries.
🔬 How It Works: Aromatase is an enzyme found in adipose tissue, muscle, and liver cells. Before menopause, the ovaries produce the majority of circulating estrogen, and adipose aromatase activity plays a secondary role. After menopause, the ovaries cease functioning — and adipose tissue becomes the dominant estrogen source for the entire body. A woman with significantly elevated BMI can have circulating estradiol levels two to three times higher than a normal-weight postmenopausal woman, driven entirely by adipose aromatase activity. That estrogen circulates to breast tissue and activates hormone receptor-positive tumor growth at a sustained, daily rate.
The aromatase pathway: why fat cells produce estrogen
A second mechanism compounds the aromatase effect. Obesity reduces sex hormone-binding globulin (SHBG) — a protein that normally binds estrogen in the bloodstream and keeps it in an inactive form. Lower SHBG means more estrogen circulates freely, reaching breast tissue in its biologically active state.
The result is a double burden: higher total estrogen production from adipose aromatase activity, plus higher free estrogen availability because SHBG is reduced. Both pathways push in the same direction, simultaneously.
📊 Clinical Data Point: According to the American Cancer Society’s 2026 data on body weight and breast cancer risk, postmenopausal women with obesity face a meaningfully elevated risk of hormone receptor-positive breast cancer compared to normal-weight women — a relationship directly mediated by adipose-derived estrogen production through aromatase activity.
Postmenopausal vs. premenopausal: why the risk profile is different
Before menopause, the ovaries dominate estrogen production — so adipose tissue is a secondary contributor, and the obesity-estrogen link, while present, is partially dampened. After menopause, the ovaries shut down entirely, and adipose tissue assumes full responsibility as the body’s estrogen source.
This is why postmenopausal breast cancer risk shows the strongest, most direct response to BMI elevation. Premenopausal women with obesity carry elevated risk through insulin resistance and chronic systemic inflammation — but the hormone-driven mechanism is exponentially more pronounced after menopause.
Why obesity is specifically linked to hormone receptor-positive tumors
The estrogen excess produced by adipose tissue preferentially fuels hormone receptor-positive (HR+) breast cancer — specifically ER+ and PR+ subtypes, which carry estrogen or progesterone receptors on their surface and grow in direct response to circulating hormones.
Triple-negative breast cancer (TNBC) lacks these receptors and does not respond to estrogen signaling directly. However, obesity contributes to TNBC risk through insulin resistance, hyperinsulinemia, and elevated adipokines including leptin. Women living with triple-negative breast cancer should discuss how their individual metabolic profile affects their risk with their oncologist.
📊 Clinical Data Point: A 2026 peer-reviewed analysis of aromatase activity and adipose tissue confirmed the mechanistic relationship between elevated BMI, adipose-derived estradiol, and HR+ breast cancer incidence — with the effect size strongest in postmenopausal women carrying adipose tissue predominantly in abdominal visceral depots.
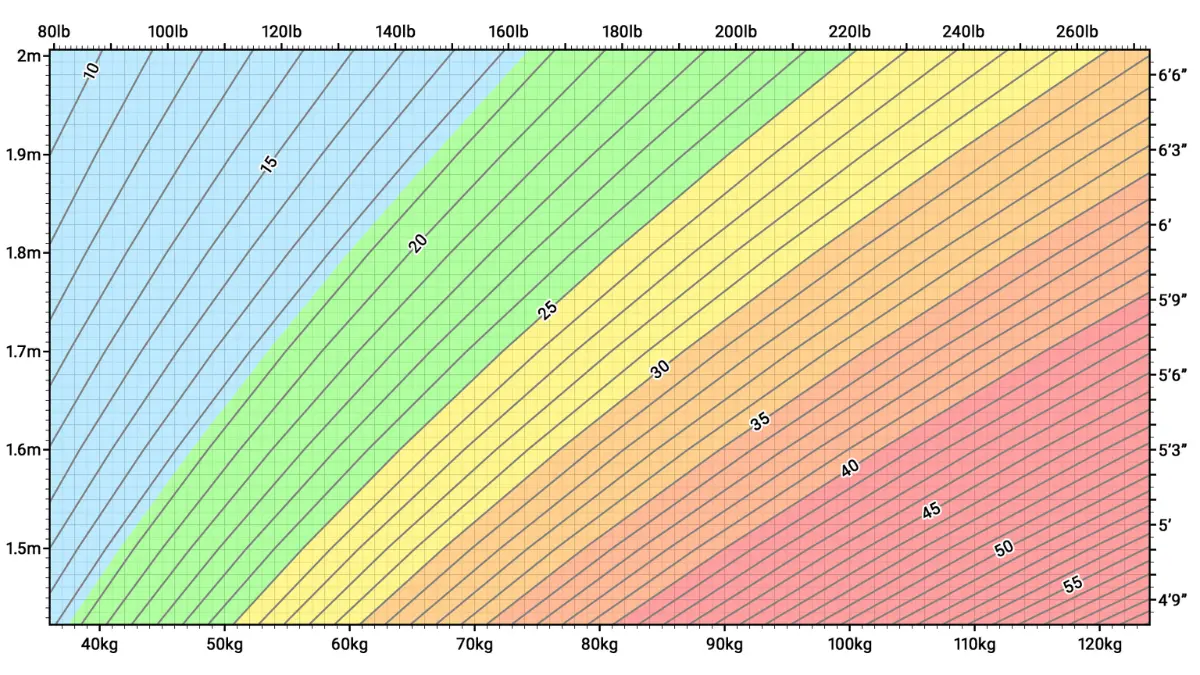
Which BMI numbers actually raise your breast cancer risk?
A BMI of 30 or higher is associated with a clinically significant increase in postmenopausal breast cancer risk, with risk rising progressively through Class II obesity (BMI 35.0–39.9) and Class III obesity (BMI ≥40). The relationship is not a cliff — it is a dose-response slope. Every unit of BMI above 25 carries a measurable increase in adipose-driven estrogen production and inflammatory marker elevation.
The table below summarizes how breast cancer risk scales with BMI category based on 2026 NCI and ACS surveillance data:
| BMI Category | BMI Range | Postmenopausal HR+ BC Risk | Key Clinical Detail |
|---|---|---|---|
| Normal weight | 18.5–24.9 | Reference | Lowest aromatase activity; SHBG at optimal level |
| Overweight | 25.0–29.9 | Modestly elevated | SHBG begins to decline; free estrogen rises |
| Obese — Class I | 30.0–34.9 | Meaningfully elevated | Aromatase activity substantially increased |
| Obese — Class II | 35.0–39.9 | Substantially elevated | Free estradiol highest; leptin signaling elevated |
| Obese — Class III | ≥40.0 | Highest risk tier | Maximum adipose estrogen burden; highest surgical risk |
Source: NCI/ACS 2026
📊 Clinical Data Point: The NCI’s 2026 breast cancer risk and prevention fact sheet identifies body weight as a modifiable breast cancer risk factor with a documented dose-response relationship — the greater the BMI above the normal range, the greater the measured postmenopausal HR+ breast cancer risk increase.
BMI categories and breast cancer risk: what the 2026 data shows
The obesity and breast cancer risk gradient is not uniform across subtypes. Postmenopausal HR+ breast cancer shows the steepest BMI-linked risk slope. NCCN 2026 clinical practice guidelines specifically name weight management as a cancer prevention recommendation for women in the overweight and obese BMI categories — placing it alongside screening frequency and chemoprevention discussions.
✅ Patient Action: If your BMI falls in the Class II or Class III range, ask your board-certified oncologist or primary care physician: “Given my BMI, should my mammography schedule include supplemental imaging — such as ultrasound or MRI — beyond the standard annual mammogram?” This question directly affects your screening plan and is one most clinicians will not raise unprompted.
Use our BMI Calculator to confirm your current number before your next appointment — it takes under 60 seconds and gives you a documented starting point for this conversation.
Postmenopausal women: why the threshold effect is strongest after 50
For women who have passed menopause — whether naturally or due to cancer treatment — the BMI risk gradient is steepest. Adipose-driven aromatase activity is unrestricted by ovarian competition, and the free estrogen elevation from reduced SHBG operates without interruption, continuously, year over year.
Women in this population who are in the overweight or obese range have the most to gain, clinically, from intentional weight reduction as a prevention strategy.
Why waist circumference matters as much as BMI
Visceral adiposity — fat stored around internal organs in the abdominal cavity — carries substantially higher aromatase activity than subcutaneous fat. A waist circumference of 35 inches or more in women is an independent breast cancer risk marker, separate from total BMI.
Some women with a normal overall BMI but a waist measurement above this threshold carry a meaningfully higher breast cancer risk than their BMI alone suggests. This “metabolically obese, normal weight” phenotype is a clinical pattern I see frequently, and it is systematically missed when risk assessment stops at BMI.
📊 Clinical Data Point: The CDC’s 2026 adult obesity prevalence data confirms that a substantial proportion of US women across all age groups meet criteria for overweight or obesity — making weight-related breast cancer risk a population-level concern, not a rare individual circumstance.
Black women face a disproportionately higher incidence of triple-negative breast cancer regardless of BMI — a risk disparity that requires a specific oncology discussion beyond standard BMI-based frameworks. Our dedicated clinical guide on breast cancer risk in Black women provides a detailed breakdown of this risk profile.
For a broader overview of all modifiable and non-modifiable breast cancer risk factors, see our full guide on breast cancer risk factors.
Diet and exercise changes with real evidence behind them
The Mediterranean diet and the DASH dietary pattern carry the strongest 2026 clinical evidence for reducing the hormonal and inflammatory drivers of breast cancer risk. Both prioritize vegetables, legumes, whole grains, and healthy fats — while limiting refined sugars, processed foods, and alcohol.
The mechanism goes deeper than weight loss. High-glycemic foods elevate insulin resistance and drive hyperinsulinemia, which independently raises IGF-1 (insulin-like growth factor 1) signaling in breast tissue. Elevated IGF-1 promotes cellular proliferation — the same biological process that sustains tumor growth. Reducing glycemic load is not simply about calories. It is about reducing a specific breast cancer signaling pathway.
What to eat: anti-inflammatory dietary patterns and breast cancer risk
The dietary targets with the strongest evidence for reducing obesity-related breast cancer risk address both circulating estrogen and chronic inflammation simultaneously:
- Cruciferous vegetables (broccoli, cauliflower, Brussels sprouts, kale) — contain indole-3-carbinol, which supports estrogen metabolism and clearance pathways
- Fatty fish and omega-3 fatty acids (salmon, sardines, mackerel) — reduce pro-inflammatory adipokines including leptin; 2026 clinical data supports measurable inflammatory marker reduction
- Whole grains and legumes — lower glycemic impact, reduce IGF-1 signaling, and support gut microbiome processing of estrogen metabolites
- Limiting alcohol — alcohol independently elevates circulating estrogen at any BMI level and is a standalone breast cancer risk factor with no safe lower threshold per 2026 ACS guidance
🔬 How It Works: Adipose tissue is not passive storage. It secretes a class of signaling molecules called adipokines — including leptin, which promotes tumor cell proliferation, and adiponectin, which has documented anti-tumor properties. Obesity shifts this balance toward leptin excess and adiponectin deficiency, creating a pro-inflammatory tumor microenvironment that sustains cancer cell survival. Anti-inflammatory dietary patterns directly suppress leptin elevation and support adiponectin production — a targeted nutritional intervention with a mechanistic basis, not a generic wellness recommendation.
How much exercise matters — and what type the evidence supports
NCCN 2026 clinical practice guidance recommends 150 minutes of moderate-intensity aerobic activity per week — or 75 minutes of vigorous-intensity aerobic activity — plus at least two sessions of resistance training per week. This is not a general wellness target. It is a cancer prevention recommendation with a specific biological rationale.
Aerobic exercise reduces circulating estrogen by decreasing adipose tissue mass and lowering peripheral aromatase activity. Resistance training preserves lean muscle mass — critical for avoiding sarcopenic obesity (fat gain alongside muscle loss), which worsens treatment tolerance and surgical risk if cancer develops.
Use our Heart Rate Zone Calculator to identify the specific heart rate ranges corresponding to moderate and vigorous intensity for your individual physiology — the precision that turns a general guideline into an actionable workout target.
To build a calorie plan that supports your exercise goals without triggering muscle loss, our Calorie Deficit Calculator can generate a clinician-shareable daily target before your next appointment.
Weight management tools your care team can offer
For women with Class II or Class III obesity, lifestyle modification alone may not produce the degree of weight reduction needed to meaningfully reduce hormonal burden. GLP-1 receptor agonist pharmacotherapy — an FDA-approved class of weight management medications — has emerging 2026 clinical data on its effects on cancer-associated inflammatory and hormonal markers.
✅ Patient Action: Before starting any supervised weight management program — including GLP-1 receptor agonist pharmacotherapy — ask your board-certified oncologist or primary care physician: “Is pharmacological weight management appropriate for my specific situation, and does it interact with any medications I am taking for cancer prevention or treatment?” This question determines whether the intervention fits safely within your current medical plan.
⚠️ Clinical Warning: Aggressive caloric restriction without specialist guidance can cause rapid muscle mass loss alongside fat — a pattern called sarcopenic obesity. This condition increases surgical complication risk and reduces chemotherapy tolerance. All cancer-related weight management should proceed under specialist oversight, with protein intake actively monitored.
If you’ve already been diagnosed: can weight loss change your outcome?
Intentional weight loss of 5–10% of body weight has been associated in 2026 clinical evidence with measurable reductions in circulating estrogen, inflammatory adipokines, and insulin levels — all three of which are mechanistically linked to breast cancer development and HR+ recurrence risk. This is not an optimistic estimate. It is a documented hormonal effect with direct clinical relevance to survivorship outcomes.
The question patients ask most frequently in my clinic is not whether weight loss helps — they sense that it does. The question that actually needs a clinical answer is when to pursue it, how much is needed, and whether method affects the result.
What 2026 research says about weight loss and breast cancer recurrence
The most clinically significant intervention window is the survivorship period — after active treatment ends, when the body has recovered sufficient metabolic tolerance for caloric adjustment and exercise. Women who achieve intentional weight loss during survivorship reduce adipose-driven aromatase activity, lower circulating estradiol, and improve the adiponectin-to-leptin ratio — all of which are linked to HR+ breast cancer recurrence risk reduction.
For a comprehensive clinical overview of recurrence risk, triggers, and what to monitor during survivorship, see our guide on breast cancer recurrence.
📊 Clinical Data Point: Active 2026 clinical trials on weight management and breast cancer outcomes registered through ClinicalTrials.gov are specifically investigating structured weight loss interventions in HR+ breast cancer survivorship — confirming that this is now a formal oncology research priority with multiple active enrollment protocols.
How much weight loss matters — and does the method affect outcomes?
A clinically meaningful reduction in circulating estrogen and inflammatory markers begins at approximately 5% of body weight. For a woman weighing 200 pounds, that is 10 pounds — achievable through structured dietary change alone for many patients, and with GLP-1-based pharmacotherapy for those whose metabolic profile requires a more intensive intervention.
Use our Weight Loss Calculator to set your personal 5% milestone and generate a realistic timeline — a concrete number to bring to your next oncology appointment, rather than a vague intention.
✅ Patient Action: Before initiating any structured weight loss program during or after breast cancer treatment, ask your board-certified oncologist: “Given my tumor subtype, my current treatment phase, and my BMI, what weight loss method is safest for me right now — and what timeline is appropriate?” The clinical answer differs completely between someone in active chemotherapy and someone twelve months post-treatment.
Should you lose weight while in active treatment?
This requires a direct answer. Do not pursue aggressive caloric restriction during active chemotherapy. The reason is specific: chemotherapy significantly increases the risk of sarcopenic obesity — a condition in which the body preferentially loses lean muscle mass alongside fat during periods of caloric deficit or metabolic stress.
Sarcopenic obesity impairs treatment tolerance, increases surgical complication risk, and prolongs recovery. During active treatment, the clinical priority is maintaining weight and actively preserving lean mass through adequate protein intake — not achieving caloric deficit.
🩺 Physician Note: The most common error I see postmenopausal HR+ patients make during chemotherapy is self-directed aggressive dieting — driven by the correct instinct that weight matters, but applied at the wrong time. During treatment, muscle preservation and adequate protein intake are the clinical priorities. Weight reduction as a cancer recurrence prevention strategy belongs in the post-treatment survivorship window, where it is both safe and mechanistically meaningful.
How obesity affects breast cancer survival and recurrence rates
2026 SEER database analysis shows that women with Class II or Class III obesity at breast cancer diagnosis have lower five-year overall survival rates compared to normal-weight women — with the gap widening specifically in HR+ disease, where adipose-derived estrogen actively competes with aromatase inhibitor therapy, the standard of care for postmenopausal HR+ breast cancer.
The survival impact of obesity and breast cancer extends beyond treatment response. It includes lymphedema incidence, surgical complication rates, and long-term recurrence probability — each of which worsens incrementally as BMI rises.
Survival outcomes by BMI: what the 2026 data shows
The table below summarizes 2026 surveillance data on how BMI category affects breast cancer outcomes in the HR+ postmenopausal population:
| BMI Category | 5-Year Survival Impact (HR+ BC) | Recurrence Risk Change | Primary Clinical Mechanism |
|---|---|---|---|
| Normal weight (<25) | Reference | Reference | Lowest adipose estrogen burden |
| Overweight (25–29.9) | Modestly reduced | Slightly elevated | Early SHBG decline; free estrogen rises |
| Obese Class I (30–34.9) | Meaningfully reduced | Elevated | Aromatase competes with AI therapy |
| Obese Class II+ (≥35) | Most significantly reduced | Substantially elevated | Maximum aromatase competition; highest lymphedema risk |
Source: NCI/SEER 2026, ACS 2026
📊 Clinical Data Point: Per the American Cancer Society’s 2026 cancer statistics, obesity at the time of breast cancer diagnosis is associated with reduced aromatase inhibitor efficacy in HR+ disease — because peripheral adipose-derived estrogen production continues even while aromatase inhibitor therapy is active, partially offsetting the medication’s intended mechanism.
Obesity and breast cancer recurrence: what raises the risk
For women in survivorship following HR+ breast cancer treatment, elevated BMI sustains the same aromatase-driven estrogen production that initially fueled tumor development. Aromatase inhibitors suppress ovarian and peripheral estrogen conversion — but they cannot fully overcome the continuous estrogen output of significant adipose tissue.
For a clinical comparison of how tamoxifen and aromatase inhibitors interact differently with this biological mechanism, see our guide on tamoxifen vs. aromatase inhibitors — a distinction that matters specifically for postmenopausal patients with elevated BMI.
Surgical and treatment complications linked to high BMI
Elevated BMI creates a specific set of operative risks for breast cancer patients that are independent of tumor biology:
- Lymphedema — women with higher BMI and axillary node dissection face meaningfully higher rates of chronic arm lymphedema, because adipose tissue compresses lymphatic drainage vessels and restricts fluid clearance after surgery
- Wound healing complications — adipose tissue has lower vascular density than lean tissue, slowing repair after mastectomy or lumpectomy incisions
- Anesthesia exposure duration — high-BMI surgical procedures typically require extended anesthesia time, increasing cardiovascular and pulmonary complication risk
✅ Patient Action: If your BMI is in the obese range and you are planning breast cancer surgery, ask your board-certified surgical oncologist: “What is my specific lymphedema risk given my BMI and planned lymph node involvement — and what pre-operative steps can I take now to reduce it?” Our dedicated guide on lymphedema after breast cancer surgery covers prevention strategies, early symptoms, and management protocols in detail.
Black women with high BMI and triple-negative breast cancer face a compounded risk profile — one where race-specific TNBC incidence intersects with obesity-driven metabolic risk — that warrants individualized assessment from a board-certified oncologist experienced with this specific population.
Dr. Fairweather’s clinical perspective on weight and breast cancer
There is a conversation that belongs in every oncology appointment for postmenopausal HR+ breast cancer patients with a BMI above 30 — and in my experience, it rarely happens within the standard visit structure. I want to put it on record here.
What I tell patients when BMI comes up in the treatment conversation
When a postmenopausal patient with HR+ breast cancer starts an aromatase inhibitor, I discuss weight management as a treatment priority — not a lifestyle suggestion. The clinical reason is mechanistically direct.
Aromatase inhibitors work by blocking the aromatase enzyme, reducing the conversion of androgens to estradiol in peripheral tissue. If a patient carries significant adipose tissue, that tissue is generating estrogen continuously, through aromatase activity the medication is working to suppress. Every pound of adipose tissue maintained is an active estrogen production site. Reducing that adipose mass is not supplementary to her aromatase inhibitor therapy. It is reinforcing it at the biological level.
🩺 Physician Note: The question patients on aromatase inhibitor therapy almost never ask — but almost always should — is this: “Is my current BMI reducing how well my medication is working?” In my clinical practice, this question shapes whether weight management becomes a formal, documented part of the oncology plan rather than an afterthought at the end of a follow-up visit. If you are on an aromatase inhibitor and your BMI is above 30, that question belongs at your next appointment.
The question I wish more patients asked before starting aromatase inhibitors
Gynecologic oncology survivorship care in 2026 is increasingly precise. NCCN 2026 clinical practice guidelines specifically include weight management as a component of survivorship care planning for HR+ breast cancer patients — not as optional lifestyle guidance, but as a documented clinical recommendation at the guideline level.
Use our Genetic Risk Assessment Tool to review how your BMI interacts with your other known breast cancer risk factors. The tool generates a structured risk summary you can print and bring to your oncologist — a clinical conversation starter that makes weight management impossible to skip past in an appointment.
Frequently asked questions about obesity and breast cancer risk
Q1: Does being overweight increase breast cancer risk?
Yes — obesity and breast cancer risk are directly linked, particularly after menopause. Overweight (BMI 25–29.9) modestly elevates risk; obesity (BMI ≥30) elevates it meaningfully. The mechanism is adipose tissue producing estrogen through aromatase enzyme activity, which drives hormone receptor-positive breast tumor growth. Risk increases on a dose-response slope — the higher the BMI above normal, the greater the measured risk elevation.
Q2: What BMI is considered high risk for breast cancer?
A BMI of 30 or higher enters the clinically elevated tier for postmenopausal breast cancer risk, with risk rising progressively through Class II (BMI 35–39.9) and Class III obesity (BMI ≥40). Even overweight BMI (25–29.9) is associated with modestly elevated risk due to early SHBG reduction and increased free circulating estrogen. Consult a board-certified gynecologic oncologist to discuss your individualized risk profile and screening schedule.
Q3: Is obesity linked to triple-negative breast cancer?
The obesity and triple-negative breast cancer (TNBC) relationship is real but operates through different pathways than HR+ disease. TNBC lacks hormone receptors, so adipose-derived estrogen is not the direct driver. Instead, insulin resistance, elevated leptin signaling, and chronic systemic inflammation create independent TNBC risk pathways. Black women face disproportionately higher TNBC incidence regardless of BMI — a disparity requiring specialist evaluation beyond standard risk frameworks.
Q4: Can losing weight after a breast cancer diagnosis help?
Yes — intentional weight loss of 5–10% of body weight during survivorship is associated with measurable reductions in circulating estrogen, inflammatory markers, and insulin levels linked to HR+ breast cancer recurrence risk. Weight loss during active chemotherapy, however, carries sarcopenic obesity risk and requires oncologist oversight to avoid muscle mass loss. Consult your board-certified oncologist about the safest timing and method for your specific treatment phase.
Q5: How does fat tissue produce estrogen?
Adipose tissue contains the aromatase enzyme, which converts androgens — male sex hormones present in all women — into estradiol, the most biologically active estrogen form. After menopause, when ovarian estrogen production ceases, adipose-based aromatase conversion becomes the body’s primary estrogen source. Obesity also reduces SHBG, a protein that normally binds and inactivates estrogen in the bloodstream — so more free estradiol reaches breast tissue in a biologically active state.
Q6: Does obesity affect breast cancer survival rates?
Yes — women with Class II or Class III obesity at breast cancer diagnosis have lower five-year overall survival rates compared to normal-weight women, particularly in HR+ disease. Adipose-driven estrogen production directly competes with aromatase inhibitor therapy, potentially reducing its effectiveness over time. Lymphedema rates and surgical complication rates are also meaningfully higher in this BMI tier. Consult a board-certified oncologist to assess your individual outcome profile.
Q7: What diet changes help reduce obesity-related breast cancer risk?
The dietary patterns with the strongest evidence for reducing obesity-related breast cancer risk are the Mediterranean and DASH diets — high in cruciferous vegetables, legumes, whole grains, and omega-3 fatty acids, and low in refined sugars, processed foods, and alcohol. Reducing glycemic load lowers IGF-1 signaling in breast tissue. Limiting alcohol is clinically important at any BMI, as alcohol independently elevates circulating estrogen at all consumption levels.
Q8: How much weight loss reduces breast cancer risk?
A 5–10% reduction in body weight produces measurable decreases in circulating estrogen, inflammatory adipokines, and insulin levels — all mechanistically linked to breast cancer development and HR+ recurrence risk. Greater weight loss amplifies these hormonal effects. The post-treatment survivorship window is the optimal intervention period. Consult your board-certified oncologist about the safest method and realistic timeline for your specific treatment history and BMI.
Q9: Does obesity increase the risk of breast cancer coming back?
Yes — elevated BMI during survivorship sustains adipose-driven aromatase activity that competes with aromatase inhibitor therapy, the standard of care for preventing breast cancer recurrence in postmenopausal HR+ disease. Residual adipose estrogen production is one of the primary mechanisms through which obesity elevates recurrence risk after treatment. Consult your board-certified gynecologic oncologist about whether weight management should be a formal component of your survivorship care plan.
Q10: Are women with obesity more likely to get aggressive breast cancer?
Obesity is most strongly associated with hormone receptor-positive breast cancer through the estrogen-aromatase pathway. HER2-positive and triple-negative subtypes — both more aggressive — are linked to obesity through insulin resistance, IGF-1 signaling elevation, and chronic inflammation rather than estrogen excess directly. Women with obesity and a personal or family history of aggressive breast cancer subtypes should discuss their full subtype-specific risk with a board-certified oncologist.
Q11: Should I lose weight while going through chemotherapy?
No — aggressive caloric restriction during active chemotherapy is not recommended without direct oncologist guidance. Chemotherapy increases the risk of sarcopenic obesity — disproportionate muscle mass loss alongside fat — which reduces treatment tolerance and surgical recovery capacity. The clinical priority during active breast cancer treatment is maintaining weight and preserving lean muscle through adequate protein intake. Weight management as a prevention or recurrence reduction strategy is appropriate in the pre-diagnosis and post-treatment survivorship periods.
Your next steps for managing obesity-related breast cancer risk
Three concrete actions before you close this article:
One: Calculate your BMI and measure your waist circumference. Write both numbers down before your next physician visit. A BMI above 30, or a waist measurement above 35 inches, is information your care team needs to give you individualized risk guidance — and a specific number changes a general health conversation into a clinical one.
Two: Bring the clinical framework in this article directly to your oncologist or primary care physician. Ask this specific question: “What does my current BMI mean for my breast cancer risk or recurrence risk — and should weight management be a formal, documented part of my care plan?” That question, asked by name, changes the appointment.
Three: Use our Genetic Risk Assessment Tool to document how your weight interacts with your other known breast cancer risk factors. The output gives you a structured, printable risk summary to share with your physician.
As I tell every patient I see: obesity is a modifiable risk factor. Modifiable means there is always a clinical path forward — and you and your care team can build it together, starting with the numbers you now have.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.