On This Page – Quick Medical Summary
Why Black Women Face a 40% Higher Breast Cancer Death Rate
If you are currently experiencing new breast symptoms, check your symptoms using our clinical symptom tool before your next appointment.
As a gynecologic oncologist, I have watched this pattern repeat across my clinical career. Black women in the United States are approximately 40% more likely to die from breast cancer than white women — despite having comparable or lower diagnosis rates in some age groups. That gap is not coincidence. It is not inevitable.
Two causes drive it: a tumor subtype that behaves differently at the molecular level, and a healthcare system that fails Black patients at predictable, documented points. A complete explanation of breast cancer staging and what survival rates actually mean is essential context for everything in this article. Understanding both causes is the first step toward changing your outcome.
ℹ️ Medical Disclaimer: The diagnostic criteria, genetic testing guidance, screening recommendations, treatment options, and medication information in this article reflect current clinical guidelines and are provided for educational purposes only. Individual diagnostic conclusions — including breast cancer subtype classification, BRCA1/2 mutation status, staging, and treatment eligibility — depend on personal medical history, comorbidities, imaging results, biopsy pathology, and specialist assessment. Insurance coverage and clinical trial eligibility are governed by plan-specific and protocol-specific criteria that vary by individual.
Consult a board-certified gynecologic oncologist or breast oncologist before acting on any clinical information in this article, particularly regarding genetic testing, screening schedule adjustments, treatment selection, or clinical trial enrollment.
The Mortality Gap: What the Numbers Actually Mean for You
Black women in the United States face a persistently higher breast cancer mortality rate than white women — and the gap exists even when income and insurance status are controlled for.
The 40% gap — what this number actually measures
According to CDC breast cancer mortality surveillance data, Black women are approximately 40% more likely to die from breast cancer than white women.
📊 Clinical Data Point: Black women face a breast cancer death rate approximately 40% higher than white women, despite having comparable or lower incidence in several age groups — Source: CDC cancer surveillance, 2026.
That figure describes a population pattern — not an individual outcome. The gap is concentrated in specific tumor subtypes, age groups, and geographic regions. It is not a biologically fixed ceiling on what any individual Black woman’s outcome can be.
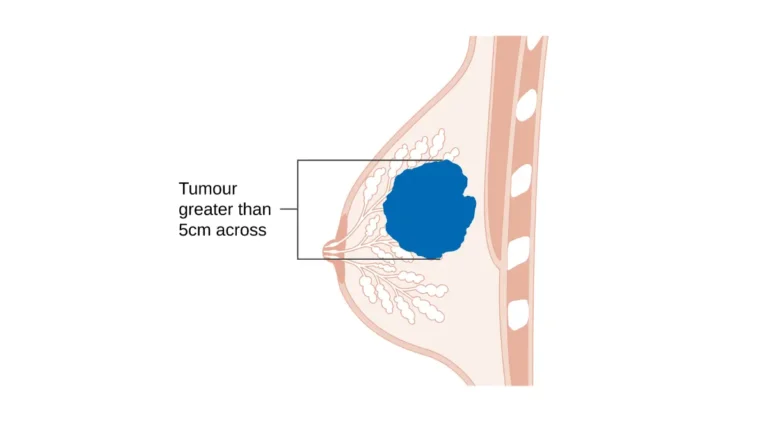
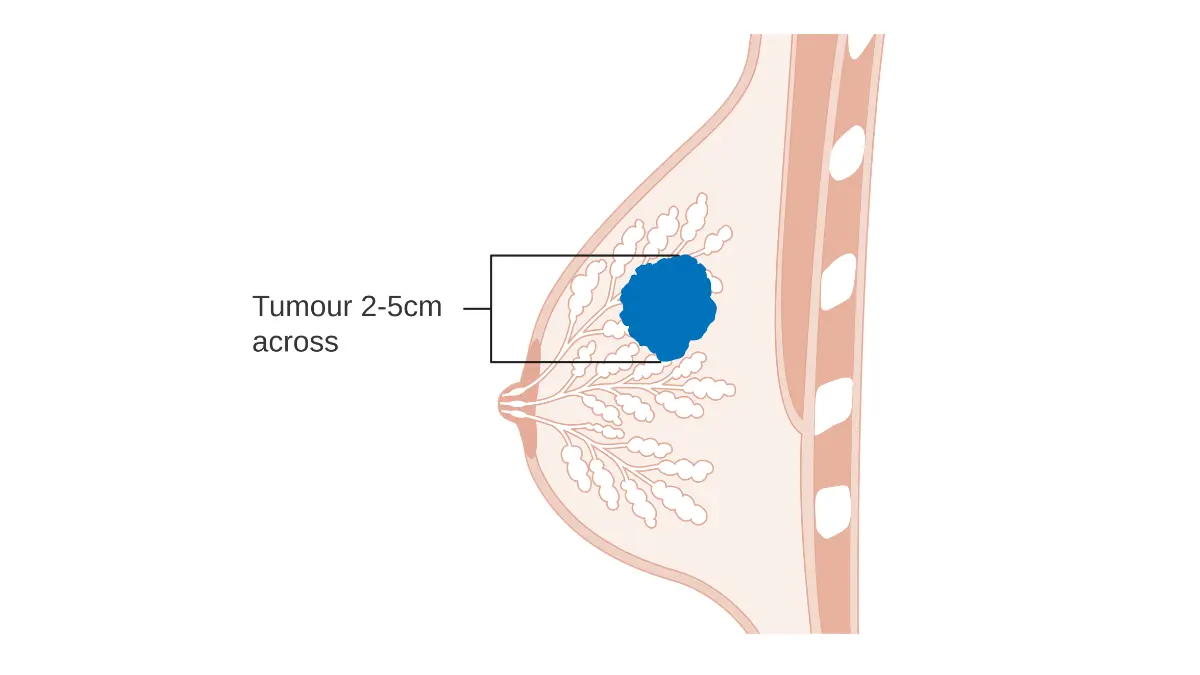
Black women are diagnosed with late-stage breast cancer at disproportionately higher rates than white women. Stage at diagnosis — not race in isolation — is the dominant predictor of survival. Recognizing the early warning signs of breast cancer and knowing your complete breast cancer risk profile by category are two of the most direct individual-level interventions available before a diagnosis is made.
Two causes, not one — and why the distinction matters for your survival
The racial disparity driving this gap has two distinct and separately addressable mechanisms.
The first is biological: a specific tumor subtype — triple-negative breast cancer — appears at significantly higher rates in Black women and is resistant to the most commonly prescribed breast cancer drug classes. The second is systemic: insurance gaps, implicit clinical bias in symptom assessment, and documented referral delays push Black women further into the disease trajectory before treatment begins. Both causes are real. The distinction matters because each one requires a different response.
The Tumor Biology Difference: TNBC and Genetic Risk in Black Women
Triple-negative breast cancer — defined by the absence of estrogen receptor (ER), progesterone receptor (PR), and HER2 protein expression — affects approximately 25% of Black women diagnosed with breast cancer, compared with roughly 10–15% of white women.
📊 Clinical Data Point: TNBC prevalence in Black women with breast cancer is estimated at approximately 25%, compared with 10–15% in white women — Source: NCI.
What triple-negative means — and why it limits standard treatment
🔬 How It Works: The three most widely prescribed breast cancer drug classes each work by targeting a specific molecular receptor. Tamoxifen and aromatase inhibitors block estrogen receptors. Trastuzumab (Herceptin) targets HER2 protein overexpression. Triple-negative tumors carry none of these molecular targets — which locks out all three drug classes. The remaining systemic options are chemotherapy, immunotherapy (pembrolizumab for PD-L1–positive tumors), and PARP inhibitors (for women who carry a BRCA1 or BRCA2 pathogenic variant).
TNBC is not simply “more aggressive.” It is specifically resistant to hormonal therapy and HER2-directed agents — a mechanistic distinction that determines the entire treatment pathway from the first oncology appointment forward. For a detailed breakdown of how TNBC is staged and treated, see our complete guide to triple-negative breast cancer treatment options and prognosis.
BRCA1 and West African ancestry: the genetic connection explained
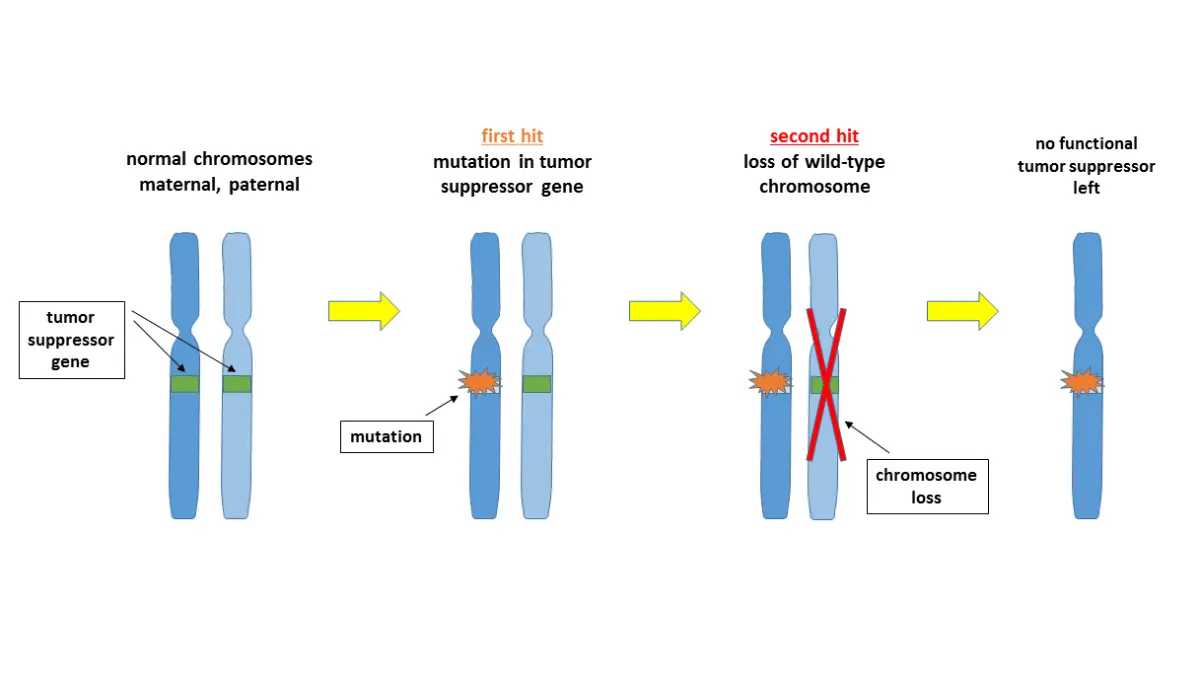
Specific BRCA1 pathogenic variants — including founder mutations that occur at higher documented frequencies in populations of West African genetic ancestry — are strongly associated with triple-negative tumor biology. A woman who carries a BRCA1 mutation has a significantly elevated risk of developing TNBC specifically, not breast cancer in general.
This is why BRCA1/2 testing is not equally offered across patient populations — and why that clinical gap matters directly to outcomes.
✅ Patient Action: If you have not been offered BRCA1/2 genetic testing and you are a Black woman with a breast cancer diagnosis or a first-degree family history of breast or ovarian cancer, ask a board-certified genetic counselor or gynecologic oncologist: “Does my ancestry profile, personal history, and tumor subtype qualify me for BRCA1/2 testing under the current NCCN criteria?” Use our genetic risk assessment tool to document your family history before that appointment. Our guide to what a positive BRCA gene test result means for your treatment plan explains how that result changes your surgical, pharmacological, and screening options.
Why the Healthcare System Delays Diagnosis for Black Women
The biological cause of the breast cancer disparities gap is real. The systemic cause is equally documented — and it operates before a single treatment decision is ever made.
Insurance status and the diagnostic delay it creates
Lack of insurance or inadequate coverage is directly correlated with later stage at breast cancer diagnosis. Screening mammograms, diagnostic imaging, and genetic testing all require coverage to be clinically accessible in a timely way.
📊 Clinical Data Point: Uninsured and underinsured women are significantly more likely to be diagnosed at Stage III or IV breast cancer than women with private insurance — Source: 2026 publication.
Black women are disproportionately represented among the uninsured and underinsured in the United States, and the downstream effect on stage at first diagnosis is measurable and documented.
Implicit bias at the clinical appointment — what the research shows
There is a documented pattern of implicit clinical bias in pain assessment and symptom severity rating for Black patients across multiple medical specialties. In the breast cancer context, this translates directly to a higher rate of under-referral after an initial symptom report to a primary care provider.
A Black woman who reports a palpable breast mass or unexplained breast pain is statistically more likely to be asked to monitor and wait before receiving an imaging order or specialist referral. That waiting period adds weeks or months to the diagnostic timeline at the highest-risk stage of the disease course.
The referral gap: how long Black women wait for a specialist
The interval between first reported breast symptom and first oncology specialist referral is longer, on average, for Black women than for white women with equivalent symptom presentations. That gap is not biologically caused. It is a documented systemic failure with a direct stage-at-diagnosis consequence.
If you are navigating this on behalf of a family member, our guide to supporting a loved one through a breast cancer diagnosis includes specific language you can use at clinical appointments to advocate for faster specialist access.
✅ Patient Action: If you have reported a breast symptom to a primary care provider and have not received a specialist referral within a clinically appropriate timeframe, ask directly: “What guideline governs the referral timeline for a presentation like mine, and does my demographic risk profile qualify me for an expedited referral?” A board-certified gynecologic oncologist or breast specialist — not a general practitioner — is the appropriate clinician for this next conversation.
Breast Cancer Survival Rates by Race and Stage: The 2026 Data
5-year survival rates: Black vs. white women by stage at diagnosis
“Stage at diagnosis — not race — is the single strongest predictor of breast cancer survival,” says Dr. Fairweather. The table below is drawn from NCI SEER breast cancer statistics by race and ethnicity and American Cancer Society Breast Cancer Facts and Figures, 2026.
| Stage at Diagnosis | Overall 5-Year Survival | Black Women (est.) | White Women (est.) | Key Clinical Note |
|---|---|---|---|---|
| Stage I | ~99% | ~96% | ~99% | Gap narrows substantially with equivalent treatment access |
| Stage II | ~86% | ~81% | ~87% | TNBC subtype prevalence difference contributes to gap |
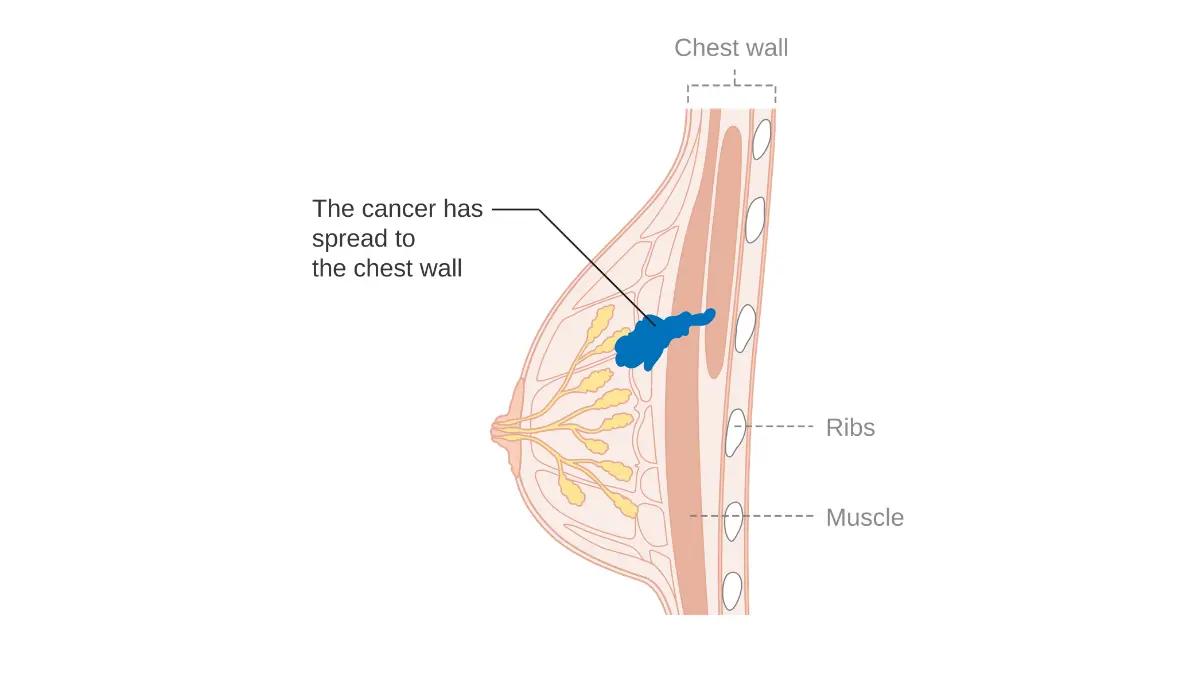
| Stage III | ~72% | ~64% | ~74% | Stage-at-diagnosis disparity most pronounced here |
| Stage IV | ~28% | ~23% | ~29% | PARP inhibitors available for BRCA1/2 carriers |
📊 Clinical Data Point: Stage-stratified, race-specific 5-year breast cancer survival rates — Source: NCI SEER, 2026 | ACS Breast Cancer Facts and Figures, 2026.
⚠️ Clinical Warning: These figures are population medians — not individual predictions. A Black woman diagnosed at Stage I with equivalent treatment access to a white woman at Stage I has comparable survival odds. The gap in the table is driven primarily by a higher proportion of Black women reaching diagnosis at Stage III or IV — not by a lower biological survival ceiling at any equivalent stage.
What these numbers mean for a Black woman diagnosed today
The survival gap is real and stage-dependent. The most powerful variable in your individual outcome is the stage at which your cancer is identified. For a complete stage-by-stage breakdown, see our guide to breast cancer survival rates by stage and treatment type.
✅ Patient Action: Ask your oncologist directly: “Given my specific stage, tumor subtype, and receptor status, how does my individual prognostic profile compare with the population averages in current SEER data?” A board-certified breast oncologist or gynecologic oncologist can interpret these population figures for your specific clinical situation.
What Black Women Can Do Right Now to Close the Survival Gap
Based on current NCCN clinical guidelines for high-risk populations, three specific actions can meaningfully change the stage at which breast cancer is identified — and the treatment options available at that moment.
Step 1: Have the screening age conversation before 40
The standard mammography screening recommendation does not account for elevated individual risk. Black women with dense breast tissue, a BRCA1/2 pathogenic variant, or a first-degree family history of breast or ovarian cancer may qualify for earlier annual mammography — in some risk categories beginning as early as age 30 — under NCCN high-risk population guidelines.
Our detailed guide to when Black women should start mammograms and how screening intervals are determined by risk profile explains precisely how risk factors change your recommended timeline.
Step 2: Request BRCA genetic testing if it has not been offered
If you are a Black woman and BRCA1/2 genetic counseling has never been offered, it has not been offered because the system defaulted to a lower-risk assumption — not because you do not qualify.
✅ Patient Action: At your next appointment, say this directly: “Given my ancestry profile and personal or family history, does my risk profile qualify me for BRCA1/2 testing under the current NCCN testing criteria?” That answer changes your screening schedule, your surgical risk-reduction eligibility, and your chemotherapy options if you are already diagnosed.
Step 3: Know when to ask for a second opinion — and how
A second opinion is a clinical right — not a confrontation. Most major cancer centers maintain a formal second-opinion program. Arriving with prepared questions accelerates that process significantly.
✅ Patient Action: Use our guide to questions to ask your oncologist at your next breast cancer appointment as your preparation checklist. Ask your provider specifically: “Can you refer me to a board-certified breast oncologist or gynecologic oncologist for a formal second opinion on my tumor subtype, BRCA mutation status, and treatment plan?” A competent specialist will not treat that question as a challenge.
A Gynecologic Oncologist’s Direct Message to Black Women With Breast Cancer
What I want every Black patient to know before their next oncology appointment
What I tell every Black patient who sits across from me in my practice is this: the statistics are real — and they describe a system, not you.
🩺 Physician Note: In my clinical experience, the Black women who achieve the best outcomes share one consistent pattern: they asked specific questions, they requested formal second opinions, and they did not accept a dismissal of their initial concern at face value. The disparity is structural. Your response to it can be strategic. The two most consequential appointments in your breast cancer trajectory are the one where you first report a symptom and the one where your treatment plan is set — and both are points where arriving prepared changes what happens next.
The language of “awareness” around breast cancer disparities understates what this gap actually is: a predictable, documentable system failure with a specific clinical mechanism at every stage of care.
Why clinical trial enrollment matters more for Black women than for anyone else
Black women are significantly underrepresented in the oncology clinical trials that validated the treatments currently offered as standard of care.
📊 Clinical Data Point: Black women represent a disproportionately small percentage of participants in the pivotal oncology trials that established pembrolizumab for early high-risk TNBC and olaparib for BRCA-mutated HER2-negative breast cancer as standard therapies — Source: 2026 trial enrollment demographic data
This matters because treatment efficacy data specifically for Black women is thinner than for white women — a gap that enrollment in current trials can begin to close. Our guide to active breast cancer clinical trials enrolling patients now includes protocols specifically designed to address this enrollment gap.
✅ Patient Action: Ask your oncologist: “Am I eligible for any active clinical trial that prioritizes enrollment from underrepresented populations?” Then search active clinical trials for breast cancer patients directly. A board-certified breast oncologist at a comprehensive cancer center — or a dedicated clinical trial navigator — can run this eligibility search on your behalf.
Frequently Asked Questions About Breast Cancer Disparities in Black Women
1. Why do Black women have a higher breast cancer death rate than white women?
Breast cancer disparities in mortality are driven by two documented causes: a higher prevalence of triple-negative breast cancer — a subtype resistant to standard hormonal and HER2-directed therapies — and systemic healthcare failures including insurance gaps, implicit clinical bias, and referral delays that result in later-stage diagnoses. Both causes are real. Both are separately addressable through specific clinical and self-advocacy actions.
2. What is the 5-year breast cancer survival rate for Black women?
Survival rates differ primarily by stage at diagnosis, not by race alone. At Stage I, Black and white women have nearly comparable outcomes when treatment access is equivalent. The gap widens at Stage III and IV, where Black women are diagnosed at disproportionately higher rates. Stage at diagnosis — shaped by screening access and referral timing — is the strongest predictor of outcome. Consult a board-certified breast oncologist to interpret population figures in the context of your specific stage and tumor subtype.
3. Does triple-negative breast cancer affect Black women more often?
Yes. Triple-negative breast cancer — defined by absent estrogen, progesterone, and HER2 receptors — affects approximately 25% of Black women with breast cancer, compared with roughly 10–15% of white women. TNBC cannot be treated with hormonal or HER2-directed therapies, leaving chemotherapy, immunotherapy, and PARP inhibitors as the primary systemic options. Ask a board-certified breast oncologist whether pembrolizumab or olaparib eligibility applies to your specific case.
4. Why are Black women more often diagnosed with breast cancer at a later stage?
Three documented systemic barriers drive later-stage diagnosis: inadequate insurance coverage limiting access to screening mammograms, implicit clinical bias resulting in symptom dismissal and delayed specialist referrals, and geographic barriers to oncology access. If you have reported a breast symptom without receiving a referral, ask your provider directly for an expedited referral to a board-certified gynecologic oncologist or breast specialist — not a general practitioner.
5. What genetic factors increase breast cancer risk in Black women specifically?
Specific BRCA1 pathogenic variants — including founder mutations occurring at higher documented frequency in populations of West African genetic ancestry — are associated with triple-negative tumor biology and elevated lifetime breast and ovarian cancer risk. BRCA1/2 testing is not universally offered at primary care. Ask a board-certified genetic counselor whether your ancestry profile and personal or family history qualify you for testing under current NCCN criteria.
6. How can Black women reduce their breast cancer risk and improve survival odds?
Three actions have the strongest clinical evidence: scheduling a dedicated risk assessment with a breast specialist before age 40, requesting BRCA1/2 genetic testing if it has not been offered, and asking explicitly about clinical trial eligibility. Risk reduction depends on tumor biology, genetic status, and screening history. Consult a board-certified breast oncologist or gynecologic oncologist for a personalized plan that accounts for your individual risk profile.
7. Should Black women start mammograms before age 40?
Black women with dense breast tissue, a BRCA1/2 pathogenic variant, or a first-degree family history of breast or ovarian cancer may qualify for earlier annual screening mammography — beginning as early as age 30 in some risk categories — under NCCN high-risk population guidelines. Ask a board-certified breast specialist whether your risk profile qualifies for earlier or supplemental MRI screening before your standard screening start age.
8. Does insurance status affect breast cancer survival outcomes in Black women?
Yes. Uninsured and underinsured women are significantly more likely to be diagnosed at Stage III or IV breast cancer because screening mammograms, diagnostic imaging, and genetic testing require coverage to be accessible. Black women are disproportionately represented among the underinsured. If you are currently uninsured, contact your state’s Medicaid office or a cancer center patient navigator about coverage for breast cancer screening and genetic testing.
9. Are there clinical trials specifically enrolling Black women with breast cancer?
Several active oncology trials specifically prioritize enrollment from underrepresented populations, including Black women. Black women have been significantly underrepresented in trials validating current TNBC and BRCA-mutated breast cancer therapies, meaning efficacy data specific to Black women remains thinner. Ask your oncologist to search for active trials with underrepresentation as an explicit enrollment priority, or ask a clinical trial navigator at a comprehensive cancer center to conduct that search on your behalf.
10. What specific questions should a Black woman ask her oncologist about breast cancer?
Four questions with the highest clinical impact: (1) “Has my tumor been fully typed for ER, PR, and HER2 receptor status?” (2) “Does my ancestry profile and family history qualify me for BRCA1/2 testing under current NCCN criteria?” (3) “Does my personal risk profile support earlier or more frequent mammography?” (4) “Am I eligible for a clinical trial that prioritizes underrepresented populations?” These questions are most productive in a dedicated appointment with a board-certified breast oncologist or gynecologic oncologist.
11. Is the breast cancer survival gap between Black and white women closing?
The gap has narrowed modestly in some age groups over the past decade but has not closed. Two structural barriers maintain it: persistent underrepresentation in clinical trials producing thinner treatment efficacy data for Black women, and ongoing insurance and referral disparities that drive later-stage diagnoses. Individual action — earlier screening, genetic testing, and clinical trial enrollment — changes personal outcomes independent of any population-level trend line.
Your Next Step Starts Before Your Next Appointment
The survival gap described in this article is real. Its two causes — tumor biology and systemic failure — are both documented, and both are addressable.
What is equally documented is this: when Black women are diagnosed at Stage I, when they receive BRCA testing, when they access specialist care without delay, and when they enroll in clinical trials, their outcomes improve. The gap is not biologically fixed.
The single most protective action available to you today is scheduling a dedicated risk assessment with a board-certified gynecologic oncologist or breast specialist — and arriving with the questions outlined in this article.
For the clinical foundation behind every decision ahead, start with our complete guide to breast cancer staging and what survival rates actually mean.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.