On This Page – Quick Medical Summary
If you are reading this, you are probably in one of four places right now, and where you start should depend on which one it is.
If you were just diagnosed and you are trying to understand what this means, the two sections that will steady you fastest are the one on survival rates by stage and the one on choosing between active surveillance and treatment. Most prostate cancer is not the emergency it first feels like.
If you are worried about symptoms or a PSA result and have not yet seen a specialist, start with the signs section and the screening section, in that order.
If you already have a diagnosis and are choosing how to treat it, go straight to the treatment-comparison section and the side-effects section, where the real tradeoffs live.
If you are caring for a partner or parent and doing this research for someone else, the treatment-comparison section and the list of questions to bring to the specialist will give you the most leverage in the least time.
Wherever you start, here is the single most important thing to hold onto before you read another word. Prostate cancer is the most common cancer diagnosed in men, but for most men it grows slowly, and when it is caught before it spreads, the 5-year relative survival rate approaches 100%. The fear you are feeling is real. The odds, for the majority of men, are better than that fear suggests.
ℹ️ Medical Disclaimer: The diagnostic criteria, screening guidance, staging definitions, treatment options, medication information, surgical and radiation procedure descriptions, genetic-risk discussion, and insurance and coverage notes in this article reflect current clinical guidelines and are provided for educational purposes only. Individual diagnostic conclusions, screening decisions, treatment choices, medication selection, procedure consent, and genetic testing decisions depend on factors including your age, PSA level, Gleason score and Grade Group, stage, life expectancy, comorbidities, family history, and specialist assessment. Consult a board-certified urologist, urologic oncologist, genitourinary medical oncologist, or radiation oncologist before acting on any clinical information here.
What prostate cancer is and how it develops
Prostate cancer begins when cells in the prostate gland start growing in an uncontrolled way, and understanding what that gland does explains why this cancer behaves the way it does.
What the prostate does and where it sits
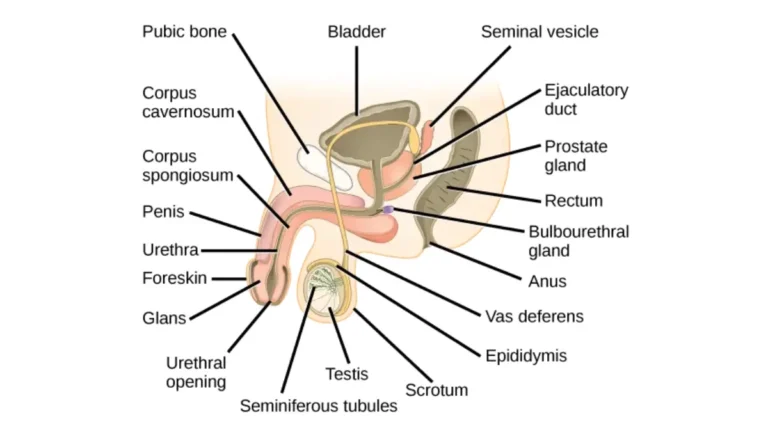
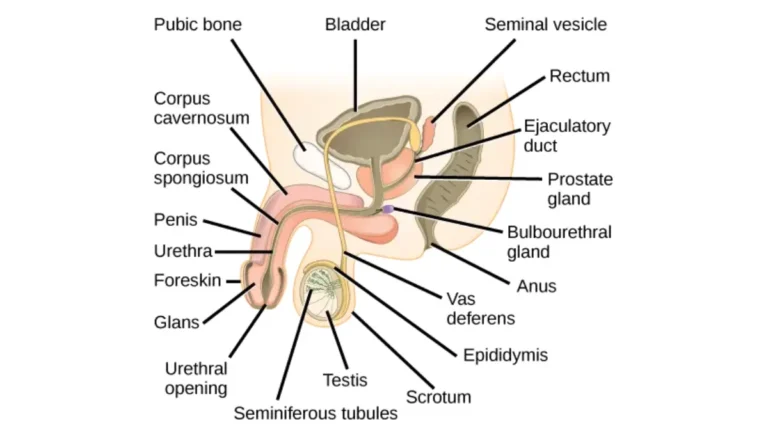
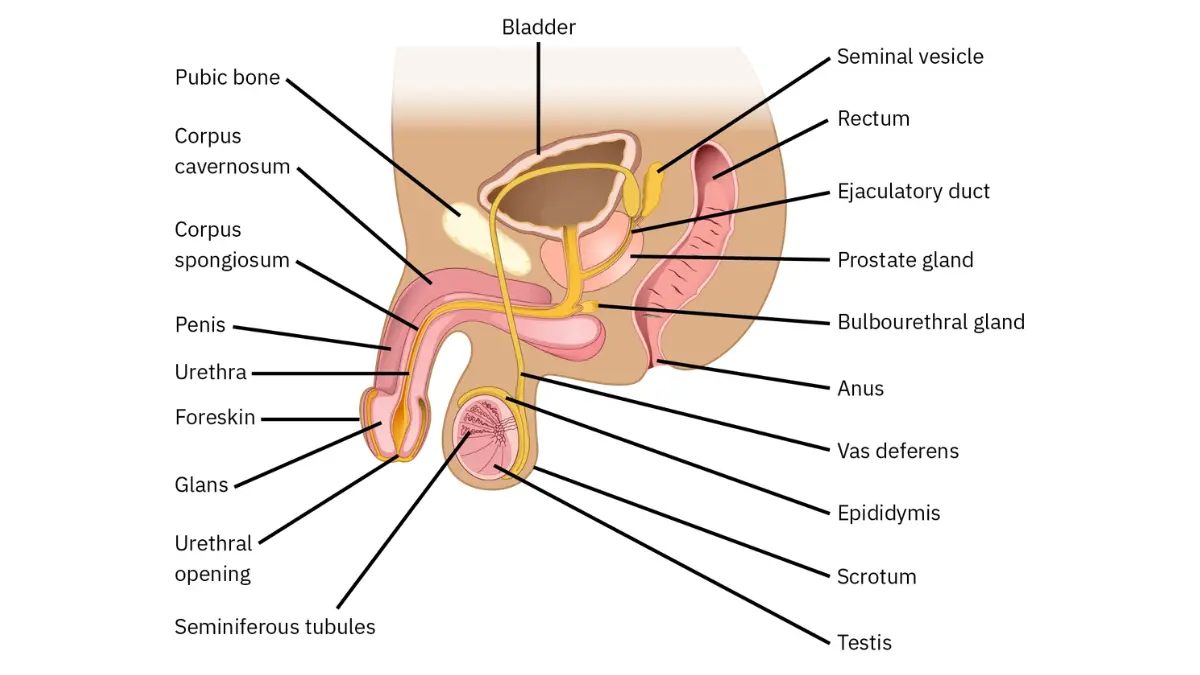
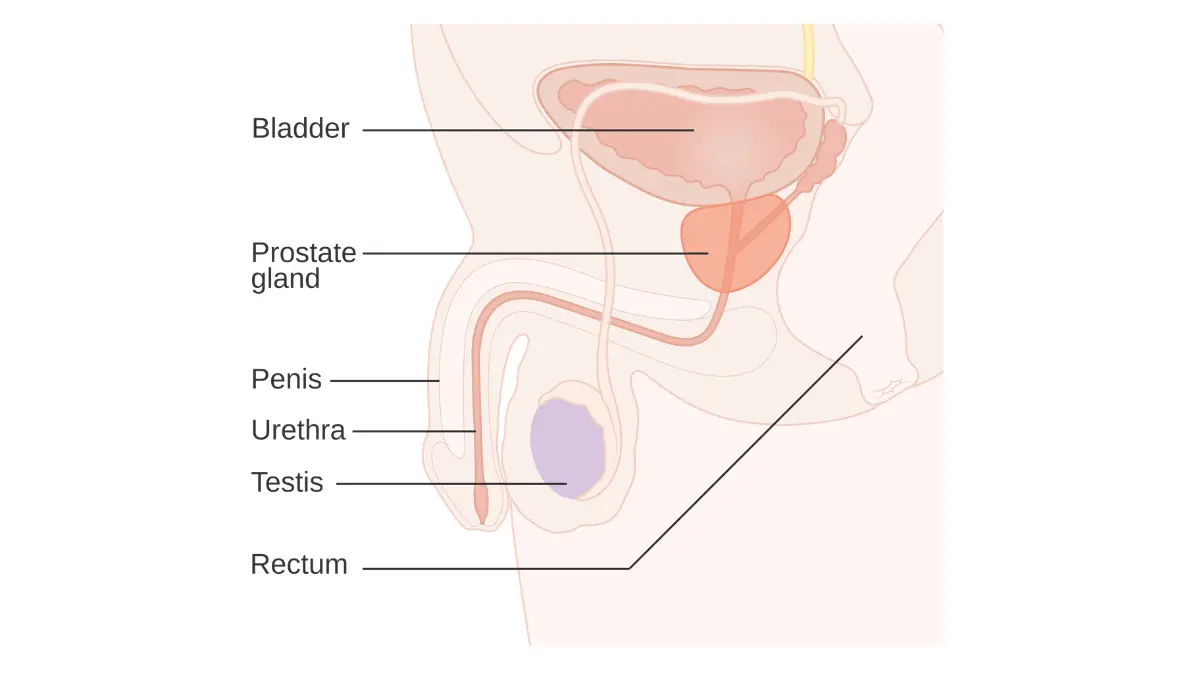
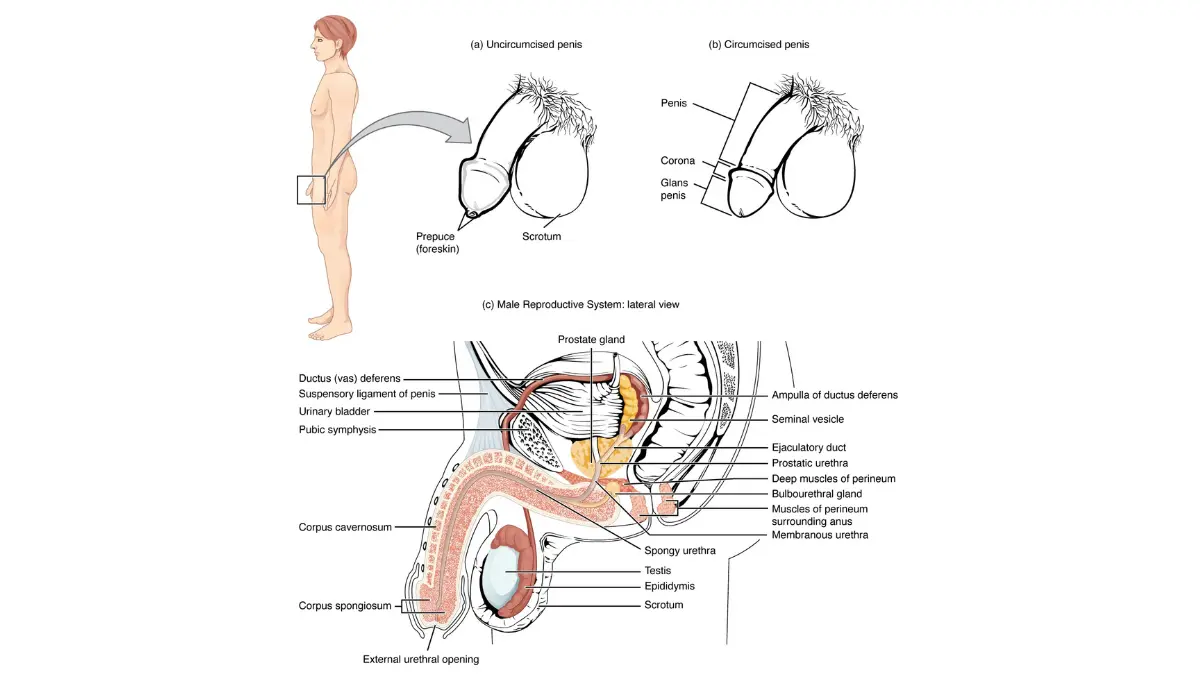
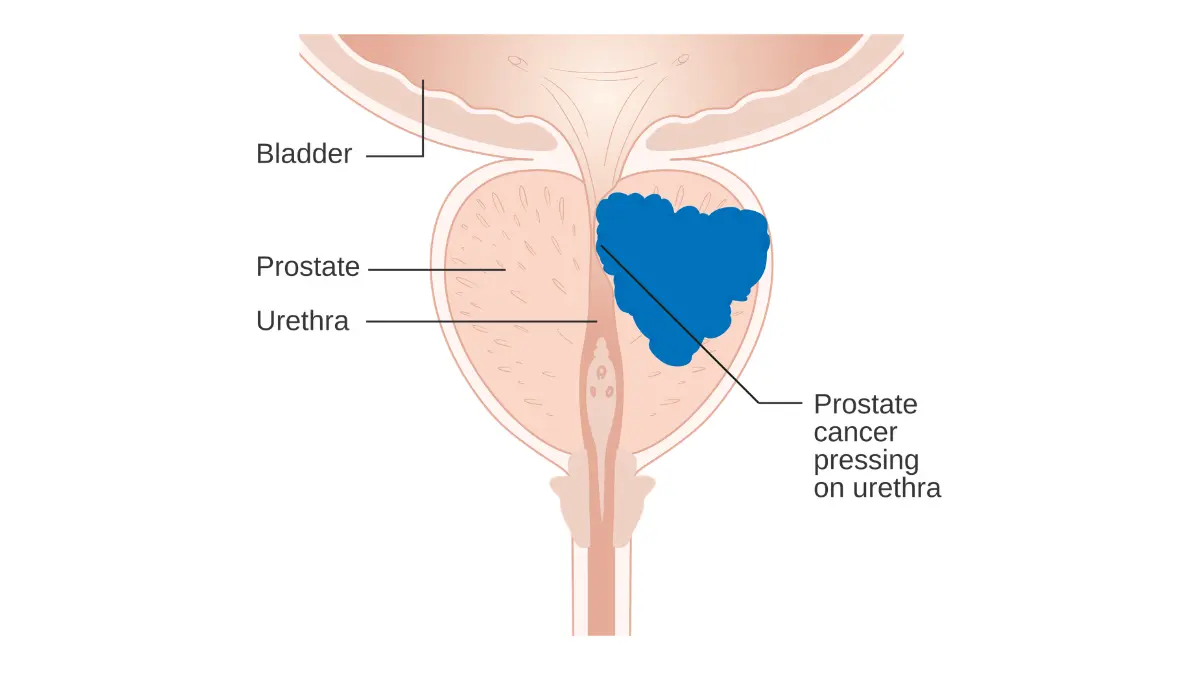
The prostate gland is a walnut-sized gland that sits just below the bladder and in front of the rectum, wrapped around the top of the urethra. Its main job is to make part of the fluid that nourishes and carries sperm.
Because the urethra runs directly through it, anything that enlarges the prostate — cancer, but far more often a benign condition — can press on that tube and change the way a man urinates. That anatomy is why urinary symptoms get so much attention, and also why they are so often misread.
How prostate cancer starts and why it’s often slow-growing
Most prostate cancers are adenocarcinomas, meaning they arise from the gland cells that produce prostatic fluid. They typically begin in the outer (peripheral) zone of the prostate, which is part of why early disease so rarely causes symptoms — a small tumor there is nowhere near the urethra.
A defining feature of this cancer is how variable its pace is. Many prostate cancers grow so slowly that they would never threaten a man’s life within his natural lifespan, while a minority are genuinely aggressive and spread early.
🔬 How It Works: Prostate cancer cells usually keep making prostate-specific antigen (PSA), the same protein normal prostate cells produce. When cancer is present, more of this protein can leak into the bloodstream, which is why a PSA blood test can raise suspicion long before any symptom appears. PSA is not cancer-specific, though — a benign enlarged prostate, infection, or even recent ejaculation can raise it too, which is exactly why a single number never tells the whole story.
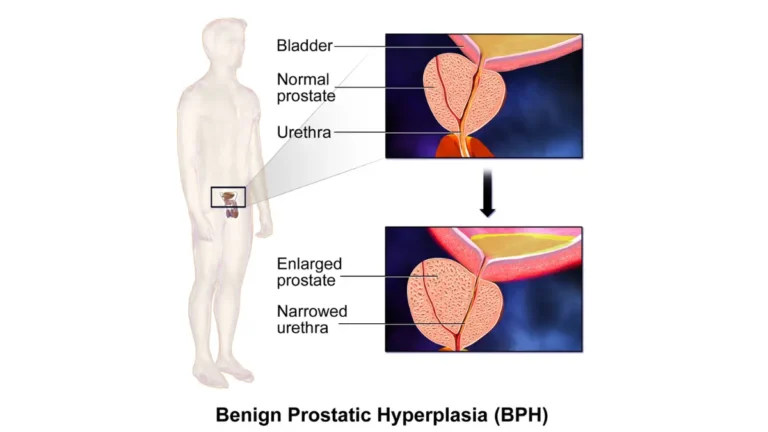
Prostate cancer vs. an enlarged prostate (BPH)
This is the distinction that causes the most needless fear, so it is worth getting right. Benign prostatic hyperplasia (BPH) is a non-cancerous enlargement of the prostate that is extremely common with age and causes urinary symptoms by squeezing the urethra.
BPH is not cancer, does not become cancer, and does not raise your cancer risk. The two conditions can coexist, and they can produce similar urinary symptoms, but they are biologically different — BPH is overgrowth of normal cells, while cancer is the growth of malignant ones.
The practical consequence: the urinary symptoms most men worry about are far more often BPH than cancer. That does not mean they should be ignored, but it does mean they are usually not the catastrophe they feel like at 2am.
The signs and symptoms men miss
The hardest truth about prostate cancer symptoms is that the cancers most worth catching early usually cause no symptoms at all.
Why early prostate cancer usually has no symptoms
Because most prostate cancers start in the peripheral zone, away from the urethra, early prostate cancer typically produces no warning signs a man would notice. This is the central reason the screening conversation exists — by the time symptoms appear from the tumor itself, the disease is often more advanced.
This is also why “I feel fine” is not reassurance about prostate cancer specifically. Feeling well is the normal state of a man with early, localized disease.
Urinary changes and what they can mean
When urinary symptoms do occur, they are far more often caused by BPH than by cancer, but they are still worth evaluating. The urinary symptoms men report include:
- A weak or interrupted urine stream, or having to push or strain to start
- Needing to urinate more often, especially at night (nocturia)
- A sudden, hard-to-control urge to urinate
- A feeling that the bladder does not fully empty
- Difficulty starting urination despite the urge
Each of these can come from a benign enlarged prostate, a urinary tract infection, or other causes. The point of listing them is not to alarm you but to give you language for the conversation with a clinician, who can sort out the cause.
Symptoms of advanced prostate cancer
A different set of symptoms can appear when prostate cancer has spread beyond the gland, and these warrant prompt medical attention rather than watchful waiting at home:
- New, persistent bone pain, especially in the back, hips, or pelvis
- Blood in the urine or semen
- Unexplained weight loss or fatigue
- New erectile difficulty alongside other changes
- Weakness or numbness in the legs, or new trouble with bladder or bowel control (which can signal spinal cord involvement and is a medical emergency)
⚠️ Clinical Warning: New weakness or numbness in the legs, or a sudden loss of bladder or bowel control, can signal spinal cord compression from cancer that has spread to the spine. This is a medical emergency — seek emergency care the same day rather than waiting for a scheduled appointment.
When to see a doctor
You do not need to wait for advanced symptoms to act, and you should not. Persistent urinary changes, any blood in the urine or semen, or new unexplained bone pain are all reasons to be evaluated.
If you want a starting point before booking, you can check your symptoms with our symptom checker, though a tool can only ever prompt the conversation — it cannot replace a clinician’s assessment. For the full picture of how these symptoms present, our guide to the early signs of prostate cancer goes deeper than this overview.
✅ Patient Action: If you have new bone pain that does not go away, blood in your urine or semen, or urinary symptoms that are steadily worsening, see a urologist or your primary care physician and ask specifically: “Given my age, race, and family history, is a PSA test and digital rectal exam appropriate for me now?”
Who’s at risk: age, family history, and genetics
Knowing your real risk level changes when you should start the screening conversation and, for some men, what treatment options will later be available.
Age, race, and the risk factors you can’t change
The strongest risk factors for prostate cancer are ones no one can control:
- Age. Risk rises sharply after 50; the majority of diagnoses occur in men over 65.
- Race and ancestry. Black men are diagnosed more often, tend to be diagnosed younger, and are more likely to have aggressive disease.
- Family history. Having a father or brother with prostate cancer roughly doubles a man’s risk, and the risk climbs further with more affected relatives or relatives diagnosed young.
📊 Clinical Data Point: About 1 in 8 men will be diagnosed with prostate cancer in his lifetime, and Black men and Native American men carry the highest prostate cancer mortality of any groups in the United States (American Cancer Society, Cancer Statistics 2026 and Prostate Cancer Statistics). These disparities reflect a mix of biology and differences in access to early detection and care.
When prostate cancer runs in the family
Family history matters in two ways. It raises a man’s baseline risk, and it can be a clue to an inherited mutation that affects both screening timing and, later, treatment.
A pattern worth flagging to a doctor is prostate cancer in multiple close relatives, a relative diagnosed before 65, or a family history that also includes breast, ovarian, or pancreatic cancer. That mix can point toward a hereditary cancer syndrome.
BRCA and inherited risk: when genetic testing matters
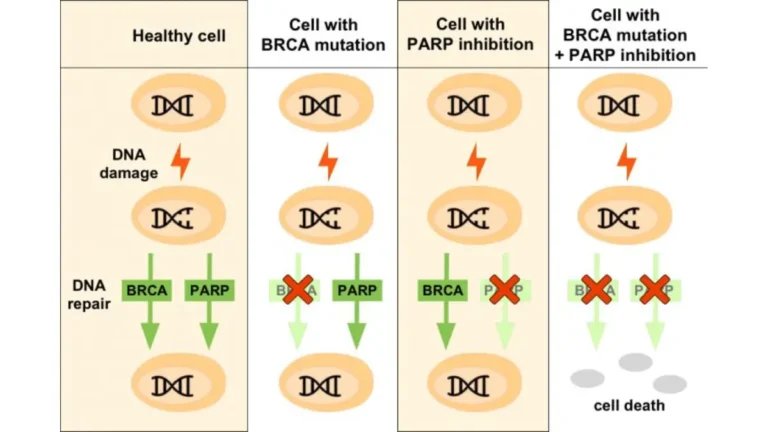
Most people associate BRCA1 and BRCA2 mutations with breast and ovarian cancer, but these same genes raise prostate cancer risk and can make the disease more aggressive. They belong to a larger group of homologous recombination repair (HRR) genes that help cells fix damaged DNA.
🔬 How It Works: Genes like BRCA1, BRCA2, ATM, and CHEK2 normally repair breaks in a cell’s DNA. When one is mutated, DNA damage accumulates and cancer becomes more likely — and the tumor that results often has the same repair defect. That defect is not only a risk factor; later in the disease it becomes a treatment target, because drugs called PARP inhibitors exploit cells that cannot repair their own DNA.
A germline (inherited) mutation also has implications for your relatives, who may want testing of their own. If your family history fits the pattern above, you can assess your inherited risk before raising genetic testing with your doctor.
✅ Patient Action: If a first-degree relative was diagnosed with prostate cancer before 65, or your family has a history of BRCA-related cancers (breast, ovarian, pancreatic), ask your doctor: “Do I meet criteria for germline genetic testing and a referral to genetic counseling?”
Should you get screened? PSA testing explained
Prostate cancer screening is one of the few cancer screenings where the right answer genuinely depends on the individual, so this section is built to help you decide rather than to push you in either direction.
What a PSA test measures and what’s “normal”
There is no single PSA number that means “cancer” and no single number that means “safe.” The PSA test measures prostate-specific antigen in the blood, and while higher levels are associated with higher prostate cancer risk, the relationship is a gradient, not a line in the sand.
Historically a level under 4 nanograms per milliliter was treated as reassuring, but cancer can occur below that and many men above it do not have cancer. Modern practice looks at the trend over time, the PSA density (PSA relative to prostate size), the ratio of free to total PSA, your age, and your risk factors — not the single number alone.
Can you have prostate cancer with a normal PSA?
Yes. A “normal” PSA lowers the probability of significant prostate cancer but does not rule it out, which is one reason a digital rectal exam (DRE) and your risk profile still matter.
This is also why a reassuring PSA is not a reason to ignore new symptoms or a strong family history. The number is one input among several.
Screening guidelines by age and risk
Major guidelines agree on one thing above all: PSA screening should be a shared decision-making conversation, not an automatic test. They differ on the specifics.
| Guideline | Average-risk men | Higher-risk men | Key point |
|---|---|---|---|
| USPSTF (2018) | Individual decision, ages 55–69 (grade C) | — | Not recommended at 70+ |
| American Cancer Society | Discuss starting at age 50 (10+ yr life expectancy) | Discuss at 45 (Black men; father/brother diagnosed before 65); at 40 (multiple relatives diagnosed young) | Emphasizes informed, shared decision-making, not routine testing |
| AUA/SUO (2026) | Shared decision-making; risk calculators and MRI used to refine who needs biopsy | Earlier discussion for higher-risk men | PSA velocity alone should not trigger biopsy |
Sources: U.S. Preventive Services Task Force recommendation (2018); American Cancer Society early-detection guidance; American Urological Association/Society of Urologic Oncology Early Detection of Prostate Cancer guideline (2026).
📊 Clinical Data Point: The USPSTF (2018) gives PSA-based screening a grade C recommendation for men aged 55 to 69, meaning the decision should be an individual one, and recommends against routine PSA screening for men 70 and older. The American Cancer Society frames the screening conversation beginning at age 50 for average-risk men, 45 for higher-risk men, and 40 for those at highest risk.
The benefit-versus-overdiagnosis tradeoff
Here is the real tension, stated plainly. Screening can catch aggressive cancer early, when it is most curable — and it can also detect slow-growing cancers that would never have caused harm, leading some men to treatments with lasting side effects they did not need.
This is why the decision is individual. A 58-year-old Black man with a father diagnosed at 60 has a very different calculus than a 72-year-old man with significant heart disease and a 10-year life expectancy.
Newer tools: MRI and biomarkers before biopsy
The screening pathway has improved specifically to reduce unnecessary biopsies. A multiparametric MRI (mpMRI) before biopsy can show whether a suspicious area is likely to be significant, and validated blood and urine biomarkers can further refine who truly needs a biopsy.
If you want the deeper mechanics of PSA interpretation, our explainer on what your PSA level actually means breaks down free versus total PSA, PSA density, and velocity. The CDC’s overview of prostate cancer screening summarizes the same benefit-and-harm tradeoff in plain language.
✅ Patient Action: Before agreeing to or declining a PSA test, ask a urologist or your primary care physician: “Given my specific age, race, and family history, do the benefits of screening outweigh my personal risk of overdiagnosis and overtreatment?”
How prostate cancer is diagnosed
If a PSA result or exam raises concern, a defined sequence of steps turns suspicion into an actual diagnosis — and the order of those steps has changed for the better.
From elevated PSA to next steps
An elevated or rising PSA does not mean you have cancer, and the next step is rarely an immediate biopsy. A clinician will usually repeat the PSA, consider causes like infection or recent ejaculation, and look at the full picture before going further.
The modern pathway, in order, generally runs: PSA and DRE, then mpMRI if suspicion persists, then a targeted biopsy if the MRI shows something concerning, and finally additional imaging only if the cancer looks like it could have spread.
Why an MRI now often comes before biopsy
For years, men with an elevated PSA went straight to biopsy. Today, an MRI first is increasingly standard because it changes who needs the needle at all.
🔬 How It Works: A multiparametric MRI combines several types of MRI images to map suspicious areas of the prostate and score them by how likely they are to harbor significant cancer. If the MRI is clear, some men can safely avoid a biopsy; if it shows a suspicious lesion, the biopsy can be aimed directly at it rather than sampling the gland blindly. The result is fewer unnecessary biopsies and better detection of the cancers that actually matter.
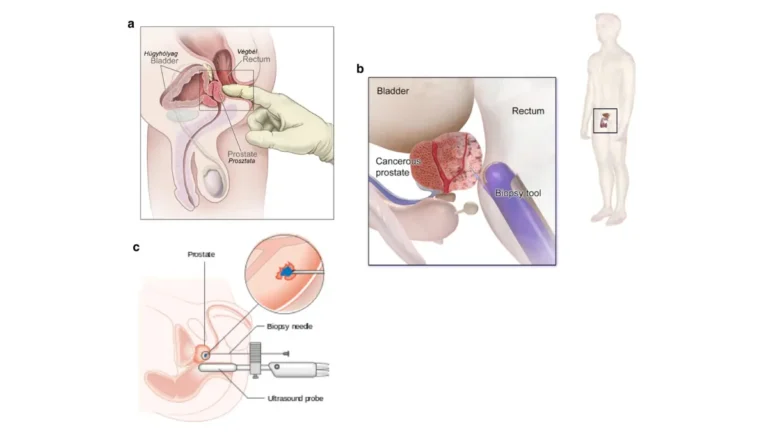
What a prostate biopsy actually involves
A prostate biopsy removes small cores of tissue so a pathologist can confirm whether cancer is present and how aggressive it looks. There are two main approaches, and the difference matters more than most men are told.
- Transrectal biopsy passes the needle through the rectal wall. It is widely used but carries a small risk of serious infection.
- Transperineal biopsy passes the needle through the skin between the scrotum and anus, which has been shown to substantially lower the infection risk and is increasingly preferred.
The procedure is usually done with local anesthesia, takes a short time, and is associated with temporary blood in the urine or semen afterward. Knowing which approach your urologist uses, and why, is a fair question to ask.
PSMA-PET imaging and when it’s used
For men whose cancer looks higher-risk, a newer scan can find disease that older imaging misses. A PSMA-PET scan uses a tracer that binds to prostate-specific membrane antigen on prostate cancer cells, lighting them up on a PET scan with greater accuracy than a traditional CT or bone scan for detecting spread.
✅ Patient Action: If your PSA is elevated, ask your urologist: “Is a multiparametric MRI appropriate before any biopsy in my case?” — because for many men it can avoid an unnecessary biopsy or make the biopsy more accurate.
Understanding your Gleason score and Grade Group
The two numbers on a prostate pathology report that confuse men most — the Gleason score and the Grade Group — are also the ones that most determine what happens next.
What the Gleason score means
The Gleason score measures how abnormal the cancer cells look under the microscope, which predicts how aggressively the cancer is likely to behave. A pathologist grades the two most common cell patterns from 3 to 5 and adds them, so reported scores run from 6 to 10.
Here is the part most websites get wrong: the scale effectively starts at 6, not 2. A Gleason 6 is the least aggressive cancer routinely diagnosed today, even though “6 out of 10” sounds frightening.
Grade Groups 1 to 5 in plain language
Because “Gleason 6” sounding mid-range caused so much needless fear, pathologists now also report a Grade Group from 1 to 5, where 1 is the least aggressive and 5 the most.
| Grade Group | Gleason score | What it generally means |
|---|---|---|
| Grade Group 1 | 6 (or 3+3) | Least aggressive; often suitable for active surveillance |
| Grade Group 2 | 7 (3+4) | Favorable intermediate risk |
| Grade Group 3 | 7 (4+3) | Unfavorable intermediate risk |
| Grade Group 4 | 8 | High risk |
| Grade Group 5 | 9–10 | Highest risk; most aggressive |
The 3+4 versus 4+3 distinction in Grade Groups 2 and 3 is not a technicality. The first number is the dominant pattern, so a 4+3 (Grade Group 3) is meaningfully more aggressive than a 3+4 (Grade Group 2), even though both are “Gleason 7.”
Why your grade drives your treatment options
Grade is the single biggest factor in whether monitoring is reasonable or treatment is urgent. A Grade Group 1 cancer is often a candidate for active surveillance, while a Grade Group 4 or 5 generally calls for prompt treatment.
For the full grading breakdown, see our explainer on how Gleason scores and Grade Groups work.
✅ Patient Action: Ask your urologist to confirm your exact Grade Group in writing, and to explain how it combines with your PSA and stage into your overall risk category — because two men with the same Gleason 7 can have very different recommended paths depending on whether it is 3+4 or 4+3.
The stages of prostate cancer explained
Staging answers the question every newly diagnosed man asks — how far has it gone — and for prostate cancer the answer is built from more than anatomy alone.
How prostate cancer is staged (the TNM system)
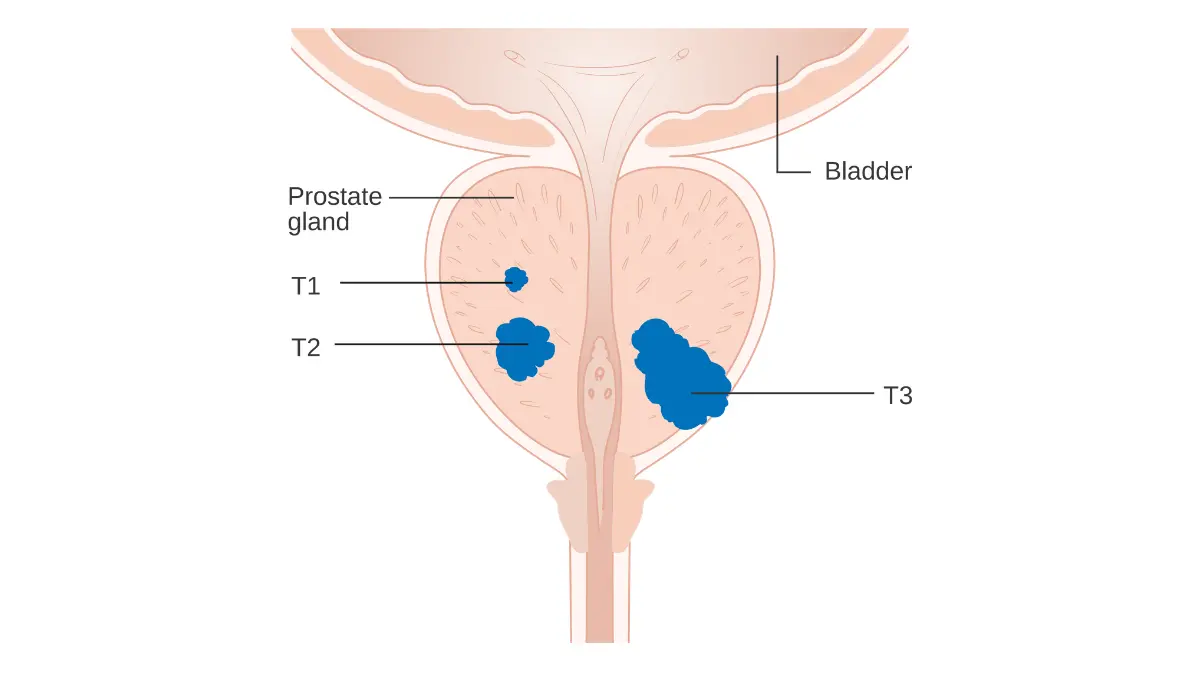
Doctors stage prostate cancer using the TNM staging system: T describes the size and extent of the tumor in and around the prostate, N whether it has reached nearby lymph nodes, and M whether it has spread (metastasized) to distant sites such as bone.
What makes prostate staging distinctive is that the final stage also incorporates your PSA level and your Grade Group, not just the physical extent of the tumor. That combination is why your stage reflects biology, not only geography.
Stages 1 through 4 in plain language
In broad terms, the four stages describe a progression from a cancer confined to the prostate to one that has spread to distant organs:
- Stage I: Cancer is small, confined to the prostate, low PSA, and low grade — often not even felt on exam.
- Stage II: Still confined to the prostate but larger, higher PSA, or higher grade.
- Stage III: Cancer has grown outside the prostate or into the seminal vesicles, or has high-risk features, but has not reached distant sites.
- Stage IV: Cancer has spread to nearby lymph nodes or to distant sites such as bones or other organs.
Risk groups: low, intermediate, and high
In day-to-day decisions, urologists often rely on risk stratification even more than the stage number. Combining PSA, Grade Group, and clinical stage, prostate cancer is grouped as low risk, intermediate risk (subdivided into favorable and unfavorable), or high risk.
These groups map directly onto options: low and favorable-intermediate risk open the door to active surveillance, while unfavorable-intermediate and high risk generally call for active treatment.
What “localized,” “regional,” and “metastatic” mean
You will also hear three plain-language terms that statistics are reported by. Localized means the cancer is confined to the prostate, regional means it has reached nearby tissue or lymph nodes, and metastatic (or distant) means it has spread to distant parts of the body.
Our dedicated guide covers the stages of prostate cancer in detail, including the substages within Stage II.
✅ Patient Action: Ask your urologist or urologic oncologist to state your full clinical stage and risk category, and to explain it in the localized/regional/metastatic terms the survival statistics use, so the numbers you read next actually apply to your situation.
Prostate cancer survival rates by stage
These are the numbers most men are afraid to look up, so they deserve to be presented honestly and with the context that lets you read them correctly.
5-year survival by stage, explained
The headline figure is genuinely reassuring for most men. When prostate cancer is caught before it spreads, survival is excellent; the figures drop sharply only once the disease has reached distant sites.
| Stage at diagnosis | 5-year relative survival | What it means |
|---|---|---|
| Localized (confined to prostate) | Approaches 100% | Cancer found before any spread |
| Regional (nearby nodes/tissue) | Approaches 100% | Limited local spread |
| Distant (metastatic) | About 37% | Spread to bone or distant organs |
Source: National Cancer Institute SEER program and American Cancer Society, Cancer Statistics 2026. Figures are 5-year relative survival for men diagnosed in recent years and describe groups, not individuals.
📊 Clinical Data Point: The 5-year relative survival rate for prostate cancer approaches 100% for localized and regional disease and is about 37% to 38% for distant-stage disease (National Cancer Institute SEER; American Cancer Society, Cancer Statistics 2026). The American Cancer Society estimates roughly 333,830 new prostate cancer diagnoses and about 36,320 deaths in the United States in 2026.
What these numbers do and don’t tell you
“Relative survival” compares men with prostate cancer to men without it, which is why the localized figure can approach 100%. It is a population statistic, and it cannot predict any single man’s outcome.
🩺 Physician Note: A survival percentage is a description of a large group of men diagnosed years ago, treated with the methods of that era. It is not a clock counting down for you. Your own outlook depends on your grade, your PSA, your overall health, and how your specific cancer responds to treatment — which is why I tell patients to use these numbers for reassurance and context, never as a personal prognosis.
Why survival has been improving
Two forces have pushed prostate cancer survival up over time: earlier detection through PSA testing, and a steady expansion of effective treatments for advanced disease. Even men with metastatic disease are living meaningfully longer than they did a generation ago.
The rising-late-stage trend and why early detection matters
There is one trend worth taking seriously. After years of decline, the rate of men diagnosed at an advanced stage has been rising, including in younger men, even as overall mortality declines have slowed.
📊 Clinical Data Point: Advanced-stage prostate cancer diagnoses have been rising by roughly 4.6% to 4.8% per year over the most recent reporting period, while the decline in prostate cancer mortality has slowed to about 0.6% per year (American Cancer Society, Prostate Cancer Statistics). This is precisely why an informed screening decision matters — the disease is most curable before it spreads.
Our full breakdown of prostate cancer survival rates by stage includes 10-year and cause-specific figures. For the underlying data, the NCI’s SEER survival statistics for prostate cancer are updated as new figures are released.
Active surveillance vs. treatment: how to choose
For many men with low-risk prostate cancer, the most important decision is not which treatment to choose but whether to treat at all right now — and getting this decision right can spare you side effects you may never have needed.
What active surveillance actually means
Active surveillance is a deliberate, structured plan to monitor a low-risk cancer closely and treat it only if it shows signs of progressing. It is not ignoring the cancer, and it is not giving up.
A typical surveillance program includes regular PSA tests, periodic MRI, repeat biopsies on a schedule, and clear triggers — a rising grade, a growing lesion — that would prompt a switch to treatment. The goal is to delay or avoid the side effects of surgery and radiation in men whose cancer may never need either.
Who’s a candidate for surveillance
Surveillance is most appropriate for men with low-risk disease — typically Grade Group 1, a contained tumor, and a modest PSA — and for some men with favorable-intermediate-risk disease. Life expectancy and personal preference both factor in.
The overtreatment problem in plain terms
This is the issue that defines modern prostate cancer care. Because PSA testing finds many slow-growing cancers, treating every one of them aggressively would expose large numbers of men to incontinence and erectile dysfunction to cure a cancer that would never have harmed them.
🩺 Physician Note: The mistake I most want men to avoid is rushing to surgery or radiation out of fear the week they hear the word “cancer.” For a Grade Group 1 cancer, active surveillance is not the cautious option — it is often the standard of care, and choosing it does not mean you are gambling with your life. The men who regret their decision are far more often those who were treated unnecessarily than those who were carefully monitored.
Questions that should drive your decision
A good decision rests on a handful of honest questions, not on fear:
- What is my exact Grade Group, and is my cancer low or favorable-intermediate risk?
- What is my life expectancy, and how does that change the math?
- How would the side effects of treatment affect the life I actually want to live?
- What specifically would trigger a switch from surveillance to treatment?
- How anxious would monitoring make me, and can I live with that uncertainty?
Our complete guide to active surveillance for prostate cancer covers the typical monitoring schedule and the triggers for switching to treatment.
When watchful waiting is different from surveillance
These two terms are often confused, and the difference is real. Active surveillance is curative-intent monitoring for men healthy enough for treatment later, with the plan to act if the cancer progresses.
Watchful waiting is a less intensive approach, generally for older men or those with limited life expectancy, where the aim is to manage symptoms if they arise rather than to cure the cancer. Mixing them up can lead to either over- or under-treatment.
✅ Patient Action: Before choosing treatment for low-risk or favorable-intermediate-risk disease, ask a urologic oncologist: “Do I qualify for active surveillance, and what is my specific risk of the cancer progressing on surveillance compared with treating it now?”
Treatment options: surgery, radiation, and hormones
When treatment is the right path, the main options control the cancer comparably well for localized disease but differ sharply in their side effects — and that difference is where your decision should focus.
A side-by-side look at the main options
| Treatment | Best for | Main side effects | Key clinical detail |
|---|---|---|---|
| Radical prostatectomy | Localized cancer; younger, healthier men | Early urinary incontinence; erectile dysfunction | Side effects appear early, often improve over months |
| External beam radiation | Localized or locally advanced; men avoiding surgery | Urinary/bowel irritation; later erectile dysfunction | Side effects tend to appear later, build gradually |
| Brachytherapy | Low/favorable-intermediate risk | Urinary symptoms; erectile dysfunction | Radioactive seeds placed directly in the prostate |
| SBRT | Selected localized cancer | Similar to other radiation, fewer sessions | Delivered in about 5 high-dose sessions |
| Hormone therapy (ADT) | Added to radiation in higher-risk; advanced disease | Hot flashes, fatigue, bone loss, libido loss | Lowers testosterone to slow cancer growth |
Surgery (radical prostatectomy): what to expect
A radical prostatectomy removes the entire prostate gland, most often today using a robotic prostatectomy approach that allows precise, minimally invasive surgery. When the cancer’s location allows, surgeons use nerve-sparing technique to preserve the nerves responsible for erections.
The honest tradeoff is timing. Urinary incontinence and erectile dysfunction are common in the early weeks and months after surgery, then improve for many men over the following year, though recovery varies and is not guaranteed.
See our detailed guide on what to expect from prostate surgery, including nerve-sparing technique and the realistic recovery timeline.
Radiation therapy: external beam, brachytherapy, and SBRT
Radiation controls localized prostate cancer as effectively as surgery for many men, with a different side-effect pattern. External beam radiation therapy (EBRT) directs precisely targeted beams at the prostate over several weeks, while brachytherapy places radioactive seeds directly inside the gland.
Stereotactic body radiotherapy (SBRT) delivers a higher dose in about five sessions instead of many, a convenience that suits selected men. Radiation’s side effects — urinary and bowel irritation, and erectile dysfunction — tend to emerge later than surgery’s rather than immediately.
Our overview of radiation options for prostate cancer compares EBRT, brachytherapy, and SBRT schedules in detail.
Hormone therapy (ADT) and when it’s added
Androgen deprivation therapy (ADT) is not usually a standalone cure for localized disease but is often added to radiation for higher-risk cancer and is central to treating advanced disease.
🔬 How It Works: Prostate cancer cells usually depend on male hormones (androgens), especially testosterone, to grow. Androgen deprivation therapy lowers testosterone to very low levels — through injections or, increasingly, oral medication — effectively starving the cancer of the fuel it needs. This slows the cancer but also produces testosterone-loss effects like hot flashes, fatigue, and bone thinning, which is why it is used deliberately rather than casually.
Getting a second opinion before you decide
One quiet fact shapes many men’s treatment choices: the recommendation often depends on which specialist they happen to see first. A surgeon tends to recommend surgery; a radiation oncologist tends to recommend radiation.
That is not cynicism — it reflects genuine clinical equipoise for localized disease. It is also the strongest argument for hearing from more than one specialty before deciding.
✅ Patient Action: Ask both a urologic surgeon and a radiation oncologist for their recommendation before you decide, since each specialty’s default differs and a second-specialty opinion changes the plan for many men. A multidisciplinary clinic, where specialists confer together, is worth seeking out if one is available to you.
Treating advanced and metastatic prostate cancer
If prostate cancer has spread, the landscape of treatment has expanded substantially in the past few years, and which therapy fits depends on the precise state of the disease.
Hormone-sensitive vs. castration-resistant disease
Advanced prostate cancer is described by whether it still responds to hormone therapy. Metastatic hormone-sensitive prostate cancer (mCSPC) still responds to lowering testosterone, while castration-resistant prostate cancer (mCRPC) has learned to grow despite very low testosterone.
This distinction drives every treatment decision in advanced disease, because the two states call for different drugs.
Androgen receptor inhibitors and chemotherapy
Treatment of advanced disease almost always starts with an ADT backbone, to which other agents are added. Androgen receptor pathway inhibitors — including abiraterone (with prednisone), enzalutamide, darolutamide, and apalutamide — block the androgen signal more completely and are now used early, often alongside ADT from the start.
When more intensive treatment is needed, chemotherapy with docetaxel, and later cabazitaxel, remains an important option, sometimes combined with ADT and an androgen receptor inhibitor as part of “doublet” or “triplet” therapy.
PARP inhibitors and why genetic testing matters
For men whose cancer carries certain DNA-repair mutations, a targeted class of drugs has changed the options. PARP inhibitors such as olaparib, rucaparib, and niraparib are effective specifically in cancers with BRCA or other HRR mutations.
📊 Clinical Data Point: In December 2025, the FDA approved niraparib in combination with abiraterone acetate and prednisone for BRCA2-mutated metastatic castration-sensitive prostate cancer (U.S. Food and Drug Administration, December 2025). This is one reason germline and tumor genomic testing now directly determines which treatments are available to a given patient.
🔬 How It Works: Cancer cells with a BRCA or HRR mutation have already lost one of their DNA-repair tools. PARP inhibitors block another repair pathway those cells rely on, so the cancer cell accumulates unrepairable DNA damage and dies, while normal cells with intact repair are largely spared. This is why these drugs work in mutation-carrying cancers and not in others — and why testing comes first.
PSMA-targeted radioligand therapy
A newer form of treatment delivers radiation directly to prostate cancer cells wherever they are in the body. Lutetium-177-PSMA-617 is a radioligand that binds to PSMA on prostate cancer cells and delivers targeted radiation, used for PSMA-positive mCRPC.
📊 Clinical Data Point: Lutetium-177-PSMA-617 (marketed as Pluvicto) was first FDA-approved in 2022 for PSMA-positive metastatic castration-resistant prostate cancer after prior therapy, and in March 2025 the FDA expanded its approval to an earlier line of treatment, before chemotherapy (U.S. Food and Drug Administration, 2022 and March 2025). Eligibility is confirmed with a PSMA-PET scan.
Immunotherapy and clinical trials
Immunotherapy plays a narrower role in prostate cancer than in some other cancers, but it matters for specific patients. Sipuleucel-T is a cellular immunotherapy for certain men with advanced disease, and pembrolizumab can help the small subset of cancers with high microsatellite instability or mismatch-repair deficiency.
Clinical trials are also a legitimate and sometimes preferable option in advanced disease, not a last resort. Our in-depth guide to treating advanced prostate cancer covers therapy sequencing and side-effect management.
✅ Patient Action: Ask a genitourinary medical oncologist: “Should I have germline and tumor genomic testing, including BRCA1, BRCA2, and other HRR genes?” — because the results determine your eligibility for PARP inhibitors and for certain clinical trials.
Side effects and life after treatment
The effects of prostate cancer treatment on urination and sexual function are the part many men quietly worry about most, and they deserve frank discussion rather than euphemism.
Urinary incontinence: what to expect and how it’s managed
Urinary incontinence is most common in the early period after surgery, when leakage with coughing, lifting, or exertion is typical, and it improves for many men over the following months. Radiation more often causes urinary urgency and irritation than leakage, and these can appear later.
Recovery is active, not passive. Pelvic-floor muscle training — ideally started before surgery — improves continence outcomes, and a range of further options exists for men whose leakage persists.
Erectile dysfunction and sexual recovery
Erectile dysfunction is common after both surgery and radiation, with the timing differing: it often appears immediately after surgery and more gradually after radiation. Nerve-sparing surgery improves the odds of recovery, but outcomes depend on age, baseline function, and the cancer’s location.
🔬 How It Works: Erections depend on the nerves that run alongside the prostate. Surgery can bruise or remove these nerves, and radiation can damage the blood vessels and nerves over time, which is why erectile function may dip and then partially recover as nerves heal. Penile rehabilitation — using PDE5 inhibitor medications and other aids early — aims to keep blood flowing to the tissue while nerves recover, improving long-term results.
Bowel, fatigue, and hormone-therapy effects
Radiation can cause bowel urgency or irritation, usually temporary. Hormone therapy carries its own distinct set of effects — hot flashes, fatigue, loss of libido, bone thinning, and metabolic changes — that warrant proactive management, including bone-density monitoring and exercise.
Rehabilitation and getting your life back
The men who recover function best are generally those who start rehabilitation early and treat it as part of the treatment plan, not an afterthought. Pelvic-floor therapy, sexual-medicine support, exercise, and honest conversations with a partner all play a role.
Our full guide on managing incontinence and ED after treatment covers pelvic-floor therapy, devices, and medication options in depth.
✅ Patient Action: Ask for a referral to pelvic-floor physical therapy, and — if sexual function matters to you — to a sexual-medicine specialist, before treatment begins rather than after symptoms set in, because early rehabilitation measurably improves recovery.
What a urologic oncologist wants men to know
Stepping back from the details, a few clinical truths change outcomes more than almost anything else a man will read.
The mistakes that lead to overtreatment
The most common and most consequential error is treating low-risk disease aggressively out of fear. A Grade Group 1 cancer caught on screening is rarely an emergency, and the rush to “just get it out” leaves some men with lifelong side effects they did not need.
🩺 Physician Note: In practice, the men who do best are the ones who slow down for two or three weeks, get their full risk picture in writing, and make a deliberate decision rather than a frightened one. Almost no low-risk prostate cancer becomes dangerous in the month it takes to get a second opinion. The clock you feel ticking is usually fear, not biology.
Why a second opinion is standard, not distrust
Seeking a second opinion is not an insult to your doctor; in cancer care it is routine and expected. Different specialties genuinely favor different approaches for the same localized cancer, and hearing more than one perspective is how you find the path that fits your life.
What to bring to your first specialist appointment
Walking in prepared changes the quality of the conversation entirely. Bring your PSA history, your Gleason score and Grade Group, your clinical stage, and a written list of questions.
✅ Patient Action: At your first specialist visit, bring your PSA, Grade Group, and stage in writing, and ask the specialist directly: “If I were a close member of your family with exactly this profile, which option would you choose, and why?”
Frequently asked questions about prostate cancer
1. Can prostate cancer be cured?
Yes, prostate cancer is often curable, especially when caught early. For localized and regional disease confined to or near the prostate, the 5-year relative survival rate approaches 100%, and surgery or radiation can be curative. Even advanced, metastatic prostate cancer can often be controlled for years with modern therapies, though it is harder to cure. Discuss your specific stage and grade with a urologic oncologist before making treatment decisions.
2. Is prostate cancer slow-growing?
Many prostate cancers are slow-growing and may never threaten a man’s life, which is why active surveillance exists for low-risk disease. A minority, however, are aggressive and spread early. Your Grade Group is the best indicator: Grade Group 1 cancers are typically slow, while Grade Group 4 and 5 cancers grow and spread faster. Ask your urologist how your specific Grade Group affects how urgently your prostate cancer needs treatment.
3. At what age should I start PSA testing?
Guidelines frame PSA testing as a shared decision rather than an automatic test. The American Cancer Society suggests discussing it at age 50 for average-risk men, 45 for higher-risk men including Black men and those with a close relative diagnosed before 65, and 40 for men at highest risk. The USPSTF supports an individual decision for men aged 55 to 69. Discuss your personal screening timing with your primary care physician.
4. What is a dangerous PSA level?
There is no single PSA level that confirms prostate cancer or rules it out, because risk rises gradually as PSA increases. A level under 4 ng/mL was once treated as reassuring, but cancer can occur below it and many men above it have no cancer. Doctors weigh your PSA trend, PSA density, free-to-total ratio, age, and risk factors together. Ask your urologist to interpret your PSA in the context of your full risk profile.
5. Can you have prostate cancer with a normal PSA?
Yes. A normal PSA lowers the probability of significant prostate cancer but does not eliminate it, which is why a digital rectal exam and your risk factors still matter. Some cancers, including some aggressive ones, produce less PSA than expected. A reassuring number is not a reason to ignore new urinary symptoms, bone pain, or a strong family history. Raise any persistent symptoms with your doctor regardless of a normal PSA result.
6. What is the difference between surgery and radiation?
For localized prostate cancer, surgery (radical prostatectomy) and radiation control the cancer comparably well, but their side effects differ in type and timing. Surgery tends to cause earlier urinary incontinence and erectile dysfunction that may improve over a year, while radiation more often causes later urinary and bowel irritation. The right choice depends on your age, health, and priorities. Consult both a urologic surgeon and a radiation oncologist before deciding.
7. Does prostate cancer always need treatment?
No. For low-risk prostate cancer, particularly Grade Group 1, active surveillance — close monitoring with PSA, MRI, and repeat biopsies — is often the standard of care, with treatment started only if the cancer progresses. This approach spares many men the side effects of surgery and radiation they may never have needed. Whether surveillance fits depends on your grade, life expectancy, and preferences. Ask a urologic oncologist whether you qualify for active surveillance.
8. What are the first symptoms of prostate cancer?
Early prostate cancer usually causes no symptoms at all, because most tumors begin in the outer part of the prostate, away from the urethra. When symptoms do occur, they often reflect a benign enlarged prostate rather than cancer, and include a weak stream, frequent urination, or trouble starting. Advanced disease may cause bone pain or blood in the urine. See a urologist promptly if you notice blood in urine or semen, or new persistent bone pain.
9. How fast does prostate cancer spread?
The speed varies enormously and depends mainly on the cancer’s grade. Low-grade (Grade Group 1) cancers may grow so slowly they never spread within a man’s lifetime, while high-grade (Grade Group 4 or 5) cancers can spread to lymph nodes and bone much faster. PSA trends and imaging help track the pace. Ask your urologic oncologist what your Grade Group and PSA suggest about your cancer’s likely behavior before choosing a treatment timeline.
10. Does prostate cancer run in families?
Yes. Having a father or brother with prostate cancer roughly doubles a man’s risk, and the risk rises further with more affected relatives or relatives diagnosed young. Inherited mutations in BRCA1, BRCA2, and related HRR genes raise risk and can make the disease more aggressive. A family history of breast, ovarian, or pancreatic cancer is also relevant. Ask your doctor whether you meet criteria for germline genetic testing and genetic counseling.
11. What is a PSMA-PET scan?
A PSMA-PET scan is an imaging test that uses a tracer binding to prostate-specific membrane antigen, a protein on prostate cancer cells, to reveal disease with greater accuracy than traditional CT or bone scans. It is used mainly to stage higher-risk cancer and to detect spread when PSA rises after treatment. It also confirms eligibility for PSMA-targeted therapy. Ask your urologic oncologist whether a PSMA-PET scan is appropriate for your stage and risk level.
12. What is castration-resistant prostate cancer?
Castration-resistant prostate cancer (mCRPC) is advanced disease that continues to grow despite hormone therapy having lowered testosterone to very low levels. It does not mean treatment has failed — several effective options remain, including androgen receptor inhibitors, chemotherapy, PARP inhibitors for certain mutations, and PSMA-targeted radioligand therapy.
Genomic testing helps match the right drug to your cancer. Discuss the full sequence of available treatments with a genitourinary medical oncologist experienced in advanced prostate cancer.
13. Can diet or lifestyle lower my risk?
A heart-healthy pattern — rich in vegetables and whole foods, with limited processed and red meat — supports overall health and may modestly affect prostate cancer risk, alongside regular exercise and not smoking. The evidence for specific foods is weak, and dietary supplements have not been shown to prevent prostate cancer; some, including high-dose vitamin E, have shown potential harm in trials. Focus on overall lifestyle rather than supplements, and discuss any supplement with your doctor first.
14. What is the survival rate for advanced prostate cancer?
For distant-stage (metastatic) prostate cancer, the 5-year relative survival rate is about 37%, far lower than the near-100% rate for localized disease. This figure describes a group and not any individual, and it predates many recent treatment advances that have extended survival for men with advanced disease. Outcomes vary widely by genetics, treatment response, and overall health. Ask a genitourinary medical oncologist what current treatment options mean for your specific situation.
15. How often is monitoring done on active surveillance?
Active surveillance schedules vary but typically include a PSA blood test every few months, a digital rectal exam periodically, an MRI on a regular interval, and a repeat biopsy at defined points. The aim is to detect any sign that the cancer is becoming more aggressive early enough to treat it with curative intent. Specific timing depends on your risk category and program. Ask your urologic oncologist what monitoring schedule and progression triggers apply to your case.
Your next steps after a prostate cancer diagnosis
If you have read this far, you likely understand your situation better than you did an hour ago, and that understanding is itself a kind of footing.
A prostate cancer diagnosis is frightening, but for most men it is not the emergency it first feels like, and you have more time to decide well than the fear suggests. The decisions ahead — whether to screen, whether to monitor or treat, which treatment fits the life you want — are real, but they are decisions you can make deliberately, with specialists who are on your side.
The one thing to do before your next appointment
The single most valuable thing you can do is walk into your next appointment prepared. Write down your PSA, your Gleason score and Grade Group, and your clinical stage, and bring a short list of questions — starting with whether active surveillance is an option for you.
To make that easier, you can download our prostate cancer appointment question list and “know your numbers” sheet, a one-page resource that organizes exactly what to bring and what to ask your specialist.
Where to go deeper
Depending on where you are, three places to read next will serve you best. If you are deciding whether to treat, return to the active surveillance guide linked earlier in this article. If you are comparing how to treat, the radiation options overview and the survival-rates breakdown linked in the sections above will give you the fullest picture.
✅ Patient Action: Before your next appointment, write down your PSA, Grade Group, and stage, and bring three questions — beginning with: “Am I a candidate for active surveillance, and if not, why not?”
The clinical information in this article is grounded in current guidance from the FDA, the National Cancer Institute and its SEER program, the CDC, the American Cancer Society, and the American Urological Association, and is reviewed by board-certified specialists on the mymedicineadvisor.com medical advisory board. Sourcing is dated to the most current guidelines and data available, so that what you read reflects how prostate cancer is actually understood and treated today.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.