On This Page – Quick Medical Summary
If a relative recently tested positive for a BRCA mutation, or your doctor raised genetic testing after a prostate cancer diagnosis, you may be carrying a quiet worry: is this in my genes, and did I pass it on? BRCA is known mainly as a breast cancer gene — but it matters for men too, and BRCA2 in particular is strongly tied to prostate cancer.
Where you are now shapes what you need. If a family member carries a mutation and you want your own risk, start with the risk and testing-eligibility sections. If you were recently diagnosed, the testing and treatment sections are for you. If you are supporting someone, the section on inherited risk will help most.
A BRCA result is not a verdict. This guide sits alongside our overview of how prostate cancer is staged and treated, and knowing your genetic status is one of the most useful steps you can take.
ℹ️ Medical Disclaimer: This article is educational and does not provide a diagnosis, treatment plan, medication guidance, or genetic-risk determination for any individual. Decisions about genetic testing, screening, medications such as PARP inhibitors, and prostate cancer treatment should be made with a board-certified urologist, medical oncologist, or certified genetic counselor who knows your personal and family history.
What BRCA1 and BRCA2 have to do with prostate cancer
A BRCA mutation does not directly cause prostate cancer, but it raises the risk because these genes normally help repair damaged DNA. When a BRCA gene is faulty, cells lose a key safeguard and cancer-driving errors can accumulate.
What BRCA genes normally do
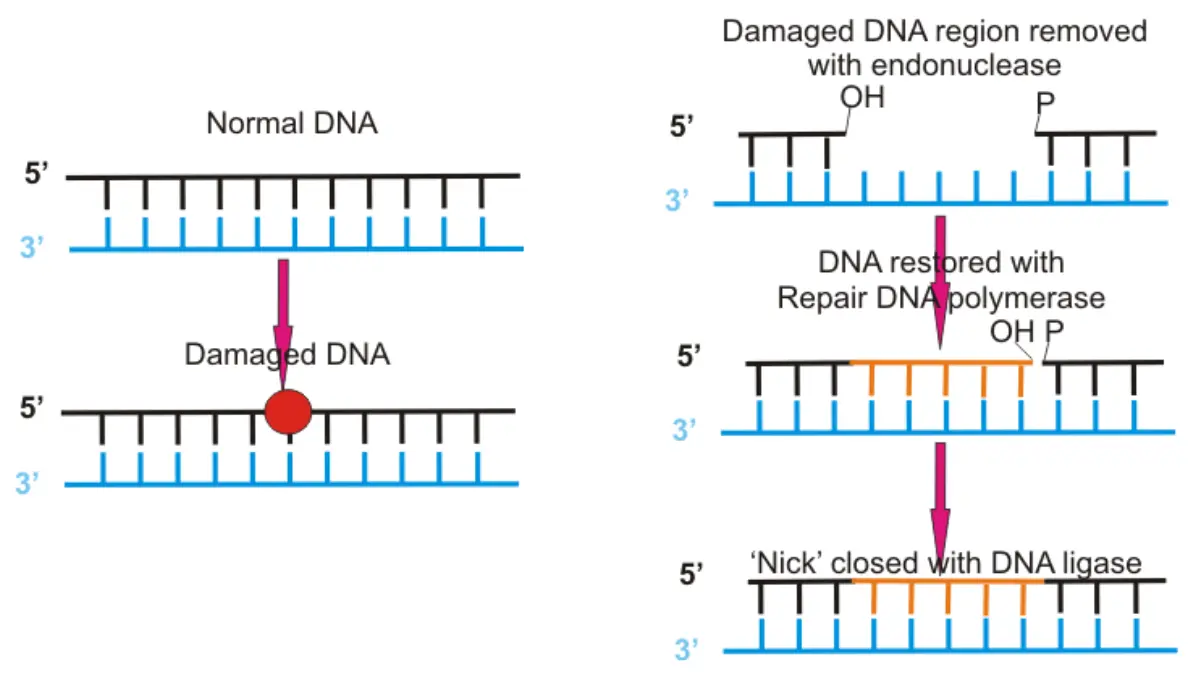
BRCA1 and BRCA2 are tumor-suppressor genes — their job is to fix breaks in DNA before those errors reach new cells. You can read more about what the BRCA2 gene normally does from MedlinePlus Genetics.
🔬 How It Works: Cells repair broken DNA through a high-accuracy process called homologous recombination, and BRCA2 helps run it. Without working BRCA2, the cell falls back on error-prone repair, and cancer-driving mistakes accumulate.
How a mutation raises risk, and why BRCA2 matters more
An inherited, or germline mutation, means every cell starts with one weakened copy of the gene, making it likelier a cell turns cancerous. It does not guarantee cancer, but it shifts the odds and can affect how a cancer behaves. Both genes raise risk, but BRCA2 carries the stronger signal and is more often linked to aggressive disease, which is why it sits at the center of prostate cancer genetics guidance alongside other prostate cancer risk factors.
How much do BRCA mutations raise prostate cancer risk?
Estimates vary by study and population, but men with a BRCA2 mutation face a substantially higher lifetime risk than average — research summaries cite roughly 4.7 to 8.6 times the risk in some carrier cohorts, with lifetime estimates reported as high as around 60% in certain prospective studies. The average man’s lifetime risk is about 1 in 8. These are population figures, not a personal prediction.
📊 Clinical Data Point: Among 692 men with metastatic prostate cancer, 11.8% carried an inherited DNA-repair mutation — versus 4.6% with localized disease and 2.7% of the general population — and BRCA2 was the most common. — Source: Pritchard et al., NEJM, 2016.
BRCA2 and BRCA1 risk, by the numbers
Treat every figure below as an estimate that shifts with study design and family history.
| Group | Estimated lifetime prostate cancer risk | Key clinical detail |
|---|---|---|
| General-population men | About 13% (roughly 1 in 8) | Baseline risk |
| BRCA1 carriers | Around 29% in some prospective data | Smaller increase than BRCA2 |
| BRCA2 carriers | Up to ~60% | Strongest hereditary link; often aggressive |
Source: synthesized from the National Cancer Institute and peer-reviewed cohort studies (JNCI; NEJM); estimates vary by study and population. See the National Cancer Institute’s prostate cancer genetics summary for a clinician-level overview.
Is BRCA prostate cancer more aggressive?
BRCA2-related prostate cancer tends to behave more aggressively, with higher rates of a pattern called intraductal carcinoma. In carriers whose disease progresses to advanced, metastatic and castration-resistant stages, some studies report 5-year cancer-specific survival around 50% to 60% — reflecting specific study populations, not an individual forecast.
✅ Patient Action: If you have prostate cancer, ask your oncologist or urologist whether you qualify for both germline and tumor (somatic) testing — they answer different questions.
Who should get genetic testing for prostate cancer?
Current NCCN guidelines recommend germline genetic testing for many men with prostate cancer, not only those with advanced disease. Testing is generally recommended if you have:
- High-risk, very-high-risk, regional, or metastatic prostate cancer — regardless of family history
- Ashkenazi Jewish ancestry
- A personal history of breast cancer
- A qualifying family history (close relatives with breast, ovarian, pancreatic, or prostate cancer)
📊 Clinical Data Point: About 50% of men with prostate cancer meet NCCN criteria for germline testing at diagnosis. — Source: Xu et al., The Prostate, 2025.
NCCN criteria and which genes are tested
If your cancer is classified as high-risk or very-high-risk disease — based on stage, grade, or PSA level — testing is recommended even with no family history. Modern panels look beyond BRCA, typically including BRCA1, BRCA2, ATM, CHEK2, PALB2, HOXB13, and the Lynch-syndrome genes MLH1, MSH2, MSH6, and PMS2. Before a clinical visit, you can estimate your hereditary risk profile — though this is educational only, not a diagnostic test.
🩺 Physician Note: Current guidance reflects a major shift. Germline testing was once reserved for late-stage or strongly familial cases; today, roughly half of men with prostate cancer qualify at diagnosis, because a result can change both treatment and family screening.
How BRCA genetic testing works, step by step
There are two different tests that answer different questions. Germline testing checks the DNA you inherited, using a blood or saliva sample; tumor (somatic) testing examines the cancer itself for mutations it acquired.
Germline vs. tumor testing
Germline testing tells you whether a mutation runs in your family and could pass to children. Tumor (somatic) testing tells you about the cancer in front of you and can guide treatment. A tumor finding in a gene like BRCA may actually be inherited — which is why it sometimes prompts a confirmatory germline test.
The process, and why counseling comes first
The steps are simple: a pre-test conversation, a blood draw or saliva sample, lab analysis, and a results appointment over a few weeks. Guidelines recommend meeting a genetic counselor before and after testing. Disclosure: some companies offer clinician-ordered or at-home genetic panels; these are not a substitute for guideline-directed testing and counseling arranged through your medical team.
✅ Patient Action: Ask your care team whether you should have both germline and tumor testing — and whether any tumor finding in a gene like BRCA needs a confirmatory germline test for your family.
What a BRCA mutation means for prostate cancer treatment
For advanced disease, a BRCA or related DNA-repair mutation can open targeted options that would not otherwise apply. The clearest example is a class of drugs called PARP inhibitors.
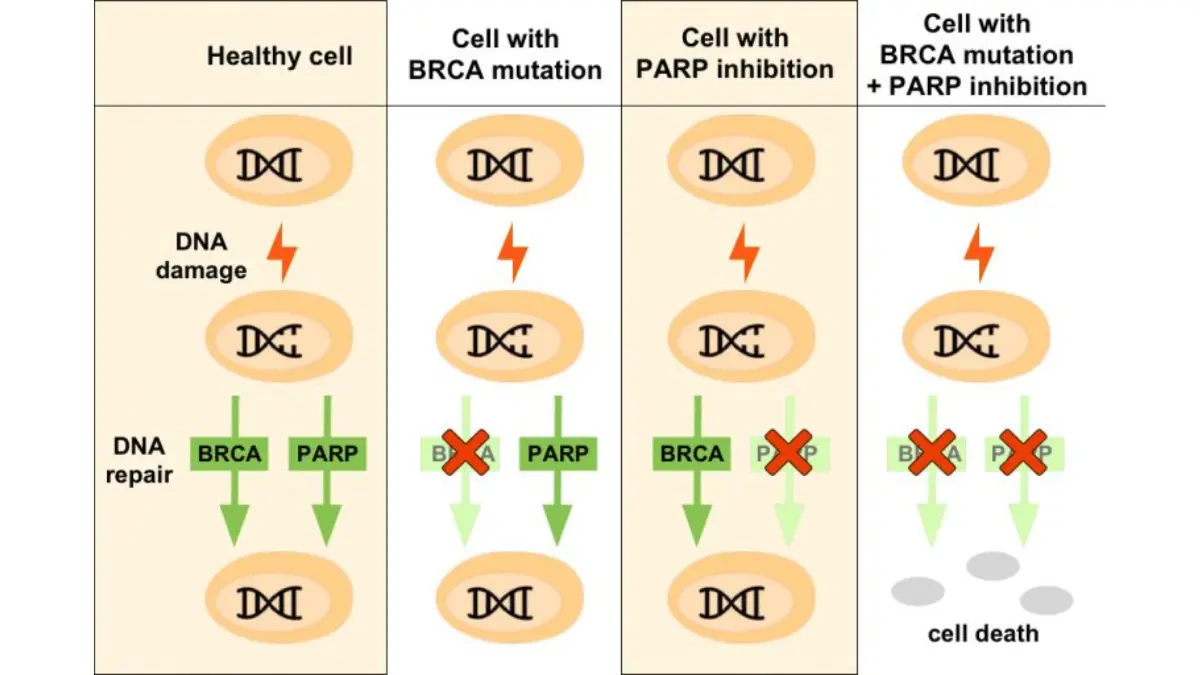
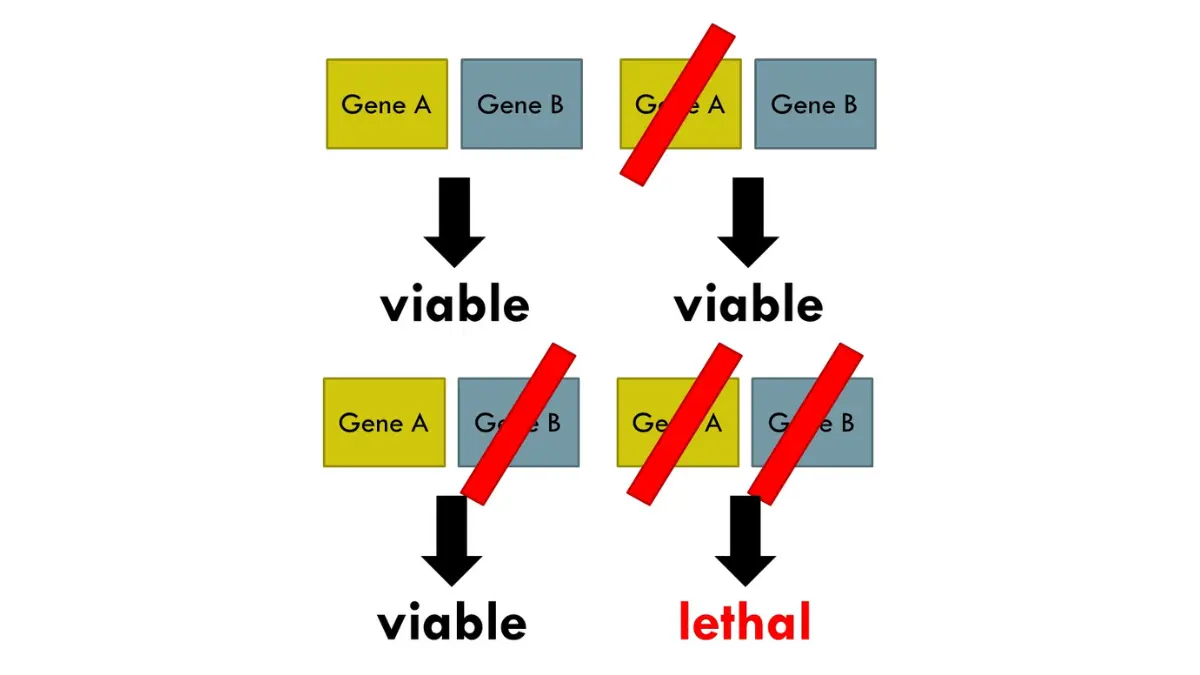
🔬 How It Works: Cancer cells with a broken BRCA gene already struggle to repair DNA. PARP inhibitors block a second repair pathway, so these cells die while healthy cells, which still repair normally, are largely spared. This is called synthetic lethality.
The FDA-approved options, in brief
Two PARP inhibitors are approved as single agents for metastatic castration-resistant prostate cancer: olaparib (Lynparza) and rucaparib (Rubraca), both approved in 2020 for advanced disease after prior hormone-pathway therapy. In 2023, combinations pairing a PARP inhibitor with androgen receptor pathway therapy were approved as first-line options, and BRCA-altered tumors may also respond to platinum-based chemotherapy. See the FDA’s approval for olaparib in prostate cancer and our closer look at PARP inhibitors.
⚠️ Clinical Warning: PARP inhibitors carry real risks — common side effects include significant anemia and fatigue, and rarely they can contribute to serious blood disorders. They require ongoing monitoring and must be prescribed and managed by an oncology specialist.
Why testing can change the plan
Because these options depend on knowing your mutation status, testing is not academic — it can directly shape which treatments are available. For early, localized cancer, treatment is still guided mainly by stage and grade.
✅ Patient Action: If you have advanced prostate cancer, ask your medical oncologist whether your tumor and germline DNA have been tested for BRCA and DNA-repair mutations, and whether a PARP inhibitor or platinum chemotherapy could fit your case.
What a positive result means for your family
BRCA mutations are inherited in an autosomal dominant pattern, which means each of your children — sons and daughters — has a 50% chance of inheriting the same mutation. Men and women can both carry it and pass it on.
Inheritance and cascade testing
A 50% chance applies to each child independently; a positive result does not mean a relative will develop cancer, but it flags a risk worth acting on. When one family member tests positive, relatives can pursue cascade testing — targeted testing for that specific mutation, which is faster and clearer than a broad panel. Talking with relatives about a genetic result is something a genetic counselor can help you navigate.
Earlier screening for male carriers
Male carriers, especially with BRCA2, may be advised to begin PSA screening earlier than the general population, because targeted screening tends to catch more clinically significant cancers in carriers. The right timing depends on the mutation and family history; our guide to earlier PSA screening for higher-risk men explains the approach.
✅ Patient Action: Ask a genetic counselor which relatives should consider testing, and ask your urologist at what age at-risk men in your family should begin PSA screening.
BRCA and prostate cancer: frequently asked questions
1. Does having a BRCA mutation mean I’ll definitely get prostate cancer?
No. A BRCA mutation raises risk — substantially for BRCA2 carriers — but it is not a certainty, and many carriers never develop prostate cancer. The lifetime-risk figures are population averages. A certified genetic counselor can put your personal risk in context.
2. Is BRCA2 worse than BRCA1 for prostate cancer?
Generally, yes. BRCA2 carries the stronger link and is more often tied to aggressive disease, while BRCA1’s effect is real but smaller. BRCA2 is also the most common inherited DNA-repair mutation in men with metastatic disease. Your oncologist can explain your result.
3. How much does a BRCA mutation increase prostate cancer risk?
Estimates vary widely. Against an average lifetime risk of about 1 in 8, some carrier cohorts show roughly 4.7 to 8.6 times the risk for BRCA2, with lifetime estimates up to around 60%. These are population statistics — discuss your own numbers with a genetic counselor.
4. Who qualifies for prostate cancer genetic testing?
Guidelines recommend germline testing for men with high-risk, very-high-risk, regional, or metastatic disease regardless of family history, plus those with Ashkenazi Jewish ancestry, a breast cancer history, or qualifying family history. About half of patients qualify at diagnosis. A urologist, oncologist, or genetic counselor can confirm eligibility.
5. What’s the difference between germline and tumor testing?
Germline testing checks inherited DNA, via blood or saliva, and shows whether a mutation runs in your family. Tumor (somatic) testing examines the cancer for mutations it acquired. A BRCA prostate cancer genetic testing plan often uses both. Ask your care team which you need.
6. How is BRCA genetic testing actually done?
Germline testing usually requires a simple blood draw or saliva sample, with genetic counseling recommended before and after. Tumor testing uses a sample of the cancer tissue. Your medical team or a genetic counselor arranges the right test for you.
7. Does a BRCA mutation change how prostate cancer is treated?
For advanced disease, yes. A BRCA or related DNA-repair mutation can make a tumor eligible for PARP inhibitors, and BRCA tumors may respond to platinum chemotherapy. For early, localized cancer, treatment follows stage and grade. A medical oncologist determines what fits your case.
8. What are PARP inhibitors and who can take them?
PARP inhibitors are targeted drugs that exploit a cancer cell’s broken DNA-repair machinery. Olaparib and rucaparib are FDA-approved for metastatic castration-resistant prostate cancer with BRCA or related mutations. They carry meaningful side effects and are managed by an oncologist. Ask your specialist whether one applies.
9. If I carry a BRCA mutation, will my children inherit it?
Each child has a 50% chance of inheriting it, because BRCA mutations follow an autosomal dominant pattern. This applies to sons and daughters, and either parent can pass it on. A genetic counselor can guide which relatives to test first.
10. Should men with a BRCA mutation start PSA screening earlier?
Often, yes. Male BRCA carriers — especially BRCA2 — may be advised to begin PSA screening earlier, because targeted screening catches more clinically significant cancers in carriers. Timing depends on your mutation and family history. Ask your urologist or genetic counselor about a personalized schedule.
11. Can BRCA-related prostate cancer be prevented?
There is no proven way to prevent it in carriers, but knowing your status enables earlier, focused screening that can catch disease sooner, when it is most treatable. The most powerful step is a personalized screening plan built with your urologist and a genetic counselor.
The bottom line on BRCA and prostate cancer
Learning that a BRCA mutation runs in your family can feel like inheriting bad news you never asked for. But in practice, a result turns uncertainty into a plan — it can sharpen screening, open targeted treatments if cancer develops, and protect your relatives through their own testing.
If any testing criteria fit you, the next step is concrete: ask your urologist, oncologist, or a certified genetic counselor about germline and tumor testing. Knowing your status is one of the few genuinely empowering moves available in prostate cancer — for you, and for the people who share your genes.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.