On This Page – Quick Medical Summary
A rising PSA after prostate cancer treatment is one of survivorship’s most frightening moments. A single higher number, though, is a reason to look closer — not proof the cancer is back.
Where you go next depends on your situation. Just saw a higher PSA on a follow-up test? Section 3 explains what the number means and whether one reading confirms anything. A caregiver decoding a lab report? Sections 2 and 4 translate the terms and the risk. Recurrence already confirmed and weighing what’s next? Sections 5 and 6 cover imaging and treatment. No symptoms and just want to understand your follow-up? That’s the most common situation here.
Prostate cancer recurrence has a precise medical meaning, and grasping it is the difference between panic and a plan. Knowing how prostate cancer is staged and treated gives you the full picture behind everything below. This guide draws on current clinical sources — and shows its work.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice, and does not create a doctor–patient relationship. Decisions about interpreting your PSA results, ordering imaging such as a PSMA PET scan, and choosing salvage treatment (radiation, surgery, or hormone therapy) belong with a board-certified urologist or radiation/medical oncologist who knows your full history. Consult that specialist before acting on anything here.
What prostate cancer recurrence actually means
Recurrence means cancer activity has returned after treatment meant to cure it — but doctors split that into two very different situations.
Biochemical vs. clinical recurrence
Biochemical recurrence is a rising PSA in your blood with no symptoms and nothing visible on a scan. It is a laboratory finding — a signal that some prostate cancer cells may remain — not a confirmed diagnosis of spreading disease. Clinical recurrence is different: the cancer can actually be seen on imaging or is causing symptoms.
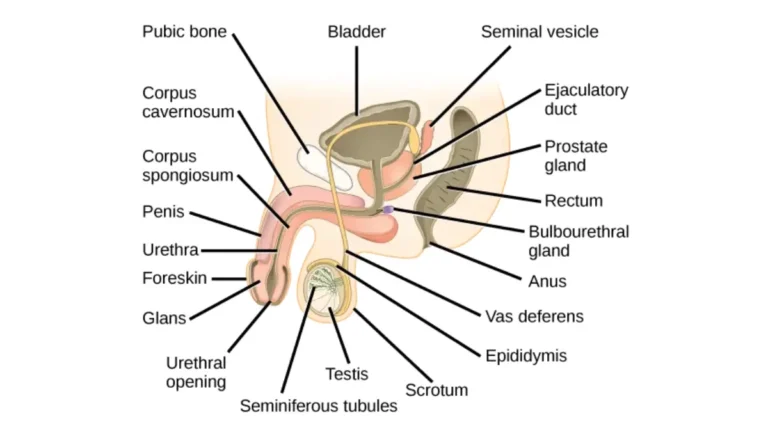
🔬 How It Works: PSA is a protein made almost entirely by prostate cells. After surgery removes the prostate, PSA should fall to undetectable; after radiation, it should drop to a low nadir — your lowest post-treatment level. A sustained climb suggests prostate cells, possibly cancerous, are active again.
Local, regional, and distant recurrence
Recurrence is also described by location. Local means cancer regrew near the original site, in the prostate bed. Regional means nearby lymph nodes, and distant (metastasis) means it has traveled to bone or other organs. Where it returns shapes nearly everything about what happens next.
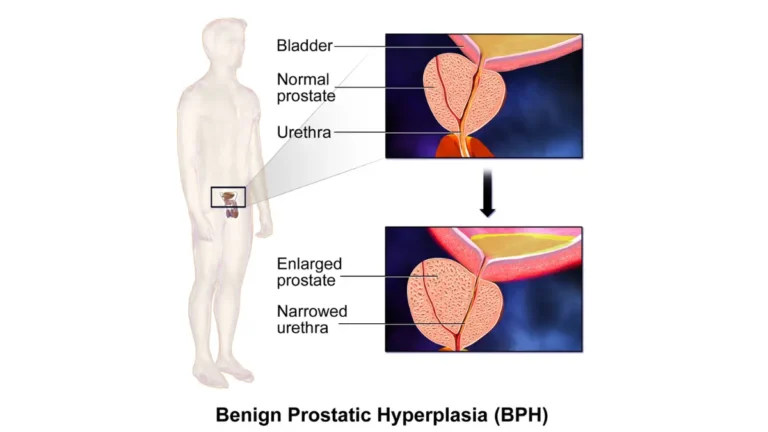
Warning signs: what a rising PSA does and doesn’t mean
For most men, the first and often only sign of recurrence is a rising PSA — not pain or other symptoms.
PSA thresholds after surgery vs. radiation
The number that defines recurrence depends on your original treatment.
📊 Clinical Data Point: After radical prostatectomy, recurrence is generally defined as a PSA of 0.2 ng/mL or higher, confirmed on two consecutive tests. After radiation therapy, it is a PSA that rises 2 ng/mL or more above your nadir. — Sources: American Urological Association recommendation; ASTRO-Phoenix consensus definition.
Some clinicians act on a lower post-surgery threshold, around 0.1 ng/mL, depending on your surgical pathology. For context on how PSA testing and levels work, it helps to know your post-treatment baseline.
Does one rising PSA mean cancer is back?
Not by itself. A confirmed recurrence requires a repeat test showing a sustained rise, because a single blip can reflect normal lab variation — a point the NCI’s overview of the PSA test underscores.
Physical symptoms to report
Symptoms usually appear only with advanced or distant disease. Tell your care team promptly about new bone pain, blood in the urine, or new trouble urinating. A quick symptom checker can help you decide whether something warrants a call, though it is not a diagnosis.
How likely is recurrence, and how to read your risk
Recurrence is common enough to plan for and uncommon enough that fear shouldn’t run the show.
How common is prostate cancer recurrence?
📊 Clinical Data Point: Roughly 20% to 40% of men develop biochemical recurrence within 10 years of surgery or radiation, with some estimates higher. — Source: peer-reviewed urology literature.
That figure describes a population, not your personal odds — and biochemical recurrence is a lab finding, not a prognosis. Many men with a slowly rising PSA never go on to develop symptoms. Your original Gleason score shapes how aggressive a recurrence is likely to be, along with your stage.
PSA doubling time: the number that matters most
How fast your PSA rises — its doubling time — tells doctors more than the single value. In research, a shorter doubling time, under roughly 6 to 9 months, has been linked to a higher risk of the cancer spreading; a slow rise over years is generally far less concerning.
✅ Patient Action: Ask your oncologist to calculate your PSA doubling time from your sequence of readings — it directly influences whether, and how quickly, treatment is recommended.
Next steps: how doctors locate a recurrence
Once a rising PSA is confirmed, the goal shifts to finding where the cancer is, because location drives treatment.
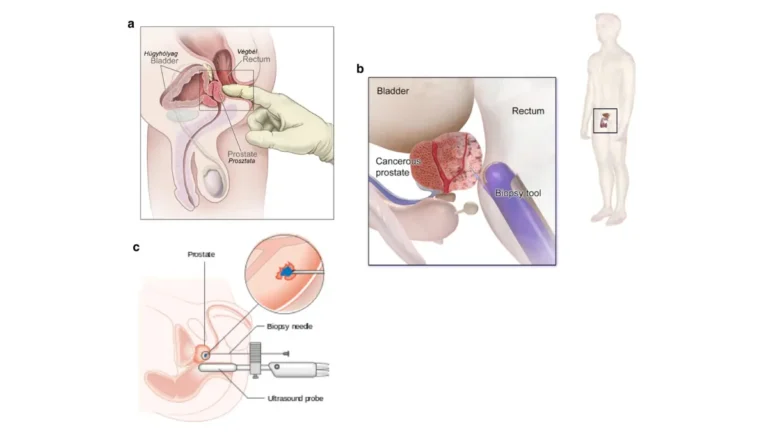
Confirming recurrence with repeat PSA and imaging
Doctors first confirm the trend with a repeat PSA, then turn to imaging to locate disease in the prostate bed, lymph nodes, or beyond.
PSMA PET scans and why they changed the picture
A PSMA PET scan is now central to this step.
🔬 How It Works: PSMA is a protein on the surface of more than 90% of prostate cancer cells. A PSMA-targeted imaging agent binds to it and lights up on a PET scan, revealing cancer that older CT or bone scans often miss.
The FDA approved the first such agent, piflufolastat F-18 (Pylarify), in May 2021 for suspected recurrence based on a rising PSA, and it can localize disease even at low PSA levels. Our guide on how a PSMA PET scan works covers what to expect.
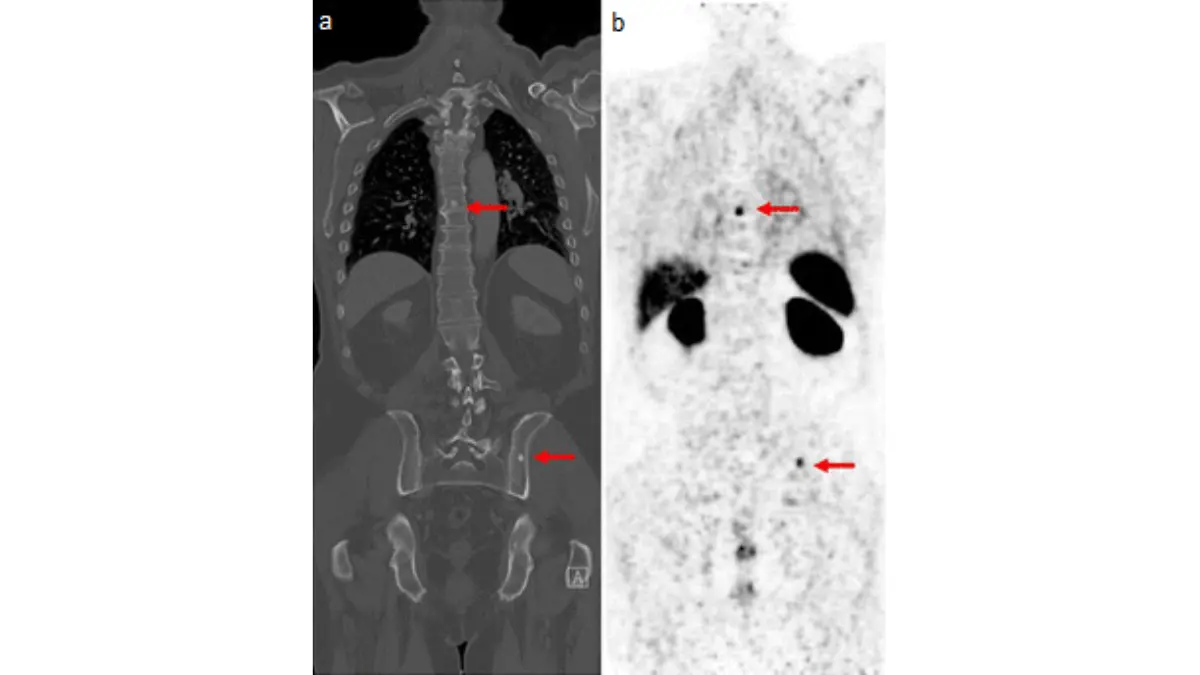
🩺 Physician Note: Current NCCN guidance recognizes PSMA PET for detecting recurrence after both surgery and radiation, and considers it more sensitive than conventional imaging at low PSA. This is why a low but rising PSA no longer means nothing can be done.
If a scan shows distant spread, your team may discuss treatment for more advanced, stage 4 disease.
Treatment options after recurrence
Effective options exist after recurrence, and which ones fit depends mostly on the treatment you already had.
If your first treatment was surgery
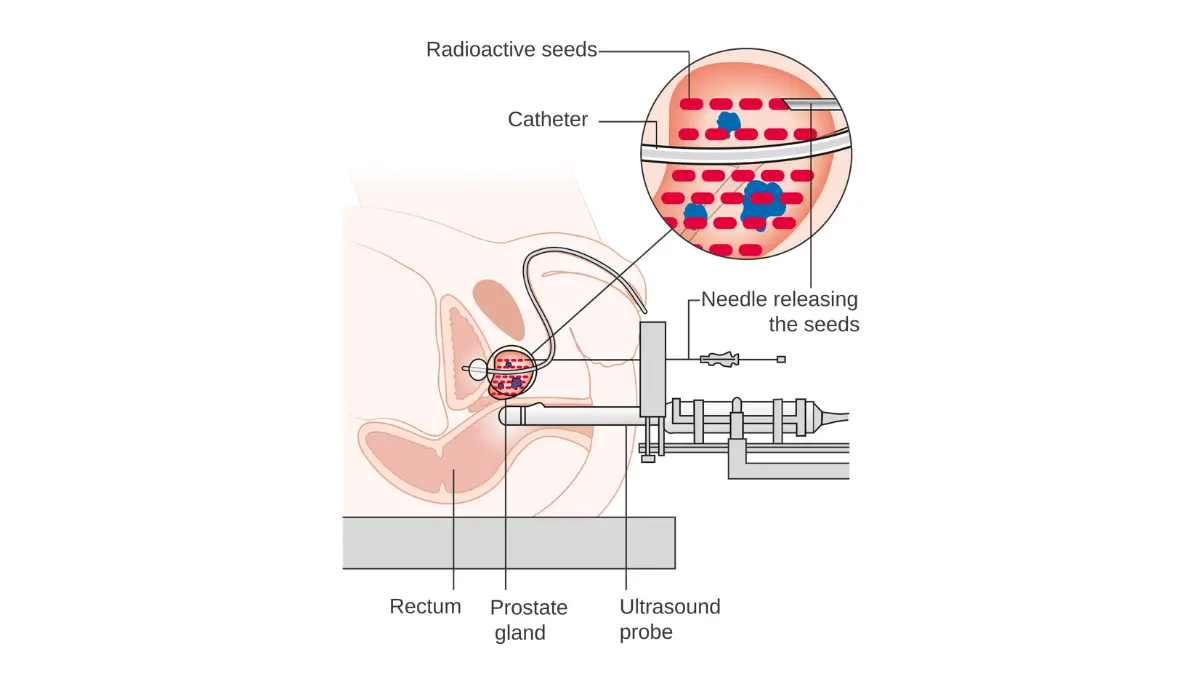
When cancer returns after prostatectomy, the most common next step is salvage radiation therapy to the prostate bed, sometimes combined with hormone therapy (androgen deprivation). For a biochemical-only recurrence with a slow rise, active surveillance is sometimes reasonable. The radiation therapy is most effective when started at a lower PSA.
If your first treatment was radiation
After radiation, options may include salvage surgery, cryotherapy, or high-intensity focused ultrasound.
⚠️ Clinical Warning: Salvage treatments done after radiation carry a meaningfully higher risk of side effects, such as urinary incontinence and erectile dysfunction, than the same procedures performed as a first treatment. This trade-off deserves a frank conversation before you decide.
When the cancer has spread
If imaging shows distant disease, treatment shifts toward systemic therapy — typically hormone therapy, with other agents layered in over time.
| Situation | Common options | Key clinical detail |
|---|---|---|
| Recurrence after surgery | Salvage radiation ± hormone therapy; active surveillance for a slow, biochemical-only rise | Earlier salvage radiation, at a lower PSA, is generally associated with better outcomes |
| Recurrence after radiation | Salvage surgery, cryotherapy, or HIFU | Higher side-effect risk than the same procedure done first-line |
| Distant (metastatic) spread | Hormone therapy ± additional systemic agents | Goal shifts from cure toward long-term control |
Source: general framework per American Cancer Society and NCCN guidance; individual options are decided with your care team.
✅ Patient Action: Ask a urologic or radiation oncologist which option matches your imaging and prior treatment — and specifically how each choice weighs cure potential against side-effect risk in your case. The American Cancer Society’s guidance on treating recurrent prostate cancer is a useful reference to bring along.
When to act, and how to cope with the fear
A possible recurrence is as much an emotional event as a medical one, and both deserve attention.
What to do this week
Three concrete steps turn worry into action: confirm the number with the repeat test your doctor orders, schedule the follow-up appointment, and write down your questions before you go.
Symptoms that warrant a prompt call
Most men feel completely well. Still, call your care team without waiting if you develop new bone pain, blood in the urine, or new difficulty urinating between scheduled tests.
Coping and support
The fear that arrives with a rising PSA is real and valid — many men describe it as harder than the original diagnosis. Lean on your care team, a support group, or a counselor; staying active and keeping a healthy weight support overall wellbeing, though they do not treat a recurrence. Structured survivorship follow-up remains your strongest tool for catching any change early.
Frequently asked questions about prostate cancer recurrence
1. Does a rising PSA always mean prostate cancer is back?
No. A single rising PSA can reflect lab variation, so confirmed prostate cancer recurrence needs a repeat test showing a sustained rise. After surgery, that means a PSA of 0.2 ng/mL or higher on two readings; after radiation, a rise of 2 ng/mL above your lowest level. Confirm any rise with your oncologist.
2. What PSA level means recurrence after prostate surgery?
After radical prostatectomy, prostate cancer recurrence is generally defined as a PSA of 0.2 ng/mL or higher on two consecutive tests, per American Urological Association guidance. Some clinicians act near 0.1 ng/mL depending on surgical pathology. A single reading is not enough — confirm the trend with your urologist.
3. What PSA level means recurrence after radiation?
After radiation therapy, prostate cancer recurrence follows the ASTRO-Phoenix standard: a PSA rising 2 ng/mL or more above your nadir, the lowest level after treatment. PSA does not fall to undetectable after radiation, so this rule replaces the surgical one. Ask your radiation oncologist what your nadir was.
4. What is PSA doubling time and why does it matter?
PSA doubling time is how long your PSA takes to double. In research, a shorter time — under roughly 6 to 9 months — links to higher risk of prostate cancer recurrence spreading, while a slow rise is less concerning. Ask your oncologist to calculate yours.
5. How likely is prostate cancer to come back after treatment?
Studies estimate roughly 20% to 40% of men develop biochemical prostate cancer recurrence within 10 years of surgery or radiation, with some estimates higher. This is a population figure, not your personal odds, and a rising PSA is a lab finding rather than a prognosis. Gleason score and stage shape individual risk.
6. Is recurrent prostate cancer more aggressive than the first time?
Not necessarily. Recurrent prostate cancer is often about as aggressive as the original disease — if your first cancer was high-grade, a recurrence is more likely aggressive too. Your original Gleason score guides how a recurrence may behave. Your oncologist can interpret your specific risk factors.
7. What is a PSMA PET scan and when is it used?
A PSMA PET scan detects prostate cancer cells by binding to a protein on their surface. It is used after a confirmed rising PSA to locate prostate cancer recurrence, and it can find disease at low PSA levels that older scans miss. Your team decides when it fits.
8. What are the treatment options if cancer returns after surgery?
After surgery, options for prostate cancer recurrence may include salvage radiation therapy, sometimes with hormone therapy, or active surveillance for a slow biochemical-only rise. The choice depends on where the cancer is and how fast PSA rises. Discuss cure-versus-side-effect trade-offs with a radiation or medical oncologist.
9. What are the options if cancer returns after radiation?
After radiation, treating prostate cancer recurrence may involve salvage surgery, cryotherapy, or high-intensity focused ultrasound, plus hormone therapy in some cases. These procedures carry higher side-effect risks after radiation than as a first treatment. A urologist experienced in salvage procedures should review the realistic risks with you.
10. Can recurrent prostate cancer be cured?
Sometimes. When prostate cancer recurrence is caught early and stays local, salvage treatment can still aim for cure, and many men do well. When cancer has spread to distant sites, the goal usually shifts to long-term control. Outlook depends on location, doubling time, and prior treatment — discuss specifics with your oncologist.
11. How often should I get PSA tests after treatment?
PSA testing after prostate cancer treatment is typically every few months early on, then less often if levels stay low, but your care team sets the schedule by your risk. Regular testing catches recurrence early, often before symptoms. Confirm your personal follow-up schedule with your oncologist.
The bottom line on prostate cancer recurrence
A rising PSA after treatment is a prompt to investigate, not a verdict. The single number matters less than the trend — your PSA doubling time — and modern imaging like a PSMA PET scan means even a low, rising PSA can be located and acted on.
Effective next steps exist whether recurrence is local or distant, chosen with your care team based on your prior treatment and your scans. You now know what the numbers mean and what to ask — bring your written questions to your next appointment.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.