On This Page – Quick Medical Summary
A diagnosis of metastatic prostate cancer — also called advanced or stage 4 prostate cancer — often arrives with a single number attached: a 38% five-year relative survival rate. If you found this page after seeing the word “metastatic,” “distant,” or “stage 4” on a report, that number can land like a verdict. It is not one, and the rest of this page explains why.
Where you are right now shapes what you need most:
- Newly diagnosed? Start with what metastatic actually means and where the 38% figure comes from.
- Caring for a partner or parent? The treatment and warning-signs sections will matter most to you.
- Reassessing the outlook after living with prostate cancer for a while? The statistics section puts that number in real context.
Metastatic prostate cancer usually cannot be cured, but it can be treated — often for years. The survival figure you may have seen reflects men diagnosed several years ago, before the newest therapies were in wide use. It describes a population’s past, not your future. Here is what the evidence actually says.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice, diagnosis, or a treatment, medication, or insurance recommendation. Survival statistics describe groups of people, not individuals. Decisions about staging, treatment, medication, and clinical trials should be made with a board-certified medical oncologist or urologic oncologist who knows your full history. If a symptom worries you, contact your care team rather than waiting.
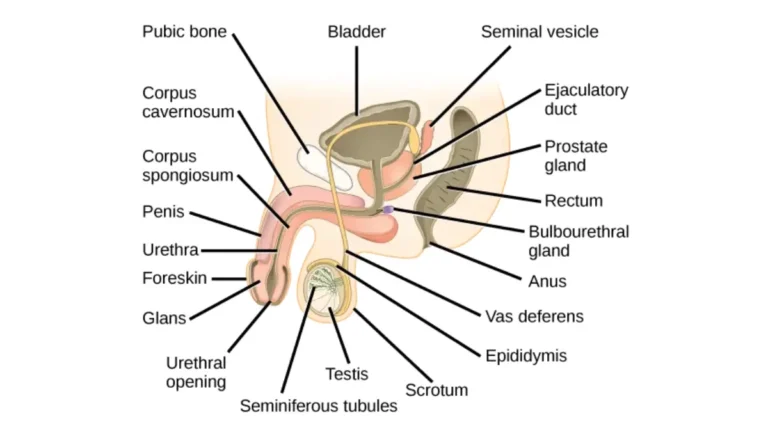
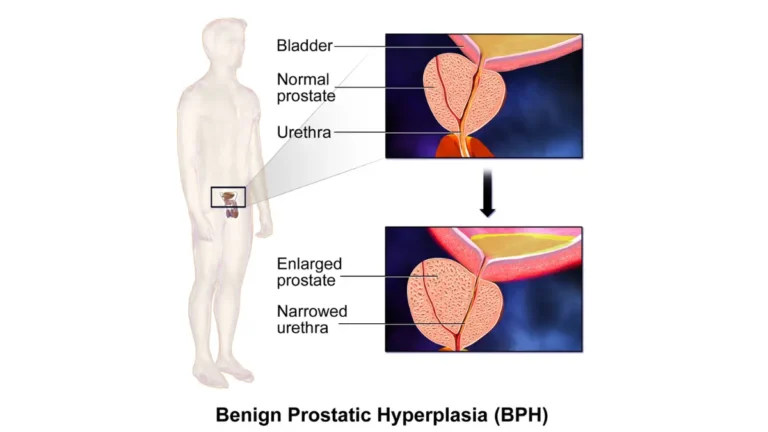
What metastatic prostate cancer actually means
Metastatic prostate cancer is prostate cancer that has spread beyond the prostate gland and the nearby pelvic tissue to distant parts of the body. The most common destination, by a wide margin, is bone.
Where prostate cancer spreads first
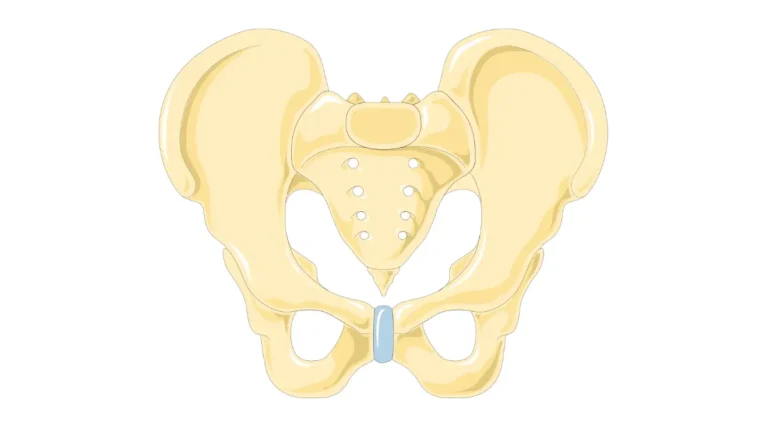
When prostate cancer cells break away, they travel through the bloodstream or lymphatic system and settle elsewhere. According to the American Cancer Society and the National Cancer Institute, the bones are the most common site — especially the spine, pelvis, hips, ribs, and upper thighs. It can also reach distant lymph nodes, the liver, and the lungs.
🔬 How It Works: Prostate cancer in bone is usually osteoblastic — the cancer signals bone cells to overbuild, so the bone turns dense rather than developing holes. That dense, abnormal bone is weaker than healthy bone, which is why fractures and pain can follow.
Metastatic, advanced, stage 4 — the same thing?
Largely, yes. “Metastatic,” “advanced,” and “stage 4” (the distant stage) all describe cancer that has spread beyond the prostate and immediate surrounding area. You may see these terms used interchangeably across reports and clinicians.
Treatable but not curable: what that means
Once prostate cancer reaches distant sites, current medicine can rarely eliminate it entirely. What treatment can do is control the cancer, ease symptoms, and extend life — sometimes for many years. If you want the full staging picture first, our pillar guide explains how prostate cancer is staged from early disease through advanced stages.
Symptoms and how metastatic spread is confirmed
The symptoms of metastatic prostate cancer depend almost entirely on where the cancer has traveled. Many overlap with non-cancer conditions, so only testing can confirm spread.
Common symptoms of metastatic prostate cancer
Possible signs reported by cancer authorities include:
- Bone pain — the most common symptom of bone spread, often persistent and sometimes worse at night
- Bones that fracture more easily, or new back, hip, or thigh pain
- Fatigue and unintended weight loss
- Urinary changes, or blood in the urine or semen
- Swelling in the legs or pelvic area
- Nausea, excessive thirst, or confusion, which can signal high blood calcium from bone breakdown
These symptoms do not confirm metastasis on their own. They warrant a conversation with your care team rather than self-diagnosis.
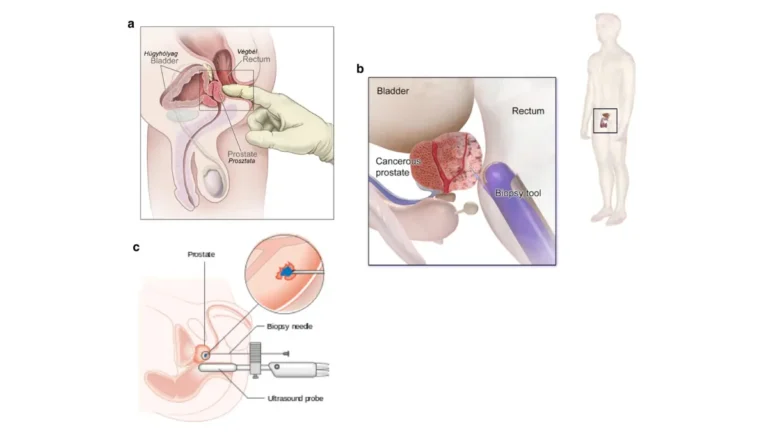
How doctors confirm distant spread
Confirming spread typically combines a rising PSA level with imaging — a bone scan, CT, MRI, or a PSMA PET scan — and sometimes a biopsy of a suspected site.
Why PSMA PET changed staging
A PSMA PET scan detects prostate cancer cells more sensitively than older imaging, picking up smaller deposits that a standard scan can miss. Our detailed guide explains how PSMA PET imaging works and when it is used.
✅ Patient Action: Before treatment planning, ask your urologist or oncologist whether a PSMA PET scan is appropriate for staging your cancer accurately.
How the distant stage fits into prostate cancer staging
To read any survival number correctly, it helps to know how the figures are grouped. The SEER database — the national cancer statistics program — sorts prostate cancer not by stage 1 through 4, but into three buckets.
Localized, regional, and distant — the SEER groups
- Localized: no sign the cancer has spread outside the prostate
- Regional: spread to nearby tissue or pelvic lymph nodes
- Distant: spread to far parts of the body, such as bone or distant organs — this is metastatic disease
How many men are diagnosed at the distant stage
Most prostate cancers are caught early. Around 8% are diagnosed at the distant stage, while the large majority are found while still localized or regional, where survival approaches 100%. The American Cancer Society notes that advanced-stage diagnoses have been rising in recent years, which is part of why this information matters now. You can review the SEER stage-distribution data directly. Your Gleason score also shapes prognosis within any stage; our guide explains what your Gleason score means.
📊 Clinical Data Point: About 8% of prostate cancers are diagnosed at the distant (metastatic) stage. — Source: American Cancer Society, Prostate Cancer Statistics (2025), based on SEER data for men diagnosed 2015–2021.
The 38% survival rate — and what it really tells you
Here is the number most readers came for, with the context needed to read it honestly. The five-year relative survival rate for distant-stage prostate cancer is about 38%, compared with nearly 100% for localized and regional disease.
📊 Clinical Data Point: Five-year relative survival is roughly 38% for distant-stage prostate cancer versus nearly 100% for localized and regional disease. — Source: American Cancer Society, Prostate Cancer Statistics (2025), SEER 2015–2021.
| Stage at diagnosis | 5-year relative survival | Key clinical detail |
|---|---|---|
| Localized (confined to the prostate) | ~100% | Often curable with surgery or radiation |
| Regional (nearby tissue or nodes) | ~100% | Still highly treatable |
| Distant / metastatic (bone, distant organs) | 38% | Treatable, not usually curable; outcomes improving |
Source: American Cancer Society, Prostate Cancer Statistics (2025), based on SEER data for men diagnosed 2015–2021.
What “5-year relative survival” actually measures
This figure compares men diagnosed with distant-stage prostate cancer to men in the general population, then asks how many are still alive five years later. It is a five-year snapshot of a past group — not a prediction of how long any one person will live, and not a countdown.
Does the 38% apply to everyone?
No. The number is an average across a very mixed group. An individual’s outlook shifts with PSA level, Gleason score, how far and where the cancer has spread, age, overall health, and — importantly — how well the cancer responds to treatment.
Is metastatic prostate cancer survival improving?
There is reason for measured hope. A 2025 analysis of SEER data presented at the ESMO Congress reported that five-year relative survival for metastatic prostate cancer has been climbing across diagnosis years — roughly 29% for men diagnosed in 2010, rising in later years. Because the 38% figure reflects men diagnosed through 2021, it cannot fully capture the newest therapies, meaning it likely understates the outlook for someone diagnosed today. You can read more about what daily life with stage 4 disease can look like, and review the current five-year survival rates by stage at the American Cancer Society.
✅ Patient Action: Ask your medical oncologist what your individual outlook looks like given your specific PSA, Gleason score, and sites of spread — the population figure cannot account for any of these.
How metastatic prostate cancer is treated today
Treatment for metastatic prostate cancer has changed substantially in the past decade, which is part of why survival is improving. The approach is usually whole-body and built around lowering the hormones that feed the cancer.
Hormone-sensitive vs. castration-resistant disease
At first, most metastatic prostate cancer responds to lowering testosterone — this phase is called hormone-sensitive disease. Over time, the cancer typically learns to grow even when testosterone is very low, a phase called castration-resistant disease, often signaled by a rising PSA.
🔬 How It Works: Prostate cancer is fueled by testosterone. Androgen deprivation therapy lowers it to slow the cancer. Research now shows that this hormone therapy alone is often not enough for metastatic disease, so modern care usually combines it with additional agents from the start.
The main treatment types
Depending on the situation, an oncologist may draw on:
- Androgen deprivation therapy (ADT) plus newer hormone-pathway agents, the backbone of first-line treatment
- Chemotherapy for prostate cancer, such as docetaxel, often combined with hormone therapy
- PSMA-targeted radioligand therapy for certain PSMA-positive castration-resistant cancers
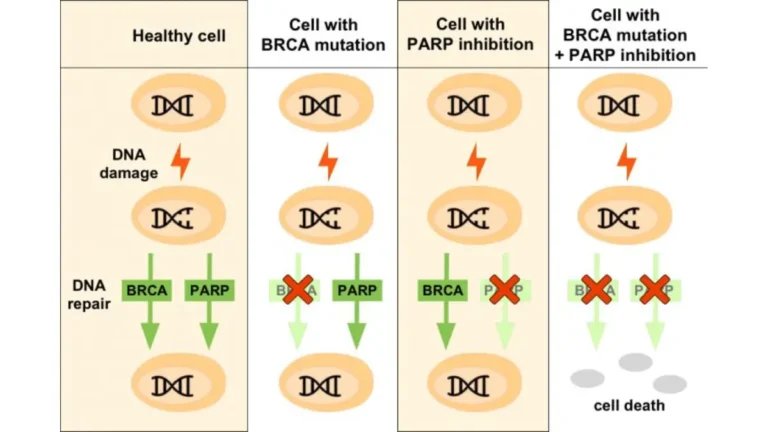
- PARP inhibitors for cancers with specific inherited or tumor mutations
- Immunotherapy in selected cases
Why genetic testing matters for advanced disease
Inherited mutations such as BRCA1 or BRCA2 can change which treatments are options, and they carry information for blood relatives. You can assess inherited risk factors and discuss formal testing with your team. For the standard-of-care picture, see the National Cancer Institute’s treatment overview, and you can search for open prostate cancer clinical trials if you want to explore newer options.
✅ Patient Action: Ask your oncologist which phase you are in — hormone-sensitive or castration-resistant — and whether genetic or biomarker testing should guide your treatment plan.
Warning signs to act on and questions to ask your team
Living with metastatic prostate cancer means knowing which symptoms can wait for a routine visit and which cannot. A few situations need urgent attention.
Symptoms that need prompt medical attention
⚠️ Clinical Warning: When prostate cancer spreads to the spine, it can press on the spinal cord. New or worsening back pain combined with leg weakness, numbness, or loss of bladder or bowel control may signal spinal cord compression — a medical emergency. Contact your treatment team immediately or seek emergency care; rapid treatment can prevent permanent nerve damage.
Signs of high blood calcium — intense thirst, nausea, or new confusion — also warrant prompt evaluation rather than waiting.
Questions to ask your oncologist
It helps to walk into an appointment with a written list. Useful questions include: what does my individual prognosis look like; which treatment phase am I in; should I have genetic or biomarker testing; am I eligible for a clinical trial; and how will we manage bone pain and protect my bone health? You can bring these questions with you so nothing gets missed.
Frequently asked questions about metastatic prostate cancer
1. What does it mean when prostate cancer is metastatic?
Metastatic prostate cancer means cancer that began in the prostate has spread beyond the gland and nearby pelvic tissue to distant parts of the body, most often the bones. It is also called advanced or stage 4 prostate cancer. It is generally treatable but not curable. Discuss your specific situation with a urologic or medical oncologist.
2. Where does prostate cancer spread first?
Prostate cancer most commonly spreads to the bones — particularly the spine, pelvis, hips, ribs, and upper thighs — according to the American Cancer Society and the National Cancer Institute. It can also reach distant lymph nodes, the liver, and the lungs. Bone pain is often the first noticeable symptom of this spread.
3. Is stage 4 prostate cancer curable?
Stage 4 (metastatic) prostate cancer usually cannot be cured, but it can be controlled and treated, often for years. Treatment focuses on slowing the cancer, relieving symptoms, and extending life. Outcomes are improving with newer therapies. Your oncologist can explain what the realistic goals are for your specific case.
4. How long can you live with metastatic prostate cancer?
There is no single answer. The five-year relative survival rate for distant-stage prostate cancer is about 38% (American Cancer Society, 2025), but that is a population average from men diagnosed years ago. Individual survival varies widely with PSA, Gleason score, extent of spread, and treatment response. Ask your medical oncologist about your specific outlook.
5. Does the 38% survival rate apply to everyone?
No. The 38% five-year relative survival figure is an average across a diverse group of men diagnosed between 2015 and 2021. An individual’s outlook depends on PSA level, Gleason score, where and how far the cancer has spread, age, overall health, and how the cancer responds to treatment. Your oncologist can give you a more personalized picture.
6. Is metastatic prostate cancer survival improving?
Evidence suggests it is. A 2025 SEER data analysis presented at the ESMO Congress reported five-year relative survival for metastatic prostate cancer rising across diagnosis years. Because the 38% figure reflects men diagnosed through 2021, it likely understates today’s outlook, since the newest treatments are not fully captured. Your oncologist can explain how current therapies may apply to you.
7. What are the symptoms of metastatic prostate cancer?
Symptoms depend on where the cancer has spread. Common signs include bone pain (often in the spine, hips, or thighs), fractures, fatigue, weight loss, urinary changes, blood in the urine or semen, and leg swelling. High blood calcium can cause nausea or confusion. These symptoms have many causes, so see your care team for evaluation.
8. How is metastatic prostate cancer diagnosed?
Doctors confirm metastatic prostate cancer using a rising PSA level alongside imaging — a bone scan, CT, MRI, or a PSMA PET scan — and sometimes a biopsy of a suspected site. A PSMA PET scan detects spread more sensitively than older imaging. Ask your urologist or oncologist which imaging is appropriate for accurate staging.
9. What treatments are used for metastatic prostate cancer?
Treatment usually begins with androgen deprivation therapy to lower testosterone, now often combined with additional hormone-pathway agents. Depending on the case, options include chemotherapy, PSMA-targeted radioligand therapy, PARP inhibitors for certain mutations, and immunotherapy. The plan is tailored to your disease. Your medical oncologist determines which combination fits your situation.
10. What’s the difference between hormone-sensitive and castration-resistant disease?
Hormone-sensitive metastatic prostate cancer responds to lowering testosterone. Over time, most cancers progress and keep growing even when testosterone is very low — this is castration-resistant disease, often marked by a rising PSA. The distinction guides which treatments come next. Ask your oncologist which phase you are in and what it means for your plan.
11. When is metastatic prostate cancer a medical emergency?
Seek urgent care if you develop new or worsening back pain with leg weakness, numbness, or loss of bladder or bowel control — these can signal spinal cord compression, an emergency that needs rapid treatment to prevent permanent nerve damage. Signs of high blood calcium, such as severe thirst or confusion, also need prompt evaluation. Contact your team immediately.
The bottom line
A 38% five-year survival figure can read like a sentence, but it is a population average from the past — not a prediction for you, and not the full story. Metastatic prostate cancer is generally treatable rather than curable, often for years, and survival has been climbing as newer therapies reach more men.
The most useful next step is a focused conversation with a medical oncologist about your specific PSA, Gleason score, sites of spread, and treatment options, including whether genetic testing or a clinical trial fits your case. Our guides to hormone therapy and the full staging picture can help you prepare for that appointment. The number is a starting point for that conversation, not the end of it.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.