On This Page – Quick Medical Summary
If your oncologist has raised immunotherapy, or you are weighing options after prostate cancer stopped responding to hormone treatment, you are likely trying to answer one question: what would this actually do for me? This guide is written for three readers. If you or someone you love was just told the cancer is metastatic and castration-resistant, the sections on what Provenge does and who qualifies are for you. If you are comparing treatments, the comparison with other options will help most. If you are a caregiver organizing care, the treatment-process and side-effect sections explain what to expect.
Immunotherapy uses a person’s own immune system to recognize and attack cancer. For prostate cancer, the main approved option is Provenge (sipuleucel-T) — the first immunotherapy the U.S. Food and Drug Administration approved for this disease. It can extend survival for a specific group of men. It is not a cure, and being clear about that from the start is part of using it well. Here is how prostate cancer treatment fits together across each stage, and where Provenge sits within it.
ℹ️ Medical Disclaimer: This article explains a treatment, a medication, a diagnostic process, and survival data for general education only. It does not diagnose disease, recommend or prescribe treatment, or replace your care team’s judgment. Decisions about Provenge, other immunotherapy, or any prostate cancer treatment should be made with a board-certified urologist or medical oncologist who knows your full history.
What Provenge actually does
Provenge (sipuleucel-T) is a personalized immunotherapy that uses a man’s own immune cells to target prostate cancer; it is given as three infusions and has been shown to extend survival in advanced disease.
How your own immune cells are used
Provenge is an autologous cellular immunotherapy, meaning it is built individually from each patient’s cells rather than mass-produced. Immune cells called antigen-presenting cells are collected from the blood, sent to a laboratory, activated, then returned to the same patient. Because every dose is made from one person’s own cells, it can be given only to that person.
🔬 How It Works: In the lab, your immune cells are exposed to a protein called prostatic acid phosphatase (PAP) — found on most prostate cancer cells — fused to an immune-signaling molecule (GM-CSF). This trains the cells to flag PAP as a target. Once reinfused, they help your wider immune system recognize and attack prostate cancer cells carrying PAP.
What targeting PAP means
PAP is made in prostate tissue and rises as prostate cancer progresses, which makes it a useful flag for the immune system. Provenge contains no drug that directly kills cancer; instead it prompts a T-cell response against PAP-bearing cells, which is why it is classed as a therapeutic cancer vaccine rather than how immunotherapy works in cancer treatment of the chemotherapy kind. The mechanism and manufacturing steps are described in the FDA’s overview of how Provenge is made and works.
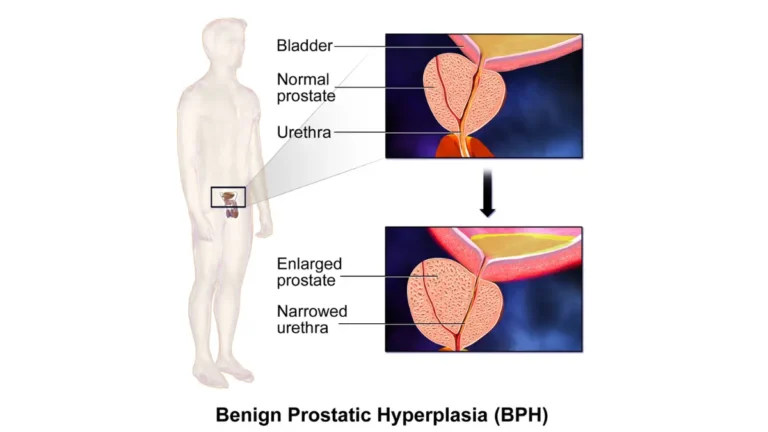
Who Provenge is — and isn’t — for
Provenge is approved for men who meet three conditions:
- The cancer is metastatic — it has spread beyond the prostate.
- It is castration-resistant — still progressing despite treatment that lowers testosterone.
- It is causing few or no symptoms (asymptomatic or minimally symptomatic).
The three core eligibility criteria
Metastatic means the cancer has reached lymph nodes, bone, or other sites, which you can read more about in what the stages of prostate cancer mean. Castration-resistant means it keeps growing even after hormone therapy that lowers testosterone has been working. The “few or no symptoms” requirement is central — Provenge is positioned for men who feel relatively well, not those in significant pain.
When Provenge is not recommended
Provenge has not been shown to help when cancer has spread to the liver or other internal organs (visceral metastases), and it is not recommended in that setting. It is also not used for small cell or neuroendocrine prostate cancer. These limits matter, because a man who does not fit them deserves to learn that early rather than after hope is raised.
⚠️ Clinical Warning: Provenge is not recommended for men with visceral (organ) metastases or small cell/neuroendocrine prostate cancer, where benefit has not been shown. Confirming the exact location and type of spread is part of deciding whether it is an option — a job for your oncologist, not a self-assessment.
Why timing matters
In the trials, the clearest benefit appeared in men with a lower disease burden, one reason Provenge is used for earlier, less symptomatic castration-resistant disease rather than late, heavily symptomatic disease. Eligibility also weighs general fitness and recent steroid or chemotherapy use.
✅ Patient Action: Ask your medical oncologist: “Given my scans and symptoms, am I a candidate for Provenge, or do the location of my metastases or my symptom level rule it out?”
What getting Provenge actually involves
Provenge is given as three infusions about two weeks apart, and each one is preceded a few days earlier by a cell-collection step called leukapheresis.
The collection step (leukapheresis)
About three days before each infusion, your white blood cells are collected at a cell-collection center through leukapheresis, which filters cells from your blood and usually takes three to four hours. Those cells go to the manufacturer, are activated against PAP, and come back as your personalized dose. The process is described in the MedlinePlus drug information for sipuleucel-T.
📊 Clinical Data Point: A full course is 3 doses given about 2 weeks apart, each infused into a vein over roughly 60 minutes. — Source: FDA prescribing information and MedlinePlus (NLM), 2023.
The three infusions
Before each infusion, patients are typically given acetaminophen and an antihistamine to reduce reactions. The three doses together make up one complete course, and the schedule is personalized so collection and infusion dates line up for each man.
What to expect on infusion day
Infusions happen in a clinic or infusion center with monitoring. Reactions, when they occur, tend to start during the infusion and are usually short-lived. Bringing a caregiver and planning a restful day afterward is reasonable.
🩺 Physician Note: Because Provenge is made from one person’s cells, the labeling stresses that the leukapheresis-and-infusion schedule is personalized and that each dose is given only to the patient it was made for — keeping appointments on schedule matters for the product’s preparation.
What the evidence shows about Provenge and survival
Provenge has not been shown to shrink prostate tumors or delay their progression on scans. Instead, it extended overall survival in clinical trials — a benefit that shows up in how long men lived, not in tumor size.
How much longer: the IMPACT trial
In the phase 3 IMPACT trial of 512 men with metastatic castration-resistant prostate cancer, those who received Provenge lived a median of 25.8 months versus 21.7 months with placebo — about a 4.1-month improvement, with a 22% reduction in the relative risk of death. A median is the midpoint of a group, not a promise for any one person. Some men gained more time, others less.
📊 Clinical Data Point: Median overall survival was 25.8 months with Provenge versus 21.7 months with placebo (a 4.1-month benefit; 22% relative reduction in risk of death). — Source: IMPACT trial, New England Journal of Medicine, 2010.
Why scans may not change
Here is the point many summaries skip: because Provenge works through the immune system rather than by directly killing tumor cells, scans and PSA can keep rising even when the treatment is helping. A progressing scan after Provenge is not automatically a sign of failure, which is why oncologists judge its benefit differently than chemotherapy. You can read more about prognosis in life expectancy with metastatic prostate cancer.
What real-world data adds
Outside the trials, a large registry of men treated with Provenge reported survival broadly consistent with the trial findings. The clearest benefit in studies appeared in men with a lower disease burden, supporting earlier use in castration-resistant disease.
🩺 Physician Note: Current patient guidance from the American Cancer Society describes Provenge as not shown to stop prostate cancer from growing, while studies suggest it may help some men live an average of several months longer — and, like hormone therapy and chemotherapy, it has not been shown to cure the disease.
Provenge vs. other immunotherapy for prostate cancer
Besides Provenge, the checkpoint inhibitor pembrolizumab is FDA-approved for the small share of prostate cancers with specific genetic features; most prostate cancers do not have them.
Why prostate cancer is a “cold” tumor
Prostate cancer is often called immunologically “cold,” meaning it tends not to draw a strong immune attack. That is a major reason the checkpoint inhibitor drugs that transformed melanoma and lung cancer have so far helped far fewer men with prostate cancer. Provenge’s vaccine approach was designed to work around that coldness, and it remains the only immunotherapy with a prostate-specific FDA approval.
Pembrolizumab for MSI-H, dMMR, or TMB-high tumors
Pembrolizumab (Keytruda) is approved across cancer types — including prostate — when a tumor is microsatellite instability-high (MSI-H), mismatch-repair deficient (dMMR), or has a high tumor mutational burden. Only about 3–5% of prostate cancers carry these features, which is why testing the tumor matters. Because dMMR can be linked to inherited Lynch syndrome, some men benefit from genetic counseling and may want to assess inherited cancer-risk factors.
Where each option fits
A patient-friendly overview sits in the American Cancer Society’s guide to prostate cancer immunotherapy.
| Treatment | Type | Who it’s for | What the evidence shows | Best for patient profile |
|---|---|---|---|---|
| Provenge (sipuleucel-T) | Cellular immunotherapy (vaccine) | Metastatic castration-resistant, few/no symptoms, no visceral spread | ~4.1-month median survival gain; no tumor shrinkage | Earlier, low-symptom castration-resistant disease |
| Pembrolizumab | Immune checkpoint inhibitor | mCRPC that is MSI-H, dMMR, or TMB-high (~3–5%) | Responses in biomarker-selected men; limited in others | Tumor with specific genetic markers |
| Other systemic options | Chemotherapy, hormonal agents, radioligand therapy | Varies by spread and prior treatment | Established survival roles in mCRPC | Depends on symptoms, spread, prior therapy |
Verified against FDA labeling, the American Cancer Society, and the IMPACT trial (NEJM, 2010).
For men whose cancer is PSMA-positive and has progressed after other treatments, Pluvicto (lutetium-177) radioligand therapy is another advanced-disease option, and chemotherapy such as docetaxel has an established survival role.
Radiation therapy is also used in specific situations. Provenge is often given earlier than chemotherapy because it suits men with few symptoms.
Provenge side effects and warning signs
The most common Provenge side effects are usually mild to moderate and include:
- chills
- fatigue
- fever
- back pain
- nausea
- joint ache
- headache
Common side effects
These reactions most often begin during the cell infusion and tend to last no more than a couple of days, reflecting the immune system being activated. Acetaminophen and an antihistamine are usually given beforehand to reduce them. A reference summary is available in the NCI drug information for sipuleucel-T.
Serious reactions and red flags
Less commonly, more serious problems can occur, including severe infusion reactions, trouble breathing or high blood pressure, and — reported rarely — stroke. Men who need a central venous catheter for treatment can develop infections, including sepsis. These are reasons to seek care promptly rather than wait.
⚠️ Clinical Warning: After a Provenge infusion, seek urgent medical care for trouble breathing, chest pain, a fast or irregular heartbeat, fainting, sudden weakness or trouble speaking (possible stroke), or fever with redness or pain at the infusion or collection site (possible infection).
✅ Patient Action: Before your first infusion, ask your oncology nurse: “Which symptoms after treatment mean I should call your team, and which mean I should go to the emergency room?”
Frequently asked questions about Provenge
1. What does Provenge (sipuleucel-T) do?
Provenge is a personalized immunotherapy that uses your own immune cells, activated against a prostate cancer protein (PAP), to help your immune system attack prostate cancer. It is given as three infusions and has been shown to extend survival in advanced, castration-resistant disease. Whether it fits your situation is a decision for your oncologist.
2. Who is eligible for Provenge?
Provenge is approved for men with metastatic, castration-resistant prostate cancer who have few or no symptoms and no spread to internal organs such as the liver. Men with small cell or neuroendocrine prostate cancer are not candidates. Your oncologist confirms eligibility using your scans and symptoms.
3. How many Provenge treatments do you need?
A full course of Provenge is three doses, given about two weeks apart, each infused over roughly 60 minutes. About three days before each dose, your immune cells are collected through leukapheresis and made into that dose. Your care team coordinates the personalized schedule.
4. Does Provenge shrink prostate tumors?
No — Provenge has not been shown to shrink prostate tumors or delay their progression on scans. Its benefit appears as longer survival rather than smaller tumors, so an unchanged or progressing scan does not automatically mean the treatment failed.
5. How much longer do you live with Provenge?
In the IMPACT trial, men receiving Provenge lived a median of 25.8 months versus 21.7 months with placebo — about a 4.1-month improvement. A median is a group average, not a guarantee; some men gain more time and some less. Your oncologist can discuss what is realistic for you.
6. What are the side effects of Provenge?
The most common Provenge side effects are chills, fatigue, fever, back pain, nausea, joint ache, and headache, usually mild to moderate and lasting a couple of days. Rarely, serious reactions including severe infusion reactions or stroke can occur. Seek urgent care for breathing trouble or stroke-like symptoms.
7. Is Provenge a cure for prostate cancer?
No. Provenge is not a cure for prostate cancer; like hormone therapy and chemotherapy, it has not been shown to cure the disease. It is used to extend survival for a specific group of men with advanced, castration-resistant prostate cancer who have few or no symptoms.
8. Is Provenge chemotherapy?
No. Provenge is an immunotherapy, not chemotherapy. It contains no drug that directly kills cancer cells; instead it activates your own immune cells against a prostate cancer marker. This is why its side-effect pattern and the way doctors measure its benefit differ from chemotherapy.
9. Can you have Provenge with liver or visceral metastases?
Provenge is not recommended when prostate cancer has spread to the liver or other internal organs, because benefit has not been shown in that setting. The location of metastatic spread is one of the key factors your oncologist checks before considering Provenge.
10. What other immunotherapy is available for prostate cancer?
Besides Provenge, the checkpoint inhibitor pembrolizumab is approved for prostate cancers that are MSI-H, dMMR, or have a high tumor mutational burden — only about 3–5% of cases. Most prostate cancers are immunologically “cold” and respond poorly to checkpoint immunotherapy.
11. What is leukapheresis, and how is Provenge given?
Leukapheresis is a procedure that filters white blood cells from your blood, taking about three to four hours, done roughly three days before each Provenge dose. Those cells are activated in a lab and returned to you by IV infusion. Each dose is made for, and given only to, you.
The bottom line on Provenge for prostate cancer
Provenge is a real, FDA-approved immunotherapy that can add time for a specific group of men — those with metastatic, castration-resistant prostate cancer who have few or no symptoms and no spread to internal organs. It works by turning a man’s own immune cells against a prostate cancer marker, and its benefit shows up as longer survival rather than smaller tumors. It does not cure the cancer, and unchanged scans do not mean it failed. The most useful next step is a focused conversation with a medical oncologist about whether you qualify and what to expect.
✅ Patient Action: Bring three questions to that visit: am I eligible, should my tumor be tested for markers like MSI-H, and how will we measure whether the treatment is helping?
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.